Article Text

Abstract
Background Peer support is an important supplement to medical resources for persons living with HIV (PLHIV). However, previous studies have shown mixed results about intervention effects. It is necessary to explain the mechanism of peer support interventions’ effectiveness and sustainability to help design more valid peer support interventions.
Objective To identify and explain the mechanisms that drive the effectiveness and maintain the sustainability of peer support interventions.
Methods A preliminary theoretical framework was developed through a scoping review of the grey literature and international project frameworks in five professional websites. We then refined the framework by systematically searching evidence in databases including PubMed, EMBASE, Web of Science, ProQuest, CINAHL, CNKI and Wanfang. Qualitative methods were used to generate codes and themes relating to the studies’ context, mechanisms and outcomes. We checked chains of inference (connections) across extracted data and themes through an iterative process.
Results A total of 6345 articles were identified, and 52 articles were retained for final synthesis. The refined theoretical framework presents five areas of peer support, including informational support, instrumental support, emotional support, affiliational support and appraisal support; five types of outcomes that peer support can improve for PLHIV, including physiological outcomes, psychological outcomes, behavioural outcomes, cognitive outcomes and social outcomes; the effectiveness mechanism coding system from peer volunteers and the relationship between peer volunteers and PLHIV; and the sustainability mechanism coding system in terms of peer volunteers, PLHIV and study context.
Conclusions Given that peer support has huge potential human resources, that is, all the qualified PLHIV, irreplaceable advantages in dealing with barriers to HIV-related discrimination and potential comprehensive benefits for PLHIV, it is necessary to develop and organise more peer support projects for PLHIV. Our study highlights that the expansion of peer support projects should be based on their effectiveness and sustainability.
PROSPERO registration number CRD42022339079.
- HIV
- AIDS
- systematic review
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Peer support is an important supplement to medical resources and a common strategy for preventing HIV and promoting health worldwide. However, the intervention effects of peer support are greatly influenced by the study context and have shown mixed results in previous studies. Many HIV peer support studies have only shown short-term intervention effects.
WHAT THIS STUDY ADDS
This realist synthesis provides a theoretical framework that explains the mechanisms driving the effectiveness and sustainability of peer support interventions. The effectiveness mechanisms include coding system from peer volunteers and the relationship between peer volunteers and persons living with HIV (PLHIV). The sustainability mechanisms include a coding system in terms of peer volunteers, PLHIV and study context.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This framework helps contribute to designing effective and sustainable peer support interventions for PLHIV, thus improving PLHIV’s health outcomes and saving medical resources.
Introduction
With the advent of antiretroviral therapy (ART), HIV infection has become a chronic disease.1 The goals of HIV treatment and care are no longer just about prolonging the lives of people living with HIV (PLHIV), but more about improving their quality of life.2 Medical resources need to cover all the PLHIV with a diagnosis of HIV infection regardless of any stages. This transition poses additional challenges to the healthcare system to meet PLHIV’s various medical care needs, especially in environments where medical resources are in short supply.3 Previous studies indicate that PLHIV commonly confronts various distress and unmet medical care needs.4 5 Moreover, the issue of HIV-related discrimination also acts as a barrier to PLHIV seeking medical and psychosocial support.6 7 Therefore, more medical care resources, especially those that can lower PLHIV’s psychological defences, are needed to improve PLHIV’s quality of life, thus promoting the achievement of the ‘95-95-95’ goal (95% of PLHIV know their HIV infection, 95% of PLHIV with HIV-positive diagnosis receive ART, 95% of PLHIV on ART achieve viral load suppression)8 and improving health-related quality of life for PLHIV at any stage.9
Peer support is defined as ‘the giving of assistance and encouragement by an individual considered equal’.10 It is an important supplement to medical resources and a common strategy for preventing HIV and promoting health worldwide.11 Common peer support forms in the field of HIV care include but are not limited to peer education and peer counselling by other PLHIV.12–14 Compared with medical professionals, peer volunteers can generate more interpersonal interactions with PLHIV and offer them more authentic empathy and validation because of their similar experiences, which have irreplaceable advantages in the context of HIV-related discrimination.15 They can even offer practical advice and suggestions that professionals may not offer or even know about.16 By drawing on their own lived experience, peer volunteers can offer practical advice on the day-to-day aspects of living with HIV, advice that extends beyond the expertise of clinically-based medical professionals. Furthermore, peer support is more cost-effective and provides potentially more access than traditional services from medical care providers.17 18 Therefore, many countries, such as the UK,19 Australia20 and Canada,21 have published national standards or practice guidelines for peer support for HIV. The United Nations Programme on HIV/AIDS (UNAIDS) also proposed the Greater Involvement of People Living with HIV (GIPA) principle to advocate for more participation and contribution of peer volunteers.22
Previous studies have validated the effects of peer support on many outcomes, such as helping PLHIV improve mental health, social support, medication adherence, HIV care visit adherence and viral suppression.23–26 The intervention effects of peer support have also been verified among different specific characteristics, such as adolescents living with HIV,27 28 mothers living with HIV29 30 and PLHIV in prison or jail.31 However, the intervention effects of peer support are greatly influenced by the study context.32 Moreover, many HIV peer support studies have only shown short-term intervention effects.32 33 PLHIV may not continue to benefit after the completion of the peer support project. Consequently, it is necessary to explain significant components and factors of peer support interventions’ effectiveness and sustainability, that is, the mechanisms, to help design more valid peer support interventions. This study aims to conduct a realist synthesis to propose a theoretical framework with context-mechanism-outcome (CMO) configurations34 to explain the effectiveness and sustainability of HIV peer support interventions. Our attempt provides important insights to help activate and realise potential great contributions to promoting PLHIV’s health.
Methods
This realist synthesis is reported according to the Realist and Meta-narrative Evidence Syntheses: Evolving Standards quality and publication standards (RAMESES).35 We prospectively registered the current review in the PROSPERO database.36 The realist synthesis method with five steps was applied for this review.37
Step 1: formulating a preliminary theoretical framework
The preliminary theoretical framework was developed through a scoping review of the grey literature and international project frameworks from five websites, including Canada’s Source for HIV and Hepatitis C Information (CATIE),38 British HIV Association (BHIVA),39 National Association of People with HIV Australia (NAPWHA),40 National HIV Nurse Association (NHIVNA)41 and UNAIDS.42 Considering that these websites lack advanced search functions, we only applied basic and sample search strategies. Free terms including ‘HIV’ and ‘peer’ were used to perform the search in May 2022. One researcher (SH) screened all the records, included records according to the relevance of the study objectives and extracted supportive information for the preliminary theoretical framework in terms of, areas of peer support interventions, types of outcomes, effectiveness mechanisms and sustainability mechanisms. A record was included if it was relevant to at least one aspect of the extracted information.
Step 2: search strategy
Our search strategy can be divided into three stages. First, we conducted a preliminary search in PubMed to develop search strategies tailored to each database. The expanded search strategies were discussed with the research team before conducting systematic searches in each database. Second, we implemented the search strategies in PubMed, EMBASE, Web of Science, ProQuest, CINAHL, CNKI and Wanfang. Both free terms and Medical Subject Headings were used in each database if applicable. We limited the publication date to after 1 January 1996 because ART was broadly introduced after 1996.1 The detailed search strategies for each database are available in online supplemental appendix I. Third, the references of all the included articles were reviewed to identify eligible literature not found in the systematic search strategies. During the framework refinement process, the necessary purposive iterative searching was conducted to identify additional articles that might support any element in the framework. The search stopped when there was sufficient evidence to reasonably claim that the final theoretical framework was plausible.
Supplemental material
Step 3: study selection criteria
All the records searched from the database were imported, and duplicates were removed in NoteExpress. Two researchers (SH and KL) who had been trained in evidence-based methodologies independently filtered the records by reading titles and abstracts to initially exclude literature that was not relevant to the theoretical framework. A third researcher (ZW) resolved disagreements in the preliminary study selection process.
The inclusion criteria were as follows: (1) Population: PLHIV aged 18 years and older in any country or setting regardless of any stage of HIV. We excluded PLHIV who were in special situations, including pregnancy, in prison and with severe mental health diseases. (2) Intervention: Any intervention provided by HIV-positive peer volunteers was eligible for this review. We did not limit the types of peer support interventions available. However, to clarify the intervention effectiveness of peer support, we only included clinical trials in which peer volunteers were the unique intervention providers. Clinical trials with multiple types of intervention providers (such as medical professionals and psychologists) that did not report clear intervention doses were excluded. (3) Language: We only included articles that were published in English or Chinese. There were no exclusions based on the outcomes of HIV peer support projects, study design or study quality of the involved articles. Study designs other than clinical trials were not restricted as seriously as clinical trials in terms of intervention. For instance, the background of a qualitative study might be an HIV peer support project delivered by both peer volunteers and medical professionals. However, the results of the qualitative study were only focused on peer support. Under these circumstances, this qualitative study was eligible for the current study. Every excluded study was recorded along with the reason for its exclusion.
The full-text screening was completed by the whole research team with members working in pairs and the papers divided among the team. Each article that was involved in the preliminary screening process was assessed for its relevance to the content in framework refinement. Generally, it is likely that only a fragment rather than the entire study will inform the theoretical framework in a realist synthesis. Therefore, consistent with the development process of the preliminary theoretical framework, a record was included if it was relevant to at least one element in the framework according to the CMO configurations. Any exclusion in this process was recorded and reasons why were noted.
Step 4: data extraction
A standardised Excel spreadsheet was used to record the extracted characteristics of the original studies involved. The characteristics of the involved original studies include author (year), setting, objectives, study design, participants, interview method, intervention and results. The data extraction process was performed by two researchers (SH and KL) independently and checked by a third researcher (ZW).
Step 5: data analysis and synthesis
Five steps for data analysis and synthesis were followed.43 First, the extracted data and their references were summarised and organised into draft evidence tables. Second, qualitative methods were used to generate codes and themes relating to the CMOs. Third, we checked chains of inference (connections) across extracted data and themes through an iterative process. Fourth, new COM configurations arose according to the chains of inference. Fifth, the preliminary theoretical framework was refined by all the supportive evidence. This process was conducted by one researcher (SH), reviewed by another researcher (KL) and discussed with the research team.
Results
Preliminary theoretical framework
A total of 1111 records were identified from the five professional websites. After reviewing and screening these records, we finally included 21 records, including six videos, to develop the preliminary theoretical framework. The links to these 21 records are available in online supplemental appendix II.
Supplemental material
As shown in figure 1, we initially identified four types of peer support interventions44 45: (1) informational support: peer volunteers provide knowledge and personal experience with PLHIV; (2) emotional support: peer volunteers help PLHIV vent their emotions, express love and care and convey positive beliefs; (3) appraisal support: peer volunteers encourage PLHIV decision-making by providing information, and weighing the pros and cons; and (4) instrumental support: peer volunteers provide material or monetary support to PLHIV. To develop effective and sustainable peer support, researchers need to pay attention to the following key points20 21 45–47: choosing qualified peer volunteers, providing effective training with peer volunteers, ensuring ongoing supervision and feedback, mitigating peer volunteers’ compassion fatigue and burnout, providing easy access to peer support with PLHIV, matching peer volunteers with PLHIV and providing PLHIV with tailored services and attaching peer support projects with open platforms.

The preliminary theoretical framework.
When PLHIV receive effective peer support interventions, they may feel a sense of compatibility, empathy, acceptance and benefit.20 These are the mechanisms by which peer support improves PLHIV’s outcomes. By reviewing peer support interventions in the scoping review, we summarised that peer support interventions could improve PLHIV’s five types of outcomes20 21: (1) physiological outcomes, such as an increase in CD4 cell counts and decrease in viral load; (2) psychological outcomes, such as relieving depression and anxiety; (3) cognitive outcomes, such as increasing confidence and supporting feelings of being in control of their own health; (4) behavioural outcomes, such as improving medication adherence and retention in care; and (5) social outcomes, such as creating social connections and enabling PLHIV to go back to work.
Literature search
As shown in figure 2, a total of 6345 articles were identified after searching seven databases. We removed 1109 records through NoteExpress and retained 5236 articles for screening. During the preliminary screening stage, we excluded 4604 records by reviewing the titles and abstracts. We finally included 52 articles after reviewing 632 full texts and conducting snowballing. Of the 52 included articles, the relevance of 46 articles was agreed between two researchers and included directly. The inter-rater reliability was 0.885. Other six included articles were discussed in the research group before their inclusion.

Flowchart of the identification and selection of studies.
Study description
Table 1 presents the research details of each included article. Of the 52 included studies, 49 were published in English and 3 were published in Chinese. The year of publication ranged from 2005 to 2022. Study settings involved 17 countries, including 19 studies in the USA, 6 studies in South Africa, 5 studies each in China and Uganda, 3 studies in Canada, 3 studies each in Vietnam and Mozambique and 1 study each in Spain, Norway, Australia, Zimbabwe, South Korea, India, Dominican Republic, UK, Myanmar and Nigeria. Of these studies, 21 were clinical trials, 20 were qualitative studies, 7 were mixed-method studies, 3 were cross-sectional studies and 1 was a cohort study.
Study characteristics
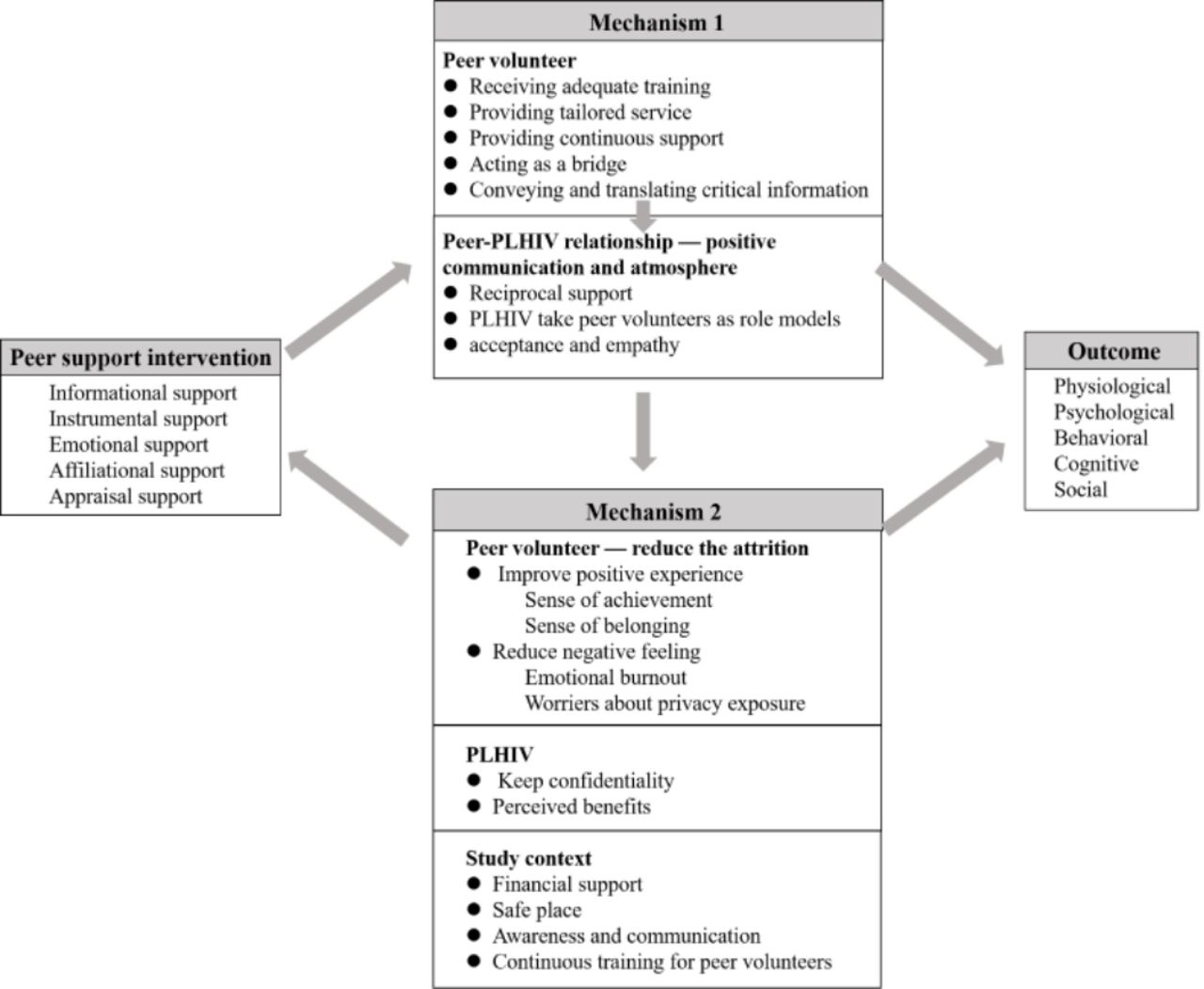
The refined theoretical framework
What can peer volunteers provide for PLHIV?
As shown in figure 3, the refined theoretical framework identifies peer support into five areas in terms of intervention contents: informational support, instrumental support, emotional support, affiliational support and appraisal support.48–51Informational support requires peer volunteers to educate PLHIV about a variety of topics and help them better comprehend medical information from their healthcare providers.49 52 Instrumental support can be divided into medical instrumental support, such as referring and transporting PLHIV to medical professionals, scheduling appointments and making calls to remind PLHIV of appointments48 51; and daily life instrumental support, such as substance abuse treatment support and food and housing security support.48 Emotional support is an important component of peer support. PLHIV also show huge unmet needs for emotional support.51 To provide emotional support to PLHIV, peer volunteers sometimes may not need to have complex professional psychological skills. It truly does work if peer volunteers just listen to PLHIV to help them alleviate their negative emotions. Other emotional support may include using listening and reflective techniques to help PLHIV gain confidence in their ability to change health-related behaviours48; appealing to PLHIV’s emotions to reinforce or change behaviours53; and demonstrating caring, empathy and comfort to help PLHIV begin to engage in HIV care and treatment.54 Affiliational support aims to help PLHIV reduce isolation and connect to social networks.48 55 Appraisal support aims to help PLHIV make decisions about their treatment, self-care and daily life conflicts by providing information, weighing the pros and cons and conducting motivational interviews.50
{kind=link}
{kind=link}
{kind=link}
The refined theoretical framework. PLHIV, persons living with HIV.
What outcomes can peer support improve?
We summarised the following types of outcomes that peer support can improve according to the involved clinical trials: physiological outcomes (viral load suppression56–58 and pain59), psychological outcomes (quality of life60), behavioural outcomes (risky behaviours,12 14 medical care compliance56 57 61 62 and medication adherence56 63–65) and cognitive outcomes (HIV knowledge,66 67 self-awareness of behaviour problems68 and enacted and internalised stigma56 66). Although there was limited evidence of effectiveness on psychological outcomes and social outcomes among clinical trials, in qualitative studies, PLHIV reflected that they acquired these benefits. PLHIV reported that peer support can help them reduce loneliness and increase their sense of attachment, sense of belonging, sense of worth, disease acceptance, confidence and hope.51 53–55 69 Social activity engagement was also improved after attending the peer support project.67
What is the mechanism that improves the effectiveness of peer support?
Peer volunteers
Ensuring peer volunteers are appropriately qualified is an important aspect of effective peer support programmes. Qualified peer volunteers should: first, receive adequate training70 71; second, provide tailored service to meet PLHIV’s personal needs50 72–75; third, provide continuous support beyond the clinical setting52; fourth, act as a bridge between PLHIV and their social relationships, community and the health system52 76–78; and fifth, convey and translate critical information.52
Peer-PLHIV relationship
A positive communication and atmosphere between peer volunteers and PLHIV is essential to guarantee intervention effects.67 69 First, the reciprocal support makes peer volunteers and PLHIV satisfied by receiving and providing support.79 Second, PLHIV take peer volunteers as role models and are encouraged by peer volunteers’ experiences and positive attitudes.76 80 Third, PLHIV feel acceptance and empathy through free expression in a positive atmosphere.54 69
What is the mechanism that maintains the sustainability of peer support?
Peer volunteers
To improve the sustainability of peer support interventions, it is important to reduce the attrition of peer volunteers.70 74 81 On the one hand, peer support projects should improve the positive experience of peer volunteers, including their sense of achievement74 81 and sense of belonging.81 82 The sense of achievement comes from helping others76 and personal growth.54 74 79 Some peer volunteers reported that participating in peer support can help improve self-management skills, regulate their own mental health and is an important way to give back to society.74 On the other hand, it is necessary to quickly identify and reduce peer volunteers’ negative feelings during practice, including emotional burnout74 81–83 and worriers about privacy exposure.74 81 84 Emotional burnout may come from negative feedback from PLHIV, repetitive work and work-related stress.69 74 81 82 85
PLHIV
In terms of PLHIV, researchers should design effective measures to maintain PLHIV’s confidentiality,52 55 86 and make them have perceived benefits.55 Perceived benefits can include perceived improvement or belief in improving one or more outcomes of physiological outcomes, psychological outcomes, behavioural outcomes, cognitive outcomes and social outcomes.
Study context
The following components in the study context are related to the sustainability of the intervention project. First, the peer support project needs sufficient financial support to pay peer volunteers’ salary and guarantee project operation.56 76 81 82 Second, access to a safe place reassures both PLHIV and peer volunteers of privacy exposure concerns.53 Third, more communication between peer volunteers and medical staff is necessary to reduce the information gap and to better integrate volunteers into the clinical setting.52 55 70 83 Fourth, the context should provide continuous training for peer volunteers to meet their self-growth needs and be more effective in their role as peer supporters.82
Discussion
To our knowledge, this is the first realist synthesis about peer support for PLHIV. The theoretical framework summarises the type of interventions that peer volunteers can provide and the potential type of outcomes that peer support can help PLHIV improve. Specifically, this theoretical framework comprehensively explains the mechanisms for developing effective and sustainable peer support interventions. Our attempt may provide researchers with theoretical reference for peer support project design and practice and motivate peer volunteers in the health management of PLHIV.
Evidence indicates that peer volunteers can provide various areas of support, including informational support, instrumental support, emotional support, affiliational support and appraisal support. Interventions in included clinical trials also usually included at least one type of support. Therefore, peer volunteers are important resources for providing comprehensive support for PLHIV beyond medical professionals. Many qualitative studies have shown the great necessity of emotional support.51 53–55 69 However, we found only weak evidence that peer support has intervention effects on psychological outcomes. We estimate that it may be associated with the following factors. First, most of the clinical trials took emotional support as a secondary intervention component, and the intervention dose may not be enough to show an intervention effect.12 14 59–61 87–89 Second, measurement tools may not be sensitive to test the intervention effect.14 61 88 Third, small sample sizes may not have enough power to test the intervention effect.59 63 87 We suggest that researchers pay more attention to peer volunteers’ emotional support skill training and encourage more peer-led emotional support for PLHIV. They should not just evaluate the necessity of peer volunteers’ emotional support through evidence of quantitative data.
We also summarised that peer support could help PLHIV improve various outcomes, including physiological, psychological, behavioural, cognitive and social outcomes. This evidence indicates the huge value of peer support for PLHIV’s health management, and the necessity of the GIPA principle for promoting the ‘95-95-95’ goal and improving health-related quality of life for PLHIV.8 9 22 Of these outcomes, behavioural outcomes, such as medical follow-up adherence, risky behaviour and medication adherence, were more frequently tested in clinical trials.12 14 57 58 61–65 68 89–92 Future studies could attempt to evaluate other types of outcome effects. Moreover, we could not clarify the specific mechanism of the peer support intervention effect on each kind of outcome. Our framework only presents the general chain of intervention (context) - mechanism - outcome. Future studies could focus on explaining the specific CMO chain, such as the mediating role between specific types of peer support interventions and specific outcomes.
The refined theoretical framework shows comprehensive mechanisms that explain the effectiveness and sustainability of peer support projects. Designing effective interventions should focus on the qualification of peer volunteers and the relationship between peer volunteers and PLHIV during the intervention operation. To ensure that peer volunteers are appropriately qualified, it is crucial to design adequate training. The type of peer support intervention can provide a framework reference for designing the training programme. Peer volunteers who receive adequate training can provide tailored service and continuous support beyond medical care service for PLHIV and play a bridging role in their social relationships. This is also a good continuation of and supplement to medical services. Peer volunteers effectively convey and translate critical information throughout the service, laying the foundation for establishing a positive connection and atmosphere with PLHIV. If PLHIV consider peer volunteers as their role models because of their positive attitudes and experiences, they may benefit from the peer-PLHIV relationship more easily. PLHIV feel accepted and empathetic in a positive relationship and atmosphere. They not only have the role of being helped but also benefit from helping others, that is, establishing reciprocal support with peer volunteers.
To improve the sustainability of peer support projects, researchers should consider factors in terms of peer volunteers, PLHIV and context. A sufficient reserve of peer volunteers is an important foundation for maintaining projects’ sustainability. Therefore, researchers should take effective measures to reduce the attrition of peer volunteers. Evidence indicates that peer volunteers report mixed feelings during the process of supporting PLHIV.54 69 74 76 79 81–85 Their positive feelings need to be reinforced, and their negative feelings need to be adjusted in time. Emotional support is also necessary for peer volunteers in projects.74 85 Project administrators can arrange psychologists or peer volunteers to provide support for them. If PLHIV feel little risk of privacy exposure and may acquire anticipated benefits, it will contribute greatly to the sustainability of the peer support programme.51 55 PLHIV’s positive attitudes toward and impressions of peer support projects are closely associated with the success of previous projects, that is, the mechanism 1 may affect the mechanism 2. For the context, researchers should provide a safe environment where both peer volunteers and PLHIV feel little risk of privacy exposure. Policymakers or hospital managers should also fully evaluate the cost-effectiveness of peer support projects, provide continuous and stable financial support for peer volunteers as compensation for their time, consider integrating peer support projects into medical care routines and raise peer volunteers as essential members of the medical team.55 81
Peer support is an important continuation of and supplement to medical services. It not only helps save medical resources and reduce medical healthcare workers’ workload, but also can provide crucial support for PLHIV that is beyond the expertise of medical professionals. To maximise the role of peer support, peer volunteers should not be independent and separated in the medical context. More awareness and communication between peer volunteers and medical professionals are necessary to help peer volunteers better integrate into the medical context.52 83 The process of communication also provides good opportunities for project feedback and communication. The medical context also needs to provide continuous training for peer volunteers, which meets PLHIV’s need for knowledge updates and self-management; it also helps peer volunteers better service PLHIV and promote the sustainability of peer support projects.81
Several limitations of this study should be noted. First, we only included articles published in English and Chinese, which may affect the results of this study due to language restrictions. Second, we only conducted qualitative data analysis and synthesis. Therefore, we cannot identify and compare effect sizes between different types of interventions and cannot define which components of the interventions are more effective. Third, although the theoretical framework summarised and synthesised from this review provides a comprehensive mechanism of peer support projects’ effectiveness and sustainability, we did not assess the risk of bias of the included original studies.
Conclusion
This realist synthesis summarises and presents a theoretical framework that explains the mechanisms of peer support interventions’ effectiveness and sustainability. Evidence indicates that the effectiveness mechanisms include coding system from peer volunteers and the relationship between peer volunteers and PLHIV. Mechanisms for sustainability include a coding system in terms of peer volunteers, PLHIV and study context. We suggest that researchers and practitioners comprehensively consider these mechanisms when designing and conducting peer support projects. It may help activate and realise more contributions of peer support for promoting PLHIV’s health.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
SH and YZ are joint first authors.
Handling editor Stephanie M Topp
SH and YZ contributed equally.
Contributors SH: Conceptualisation, Writing—original draft, Funding acquisition. YZ: Conceptualisation, Writing—original draft. XY: Conceptualisation, Writing—original draft. XC: Methodology, Validation. JG: Methodology, Validation. LZ: Writing—review and editing, Supervision. YS: Writing—review and editing. JM: Writing—review and editing. KL: Methodology, Validation. ZW: Supervision, Writing—review and editing, Project administration, Guarantor.
Funding This study was funded by the National Natural Science Foundation of China (72204006), the China Postdoctoral Science Foundation (2022M710258), the Ministry of Education of Humanities and Social Science Project (22YJCZH044) and the Peking University Evidence-Based Nursing Special Research Foundation (XZJJ-2022-10).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.