Article Text

Statistics from Altmetric.com
SUMMARY BOX
The European regulatory agencies for medicine and healthcare products are committed to a health democracy approach.
The patient could be involved at the various stages of the assessment of the benefit–risk balance of health products and decision-making processes: (1) integration of patients’ representatives as stakeholders in decision-making committees, (2) coconstruction of benefit–risk assessment with patients’ views and (3) patients’ experience and feedback as inputs to the assessment of the benefit–risk balance.
The contributions and competencies of different profiles such as users, caregivers, patients, patient representatives, victims, support organisations and patient partners should be taken into account. Their profiles and objectives should be adapted to the different levels of participation.
Experiential knowledge is complementary to medical and scientific expertise. Patient and expert participations must follow the same principles and rules, particularly in terms of ethics and links of interest.
Support should be provided to raise their awareness of the regulatory agency environment and offer them continuous capacity-building.
Introduction
In France and Europe,1–4 medicine and healthcare products regulatory agencies have been proactively engaging in health democracy for the last decade. Since 2002, the French legislation has evolved to guarantee the rights of healthcare system’s users.5 Thus, eligible patients and health system user organisations are systematically represented in French health agencies as in some other countries.6
Beyond the integration of their representatives as members of committees and as part of its transparency policy, the French National Agency for Medicines and Health Products Safety (ANSM) is striving to involve patients at the various stages of the assessment and decision-making processes, but also all people concerned with health products. These are members of the public having different profiles, such as patients, users of the health system, caregivers, victims, patient representatives, support organisations and patient partners. Regulatory agencies are responsible for the benefit–risk (BR) assessment associated with the use of health products throughout their life cycle, from clinical development to market approval and the continuous reassessment of the BR balance thereafter. The assessment processes are driven by patient risk management, enabling the Agency to make decisions in a public health policy. ANSM is particularly willing and attentive to health democracy following the crises it has had to face.7–9
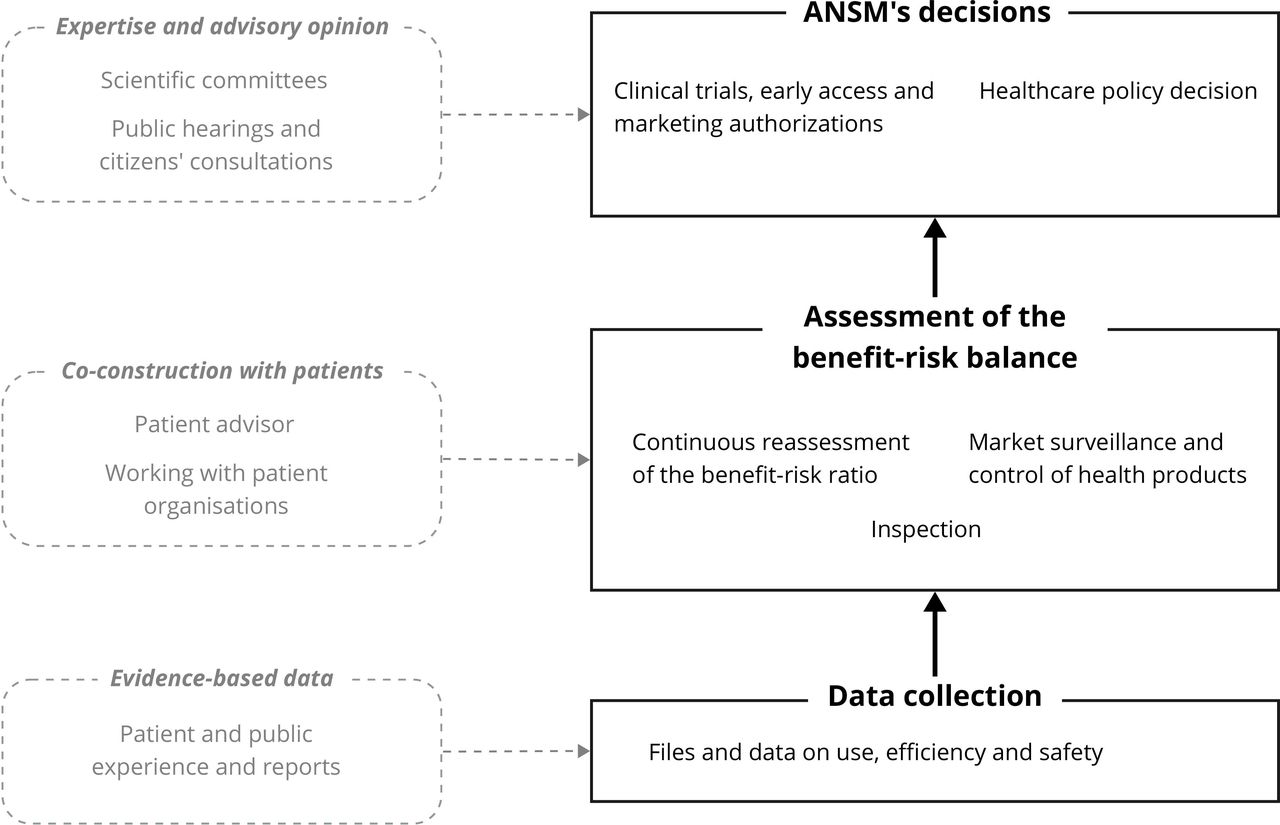
The involvement of the public and patients in a scientific and medical approach raises questions about the necessary adaptation of the BR assessment processes. To improve the BR assessment according to the approach of health democracy, the ANSM’s Scientific Advisory Board has formalised an approach to strengthen ‘people concerned’ involvement in the activities of regulatory agencies such as ANSM. The reflection was based on the ANSM’s experience. In this context, an overview of the patient’s place within regulatory assessment has been drawn up (figure 1), highlighting the conditions and framework necessary to adapt health product evaluation processes to a health democracy approach, considering the difficulties encountered in implementation.

{kind=link}
Overview of the health democracy approach within the French National Agency for Medicines and Health Products Safety
Overview of the current involvement of ‘people concerned’ within the agency
Integration of patients’ representatives as stakeholders in decision-making committees
Since 2019, representatives of patient organisations have been involved in all types and levels of the Agency’s expertise as full members of expertise committees. As such, they participate in all discussions and votes. Their appointment, following an application process, takes into account their initial competencies, which might be supplemented by a 1 day of non-mandatory training provided by the ANSM. Input from expertise committees is requested by the Agency once the BR assessment has been carried out. They provide advisory opinions on which the Agency bases its decisions. The integration of patients’ representatives complies with ethical principles and transparency applied to all members.10 Concerning patients, the independence of patient organisations from the health products industry is also a criterion.
In 2021, 58 patients’ representatives (belonging to 40 different patient organisations) participated in the governance, expertise and dialogue committees of the ANSM. In some scientific committees, it is more difficult to recruit patients’ representatives because of the topics covered (eg, microbiological controls of breast milk from lactarium). Thus, out of the 557 seats of in these committees, 10.8% are attributed to patients’ representatives.
Besides integration of patients into national committees, patients are involved at the European Medicines Agency (EMA) level through their participation as members of the management board and scientific committees for European regulatory decision-making.11
Furthermore, in addition to the decision-making committees, two other types of committees have been set up: a Health Products Information Committee to promote public communication and the dissemination of information, and an ad hoc committee to strengthen the partnership between the Agency and patient organisations and health system users.
Coconstruction of BR assessment to include patients’ views
Before submission to committees, BR assessments are carried out within the Agency. In order to build them, ANSM may request advisory opinions from health professionals as well as from patients or ‘people concerned’ (figure 1).
The Agency has developed several consultation methods with ‘people concerned’.12 Indeed, the Agency has hired a patient partner in its advisor group (a patient advisor) to improve the coconstruction of health policies on health products.13 Where appropriate, the Agency also solicits contributions from specific ‘people concerned’. They can participate as patient organisations’ representatives or as individuals.14 For example, the Agency’s communications on the management of drug shortages are shared with stakeholder organisations prior to publication, to incorporate their feedback where appropriate. In addition, the Agency ensures the implementation of different interaction modes to encourage cooperation with stakeholders. This includes public hearings and citizens’ consultations. The aim is to collect and gather the views of those concerned to integrate them into the agency’s decision-making processes.
Patients’ experience and feedback in the assessment of the BR balance
Involving ‘people concerned’ in the regulation of health products requires the development of different methods to collect patient experience data. These methods must be adapted to the patients and the professionals involved in the regulation process concerned. The Agency seeks to incorporate all dimensions required for establishing the BR balance. Thus, the following collection methods have been implemented:
Since 2011, pharmacovigilance declaration allowing the detection of signals is available to patients and their organisations (38.36% of adverse reaction reports registered in the French pharmacovigilance database were declared by patients in 2021).15 To facilitate this measure, an online portal for reporting adverse health events was set up in 2017 (www.signalement-sante.gouv.fr).
Whistle-blowers contribute to improving healthcare and patient safety.16 Their reports need to be framed. A procedure ensuring the whistle-blowers’ protection and facilitating reporting has been designed to encourage speaking out, urge ‘people concerned’ to denounce problematic situations they face and speak freely. In 2021, among the 313 reports notified to the ANSM, 65% came from private individuals and anonymous, 21% from health professionals and around 10% from employees of health product companies.
Early access approval to drugs is subject to compliance with a protocol for therapeutic use and data collection. This protocol has recently evolved to prospectively collect real-world data (patients’ characteristics, conditions of use, efficacy including quality of life, tolerance).17
With the aim of improving user relations, a unit was created in april 2021 to centralise, coordinate and respond to all kinds of inquiries from the outside (n=4335 in 2021).
To broaden the scope of information collection, the agency is making increasing use of opinion surveys, both among health professionals and the public. Using national samples that are representative of the French population in quantitative terms, knowledge, practices and perceptions are evaluated. Social networks are also used as a channel for direct exchange with the gency’s audiences.
Recently, within the framework of the EMA, the Rapporteur Member States can collect information from patients and users’ organisations for the BR assessment. This is still in the pilot phase, intending to improve methods for systematically integrating patient and consumer organisations views and preferences on the real-life use of health products in regulatory decision-making.18
Initiatives for supporting health democracy in the BR assessment
Four initiatives for the functioning of the health democracy approach were identified to involve ‘people concerned’ in regulatory activities for health products, with the aim of maintaining and encouraging patients’ involvement in the BR assessment from authorisation to surveillance of health products.
Participation in committees
Through the participation of patients’ representatives, the patients’ perspective is considered in the BR balance and help the regulators to make decisions. The patients’ knowledge derived from their experience of health products’ use is complementary to the medical and scientific expertise and should be mobilised in the same way as the latter. It is important to promote their participation and further value their commitment as is done with scientific experts. This applies to the way they are solicited and participate in the assessment, but also regarding compensation or ethical aspects.19 Their participation as members must follow the same ethical rules, and their status should be clarified so that they can contribute as experts.
The attractiveness of patients’ integration needs to be strengthened. Validation of the skills acquired through their participation in the work of regulatory agencies would allow recognition of their input.
‘People concerned’ should be able to be represented in all kind of instances such as governance, expertise and dialogue committees to enhance health democracy approach.
Training of patients’ representatives and building a sense of collegiality
Recruitment is essential to optimise the contribution of the ‘people concerned’ in the work of regulatory agencies. Considering the initial competencies of patients’ representatives and their previous skills in the application procedures can facilitate their recruitment (initial training, professional experience, experience in health products, motivation, willingness, etc).
The need to enhance patients’ and consumers’ understanding of health products regulation process and their role in the process is also acknowledged. Support could be provided to raise their awareness of the regulatory agency’s environment and provide them with continuous capacity-building.
Their participation should be a full-fledged activity within regulatory activities, to create an enabling environment for their commitment and animate the collective of patients’ representatives involved in the committees. In this context, several ways of animating and/or training the network of ‘people concerned’ currently involved could be implemented, including:
The creation of a ‘Health Democracy’ unit in charge of the health democracy approach.
The implementation of a working group gathering all patients’ representatives participating in the agency’s committees to identify the factors that hinder or facilitate their participation.
The organisation of regular exchanges between patients’ representatives and agency’s professionals to provide feedback on patients’ involvement and to jointly consider improvements.
Patient-friendly training and diplomas in health democracy, health products and health systems.20
Different forms of involvement considered
There are different profiles of ‘people concerned’ that need to be considered depending on the subject and the regulatory process. All patients have an experience of the use or conditions of use of health products that can contribute to BR assessment21 and some of them have built up specific knowledge from their experience, through continuous training or a reflective process with their peers or within patient organisations. The contribution of the ‘people concerned’ in the BR assessment varies according to their engagements, their motivations14 and the agencies’ expectations, ranging from simple information or consultation to collaboration or coconstruction.13 21 22 Interface committees and scientific committees are two different forms of patient participation.
The form of involvement expected in the different committees should be made explicit, and the profiles of the ‘people concerned’ adapted according to the various levels of participation, in the same way as it is currently established for medical experts. The parallelism mentioned highlights the interactions developed with the medical experts within committees, the dialogue with representatives of learnt societies, or the use of external expertise in a specific field. The different profiles such as users, caregivers, patients, patients’ representatives, victims, support organisations and patient partners, their contributions and skills should be considered.23 24
Adapt feedback from ‘people concerned’ for the BR assessment
The regulators are committed to ensuring that the patient’s voice is included in BR assessments. Recommendations for the evaluation of health products are currently evolving to integrate the experiential knowledge. In this perspective, the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use has proposed new guidelines to advance patient-centred drug development, integrating patient experience throughout development and thus supporting regulatory decisions.25 The subject of Patient-Reported Outcomes, once validated and effectively aggregated, analysed and verified by the ‘people concerned’, should be addressed as a concrete form of patient involvement in BR assessment.26 Already implemented at national level for health technology assessment, it would be appropriate to integrate them into the marketing authorisation process and thus to develop the European guidelines. Depending on the pilot phase conducted by the EMA, health products regulatory agencies could move forward, allowing for the establishment of ways to collect and use evidence based on experience and results perceived by ‘people concerned’ for decision-making on BR.27 This improvement would allow for the integration of input expressed by the patients, thus developing a health democracy approach.
Conclusion
The ANSM has progressively moved forward towards a health democracy approach. Putting the patient at the centre of its actions is one of its strategic approaches to public health. However, improving the involvement of ‘people concerned’ is not an easy task.28 It should not be limited to organisational methods of committees, but assessment, pharmacovigilance, surveillance and drug development processes should be adapted to incorporate the different forms of patient involvement. Training and support should be offered and tailored to the needs of patients and other members of the public involved in the process. To improve the health democracy approach within the regulatory activities, long-term actions within a continuous improvement loop are required and research undertaken, as for the use of patient-reported outcomes measures, patient-reported experience measures and patient preference studies.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Acknowledgments
The authors are very grateful to the following ANSM officers for their invaluable inputs: N Albin, S Benchetrit, J Chong, P Daynes, P Demolis, C Ingouf, B Jacquot, J Leroy, C Le-Saulnier, JM Race, N Richard, S Vignot, and M Zureik. We would also like to thank patient organisations who participated in the discussions: C Vergely, Y Mazens, JP Plançon (France Asso Santé), B Denis (Union Francophone des Patients Partenaires).
Footnotes
Handling editor Seye Abimbola
Collaborators The Scientific Advisory Board of the ANSM: Joël Ankri, Janine Barbot, Robert Barouki, Henri Bastos, Éric Bellissant, Christiane Druml, Éric Ezan, Didier Houssin, Walter Janssens, Marie-Christine Jaulent, Maria Emilia Monteiro, Dominique Pougheon Bertrand, Vololona Rabeharisoa, Victoria Rollason, Valérie Sautou, Jean-Paul Vernant.
Contributors LB led working group on the need to integrate patients in the benefit–risk assessment and wrote the manuscript. JA chaired the Scientific Advisory Board and working group and supervised the work with PM. DPB, MCJ, VRa, WJ, VRo, JB, JPV and WOG contributed their expertise during ANSM working group sessions and manuscript design and revisions. All authors reviewed the manuscript and provided feedback and edits. All authors approved the final manuscript and the decision to submit for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement statement All authors support the patient involvement in the benefit-risk assessment and decisions concerning health products. The operating principles of the health democracy approach identified for involving patient and public in health product regulatory activities were shared and discussed with two patient representative organisations and with the ANSM’s patient advisor.
Provenance and peer review Not commissioned; externally peer reviewed.