Article Text

Abstract
Background Several countries in Latin America conducted mass distribution of COVID-19 kits intended to treat mild COVID-19, thereby preventing excess hospitalisations. Many of the kits contained ivermectin, an antiparasitic medicine that was not approved at the time for the treatment of COVID-19. The study objective was to compare the timing of the publication of scientific evidence about the efficacy of ivermectin for COVID-19 with the timeline of distribution of COVID-19 kits in eight Latin American countries and to analyse whether evidence was used to justify ivermectin distribution.
Methods We conducted a systematic review of randomised controlled trials (RCTs) published on the efficacy of ivermectin or ivermectin as adjuvant therapy on mortality from, or as prevention for, COVID-19. Each RCT was assessed using the Cochrane Grading of Recommendations, Assessment, Development and Evaluations (GRADE). Information on the timing and justification of government decisions was collected through a systematic search of leading newspapers and government press releases.
Results After removing the duplicates and abstracts without full text, 33 RCTs met our inclusion criteria. According to GRADE, the majority had a substantial risk of bias. Many government officials made claims that ivermectin was effective and safe in the prevention or treatment of COVID-19, despite the lack of published evidence.
Conclusion All eight governments distributed COVID-19 kits to their populations despite the absence of high-quality evidence on the efficacy of ivermectin for prevention, hospitalisation and mortality in COVID-19 patients. Lessons learnt from this situation could be used to strengthen government institutions’ capacities to implement evidence-informed public health policies.
- COVID-19
- health systems
- public health
Data availability statement
Data are available in a public, open access repository. No applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
At least eight countries in Latin America started distributions of COVID-19 ‘kits’ containing medicines that were not approved for the treatment of COVID-19 at the time by medicine regulatory authorities in these countries.
There has been little systematic analysis of the quality of clinical evidence that was available to governments when they decided to distribute COVID-19 kits and their justification.
WHAT THIS STUDY ADDS
Even though there was an absence of clinical evidence on the efficacy and safety to prevent hospitalisation, eight countries in Latin America distributed ivermectin as part of COVID-19 ‘kits’ to the population.
Many government officials made claims that ivermectin was effective and safe in the prevention or treatment of COVID-19.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The findings raise important questions about individual countries’ institutional capacities to appraise clinical evidence, as well as concerns about political influence on technical decision-making.
The governments’ claims that ivermectin was effective and safe in the prevention or treatment of COVID-19 may have contributed to the erosion of trust in governments that have characterised the COVID-19 pandemic.
Local or national governments used scarce public funds to purchase ivermectin for the purpose of prevention or treatment of COVID-19 despite a lack of clinical evidence.
Background
In 2020, at least eight countries in Latin America (Bolivia, Brazil, El Salvador, Guatemala, Honduras, Mexico, Panama and Peru) started mass distributions of COVID-19 ‘kits’ to the population either at federal or subnational government health services for the treatment of mild COVID-19 in order to prevent hospitalisations and alleviate the burden of the pandemic on hospitals.1–5 While some countries distributed the kits to households and in the communities, others gave them to those who had tested SARS-CoV2 positive or only with a medical prescription.6–8 Many of the kits contained medicines that were not approved for the treatment of COVID-19 at the time by medicine regulatory authorities in these countries, including ivermectin, azithromycin and hydroxychloroquine.9 Prior to the COVID-19 pandemic, studies reported that some medicines, such as ivermectin, had antiviral and anti-inflammatory properties.10
Ivermectin is widely used as an antiparasitic in humans and animals.11 Common adverse reactions of ivermectin reported in humans include headache, pruritus, muscle pain, cough, dyspnoea, nausea, vomiting, diarrhoea and postural hypotension.12 Rare adverse reactions reported include the complex inflammatory responses called Mazzotti reactions.12 During the first months of the COVID-19 pandemic, ivermectin received particular attention because the results of an in vitro study in April 2020 suggested that it was an inhibitor of SARS-CoV-2.13
This study compares the timeline of the publication of scientific evidence on the efficacy of ivermectin as adjuvant therapy for COVID-19 with the timelines of dissemination of ivermectin in COVID-19 kits in eight Latin American countries and describes the justification from governments for the inclusion of ivermectin in the kits.
Methods
Using PubMed and Google Scholar, we conducted a systematic search of randomised controlled trials (RCTs) on the efficacy of ivermectin or ivermectin as adjuvant therapy for COVID-19 (online supplemental file 1). We included RCTs with outcomes of mortality, treatment, or prevention and publications available as of April 2022. First, we reviewed the RCTs of the meta-analyses and subsequently identified others RCTs that were not included in the meta-analyses. We excluded non-randomised clinical trials, trials only published as a preprint, when only an abstract was published or had a published erratum or when the authors retracted, and when the paper did not include the methodology or the data analyses.
Supplemental material
Evaluation of RCTs
The Cochrane Grading of Recommendations, Assessment, Development and Evaluations (GRADE) was used to determine each RCT’s risk of bias.14 Studies were classified into one of three categories ‘risk of bias’, ‘some concerns’ or ‘low risk of bias’. For RCTs that had been included in the meta-analyses, we compared the risk classification of the trial with our risk classification; when there were discrepancies, we used the more conservative opinion (higher risk of bias). We excluded any studies that were duplicated or had overlapping data to avoid double counting of the studies.
Each RCT was classified according to their study objective and outcome into one of the three categories: (1) whether ivermectin prevents hospitalisation, (2) time to viral clearance and (3) all other clinical questions related to ivermectin. Categories 1 and 2 were considered because they could provide evidence, among other, to justify the dissemination of ivermectin in COVID-19 kits; hospitalisation was considered a relevant outcome because it reflects the severity of COVID-19 illness and is associated with a higher risk of death. Similarly, time to viral clearance can help reduce the time of infectiousness and limit the spread of the virus. We also noted whether studies were only published as a preprint, were retracted or had a published erratum; we also recorded whether the authors reported any funding sources.
Justifications of the government
We analysed the timing and justifications of government decisions to distribute COVID-19 kits with ivermectin in eight Latin American countries (Bolivia, Brazil, El Salvador, Guatemala, Honduras, Mexico, Panama and Peru). Justifications were defined as arguments exposed by national or subnational governmental authorities to explain or justify the use of kits containing ivermectin. We conducted a systematic search in Nexis Uni and targeted web searches via Google of leading newspapers (national and international) and governmental websites; the search was limited to 2020 and 2022 and included documents in English and Spanish and, in the case of Brazil, also in Portuguese with English translation (online supplemental file 2). We identified official government announcements and news reports on the distribution of COVID-19 kits, the start dates of distribution, the contents of the kits (ivermectin only or their combination with other medicines), and the stated justifications for their distribution. We extracted the quotes from government officials that provided a justification for the COVID-19 kit distribution. We also recorded decisions directly related to the distribution of the COVID-19 kits, such as the permission from governments to use ivermectin for the treatment of COVID-19 and the dates when governments declared the discontinuation of the distribution of COVID-19 kits. We excluded the information on kits that did not contain ivermectin. We developed a timeline of the dates of the distribution of kits and the publication dates of the RCTs. Index date for publications that only listed the month and year was the first day of the month.
Supplemental material
Patient and public involvement
Patients were not involved in this study.
Results
We identified 78 RCTs from 5 meta-analyses15–20 and 9 trials not included in the meta-analyses. After removing the duplicates and abstracts without full text, 33 studies were included.
According to GRADE, 25 articles were categorised as ‘risk of bias’, 5 with ‘some concerns’ and 3 had ‘low risk of bias’ (table 1). The quality of evidence available improved over time: whereas in 2020, the majority of studies had ‘risk of bias’, in 2022, the majority were studies with ‘low risk of bias’ (figure 1). Only 9 (27.3%) of the 33 RCTs answered a clinical question related to reducing hospitalisations using ivermectin (table 1). Twelve studies focused on either the outcome of ‘time until viral clearance’ or on ivermectin as adjuvant therapy. The remaining 12 studies focused on clinical questions (such as reduction of in-hospital mortality) that were not relevant to deciding to include ivermectin in COVID-19 kits for mass dissemination.
Assessment of the RCT in relation to the clinical trial outcome of interest and the quality of the evidence presented in the trial publication
{kind=link}
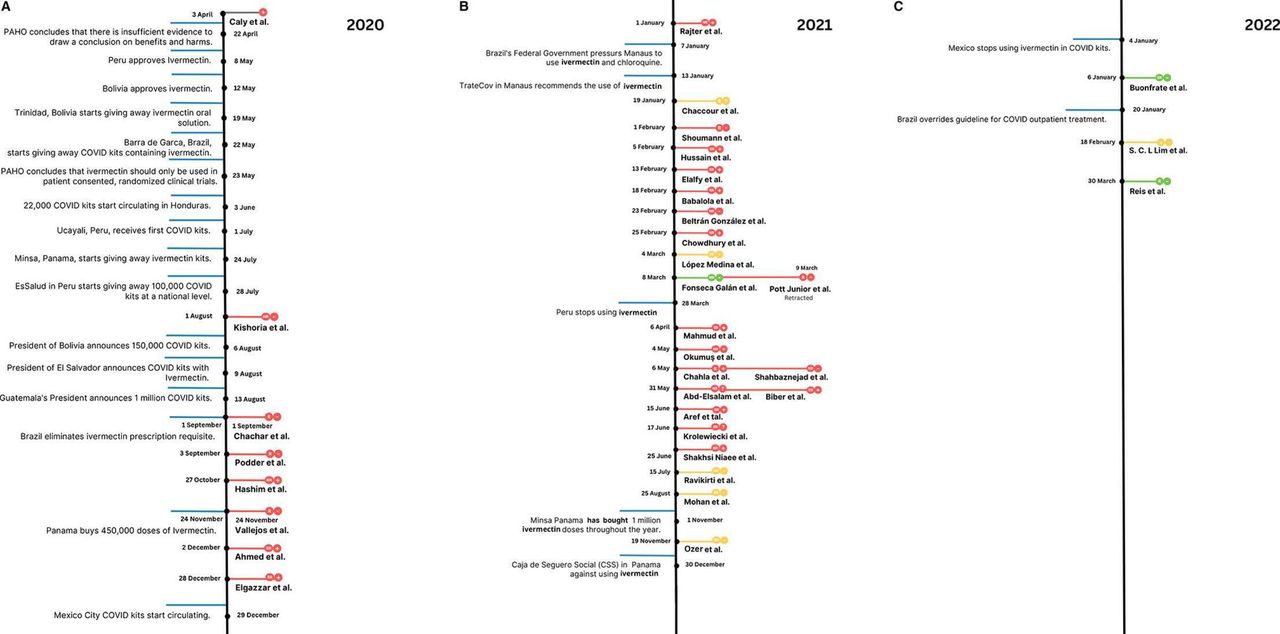
Publication timeline of ivermectin randomised controlled trial and government decisions related to mass distribution of ivermectin. Foot note: blue boxes = government announcements related to the distribution of COVID-19 kits, dates are market in bold (day/month); red boxes = RCT classified as ‘risk of bias’; yellow boxes = RCT classified as ‘some risk of bias’; green boxes = RCT classified as ‘low risk of bias’; grey box = in vitro study; + = RCT reports favorable results of ivermectin; − = RCT reports unfavorable results of ivermectin; ? = RCT reports mixed results of ivermectin. R = RCT study question is relevant to the decision of distribution of COVID-19 kits; NR = RCT study question is not relevant to the decision of distribution of COVID-19 kits; SR = RCT study question somewhat relevant to the decision of the distribution of COVID-19 kits. PAHO, Pan American Health Organization; RCT, randomised controlled trial.
Of the 33 studies included, 27 were published in a peer-reviewed journal, while 6 remained preprints only (online supplemental file 4, column D). Two studies and one meta-analysis were retracted, and one study publication had an erratum (online supplemental file 4, column G). Ten (30%) did not declare their funding sources, and six stated that no funding was used to conduct the study (online supplemental file 4, column E).
Supplemental material
In the eight countries, the COVID-19 kits included ivermectin, seven azithromycin and two hydroxychloroquine, as well as other medicines (online supplemental file 3 provides a list of all the medicines included in the kits apart from ivermectin). Figure 1 shows a timeline of the announcements of the distribution of COVID-19 kits; only the governments of Peru and Bolivia approved the usage of ivermectin for COVID-19 before the kits were announced.21 22 Local authorities in the city of Trinidad, Bolivia, started to give out ivermectin oral solution,23 and the city of Barra do Garca, Mato Grosso, in Brazil, was the first local government to begin to distribute kits.24 In June 2020, Honduras became the first of the eight countries to announce a national distribution of COVID-19 kits; President Juan Orlando Hernández then supervised the distribution of 22 000 COVID-19 kits.8 In July 2020, the city of Ucayali, Peru, received the first COVID-19 kits in that country.25 Three weeks later, EsSalud Clinics (Social Security in Peru) gave away more than 100 000 COVID-19 kits nationwide.26 Panama also started giving out COVID-19 kits during the same time.27 Up to this point—the end of July 2020—no RCT of ivermectin for COVID-19 had been published, and only one in vitro (non-human) study had been published.
Supplemental material
The first RCT of ivermectin was made available online in August 2020; this study was classified as ‘risk of bias’ and had unfavourable results on using ivermectin. Also in August, three of the eight countries (Bolivia, El Salvador, Guatemala) announced mass distributions of COVID-19 kits. Among the three countries, Guatemala’s President, Alejandro Giammattei, promised one million COVID-19 kits.28 In September 2020, Brazil eliminated its prescription requirement for ivermectin.29 Six RCTs on ivermectin were published between September and December, all of which were classified as ‘risk of bias’. Three of these had unfavourable results for ivermectin, and three had favourable results; one of these was later retracted due to suspected fraud. Between 21 December 2020 and 29 December 2020, Mexico City distributed 465 345 COVID-19 kits with ivermectin to individuals with mild to moderate COVID-19 infection.30 Shortly afterward, on 7 January, the federal government in Brazil pressured the local government in Manaus to use ivermectin and chloroquine to treat COVID-19,31 and the app ‘TrateCov’ that supported the health workers in the city, endorsed the use of ivermectin to treat COVID-19.32
In 2021, 23 more RCTs were published. Among them, 18 had ‘risk of bias’, and 4 had ‘some concern’. Only one had ‘low risk of bias’, and it reported unfavourable results of ivermectin. Thirteen reported favourable results, and seven reported unfavourable results (online supplemental file 4, column O). Three studies were inconclusive (online supplemental file 4, column O). Among the studies published between January and April 2022, it is noteworthy that all were either ‘low risk of bias’ or ‘some concern’, and all were unfavourable of ivermectin.
Table 2 presents the justifications for distributing the kits presented by governments. The Honduran President declared that the goal is to prevent hospitalisations. The press note further mentions that analyses show that this treatment (COVID-19 kit) reduces the viral load by more than 90%. On 6 August 2020, Bolivia’s President Jeanine Áñez Chávez claimed that the COVID-19 kits distributed by groups of health workers in the community “[…] administered in a timely manner are very important to prevent the disease from worsening and also to avoid the saturation of hospitals.”33 Only 3 days afterward, in El Salvador, President Nayib Bukele described the medicines, including ivermectin in the COVID-19 kits, as ‘mild medications’, but stated that they could be helpful if taken promptly.6 Four days later, the President of Guatemala, while attending a ceremony showing the kits to the public claimed that COVID-19 kits contained ‘everything necessary’ to treat a patient in the first days of the disease.6 Only Peru’s Health Minister admits that the evidence is low (only an in vitro study had been published at the time); he goes on to explain that, nevertheless, a group of experts decided in favour of its use.21
Government agency, date of announcement and Justification of the COVID-19 kit distribution
With respect to the discontinuation of kit distribution and changing recommendations on the use of ivermectin, in March 2021, Peru was the first of the eight countries to make an official announcement about discontinuing COVID-19 kit distribution.34 In December 2021, Panama’s Caja de Seguro Social stated, ‘We do not recommend the use of ivermectin’.35 Mexico City followed in early 2022.36 As of April 2022, we have not identified any other official announcements of discontinuation of kit distribution or use of ivermectin for COVID-19 in the other five countries.
Discussion
We compared the quality of evidence on the use of ivermectin to treat COVID-19 with the timing of announcements on the mass distribution of ivermectin as part of COVID-19 kits by eight governments in Latin America. We found that all eight governments initially decided to distribute COVID-19 kits to their populations despite the scarcity of high-quality evidence on the efficacy of ivermectin for prevention, hospitalisation, and mortality in COVID-19 patients. In fact, only one RCT (which had ‘risk of bias’) in favour of using ivermectin had been published when seven of the eight governments made their distribution decisions. The eighth, Mexico City, announced the use of ivermectin after seven RCTs had been published; all of those studies presented ‘risk of bias’” only three had reported favourable results, and one was later retracted. Furthermore, the large majority of RCTs published by April 2022 were not directly relevant to the question of whether mass distribution of ivermectin to treat COVID-19 was effective in preventing hospitalisations (which was the stated purpose of distributing kits to the population).
Our findings are highly concerning for several reasons that range from clinical to political. First, in 8 (25%) of the 33 Latin American countries, local or national governments made decisions that exposed hundreds of thousands of individuals to ivermectin for the purpose of prevention or treatment of COVID-19 despite a lack of clinical evidence. Furthermore, at the time of the mass kit distributions, none of these countries’ medicines regulatory authorities had either reviewed or approved applications from manufacturers for market authorisation of ivermectin for the indication of prevention or treatment of COVID-19. There is a large body of bioethics literature on the precautionary principle, which means that a proactive approach is needed to risk mitigation in the face of serious and irreversible threats to human health and the environment amid scientific uncertainty.37 For instance, in relation to the SARS outbreak in Canada in the early 2000s, the Commission to Investigate the Introduction and Spread of SARS in Ontario concluded that the precautionary principle was one of the most important lessons learnt from the outbreak concluding ‘[…]to err on the side of caution when dealing with a little understood new disease’.38 Most importantly, the precautionary principle urges researchers, policy-makers, and the public to make decisions based on the weight and credibility of evidence rather than awaiting elusive scientific certainty.37 In this study, we used GRADE to assess the weight and credibility of evidence available at the time and concluded that the evidence had low credibility and weight to justify the use of ivermectin. Furthermore, at the time the countries made decisions on the use of ivermectin as part of COVID-19 kits, international organisations, including the Pan American Health Organization (PAHO), concluded that ‘there is insufficient evidence to draw a conclusion on benefits and harms. The effectiveness is being evaluated in various randomised clinical trials’39 and ‘the use of medications such as ivermectin, antivirals, and immunomodulators, among others, should be done in the context of patient consented, randomised clinical trials that evaluate their safety and efficacy’.40 Unfortunately, many clinical trials studying the effects of potential treatment of COVID-19 were not randomised, significantly limiting their scientific value41 or, in the worst cases, not adhering to best clinical trial practices.42
Second, despite the low quality of evidence on the efficacy of ivermectin with COVID-19, many government officials, including heads of state, claimed that the COVID-19 kits contained medications that had been shown to be effective and safe for the prevention or treatment of COVID-19. Some mentioned that the medication is ‘mild’ or that ‘there is no reason to fear’ the medicines included in the COVID-19 kits. Several government officials added that the medicines have to be taken ‘in a timely manner’ or ‘taken on time’. The information releases by the Honduran Ministry of Health went even so far as to claim that the kits reduced viral load by 90%. However, the analysis of the scientific publications does not corroborate any of these claims. These public statements and justifications by authorities may have contributed to the erosion of trust in governments that have characterised the COVID-19 pandemic; this lack of trust will likely continue to have long-term effects on the acceptance of other future health interventions.4 43 44 For instance, experts in Brazil have noted that the population lost trust in the federal government due to a series of false and misleading statements about the safety of COVID-19 treatments.45 Re-establishing trust in governments is a complex endeavour. Moreover, in some countries such as Mexico, guidance on the use of medicines included in the COVID-19 kits at the national level contradicted the local level, further undermining the legitimacy of the government guidance. Whereas federal guidelines and declarations of high-rank health officials in Mexico aligned with PAHO recommendations against the use of ivermectin, the government of Mexico City distributed kits with ivermectin against national guidelines.44 The largest hospital network (Mexican Institute of Social Security (IMSS)) included ivermectin in its standard treatment guidelines46 and studied the effects on hospitalisation without the consent of those involved.47
Third, the large scale of COVID-19 kits distribution (in some countries, over a million) represents a waste of the limited resources available for health in general and COVID-19 in particular. For example, Mexico City invested a total of US$1 431 000 in kits,44 Brazil’s government under President Jair Bolsonaro spent more than US$16 million on COVID-19 kits,48 and Guatemala invested US$650 000 in 100 000 kits.6 These resources could have been invested in interventions that have been shown to be effective in preventing the overburdening of hospitals, such as e-health, where patients are monitored via phone calls and text messages at home.49 Similar inefficiencies related to the use of ivermectin occurred in the USA, although this was driven by individual prescribers, not government policy or decision-making.50 Indeed, it is noteworthy that a proposal by some politicians in the US state of Alaska to make it easier to dispense ivermectin was rejected on the advice of medical experts.51
Fourth, it is highly concerning that politicians without medical expertise facilitated and encouraged the population-wide use of an unproven treatment. While the impulse to ‘do something’ is understandable, at the time of the kit distribution, there were neither high-quality RCT results nor guidelines or recommendations from recognised international organisations such as the WHO to support ivermectin use.52 Other governments outside the Americans decided to support their population with the effects of COVID-19 by including tools for symptom relief (such as ibuprofen) and prevention-oriented devices such as masks, as was done in Japan.53 That is, it was possible for governments by the time of the distribution of the COVID-kits in May to make strong and symbolic gestures through mass distributions based on evidence54 without wasting resources and risking harm. Furthermore, this may have prevented other unintended consequences, such as the shortages of those medicines included in the COVID-19 kits that were essential to treat other diseases in which they had proven to be effective (eg, hydroxychloroquine for the treatment of rheumatological conditions).55
Fifth, our findings raise important questions about individual countries’ institutional capacities to appraise clinical evidence, as well as concerns about political influence on technical decision-making. The latter is particularly problematic when it is wielded in the absence of (or in defiance of) technical expertise when there is the potential to achieve political gains. It is noteworthy that, in six of the eight countries we studied, the heads of state—not technical experts such as the heads of public health agencies—announced the kit distributions. Preparing for future pandemics will require strengthening the capacities and public profiles of institutions dedicated to assessing health technologies and making recommendations about appropriate use.
We recognise that this study had limitations. We do not know whether policy-makers had access to other evidence that was not in the public domain. However, it could be argued that governments should be transparent about the scientific evidence that informs policy decision-making. Furthermore, this analysis did not examine the quality of scientific evidence available at the time of the decision regarding other medicines that the kit contained. However, international organisations, such as the PAHO, did recommend against the use of some of these medicines (eg, hydroxychloroquine) early on in the pandemic when decisions about the distribution of COVID-19 kits were made in the region.56 This study also focused only on correlating the timelines of scientific publications with public announcements of policy decisions. Answering more detailed questions about why and how countries made decisions to provide ivermectin in the absence of publicly available evidence was not within the scope of this initial study. It would be expected that countries take into consideration a variety of information sources to make their decision on the distribution of COVID-19 kits. It can be reasonably argued that governments should take into consideration, among other factors, information from RCTs on the efficacy of ivermectin in preventing hospitalisations. More qualitative policy research is needed to examine how the decisions were made in individual countries. Furthermore, comparative studies would provide important insights about why some Latin American countries did not disseminate either ivermectin or kits more generally.
Despite the limitations, however, this study shows that in the absence of clinical evidence on the efficacy and safety to prevent hospitalisation eight countries in Latin America decided to distribute ivermectin. It also raises many important questions about different approaches to governmental decision-making when there is insufficient evidence and significant social pressures to act.
Data availability statement
Data are available in a public, open access repository. No applicable.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @verowirtz
Contributors VJW conceptualised the study; JAR collected the data; VJW, DM-L and JAR analysed the data; VJW and JAR drafted the manuscript; JAR, DM-L and VJW all revised the manuscript. VJW is the author responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.