Article Text

Abstract
Background The number of children in sexual minority parent families has increased. This systematic review aims to synthesise the evidence of disparities in family outcomes between sexual minority and heterosexual families and to identify specific social risk factors of poor family outcomes.
Methods We systematically searched PubMed, the Web of Science, Embase, the Cochrane Library and APA PsycNet for original studies that compared family outcomes between sexual minority and heterosexual families. Two reviewers independently selected studies and assessed the risk of bias of included studies. Narrative synthesis and meta-analysis were conducted to synthesise evidence.
Results Thirty-four articles were included. The narrative synthesis results revealed several significant findings for children’s gender role behaviour and gender identity/sexual orientation outcomes. Overall, 16 of 34 studies were included in the meta-analyses. The quantitative synthesis results suggested that sexual minority families may perform better in children’s psychological adjustment and parent–child relationship than heterosexual families (standardised mean difference (SMD) −0.13, 95% CI −0.20 to −0.05; SMD 0.13, 95% CI 0.06 to 0.20), but not couple relationship satisfaction (SMD 0.26, 95% CI −0.13 to 0.64), parental mental health (SMD 0.00, 95% CI −0.16 to 0.16), parenting stress (SMD 0.01, 95% CI −0.20 to 0.22) or family functioning (SMD 0.18, 95% CI −0.11 to 0.46).
Conclusion Most of the family outcomes are similar between sexual minority and heterosexual families, and sexual minority families have even better outcomes in some domains. Relevant social risk factors of poor family outcomes included stigma and discrimination, poor social support and marital status, etc. The next step is to integrate multiple aspects of support and multilevel interventions to reduce the adverse effects on family outcomes with a long-term goal of influencing policy and law making for better services to individuals, families, communities and schools.
- child health
- public health
- systematic review
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The number of children in families with parents who are sexual minorities has increased.
Despite improvements in public attitudes towards sexual minorities nowadays, sexual minority parenting does remain a controversial topic around the world.
WHAT THIS STUDY ADDS
In countries and regions where same-sex relationships are legalised, most of the family outcomes are similar between sexual minority and heterosexual families, and sexual minority families have even better outcomes in some domains.
Sexual minority families may experience some additional stressors related to their sexual minority status. Community context and climate have an impact on the health and well-being of sexual minority parents and their children. We summarised social risk factors of poor family outcomes and would like to offer suggestions for researchers, policy-makers and practitioners.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Parents’ sexual orientation is not an important determinant of children’s development. We advocate among policy-makers, communities, schools, families and individuals for better awareness of family outcomes of sexual minorities.
More research is needed to learn more about how communities around the world can support positive development among all children of sexual minority parents and how legal and policy contexts affect their lives and their children.
Introduction
Sexual and gender minorities is an umbrella term including lesbian, gay, bisexual, transgender, queer, intersex, gender non-conforming people and other populations whose sexual orientation or gender identity and reproductive development is considered outside cultural, societal or physiological norms.1–3 Compared with the heterosexual population, sexual and gender minorities have an increased risk for health problems.4–6 In recent years, the number of children in families with parents who are lesbian, gay, bisexual, transgender and queer has increased.7–9 A report in 2018 showed that, in the USA, same-sex couples are seven times more likely than different-sex couples to be raising an adopted or foster child, and there are an estimated 114 000 same-sex couples raising children.9 Despite recent improvements in public attitudes towards sexual minority families, sexual minority parenting is still a controversial topic around the world, and the outcomes of sexual minority families remain not fully understood.10 11
Since the 1980s, many countries have started to expand marriage rights to sexual minority couples in the areas of relationship recognition, tax insurance and child adoption.12 In 1989, Denmark was the first country in the world to introduce a law allowing same-sex partnership registration.12 The legal recognition of same-sex relationships (eg, registered partnerships or civil unions) is a critical step forward in advancing equal marriage rights for sexual and gender minorities.13 14 As of December 2021, around the globe over 40 countries and territories allow sexual minority couples to marry. Once national laws and public policies of equal marriage rights for sexual minority couples are settled, the law can ultimately establish necessary conditions for children to be conceived, born and raised; and thus for children to thrive in an optimal environment.15
Given the social, cultural, political and legal divide on the topic of the sexual minority family, debate persists about whether parental sexual orientation affects family outcomes. Evidence from a previous qualitative review suggested that children raised by lesbian and gay parents do not experience adverse outcomes (eg, emotional functioning, stigmatisation) compared with other children.16 A quantitative review indicated that children of gay parents had significantly better outcomes than did children of heterosexual parents on some psychological adjustment domains.17 However, some studies have shown contradictory findings that children from sexual minority parent families may have worse developmental outcomes than children from heterosexual families in some domains, such as children’s health, education or marijuana use.18–20 The sexual minority stress theory suggests that sexual minorities often experience chronic psychosocial stress.21 In recent years, there has been greater attention to sexual minority parents and their children. Numerous studies have compared family outcomes between sexual minority and heterosexual parent households. Based on this body of literature, we included a comparison group of heterosexual parent households in this review.
Thus far, little is systematically known about the disparities in family outcomes between sexual minority and heterosexual families after the legal recognition of same-sex relationships. Further understanding of the disparities in multiple measures of outcomes may inform general debates and policy interventions in family structure and child health. This systematic review aims to compare the disparities between sexual minority and heterosexual parent families in the following major family outcomes: children, parent, household-level outcomes. We also discuss social risk factors of poor family outcomes and offer some suggestions for improving family outcomes.
Methods
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.22
Search strategy
We searched PubMed, the Web of Science, Embase, the Cochrane Library and APA PsycNet for eligible articles published in any language from 1 January 1989 to 1 April 2022. The detailed search strategies are available in online supplemental appendix S1. We also manually examined reference lists of reviews, original studies and related systematic reviews to identify additional publications that we may have missed in our electronic search.
Supplemental material
Eligibility criteria
To meet the inclusion criteria, articles had to: (1) be conducted in the country after the legal recognition of same-sex relationships; (2) be primary studies using qualitative, quantitative or mixed methods; (3) compare the differences between sexual minority and heterosexual parents, and/or their children; and (4) data that have been used once in a manuscript to avoid replication. In addition, all articles were based on the time of recognition of the first type of law, regardless of the type of law. Exclusion criteria included: (1) grey literature (eg, meeting abstracts, dissertations, theses); (2) literature review or purely theoretical discussion paper; (3) a policy statement/agenda; (4) a comment or letter; or (5) lack of data on parenting for sexual and gender minorities. In the USA, some states began to recognise same-sex relationships from 2000. Therefore, for studies conducted in the USA, we included studies conducted after 2000.
Study selection and data extraction
We first exported titles and abstracts identified through the database searches to EndNote and removed duplicates. Two investigators (YZ and MW) independently assessed the titles and abstracts of all identified articles. Then, we obtained and examined the full text of the potential articles and, if necessary, discussed the content with a third review author (MH) to decide whether or not to include articles thought to be contentious. After the study selection process, two reviewers (YZ and MW) independently extracted data from the included studies using a predesigned standardised Excel form with the following information: first author, publication year, location, sample size, age, study design, meta-analysis (yes/no), outcome measures, who reported the data and main finding.
Quality assessment
We assessed the quality of each extracted article using the Joanna Briggs Institute Checklist for Analytical Cross-Sectional Studies, Cohort Studies or Qualitative Research Critical Appraisal Tool.23 Two reviewers (YZ and MH) independently assessed risk of bias using percentage scores following Ancheta’s report.24 Low quality of a study was considered if the score percentage was 49% or lower, moderate if the score percentage was 50%–69% and high if the score was 70% or higher. Detailed information about the quality of included articles is listed in online supplemental appendix S2.
Assessment of heterogeneity and publication bias
To assess the heterogeneity of studies in meta-analysis, we applied principles from both Cochran’s Q test and Higgins I2 test. P-value of Cochran’s Q test less than 0.05 considered problematically high heterogeneity. Moderate heterogeneity was considered if I2 was 30%–50%, and high if I² exceeded 50%. Random effects model (p<0.05, I2≥50%) would be used for the data were high heterogeneity, otherwise, a fixed effects model (p>0.05, I2<50%) would be selected. Sensitivity analysis was also conducted if there was problematic heterogeneity. Publication bias was assessed by inspecting funnel plots analysis. If the Egger’s test has p>0.05, it means no evidence of publication bias; otherwise, there would be a publication bias.
Outcome measures
A thematic analysis of the literature was conducted to identify outcomes. Two researchers separately coded the outcome measures from each study. The two coding results were compared and discussed. After resolving the discrepancies, outcomes were categorised into the following three main domains with 11 themes: children’s developmental outcomes (children’s psychological adjustment, physical health, gender role behaviour, gender identity/sexual orientation and education outcomes), parents’ psychological adjustment (parental mental health, parenting stress) and household-level outcomes (parent–child relationship, couple relationship satisfaction, family functioning, social support, etc). A detailed definition and explanation of each outcome were listed in online supplemental appendix S3.
Statistical analysis
Most of the outcomes in this review were continuous, so we selected standardised mean difference (SMD) and 95% CI as the effect size for reporting the results of meta-analysis. Given that the scoring standards of measurement tools used in different studies are inconsistent, for the scale scores with inconsistent evaluation criteria, we reversed scoring to make the scale in the same direction (online supplemental appendix S4). If the outcomes were measured at a different time point, the terminal follow-up visits were chosen to compare the differences in outcomes between two family types. A fixed effects or random effects model was selected according to the deviance information criterion. We set the significance level at 0.05 for pooled estimation results and built forest plots for each outcome using R V.4.0.4, including three R packages: meta, metafor and dmetar. For the quantitative studies and qualitative studies that could not be included in meta-analysis, we used narrative synthesis to aggregate, integrate and interpret the results. We provided the data of outcome for the main findings in table 1.
Included study characteristics
Patient and public involvement
Patients or members of the public were not directly involved in this research study.
Results
The search identified 1194 articles plus 35 articles through other sources, of which 1058 articles remained after duplicates were removed. Moreover, 913 articles were considered irrelevant and further excluded after title and abstract screening, which left 145 eligible articles for full-text screening. After further excluding 111 articles for various reasons, 34 articles remained for analysis in this review (figure 1), of which, 18 were included for narrative synthesis and 16 for meta-analyses.

Flow chart of the study selection procedure.
Study characteristics
Table 1 displays the characteristics of studies included in the current systematic review and meta-analysis. Data and outcome measures of each study included in meta-analyses are listed in online supplemental appendix S4. Most studies (n=22) were conducted in the US, two were conducted in Australia and Canada, respectively; whereas the remaining studies (n=10) were conducted in Europe. Among the 34 studies, seven were cohort studies, 22 were cross-sectional studies, and three were qualitative studies. Three qualitative studies all used thematic analysis for data analysis. One research article was on gay parent families only, and three research articles were on lesbian parent families only. Twenty-eight research articles were on both gay and lesbian parent families. One research article was on lesbian, gay and bisexual parent families; and one was on lesbian, gay, bisexual, transgender, and queer parents. Our analysis included four articles at moderate risk of bias and 30 articles at low risk of bias. No studies were considered at severe risk of bias. Risk of bias was mainly related to confounding factors, or non-objective measures of exposure factors (online supplemental appendix S2). The included 34 studies were categorised into the following three areas including 11 main themes: children’s developmental outcomes (17 for children’s psychological adjustment,18 20 25–39 five for children’s physical health,19 20 37 38 40 four for children’s gender role behaviour,26 35 41 42 three for children’s gender identity/sexual orientation,20 29 41 six for children’s educational outcomes,20 33 43–46 parents’ psychological adjustment (six for parental mental health,18 27 35 36 47 48 five for parenting stress,32 35 40 48 49 household-level outcomes (six for parent–child relationship,30 35 36 40 47 50 six for couple relationship satisfaction,26 28 31 40 48 51 four for family functioning,25 26 28 49 three for social support,32 52 53 and five outcomes that cannot be grouped into themes (preschool selection considerations,54 parental school involvement,55 parent-school relationships,27 parental self-agency,28 and child’s substance use.30 The outcome measures in table 1 were listed in the order of the above themes.
Children’s psychological adjustment
We identified 17 studies in this search with regard to children’s psychological adjustment, among them, five articles were included in narrative synthesis. Three studies reported that children of sexual minority parents were as likely as children of heterosexual parents to grow up healthy and well adjusted.34 37 38 Two studies reported more emotional problems for children with sexual minority parents than for children with heterosexual parents20 39 (table 1).
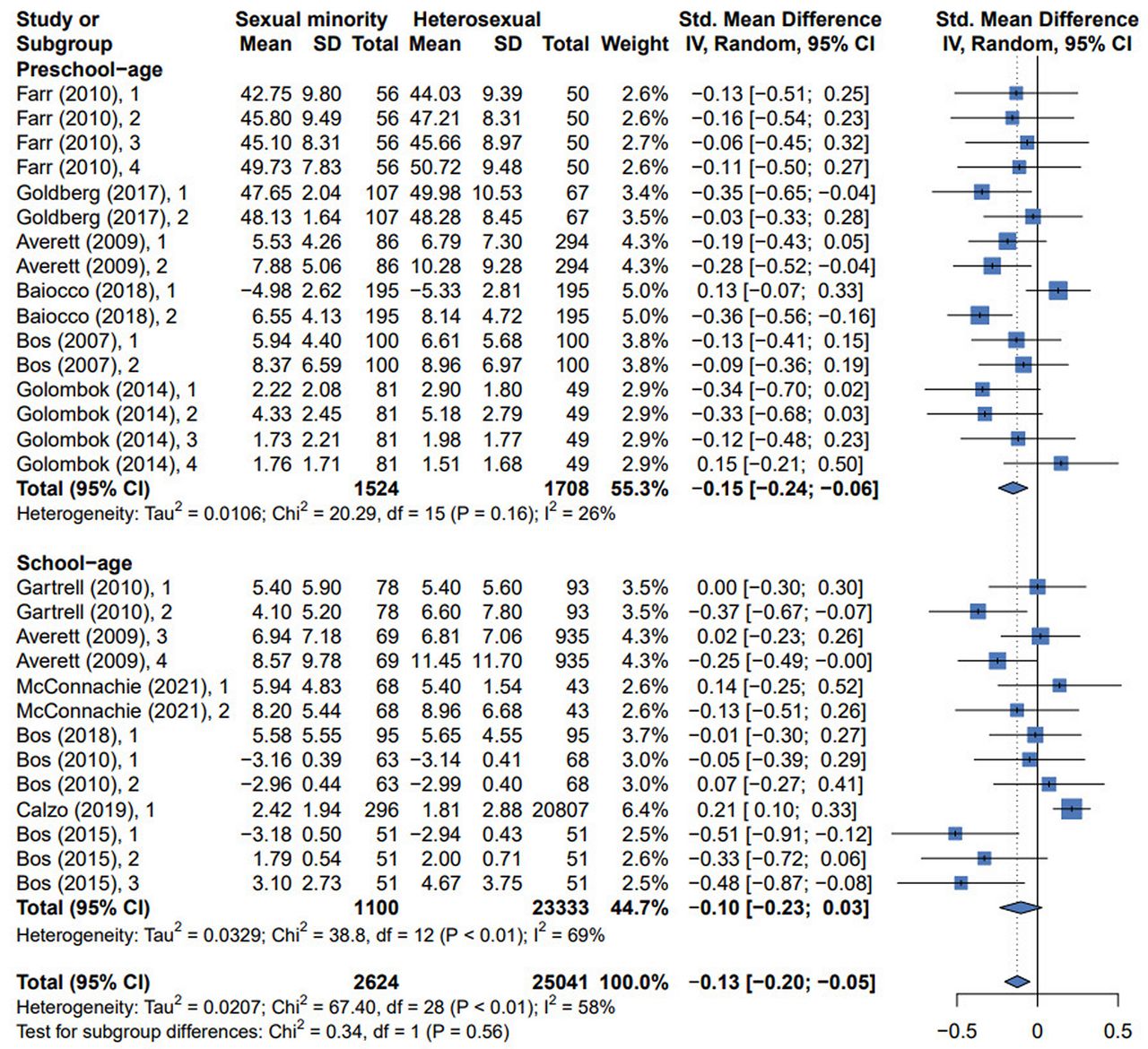
Among the 17 studies, 12 were selected for meta-analysis.18 25–33 35 36 The overall effect size for children’s psychological adjustment was statistically significant (SMD −0.13, 95% CI [95% CI] −0.20 to −0.05) (figure 2). Sensitivity analysis showed the overall effect size was not influenced by removing single effect size (online supplemental appendix S5A). Egger’s regression test showed there was a publication bias (p<0.05) (online supplemental appendix S7A). This result indicates that children raised by sexual minority parents were found to adjust better on some psychological domains than children raised by the different-sex parents.
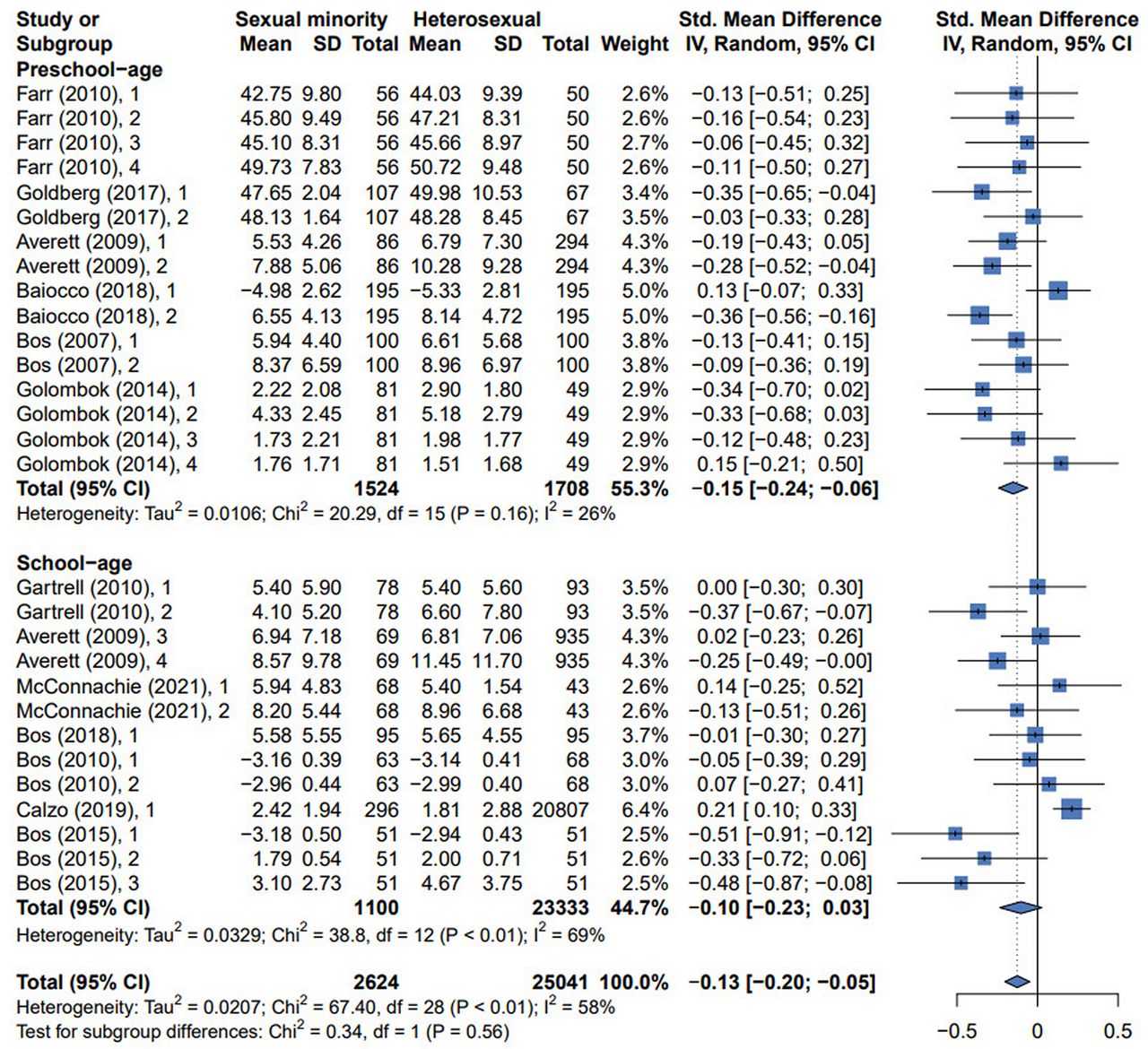
The forest plots for children’s psychological adjustment.
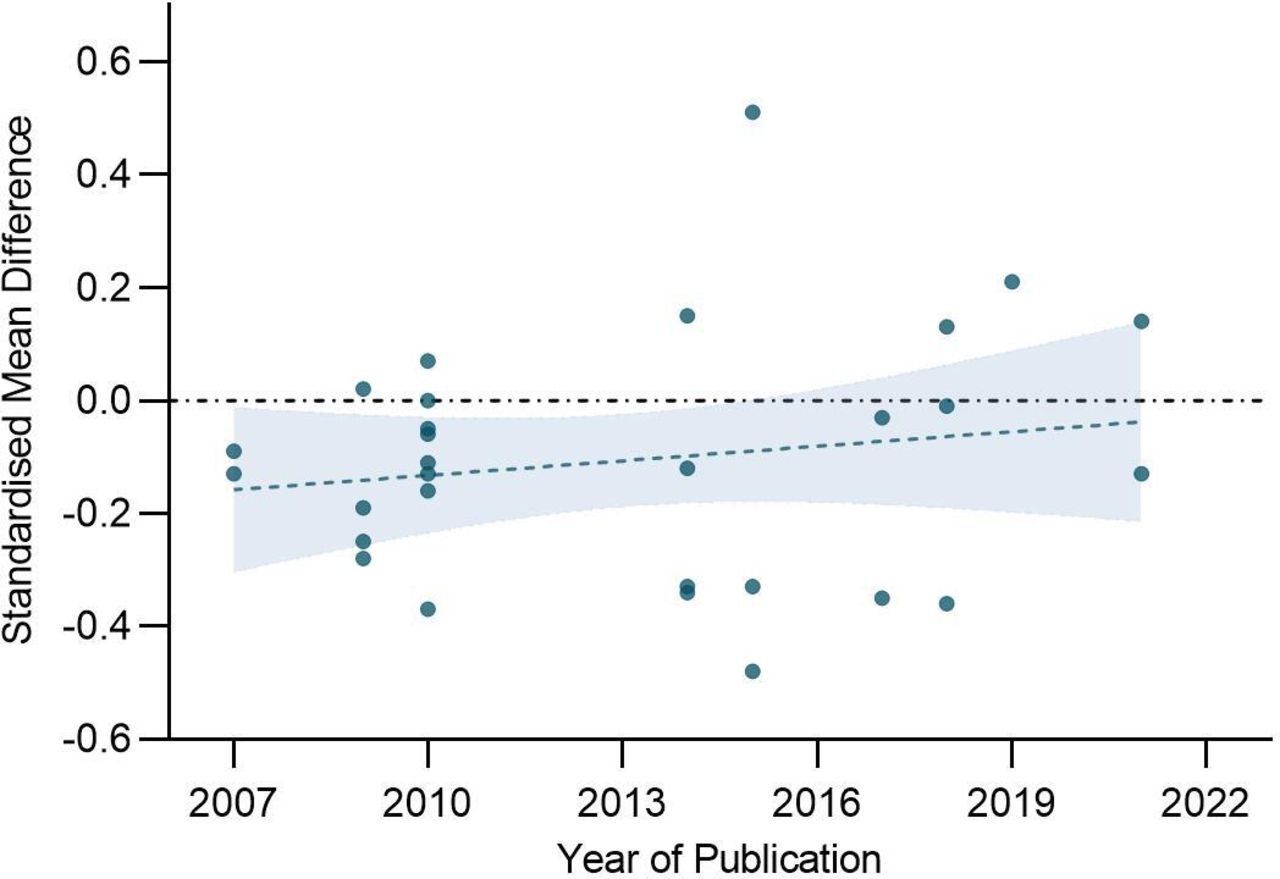
Further, we stratified studies by age of children (school-age vs preschool-age), pathway to parenthood (adopted vs biological), outcome measure type (internalising vs externalising), country (USA vs the Netherlands vs UK vs Italy), geographical region (continent) (online supplemental appendix S6). In the preschool-age group (≤ 6 years), the results indicated that sexual minority parents reported significantly fewer psychological problems of children than heterosexual parents (SMD −0.15, 95% CI −0.24 to −0.06). In the school-age group (> 6 years), no differences were found between children with sexual minority parents and children with heterosexual parents (SMD −0.10, 95% CI −0.23 to 0.03). This suggests the age of the children may be a factor affecting the pooled effect size. The effect size was significant for both the adopted subgroup and biological subgroup (SMD −0.15, 95% CI −0.23 to −0.07; SMD −0.16, 95% CI −0.28 to −0.03). In addition, subgroup analysis results showed that heterosexual parents reported significantly more internalising and externalising problems among their children than reported by sexual minority parents (SMD −0.12, 95% CI −0.21 to −0.03; SMD −0.23, 95% CI −0.32 to −0.13). When subgroup analysis was performed by country, sexual minority parents reported significantly fewer psychological problems than heterosexual parents in the Netherlands (SMD −0.16, 95% CI −0.29 to −0.03). The results of subgroup analysis by region showed that, in Europe, there is a statistically significant effect size (SMD −0.14, 95% CI −0.24 to −0.03); in the Americas, the effect size was not statistically significant (SMD −0.11, 95% CI −0.23 to −0.00). Finally, we analysed the change of difference between children in sexual minority families and children in heterosexual families in children’s psychological adjustment over time (the year of publication). As shown in figure 3, there was a decreasing trend in the difference between the two groups over time.

The change of difference between children in sexual minority families and children in heterosexual families in children’s psychological adjustment over time.
Children’s physical health
Five studies on children’s physical health were included in narrative synthesis.19 20 37 38 40 Three articles reported that children in sexual minority parent and heterosexual households are similar on physical health outcomes.37 38 40 Children in cohabiting households have poorer health outcomes than children in married households.19 37 Regnerus’s study showed that the children of lesbian parents report worse physical health,20 but it is worth noting that the result should be taken with caution because its definition of ‘child with same-sex parents’ is controversial.17 37 39
Children’s gender role behaviour
Four articles reported children’s gender role behaviour,26 35 41 42 all of which were included in narrative synthesis. Two articles show there were no significant differences among children in different family type in gender role behaviour.26 35 In Goldberg’s research, sons in lesbian parent families were less masculine than sons in gay and heterosexual parent families; but there were no significant differences across family type for girls’ behaviour at each time point.42 In addition, sons of GMM (gay-male parents both described as masculine) are similarly masculine as sons of heterosexual parents. The son of the GFF (gay-male parents both described as feminine) was perceived as less masculine than the sons of the other parent descriptions.41
Children’s gender identity/sexual orientation
All three studies show that children’s gender identity/sexual orientation may vary by family type.20 29 41 These studies found that compared with the children who lived in heterosexual parent families, the children who lived in sexual minority parent families had a lower expected likelihood of developing as heterosexual.20 29 41 The detailed results were shown in table 1.
Children’s educational outcomes
We conducted a narrative synthesis of six studies on children’s educational outcomes.20 33 43–46 Four studies indicated that children from same-sex couples appear to have the higher rate of grade retention, lower graduation rate or worse educational attainment than children from different-sex couples.20 43 44 46 On the contrary, two studies reported that children in sexual minority parent families outperform children in heterosexual parent families on standardised test scores, high school graduation rates, college enrolment, and school/academic competence.33 45
Parents’ psychological adjustment
Parental mental health (anxiety, depression and distress) and parenting stress were included in this topic. For parental mental health, bisexual individuals in general experience greater levels of psychological distress than lesbian or gay and heterosexual individuals.18 When comparing gay or lesbian vs heterosexual parents, the result did not reveal appreciable differences in distress levels.18 As for quantitative synthesis results (figure 4A), the results of six studies on parental mental health showed no significant differences between family types in terms of parental mental health (SMD 0.00, 95% CI −0.16 to 0.16).18 27 35 36 47 48 Sensitivity analysis showed the overall effect size was not influenced by removing single effect size (online supplemental appendix S5B). Egger’s regression test showed a publication bias (p<0.05) (online supplemental appendix S7B).

The forest plots for parents’ psychological adjustment.
Five articles reported the differences in parenting stress.32 35 40 48 49 All these studies were chosen for meta-analysis. The estimated overall effect size was not statistically significant (SMD 0.01, 95% CI −0.20 to 0.22) (figure 4B), showing that the parenting stress was no different between sexual minority and heterosexual parents. Sensitivity analysis showed no single effect size influenced the overall result (online supplemental appendix S5C). Egger’s regression test also showed no evidence of publication bias (p>0.05) (online supplemental appendix S7C).
Parent–child relationship
Six studies reported the differences in parent–child relationships among different family types, all of them were selected for meta-analysis.30 35 36 40 47 50 The overall effect size was statistically significant (SMD 0.13, 95% CI 0.06 to 0.20) (figure 5), indicating that sexual minority parent groups showed higher levels of parent–child relationship quality, such as higher levels of warmth, greater amounts of interaction and more supportive behaviour, when compared with the heterosexual parent groups. Egger’s regression test showed no publication bias (p>0.05) (online supplemental appendix S7D). Sensitivity analysis showed no single effect size influenced the overall result (online supplemental appendix S5D).
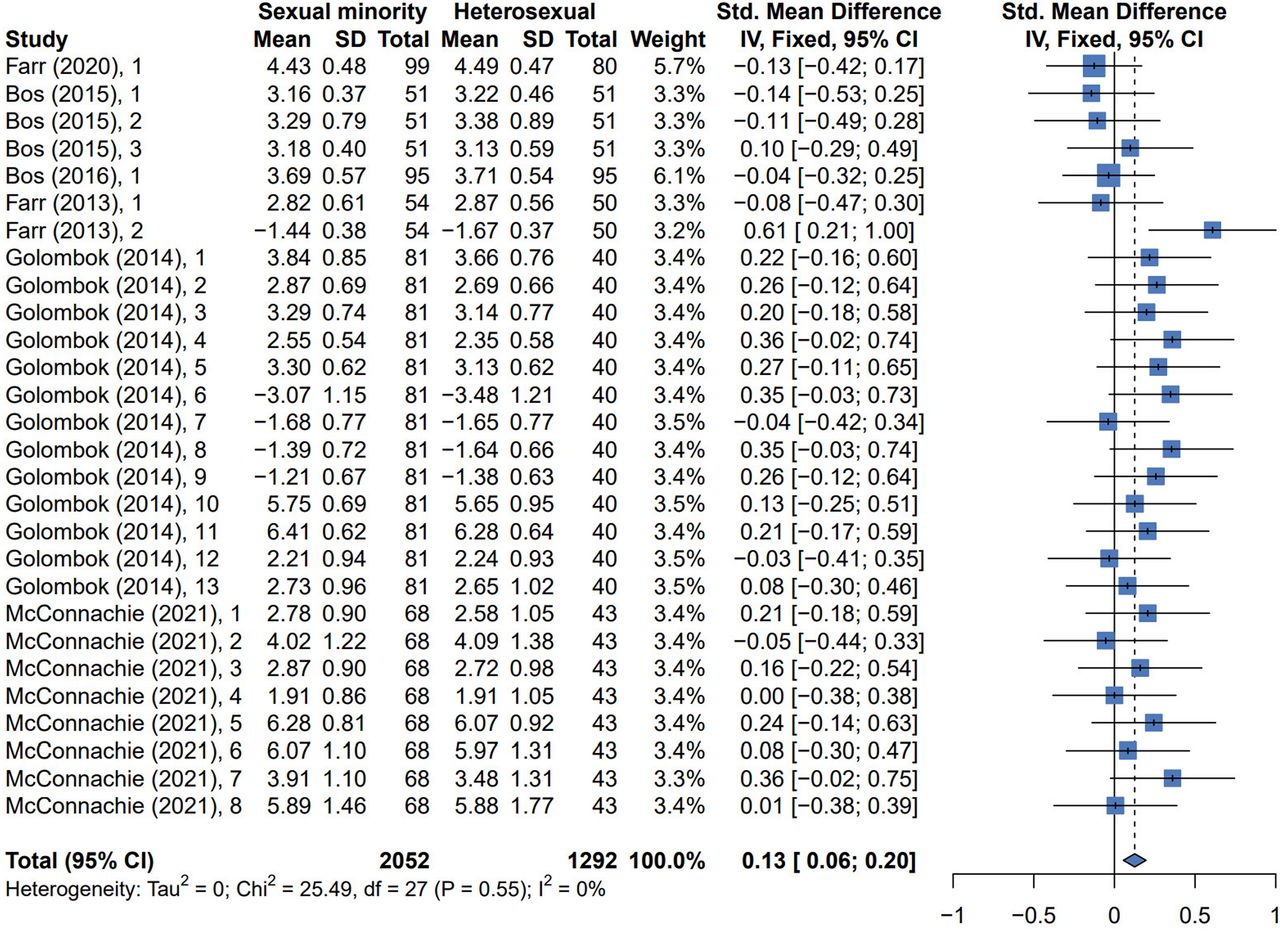
The forest plots for parent–child relationship.
Couple relationship satisfaction
Six studies collected data on couple relationship satisfaction among different family types.26 28 31 40 48 51 Among them, a qualitative study examined changes in couple intimate relationship. The finding showed few differences in intimate relationship by parent sexual orientation.51 Another five studies were chosen for meta-analysis.26 28 31 40 48 The estimated overall effect size was not statistically significant (SMD 0.26, 95% CI −0.13 to 0.64) (figure 6), indicating that sexual minority couples and heterosexual couples did not show difference on these measures of couple relationship satisfaction. Egger’s regression test showed no publication bias (p>0.05) (online supplemental appendix S7E). Sensitivity analysis showed no single effect size influenced the overall result (online supplemental appendix S5E).

The forest plots for couple relationship satisfaction.
Family functioning
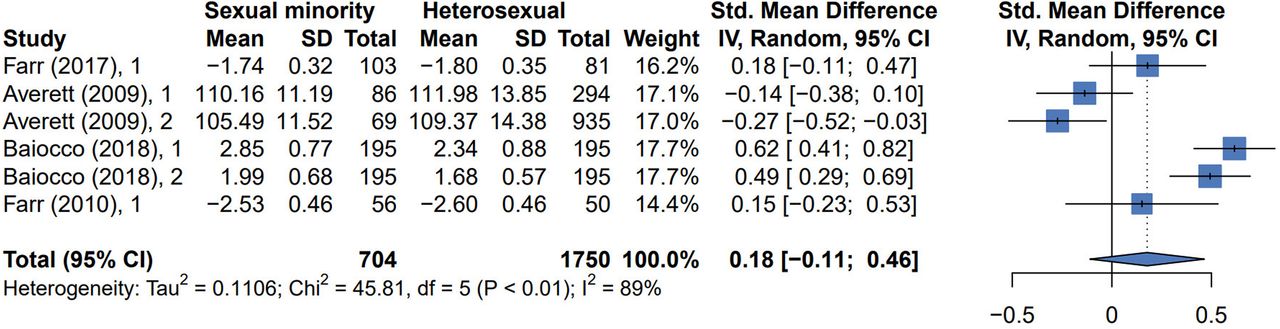
All studies of this topic were chosen for meta-analysis.25 26 28 49 From figure 7, the heterogeneity test showed wide heterogeneity across effect sizes (p<0.05, I2=89%). The random effects model was used. The overall effect size was not statistically significant (SMD 0.18, 95% CI −0.11 to 0.46), suggesting that family functioning was no different between sexual minority parent families and heterosexual families. Sensitivity analysis showed the overall effect size was influenced by removing single effect size (online supplemental appendix S5F). Leave-one-out analysis showed that no singular study when omitted diminished the significant heterogeneity present (online supplemental appendix S5F). Egger’s regression test showed there was a publication bias (p<0.05) (online supplemental appendix S7F), which also adds uncertainty to the estimates. Given that these differences are sensitive to sample exclusions, it is recommended that the result based on six effect sizes should be interpreted with caution. Thus, the certainty of evidence was graded low.
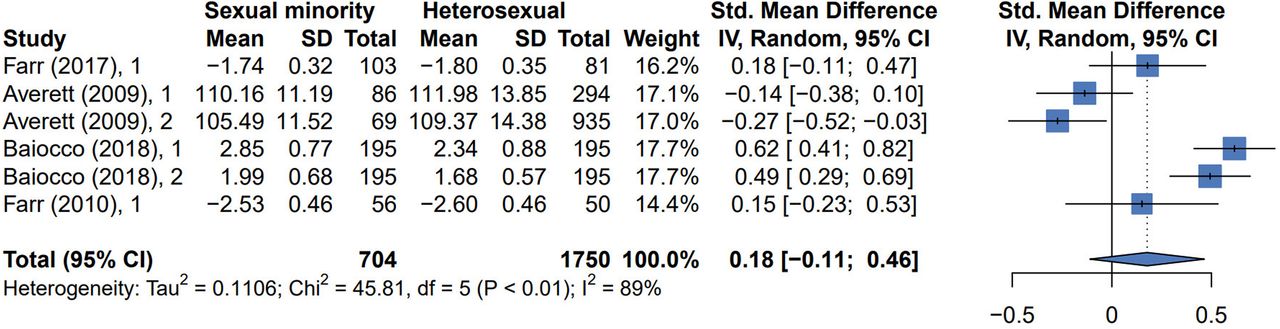
The forest plots for family functioning.
Social support
Three articles reported the differences in social support among gay, lesbian and heterosexual parent families.32 52 53 All three studies on this topic were included in narrative synthesis (table 1). Overall, same-sex parents did not perceive a significant lack of social support.32 53 Lesbian and gay participants faced additional concerns regarding the security of their placement due to the possibility of homophobic discrimination.52
Other outcomes
Five outcomes cannot be grouped into themes. Three studies report the outcomes on school-related aspects,27 54 55 the detailed results are listed in table 1. Regarding the consumption of cigarettes, alcohol, and marijuana/hashish, no significant differences were found between children in lesbian parent families and children in heterosexual parent families.30 Compared with different-sex parent families, same-sex parent families reported higher levels of parental self-agency.28
Discussion
To our knowledge, this is the first systematic review to identify the disparities in family outcomes between sexual minority parent families and heterosexual parent families against the background of legal recognition of same-sex relationships. Contrary to many concerns, our review found most family outcomes were similar between these two family types, and sexual minority families have even better outcomes in some domains, such as child psychological adjustment and child-parent relationships.
While some evidence was found that sexual minority parents were more likely than heterosexual parents to adopt hard-to-place children,54 our meta-analysis found better psychological adjustment in children raised by sexual minorities, especially in preschool age children. This result is consistent with previous reviews17 and may be due to better preparedness in the face of strong anti-gay stigma related to sexual minority parent families, and therefore may have displayed greater adjustment difficulties. Another potential explanation is potential higher socioeconomic status and more egalitarian parenting roles in sexual minority parent families.17 Sexual minorities historically have faced more rigorous scrutiny than heterosexuals regarding their rights to become parents.15 In fact, growing up with sexual minority parents may confer some advantages to children. They have been described as more tolerant of diversity and more nurturing towards younger children than children of heterosexual parents.15
Based the results of narrative synthesis, children who lived in sexual minority parent families had a lower expected likelihood of developing as heterosexual, compared with the children who lived in heterosexual parent families.20 29 41 Moreover, the level of gender stereotype is moulded by the parent-related gender-role information.41 For example, the son of the GFF was perceived as less masculine.41 There may be less gender stereotyping in minority parent families, and this effect may be positive. Regardless of family type, if parents hold more liberal attitudes towards gender-related behaviour, their children hold more flexible attitudes towards gender.29 Children of sexual minority parents receive different gender-related information and they will likely develop different ideas about gender identity or sexual orientation than their counterparts in heterosexual families. The impact of sexual minority parents’ attitudes toward gender on their children might be uniquely positive. Exploration of gender identity and sexuality may actually enhance children’s ability to succeed and thrive in a range of contexts.
Implications for policy and practice
Our findings indicated that children of sexual minority couples are not at a disadvantage when compared with children of heterosexual couples. We advocate among policy-makers, communities, schools, families, and individuals for better awareness of family outcomes of sexual minorities. Despite some shared characteristics and experiences, families headed by sexual minorities are diverse. The experiences may influence parenting practices and family dynamics.56 To address the existing key problems, several actions are necessary to improve sexual minorities’ family outcomes. Based on the findings from our systematic review as well as some specific recommendations that were originally detailed in the included studies, we summarised social risk factors of poor family outcomes and would like to offer suggestions for researchers, policy-makers, and practitioners that might lead to better family outcomes for sexual minority families (figure 8).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proposed actions to improve the family outcomes.
Factors related to children’s psychological adjustment
A growing body of research has demonstrated a link between family process variables and children’s psychological adjustment, such as parenting stress, couple satisfaction, and parenting quality.26 28 32 35 36 Much research has shown that parenting stress and parental mental health are linked to children’s psychological adjustment.17 18 20 26 32 36 39 48 49 51 Parents under greater stress are less likely to provide supportive home environments for their children, consequently children’s development may be affected.57 Children are more likely to thrive when their parents are in good mental health.58 Therefore, it is essential to provide psychological guidance or intervention for parents and children.
The family environment may influence children’s adjustment.18 30 35 59 60 Lower couple relationship satisfaction and parents’ unstable union statuses were significantly associated with assessments of child behaviour problems.26 28 31 37 And, parenting styles were also found to be significantly associated with children’s adjustment.26 49 60 Therefore, it is essential to promote positive parenting styles and increase communication and interaction among family members.
Social climate and environment may be related to children’s psychological adjustment.27 61 Figure 3 suggested that there was a decreasing trend in the difference between children of sexual minority parents and children of heterosexual parents in children’s psychological adjustment over time, which may be due to an increasingly inclusive social environment and greater public awareness of sexual minorities. Homophobic stigmatisation and perceived stigma were related to more psychological problems.33 38 Subgroup analysis by country and region showed that, sexual minority parents reported significantly fewer psychological problems than heterosexual parents in Europe, especially in the Netherlands. Indeed, the Netherlands was the first country in the world to legalise same-sex marriage.14 In a country with a rather tolerant climate toward homosexuality, life may be easier for both children and parents in a sexual minority family.
Factors related to children’s physical health
Studies have shown that children in cohabiting households or single-parent families have poorer health outcomes than children in married households.19 37 Legal marriage confers a host of protections and advantages to the couples who marry and to their children.62 These findings play an important role in health policy, improving child health outcomes.
Factors related to children’s educational outcomes
Research suggests that adequate parenting preparation and positive parenting are important for children’s educational outcomes.63–65 Discrimination and stigma related to parental sexual orientation are an important risk factor.44 Therefore, sexual-minority parents were more likely to consider racial diversity of school than heterosexual parents.54 Parental instability has been found to be detrimental for their children’s educational outcomes.44 62 Parents should make sufficient preparation for parenting, and fully participate in the children’s education process. Schools should take measures to prevent stigma, discrimination and bullying related to sexual minorities in the school setting.
Factors related to family relationship
Many new parents experienced a decline in their relationship quality across the first year of parenthood.51 Parents who reported greater use of confrontative coping, higher levels of depression, and higher levels of relationship maintenance behaviours in pre-adoption reported a greater decline in couple relationship quality.66 At the same time, the exposure to sexual minority stressors might have a negative influence on partner relationship satisfaction.48 On the contrary, some participants emphasised that the experience of parenting had enhanced their relationship and brought them closer.51 Practitioners should provide supportive interventions for diverse couples during the transition to parenthood and reduce sexual minority stressors.
Factors related to parents’ psychological adjustment
Greater social support was related to lower parenting stress.20 57 Parents with older children, more children, and children who were adopted at older ages reported more parenting stress.57 For parenting stress, there was a significant decline over time for heterosexual parents but not for gay and lesbian parents.67 Based on the sexual minority stress model, sexual minority parents may be stigmatised in relation to their sexual orientation.68 Participants with better self-identity and who were more open about their sexual orientation reported higher self-esteem and more positive feelings overall.57 Therefore, social workers or related professionals should provide parenting skills guidance and psychological intervention. At the same time, it is essential to raise public awareness and understanding of sexual minority parent families to reduce discrimination.48
Factors related to social support
Given the Netherlands’ reputation for liberal policies, Dutch children would be more likely than children in some other areas to tell peers about their mothers’ sexual identities and less likely to say they had encountered prejudice and discrimination.56 Social support and community climate variations have an impact on the health and well-being of sexual minority parents and their children.69 Overall, legal marriage confers a host of protections and advantages to the couples who marry and to their children,15 such legalisation reduces the stress and stigma of homosexuality.43 62
Limitations
Despite the significance of this review study, there were a few limitations. First, our overall pooled estimates may be overestimated. Since the studies were limited to regions where same-sex relationships were legalised, most of the studies we included originated in Western Europe and North America, where the social climate for sexual minority parents is generally favourable. The next step could be to summarise the studies conducted in the regions where same-sex relationships are illegal. Second, most of the samples included in this review were gay and lesbian households. Some also considered the unique experiences and concerns of bisexual parents. For example, bisexual parents appear to be in different-gender partnerships or single, and report higher psychological distress than parents of other sexual identities.70 Research on transgender or other sexual minority parent families remains relatively limited.71 72 Important future directions will be exploring the experiences of bisexual- and transgender-parents and their children. Thirdly, based on the availability of the existing data, we were not able to conduct more detailed and in-depth analysis for demographic characteristics. Future reviews need to pay more attention to the demographic characteristics when summarising their findings. Fourthly, we might not have fully captured the effects of changes in legislation implementation on the outcomes. The legal situation for sexual minority parents varies from one country to another around the world.56 Researchers need to learn more about how legal and policy contexts affect the lives of sexual minority parents and their children.73 In addition, our analysis included four articles with a moderate risk of bias.20 40 41 53 We should evaluate these results with caution, especially when considering the controversial study by Regnerus.20
Conclusion
This review showed that most of the family outcomes are similar between sexual minority families and heterosexual families. Research on sexual minority parents and their children has broadened our understanding of contemporary family life, and has added to our understanding of parenting and child development. One contribution of this review is the recognition that parents’ sexual orientation is not, in and of itself, an important determinant of children’s development. Another contribution of this review is that there are significant risk factors often associated with the sexual minority experience and family functioning, such as stigma, poor social support and parenting styles. Policy-makers, practitioners and the public must work together to improve family outcomes, regardless of sexual orientation. In the years ahead, we need to learn more about how communities around the world can support positive development among all children of sexual minority parents and how legal and policy contexts affect their lives and their children.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Press release
Footnotes
Handling editor Seye Abimbola
Contributors YZ, HH and MW contributed equally to this paper and are joint first authors. WP and CN contributed equally to this paper and are joint last authors. YZ, HH, MW, and CN conceived and designed the study. YZ, MW and HH conducted the systematic search, screened articles, and read the full texts for eligibility. YZ and MW extracted data from the original studies. YZ and HH evaluated the studies for risk of bias. JZ and YZ performed the analyses. YZ, HH and MW wrote the first draft of the manuscript. WP and CN contributed to the interpretation of the results and critically revised the manuscript as well as monitored the review process. All authors provided advice at different stages. All authors approved the final version of the manuscript. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. CN is the guarantor.
Funding This study received support from the National Natural Science Foundation of China (Grant Nos. 81803295 and 81760602), the Innovation Project of Guangxi Graduate Education (YCSW2022201).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.