Article Text

Statistics from Altmetric.com
Summary box
COVID-19 pandemic has highlighted the need for improved global governance and investment in resilient public health systems.
Effective public health is not the exclusive preserve of any one professional group but requires multisectoral and interdisciplinary collaboration across a broad range of occupations.
WHO and partner organisations have published a roadmap; a five-year strategy to strengthen capacity across all countries for a multidisciplinary workforce to undertake the essential public health functions, including emergency preparedness and response.
A key action area within the roadmap is the use of competency-based education as an approach to developing the skills and abilities of diverse multidisciplinary teams, with the collective capability to deliver on the essential public health functions.
Inclusion of early career professionals in decisions about education and health policy will encourage intergenerational collaboration, bidirectional learning and serves to ensure that the future workforce has agency and is well equipped to deal with evolving health system challenges.
Background
More than two years on from WHO’s declaration of a pandemic, COVID-19 continues to expose the weaknesses in health systems and public health responses worldwide. It has highlighted the need for improved global health governance and for investment in more resilient public health systems.
As the world recovers from the multisectoral impact of the pandemic, the inter-relationship between health and its social, environmental, political and economic determinants has never been more apparent. Public health requires collaboration with a diverse group of professions across health and allied sectors. While sound public health leadership can unify and guide health protection and improvement, effective public health is not the exclusive preserve of any one professional group. Multisectoral and interdisciplinary collaboration1 and core public health competencies are required to address the wider determinants of health and promote effective health systems.2
Experience from current and previous pandemics, and other global health threats has demonstrated the need for responsive, coordinated,3 established and trusted4 public health expertise at local, national and international levels. Global health threats such as non-communicable diseases, climate change, environmental degradation, increasing population density, conflict and mass-enforced migration, require coordinated professional public health action.1 Attaining universal health coverage (UHC) and ensuring health security are complementary and interrelated goals that will only be achieved with proper investment in the essential public health functions (EPHFs), including emergency preparedness and response.5 However, the key role of the workforce in achieving these outcomes is often overlooked, as are other critical health systems building blocks, such as supply chains, access to essential health services and health information systems.6 In May 2022, the WHO, working with the International Association of National Public Health Institutions (IANPHI), Association of Public Health Schools in the European Region (ASPHER), Association of Public Health Schools in Africa (ASPHA) and other leading public health networks, launched a roadmap for scoping, defining and building the capacity of the public health and emergency workforce to deliver the EPHFs.
EPHFs and public health workforce
EPHFs, defined and published by WHO in 1998, have long been regarded as the indispensable set of actions that are fundamental for achieving the goals of public health.7 Several WHO regional offices and other global and regional actors have undertaken work programmes to further define EPHFs,8 adapting them to reflect different geographical contexts. In 2016, resolution WHA69.1 of the 69th World Health Assembly stated that delivery of the EPHFs would be the most cost-effective and sustainable way to enhance the health of populations and achieve UHC.9
The public health workforce has been defined as including both those whose primary responsibility is the direct provision of core public health activities and those whose public health activities indirectly contribute to the improvement of population health.7 The public health workforce therefore includes professionals with diverse backgrounds, skillsets and competencies, whose work contributes to the delivery of one or more of EPHFs, but whose collective contribution is essential to deliver the full set of EPHFs. This heterogeneous workforce can be broadly categorised into three groups: (1) core group of public health personnel who have undergone professional training covering all the EPHFs; (2) health and care workers who contribute to one or more public health functions as part of their roles and (3) people from a wide group of other allied occupations who contribute to addressing the determinants of health.10 There is widespread variation across countries regarding which groups of individuals and associated occupations are involved in the delivery of the EPHFs.6 This has proven to be challenging as there is a resultant lack of uniformity in assessment and maintenance of the competencies of the public health workforce across different contexts.6
Competency-based education
Competence is a multidimensional and dynamic quality,11 which can be defined as the capability to perform work activities to a required standard and having the requisite skill to do this within a given context.12 Competency-based education (CBE) centres on outcomes-based learning within workplace-like conditions and is increasingly replacing more traditional training styles which focused on simple knowledge transfer or ‘time-in-seat’,11 rather than a mastery of real-world application of these principles.13 CBE has become the main approach to postgraduate medical education in some countries14 and is specifically geared towards exhibiting proficiency in given skill sets.13 While each training programme and design has its challenges, the value of an outcomes-based assessment is that it highlights an individual’s demonstrable ability to understand and action duties necessary for practice in their chosen field.11 Within the context of health, CBE and training has the potential to improve health outcomes of communities but only insofar as the contextual challenges facing health systems are considered in determining the desired competencies.15
Competency frameworks for the public health workforce are helpful to structure education programmes and ensure that the workforce gains the abilities needed to deliver EPHFs. By focusing on required skillsets rather than specific occupations, diverse professional groupings can be recognised for their contributions to the delivery of these functions. There have been several efforts on a national and regional scale to develop competency frameworks for the public health workforce. Examples include efforts undertaken by the UK,16 Canada,17 India,18 New Zealand19 China,20 WHO Regional Office for Africa21 and Europe.2
Increasingly, regional and national agencies are working across boundaries to share learning on the development of public health competency frameworks. For example, ASPHER and European higher education institution partners have established a joint project with Israel to share best practices from Europe as part of Israel’s effort to improve their public health education and workforce development.22 Similarly, there is work ongoing by ASPHA to contextualise and adapt the European competency framework to their setting.23 There is now an obvious need to consolidate and build on these existing resources so that there is a consistent yet contextually sensitive approach towards capacity building across all countries.
The ‘roadmap’
To address the challenges facing health system resilience and workforce capacity, leading organisations across the globe have co-developed a roadmap for building the public health and emergency response workforce. This initiative highlights the importance of CBE and training which has been demonstrated to be effective in improving clinical outcomes.24 The aim of the roadmap is to mobilise national, regional and global leadership to take coordinated action towards a strengthened workforce in every country, delivering all the EPHFs. It also serves to encourage academic institutions and policy makers to include young professionals in the development of these competencies and workforce strategies.
The ‘Building a Public Health Workforce: A Roadmap’ document was developed in two stages. The first stage involved an expert consultation session held virtually in January 2022 and was co-hosted by ASPHA, ASPHER, IANPHI and WHO. This expert consultation involved participants from a range of leading public health and emergency response organisations and representation from all WHO regional offices.6
The second stage of the roadmap development involved the establishment of a technical working group (TWG) with diverse membership, including early career professionals (ECPs).6 Membership of the TWG included representation from the Global Outbreak Alert and Response Network, Global Network for Academic Public Health, UK Faculty of Public Health, College of Public Health Medicine of the Colleges of Medicine of South Africa, Training Programmes in Epidemiology and Public Health Interventions Network, UK Health Security Agency, IANPHI and WHO. The TWG met twice between April and May 2022 during which they developed and finalised the roadmap. The roadmap was launched on 18 May 2022.
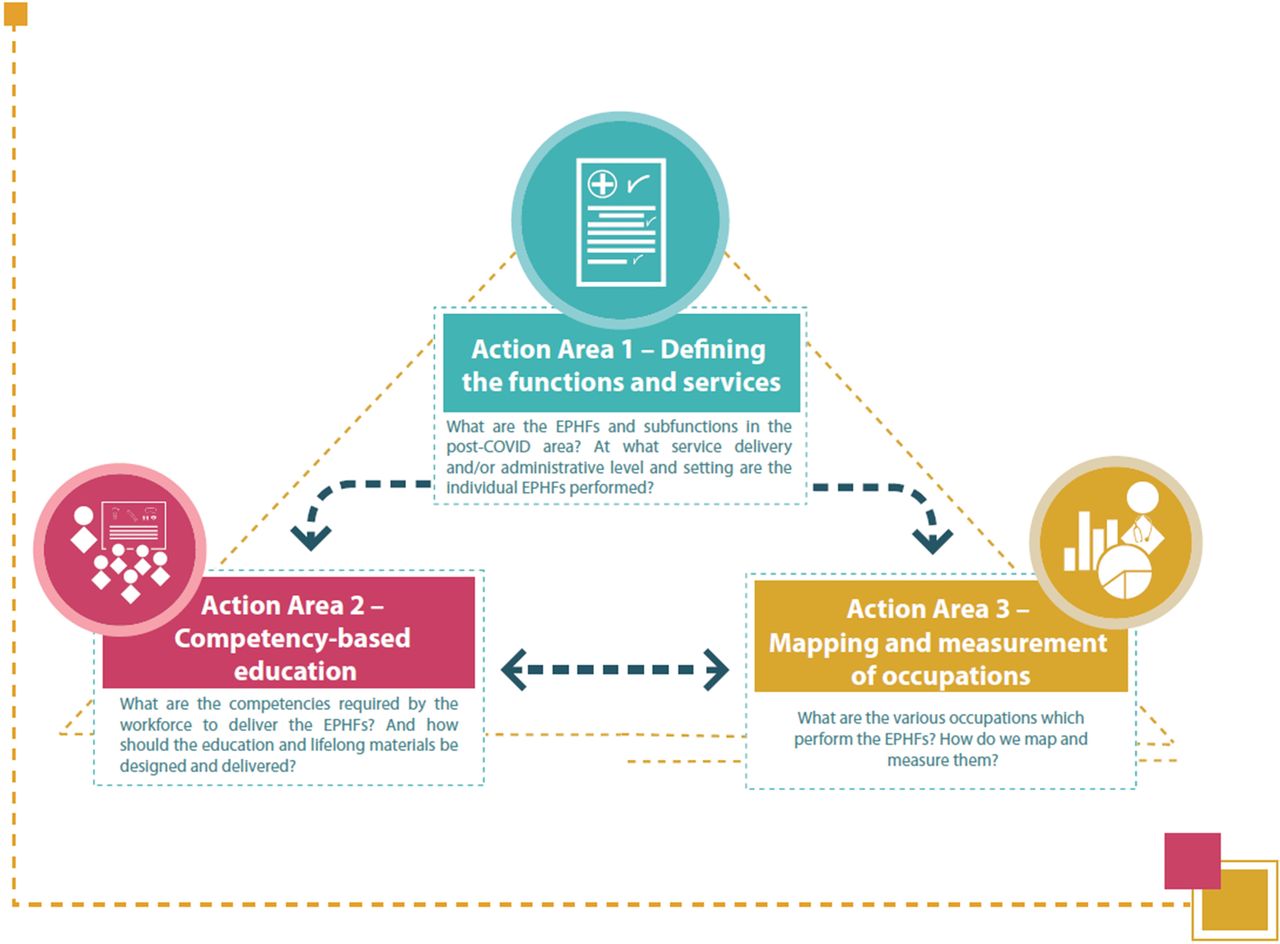
The roadmap proposes a conceptual approach for scoping, defining and building capacity of the public health workforce. It focuses on three, interconnected action areas (figure 1)6: (1) defining the EPHFs and the services associated with them; (2) strengthening CBE as an approach to developing the skills and abilities of the public health workforce to action the EPHFs and (3) mapping and measurement of occupations involved in the delivery of the EPHFs.

{kind=link}
Conceptual approach to scoping, defining and building capacity of the public health workforce.6
The third action area (figure 1) provides an opportunity for each country to identify improvements in the current workforce through a mapping and measurement framework that will allow for countries to monitor the profile and size of their workforce as well as allow for cross-country comparability.6
Involvement of ECPs
The roadmap sets out an ambitious agenda for countries to build a strengthened workforce. For these aspirational aims to be realised, the roadmap requires the support of a broad coalition of partners and stakeholders with diverse expertise. Inclusion of young professionals in decisions about education and training will enable these future leaders to engage in policy developments and inform public health structures that will shape their careers and the future of health service delivery. The unique position of students and ECPs within complex health systems affords them an appropriate vantage point from which to engage in curriculum and social wellness debates.25 It is important that the career stage of individuals is not erroneously linked to their level of competence.
It is also important to emphasise that it is not simply about allowing ECPs the platform to communicate opinions but providing them with the power to use that platform to effect meaningful change. As such, the active roles that ECPs have been given in the development and implementation of this roadmap, is to be celebrated.26 This practice will ensure that ECPs have improved agency and ownership of designing solutions to address public health workforce challenges going forward.25
Countries are encouraged to actively involve their networks of students and ECPs as they aim to use the roadmap and progress on a journey to full implementation in each action area.
Conclusion
The public health workforce, in its broadest sense, is the cornerstone in the development and maintenance of resilient and effective public health systems. In keeping with its historical roots, modern public health respects the sanctity of human life through promoting health and preventing disease.27 Understanding the inter-related nature of health with societal and economic influences is paramount in realising the shared goals of UHC and health security. Population health is everyone’s responsibility, but the case for investing in a dedicated public health profession able to lead and shape public health systems and services is now more urgent than ever.28
The ambition set out in the roadmap is to be welcomed. Having a framework to inform the development and upskilling of a diverse workforce through CBE and training will contribute to the strengthening of a workforce dedicated to improving quality of life on a global scale. The roadmap developed by the WHO and partner organisations serves to provide guidance to countries, enabling them to implement actions and activities aimed at developing public health workforce to serve the unique needs of their individual contexts. By aligning these actions to common tasks (delivering the EPHFs) that are relevant across geographical boundaries, and by strengthening competencies and skills, a trusted, effective and globally recognised workforce will be formed. The immediate activities and deliverables anticipated in the first two-year period of the roadmap have been set out in an Action Plan.29
The operationalisation of the roadmap requires the collective collaboration and action from governments, funders, technical partners, academic institutions, national public health institutes and civil society organisations.6 It also requires strong public health leadership, supported by a core, professionalised group of public health personnel to help unify and guide activities. However, professionalisation of the public health workforce, to match the professional standards of other health workers, has been a gap in many countries and is only now starting to be addressed. ASPHER recently launched a roadmap for the professionalisation of the public health workforce; this experience and recent developments in other regions could help shape global commitment to professionalise public health.
As well as inclusion of a broad range of formal and informal professional groups, it remains important to continue to engage ECPs in the implementation of the roadmap, as they can provide diverse perspectives,30 enhance sustainability of public health initiatives and ensure that the future workforce is well prepared to deal with rapidly evolving health system pressures.
Data availability statement
There are no data in this work.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to acknowledge the WHO Roadmap For Public Health and Emergency Workforce Working Groups and overarching Roadmap Steering Committee.
Footnotes
Handling editor Seye Abimbola
Twitter @O_LaFatai
Contributors MBH, FO, JM and NS developed the initial concept of the manuscript. MBH and FO produced the initial draft of the manuscript. All authors revised the manuscript and approved the final version. All authors are the guarantors. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.