Article Text

Abstract
Introduction Continuing education for midwives is an important investment area to improve the quality of sexual and reproductive health services. Interventions must take into account and provide solutions for the systemic barriers and gender inequities faced by midwives. Our objective was to generate concepts and a theoretical framework of the range of factors and gender transformative considerations for the development of continuing education interventions for midwives.
Methods A critical interpretive synthesis complemented by key informant interviews, focus groups, observations and document review was applied. Three electronic bibliographic databases (CINAHL, EMBASE and MEDLINE) were searched from July 2019 to September 2020 and were again updated in June 2021. A coding structure was created to guide the synthesis across the five sources of evidence.
Results A total of 4519 records were retrieved through electronic searches and 103 documents were included in the critical interpretive synthesis. Additional evidence totalled 31 key informant interviews, 5 focus groups (Democratic Republic of Congo and Tanzania), 24 programme documents and field observations in the form of notes. The resulting theoretical framework outlines the key considerations including gender, the role of the midwifery association, political and health systems and external forces along with key enabling elements for the design, implementation and evaluation of gender transformative continuing education interventions.
Conclusion Investments in gender transformative continuing education for midwives, led by midwifery associations, can lead to the improvement of midwifery across all United Nations’ target areas including governance, health workforce, health system arrangements and education.
- Health education and promotion
- Health systems
- Maternal health
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
This is the first study of its kind to generate an evidence-informed theoretical framework for considerations to continuing education interventions for midwives using a political and health systems approach.
WHAT THIS STUDY ADDS
Our findings suggest that if supported, midwifery associations have the capacity to host these initiatives, resulting in increases in midwifery leadership, improved integration of the profession in political and health systems, leading to improved care and access to sexual and reproductive health and rights (SRHR).
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our theoretical model can be used by SRHR stakeholders as a guide to designing, implementing and evaluating continuing education in collaboration with and for midwives.
The model provides a starting point for the inclusion of gender transformative approaches in order to impact the status of midwifery.
Investing in gender transformative continuing education for midwives is essential to the sustainable growth of the profession and to improving access to essential SRHR globally.
Introduction
While there is ample evidence in support of the positive impacts of midwifery-led care, the profession is not well integrated into most health systems.1 The 2021, State of the World’s Midwifery report (SoWMY) cites a global shortage of 900 000 midwives with less than 75% of the current need for sexual and reproductive health services being met globally.2 This schism can in part be explained by systemic discrimination of the profession driven by the intersects of gender, race, sociopolitical, professional and economic inequities.3–5 As a result, the SoWMY report calls for the inclusion of gender transformative approaches to the process of the growth of midwifery.2 3
The SoWMY report outlines four key areas of investment essential to the growth of the profession in order to meet the universal health needs of women, childbearing people and newborns: (1) health workforce; (2) education and training; (3) midwifery-led service delivery and (4) midwifery-led governance and leadership.2 Gender transformative approaches cross cut all four areas.2 In a previous publication, our findings demonstrated when appropriately supported, midwifery associations have the capacity to address all four strategic areas outlined in SoWMY, leading to improved health systems and population health outcomes.6 This companion research discusses the role of midwifery associations and gender transformative approaches to the second SoWMY key area, education and training (specifically, continuing education) for sustainable growth of the profession.
The Canadian Association of Midwives (CAM) has engaged in reciprocal capacity building partnerships since 2008 with the National Aboriginal Council of Midwives (situated in the land that is referred to as Canada). They have since extended this collaborative approach with midwifery professional associations in seven countries (Benin, Democratic Republic of Congo, Ethiopia, Haiti, Somalia and Somaliland, South Sudan and Tanzania). CAM’s strategic vision prioritises organisational capacity building and promoting excellence in the continuing education of midwives. Most often, interventions are hosted by partner midwifery associations.6 Throughout their work, CAM observed unanticipated outcomes, such as improvement to structural gender inequities, which led them to hypothesise the overarching value to their approach with continuing education interventions (CEI) and longer term gender transformative impacts to the midwifery profession.
Scholarly knowledge regarding CEI for obstetric/neonatal health professionals, including midwives, is common.7 Yet, the literature often ignores the structural dynamics of where and how programmes are designed and executed, and by whom (ie, who gets paid to do what, who is ‘in charge’ of what). Such omissions obscure power imbalances that intersectionally impact women-led professions like midwifery. Systematic reviews show that adopting a gender transformative approach to programme interventions centres the critical examination of gender and other inequities to promote system changes, which, over time create, change and improve gender-based outcomes in policy and practice.8 This strengthens the importance of building the evidence on gender transformative approaches to CEI as a conduit for promosting enabling environments for sustaining the midwifery profession and by extension impact sexual and reproductive health and rights (SRHR).3 6
We used a three-pronged approach to create an evidence-informed framework. Our first aim was to synthesise multiple sources of evidence to address the following compass question: What are the factors that impact in-service midwifery continuing education, including comprehension, competency and integration of skills? Second, to further understand the factors identified in the first aim, we used the example of CAM’s programming related to the implementation of CEI for midwives by midwifery associations and conducted key informant interviews, focus groups, observations and document review. Our third aim was to develop a conceptual framework for considerations when implementing gender transformative CEI for midwives. The second and third aims overlapped as part of an iterative process in which stakeholders informed and provided feedback on the development of the conceptual framework.
Our work is rooted in intersectional feminist, anticolonial and collaborative lenses. We purposefully do not dichotomise between World Bank classification of countries by income groups (ie, high-income countries vs low-income and middle-income countries) as we recognise that improving access to quality SRHR is relevant to all health systems.9 The importance of context is central, along with how each country’s health system(s) and political system functions within a given context.
Methods
This study was carried out in tandem with ‘Health systems factors impacting the integration of midwifery: an evidence-informed framework on strengthening midwifery associations’ and has the same methodological approach. For a more detailed description, please refer to the previous publication.6
We conducted a qualitative evidence review and synthesis to create a conceptual framework for strengthening of quality midwifery care with continuing education. We used a critical interpretive synthesis as an approach to qualitative systematic review, complemented additional qualitative sources to inform the development of concepts and theory.6 10
Critical interpretive synthesis
The systematic searches for the critical interpretive syntheses were conducted in June 2019 and refreshed in June 2021 in the following electronic bibliographic databases: CINAHL, EMBASE and MEDLINE. A librarian provided guidance on developing keywords (along with Boolean operators) and Medical Subject Heading (MeSH) and executing the searches. While we chose to use the term ‘continuing education interventions for midwives’ in the manuscript, there is no common language or definition of in-service education, and, therefore, we included various terms in the search. The search strategy was developed in the MEDLINE database, using keywords and MeSH and similar search strings were used across databases, with minor adjustments. The searches in MEDLINE included: midwifery/; midwi*.ti,ab,kf.; (emergency adj2 (obstetric or neonatal or care)).ti,ab,kf.; competency.mp.; competency.ti,ab,kf.; evaluation.ti,ab,kf.; skill.mp.; skill.mp.; skill.ti,ab,kf.; train*.ti,ab,kf. Following this step, related SRHR websites known for conducting midwifery training or standards of midwifery education were searched for relevant documents (eg, JHPIEGO, International Confederation of Midwives (ICM), WHO and United Nations Population Fund) and hand searches of reference lists from key publications were used to identify additional relevant literature.
For inclusion in the critical interpretive synthesis, documents had to provide insight into the compass question and include the continuing education of midwives. ‘Midwives’ was loosely defined, meaning it did not have to fit the international criteria for the profession as outlined by the ICM.11 Documents involving other disciplines in the intervention were accepted. Exclusion criteria included documents published before the year 2000 and other than English, Spanish or French. Because the literature is vast in this area, and due to the concentration of CAM programming in Sub-Saharan Africa and the Caribbean, we primarily included documents published in these WHO regions. Hand selection from other WHO regions was acceptable if relevant to midwifery and CAM programmes.6
Additional sources of qualitative evidence
We used key informant interviews, focus groups, observations and document review to inform the development of concepts and theory, and build the framework. All data were collected in English and French. The countries of focus for the additional sources of qualitative evidence included: Benin; Canada; Democratic Republic of the Congo (DRC); Ethiopia; Haiti; South Sudan and Tanzania.
A multistage purposive sampling approach was used to identify and recruit participants who had participated in CAM’s global projects and continuing education interventions for midwives. The four categories of participants were: (1) midwifery professional association staff, executive boards (leaders), midwives and student members; (2) midwife consultants; (3) policymakers, and (4) partner organisations, including visiting or contributing funders and hosts. We invited participants by email or face-to-face and conducted interviews either face-to-face, by phone or virtually. All interviews were audio recorded. Canadian participants were either midwife consultants or individuals working strictly within CAM’s global projects division; and who travelled extensively within the forementioned countries.
During observations in Canada, DRC and Tanzania, focus groups were conducted with stakeholders along with participant observation (CM, KB, AK). The purpose of the focus groups was to gain a deeper understanding of context-specific factors that influence integration of in-service skills and elicit insight and feedback on initial concepts. Participant observation was documented through written notes and audio recordings between researchers (CM and KB).
The selection of the documents for the document review consisted of any programme documents related to projects that included a component on in service skills education. The documents spanned CEI in all countries and ranged from grant proposals, theory of change and logic models, performance management frameworks and evaluations.
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting or dissemination plans of our research.
Data analysis and synthesis
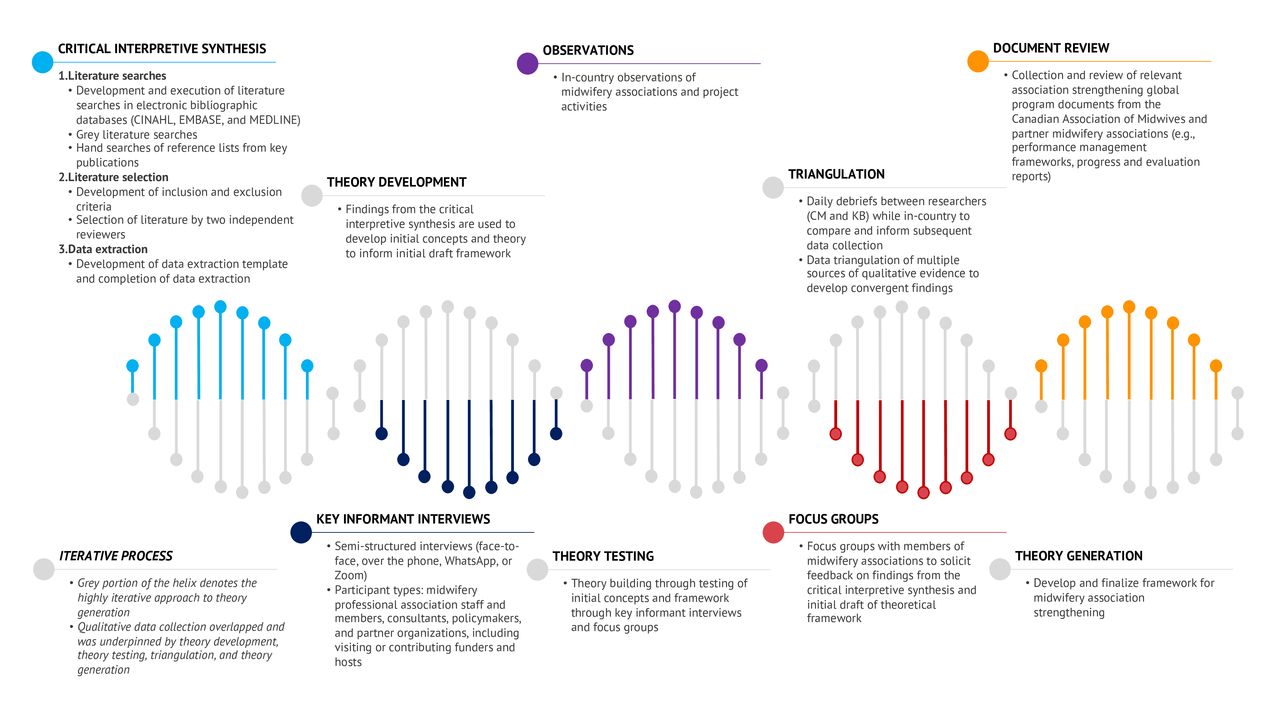
A common feature of qualitative inquiry is that analysis and interpretation overlap with sampling and data collection (figure 1).6 Data extraction for the critical interpretive synthesis was guided by a coding structure. Data were collected on publication year, study design, health professions, jurisdiction(s) of focus, the processes related to and the characteristics of continuing education programmes or interventions involving midwives. The findings from the critical interpretive synthesis were used to develop the initial core concepts and theory related to education for in-service midwives and the initial draft framework.10 Data analysis of the additional sources of qualitative evidence used the qualitative software NVivo for Mac for the organisation and coding of the data. Coding occurred in the original language that the data were collected in (French or English). We applied a constant comparative method, such that emerging data were compared with previously collected data to find similarities and differences.12 Completeness of the findings was ensured through ongoing consultation with members of the research team. During the research process, we broadened the research team to include experts in designing and implementing continuing education programmes via midwifery associations in Canada, DRC and Tanzania. These experts formed a collaborative team and worked with CM and KB during the research process (AK, SS, EH, JR and MC). For example, the research inquiry was validated, and initial results were vetted by association members and leadership. The team went on to codevelop the concepts and framework as well as the manuscript. Finally, there is ongoing collaboration with the research consortium to ensure that results are shared with participating associations, which will also include further research to understand the applicability and feasibility of our conceptual elements.
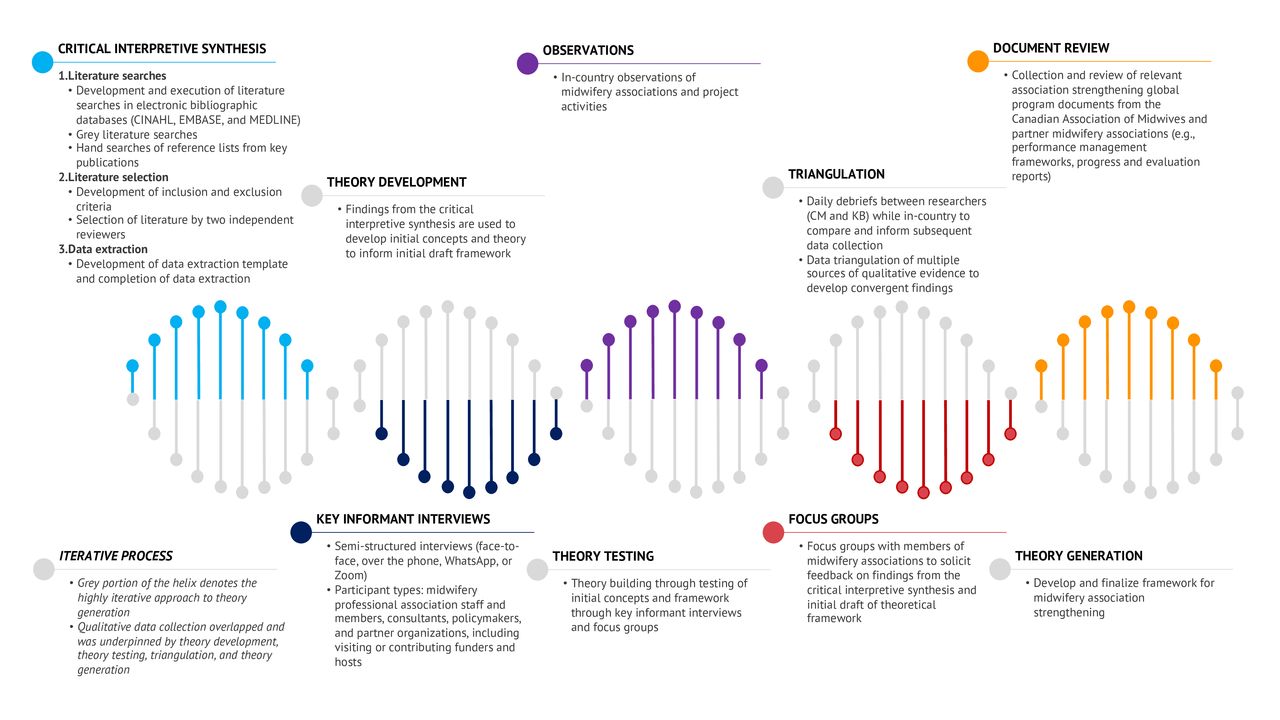
Process helix of qualitative data collection and theory generation.
Finally, researcher reflexivity was practiced through a number of strategies. Mertens principles of critical reflection for addressing constructs of power and validity of results were applied.13 We continuously critically examined dynamics of power and our geo-social positioning of privilege in order to mitigate its impacts on the research process and relationships with participants and avoid replicating historical patterns of oppression. A gender transformative lens was applied.
Results
Search results and article selection
The search of the electronic databases yielded a total of 4519 records, and once duplicates were removed (n=471), the remaining records (n=4048) were screened based on title, abstract and an explicit set of exclusion criteria. There were 206 potentially relevant records remaining. In addition to the electronic database searches, 27 records were purposively sampled for inclusion through grey literature and hand searches. These remaining documents (206) were assessed by the reviewers (CM and KB) for inclusion using the full text, resulting in a total of 103 documents included in the critical interpretive synthesis (figure 2).

Literature search and study selection flow diagram.
A majority of documents (60%) were published after 2015 and no documents were published before 2000. Of the 103 documents, 51% were primary research (n=53), which were mostly mixed methods research (n=21), descriptive studies (n=14), qualitative research (n=12), randomised control trials (n=5). Secondary research was primarily systematic reviews (n=13) and an observational study. The remaining documents were categorised as non-research (n=37), meaning that approaches taken in the documents were either not systematic or that methods were not reported transparently. Of the non-research documents, 21 were ‘other’ (eg, programme evaluations, toolkits, manuals, technical briefs, and strategic plans, etc), 11 were editorials and 5 were reviews (non-systematic). Most documents (n=74) included midwives, however only 21% were exclusive to the midwifery profession (n=22).
Additional qualitative evidence sources
We conducted 31 key informant (KI) interviews and 5 focus groups. Focus groups and a majority of the KI interviews occurred in Democrctic Republic of Congo and Tanzania. Remaining KI interviews were conducted by zoom to South Sudan, Haiti and Canada. Twenty-four CAM programme documents were included in the document review. We also analysed observation notes (255 pages) and audio recordings between researchers (CM and KB). The process was highly iterative such that the multiple types of qualitative data analysis were all used to inform the theoretical framework.
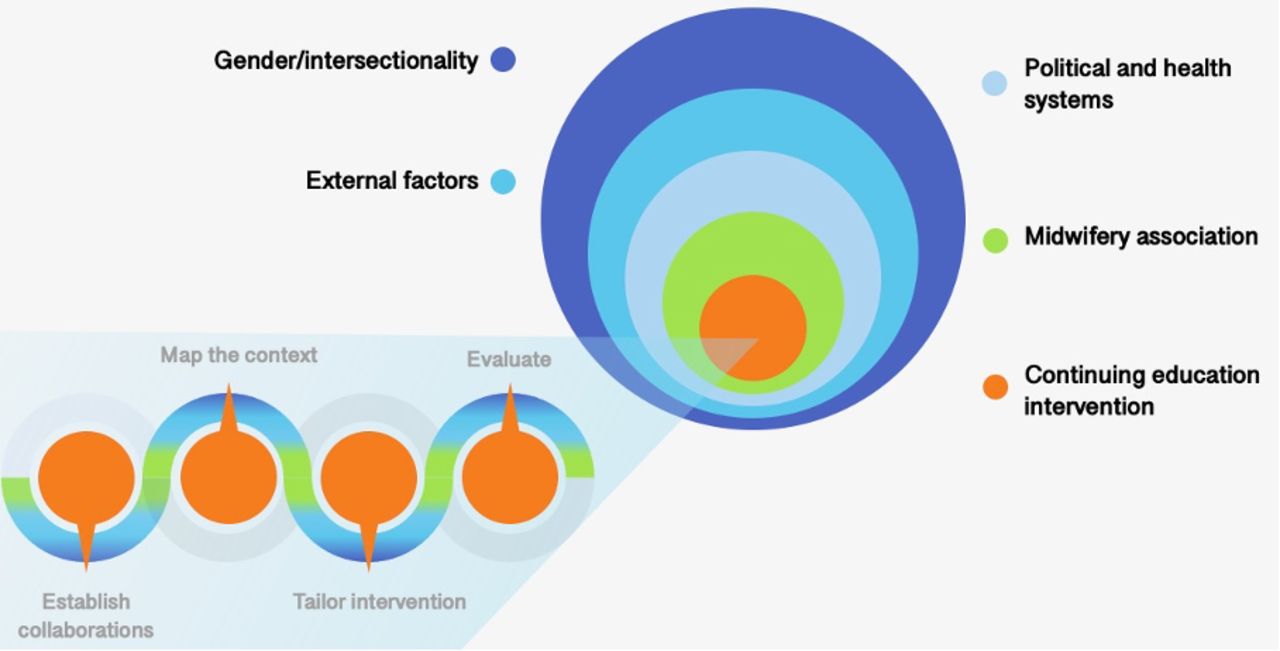
We describe below the theoretical propositions, which align with the core elements presented in our theoretical framework for key drivers of sustainable CEI for midwives (figure 3) (french see supplemental files. Figure 4 represents a subframework of the key considerations to apply during the process of planning, development, implementation and evaluation for sustainable, impactful and gender transformative CEI (figure 4) (french see supplemental files). The onion-like design, shown in figure 3, represents the interconnection of factors that impact the CEI; at the centre, is the intervention itself which is divided into a four-step process: establishing collaborations, mapping the health and political system context of midwifery including gender considerations, tailor the CEI in correspondence to the mapping and evaluation approaches that capture specific midwifery barriers and solutions. The CEI is embedded within the midwifery association, or the midwifery stakeholder, in this case, a civil society organisation; both interact with the outer context (health and political systems) and external factors that either enable or constrain the impact of the education intervention; finally, by applying a gender transformative lens, gender and its intersections are crosscutting.
Supplemental material
Supplemental material
Supplemental material
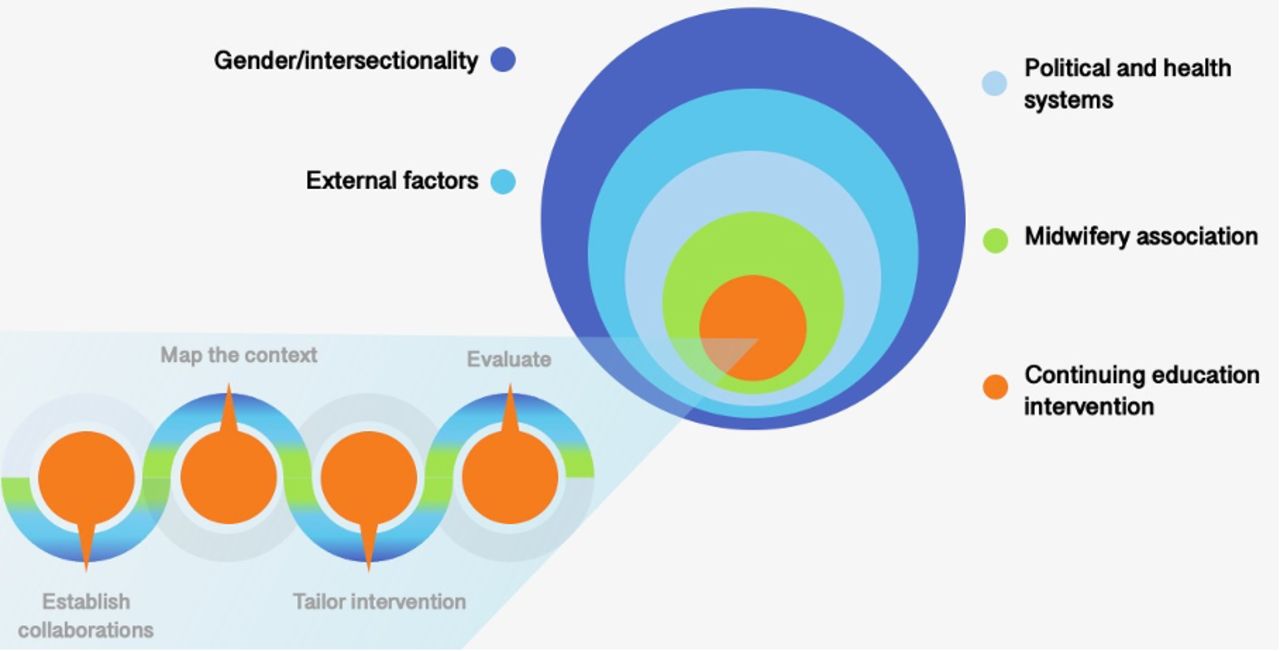
Conceptual framework for gender transformative continuing education interventions for in-service midwives.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Process for the planning, development, implementation and evaluation of gender transformative continuing education interventions for in-service midwives.
Theoretical propositions
Gender
Gender is often an assumed consideration when thinking of midwifery yet lacking explicit incorporation and assessment in CEI. Our previous research has found that the role of gender within society is integral to the political and health system context,1 14–19 and the social construction of gender impacts the value placed on women in society, and by extension midwifery.1
Gender inequities exist within midwives’ social, economic and professional spheres causing high instances of burnout, moral distress and being unsafe in the workplace. As a result, midwives describe decreased motivation to practice impacting the quality of services they provide.3 The gendered nature of the midwifery profession influences investments in midwifery education and midwifery associations’ relationships with health system decision-makers due to an overall lack of societal respect for women in many contexts.6 17 20 Finally, elements such as racism, sexism and colonialism intersect with gender or patriarchy disproportionately impacting groups of midwives in health and education systems.5 21 Despite the evidence, the scholarship for CEI for midwives does not make mention of gender transformative approaches to address these barriers that impact midwives’ ability to learn and practice.
Examples found to enable gender transformative environments include mitigating power imbalances and fostering safe spaces for all learners during the intervention by ensuring for midwife trainers, midwife mentors or midwife supervisors; designing the intervention to minimise economic impacts to participants (ie, childcare, remuneration for participation and time off work); and including a range of midwifery voices throughout the process especially those who have been oppressed by racist, colonial or patriarchal, heteronormative, systems, to explore and provide solutions for their own intersectional position in the health system such as how their gender and other intersects of oppression impact their social, economic and professional life or safety.2 In table 1, we have further detailed gender transformative considerations for the design, implementation and evaluation of interventions (french see supplemental files).
Considerations for the planning, development, implementation and evaluation of gender transformative continuing education interventions for midwives
Midwifery associations
At the heart of our framework surrounding the intervention, sits the midwifery association. Intentional partnerships with civil society or midwifery professional bodies can be an effective approach to implementing CEI in order to achieve overall goals.22–28 The core theme that underpins the remainder of our results was the positive feedback loop between the results of association strengthening and the results of the CEI. By designing, implementing and evaluating CEI, the midwifery associations were able to increase their organisation and technical capacities and their capacity to strengthen their profession in health and political systems.6 Ensuring continuous education interventions to their members resulted in midwives who felt competent to provide quality care. By extension, midwives having participated in continuous education interventions became more involved in the association further increasing the capacity of the midwifery association to respond to the needs of their members and so on. Other examples will be discussed in detail throughout the framework to demonstrate the crosscutting nature and richness of this theme.
The (association) was going out into the regions … delivering training to midwives, a whole bunch of district health officers and regional health bureaucrats and doctors gained an understanding of what “the association” was and what midwives were and (the association’s) own kind of capacity to influence things and capacity to support their members grew as an unintended benefit of those clinical skills trainings (KI#17).
Political systems
To strengthen midwifery at the service level, understanding midwifery and the midwifery association as it is placed within the broader health and political system is key to appropriately addressing the continuing education needs of the profession (see table 1).29 Policy environments either limit or enhance CEI for midwives at the service level and within the health system more broadly.6 20 Midwifery associations that housed continuing education programmes often partnered with ministries of health and other stakeholders during the process, resulting in improved relationships with dominant interest groups such as professional obstetric and neonatal associations. This cocreation of the intervention facilitated strategic links to individuals who held decision-making power and who in time became champions for the CEI and, by extension, the midwifery profession. While midwifery associations faced a general lack of political will to invest in midwives overall, they were able to make some in-roads where they had not before.
So midwifery is now known today, now known by all. Today, in all the activities that the Ministry of Health organizes in favor of the mother and the child, ___ (the association) does not miss an invitation. We always include ____ (the midwifery association) (KI#2 translated from French).
Health system
Midwives’ status and level of capacity vary greatly between and within health systems and must be mapped and understood at the ouset.1 6 The following subsections elaborate how the health system (governance, service delivery and financial arrangements) impacts the ability of midwives to integrate the skills and knowledge acquired through CEI.
Governance
Pivotal to the integration of midwifery in health systems is their level of professional autonomy or self-governance. When midwifery regulation is managed in combination with other professions (such as nursing), professional roles are unclear, diluting their presence and impact within delivery arrangements.1 Regulatory systems that autonomise midwifery also ensure that the public is protected and quality of midwifery care is monitored including continuing education competencies. The midwifery participants in the study were at various levels of self-governance and described this as a primary barrier to representation of the profession, ergo women, at various leadership levels including decision-making and policy positions (local, international). Like a domino effect, limited or no midwifery leadership resulted in less lobbying power for self-regulation, and appropriate delivery of midwifery services including the integration of continuing education competencies.3 4 20 30
Leadership training in conjunction with CEI has been used as a mitigation strategy within CEI for poor uptake of clinical skills and resulted in increased skills integration in institutions.31–37 Even when no official leadership training was given, midwives’ direct involvement with CEIs implemented principally within the midwifery association, provided them with self-awareness as a midwife, communication and advocacy skills and a new understanding of their profession within their health system and internationally. This was much more evident when midwives had gone on to become CEI facilitators, mentors or played other more consistent roles within the CEI.
It gives us, even now I can stand even in front of the gynecologists, and I can talk, because I'm a midwife, and I know these things. It’s helped a lot (KI#15).
In essence, autonomising and empowering midwives in the continuting education process led to an organic growth of midwifery leaders who became motivated and competent to advocate for their profession in multiple policy arenas. These leadership competencies and experiences in turn improved the technical expertise of the midwifery association and their ability to address systemic barriers to the integration of midwives at the health system level. For example, midwives were able to advance regulatory legislation that had been otherwise stagnant, sitting with decision-makers or hospital management to ensure that midwives were appropriately supported.
But with the Association, since we are now united, we can see the problems we face at the level of the institutions, at the level of the department, and then we meet to see how we can improve our activities (KI#11 translated from French).
Delivery arrangements
The effects of developing leaders within midwifery associations, is that as an entity, the associations were able to demonstrate the potential of midwifery-led CEI to improve midwifery leadership contributing to the integration of the profession. Poor infrastructure, lack of equipment, electricity or safety negatively impact midwifery practice and the morale and health of midwives.3 4 38–41 Together, increased leadership capacity of the association and midwives resulted in better service arrangements and practice environments for midwives. The following subsection describes how this was achieved at the service level through delivery arrangements.
With regards to post-CEI, midwife participants reported an increase in confidence and competence to practice their new skills at the service level, however, poorly structured service delivery arrangements for midwives threatened sustainability and integration of skills over time. Solutions to these system barriers for midwives came from participants who described increased leadership competencies due to their participation in CEI. For example, midwives trained as facilitators, supervisors or mentors described increased competence and confidence to advocate for midwifery within their hospitals or those of their mentees and to educate other healthcare professionals and decision-makers regarding the role of the association and the profession (see table 1). This could be as simple and impactful as ensuring that neonatal resuscitation equipment is available at the bedside for midwives to resuscitate a baby instead of carrying the neonate to the paediatric department, advocating for increased privacy for clients given birth through changes in labour and delivery infrastructure and/or teaching emergency skills to other colleagues. At the organisational level, midwifery associations were then able to better understand the needs of their members, providing mentorship, clinical support and advocacy such as proper deployment, remuneration and to access equipment (eg, neonatal resuscitation). Midwifery mentors described the positive experience of integrating change at the service level:
So it helped us to really improve the working life of our colleagues and to strengthen it further. So we're now strengthening the provider on the ground by identifying their weaknesses and we're trying to work on them to bring them back, to strengthen them further (KI#2 translated from French).
Financial arrangements
Considerations for financial arrangements within CEI did not emerge from the literature synthesis except to discuss the cost efficiency of on-site provision of training.42 However, we were able to garner further insight into the impacts of poor financial arrangements and midwives’ ability to integrate new skills, including how continuing education can positively impact midwives’ financial security. See table 1 for a description of gender transformative approaches to evaluation of these outcomes.
In our study, financial arrangements varied greatly between systems such as private insurance, donor contributions, taxation and so on. Midwives who worked within the private sector had greater financial security compared with their publicly funded counterparts, who described frequent pay gaps and decreased professional motivation and morale. Midwives were generally underpaid, and often earning well below a living wage. In some instances, midwives went without pay for months due to ruptures in funding flows or because their position was not recognised within the government’s payroll due to again to lack of self-governance.
They have to do this in an environment where those midwives are not getting paid, and when and if they get paid, they get paid probably like $15.00 (USD) per month. So, even the salary they do receive it, it’s not enough for them to survive (KI#24).
The hospital’s reliance on fee-for-service model in these contexts limited the quality and timeliness of care a midwife could provide, as clients often did not have adequate funds to receive care. Midwives described how this predicament created tension and deteriorated the client-midwifery relationship, causing mistrust and trauma for both midwives and families. One midwife told of how she personally paid out-of-pocket so that her client could receive life-saving care:
She witnessed a uterine rupture and the woman, and her family had no money. The midwife paid 3000 Congolese francs (5$USD) and the woman received a blood transfusion and did not die (translated from French, FGD 1)
These barriers were countered by stories of increased financial literacy and economic stability for midwives who, by virtue of their involvement with midwifery associations and CEI, increased their level of expertise, and subsequently their financial stability. This included writing of grants and project proposals and managing the budget aspects of activities. Furthermore, midwives involved in the coordination of continuing education activities described increases in job opportunities to work for other organisations or divisions within the government for similar continuing education activities. Finally, from the organisational perspective, midwifery associations increased their membership numbers and opportunities for other funding, which provided operational funds to pay core staff who had previously been volunteering. This improved the associations’ ability to advocate for better financial arrangements for their profession:
Midwives will be better equipped to negotiate with government policy makers, and to advocate for strengthened comprehensive midwifery services, including issues of recognition and fair pay, contracts for re-engaged midwives (KI#2).
External forces
External shocks to the system, such as pandemics, climate change, global economic crises and natural disasters tend to shift resource allocation away sexual and reproductive health services delivery, further impacting the funding for and sustainability of CEI. The COVID-19 pandemic is greatly impacting midwifery, however, our observations identified ways in which it presented windows of opportunity to raise the visibility of midwifery associations. Leaders were able to react quickly to educate their members on the use of personal protective equipment, infection prevention and control and participate in the development of training guidelines for frontline workers.
Planning, development, implementation and evaluation of CEI
Five themes emerged regarding process considerations for the planning, development, implementation and evaluation of CEI for midwives (table 1). These were: (1) position midwives within their specific political and health system’s context, so that interventions are appropriate; (2) tailor interventions for midwifery-specific content that empowers midwives to understand the role of their profession, fosters leadership skills and increases understanding of the impacts of gender discrimination; (3) midwifery-led, midwifery only CEI foster a non-hierarchical learning environment and leads to relevant and safe supports for better integration of skills, and by extension facility functions; (4) understand the specific challenges and solutions to supporting skills integration of midwives, while incorporating evaluations with a highly explanatory component and (5) house CEI for midwives within a midwifery association as an effective approach to longer term integration of skills and improvements to the profession in the health system (table 1).
Discussion
Principal findings
We present an evidence-informed conceptual framework for the gender transformative education of in-service midwives, which aligns with the core elements described in the theoretical propositions. At the centre of our conceptual framework, it is the process of conception, implementation and evaluation of the intervention which in turn is nested within the midwifery association as a partner, collaborator or host. Both components are seated within the context of midwifery in a particular health and political system. A gender transformative lens is applied to each component. The midwifery association is positioned between the intervention and the system in order to support the competencies of midwives by simultaneously enabling the profession to achieve its potential in all four of the UN’s investment areas; training, leadership, health workforce and midwifery autonomy; ultimately leading to increased access to SRHR.
Underpinning all considerations in our framework is the impact of gender inequalities within the structure of midwifery (poor remuneration, lack of professional recognition, little midwifery leadership, violence and personal safety, etc) that greatly contribute to burnout and moral distress and severely cripple midwives’ capacity to integrate new skills.3 4 41 43 44 In addition, mapping the health and political system context of midwifery, the planning, development, implementation and evaluations of CEI must begin to incorporate a feminist process and lens that critically examines gender and other intersects (eg, ethnicity, indigeneity and disability).8 45 Examples in our results provide guidance and first steps. Furthermore, we propose the value of explanatory evaluation approaches to understand and evaluate the impact of oppression, discrimination, unanticipated impacts and specific elements regarding the midwifery contexts of the intervention.41 45–47
Approaches that foster midwifery leadership are elements that must begin to be incorporated into midwifery-specific interventions when working to improve the status of midwifery and, thus, SRHR.30 32 37 44 48 When these elements were explicitly integrated into the inception and operationalisation of activities, intervention hosts (midwifery associations) and midwives were empowered to become leaders and impact the governance of midwifery within and outside of constitutional structures.6 Our findings demonstrate that when empowerment was present, there were sustainable shifts with regards to midwives’ work environments and financial security and to midwifery associations’ capacity to improve the status and integration of the profession within political and health systems.27 28 49–52 Participants described how interventions created by and implemented for midwives provided the tools and capacity to address the inequalities faced by their profession; the midwifery association became their support system and a lifeline to sustain this work.
Strengths and limitations of the study
The main strength of the research is the richness of the data gathered through multiple sources of evidence. There is a growing body of research evidence regarding the role of midwifery associations and strengthening midwifery in health systems, yet to our knowledge, our study is the first to generate theory and a conceptual framework that incorporates gender, health and political system factors and the role of midwifery associations when creating, implementing and evaluating CEI. The use of multiple sources of evidence meant that we did not have to rely on the very limited relevant published research literature, but rather used it as one of many inputs to theory generation.
Our main limitation was with respect to travel. We encountered a few challenges with visiting each of the midwifery associations that CAM is currently engaged in partnerships with due to context-specific issues of political instability and logistics related to travel to fragile states. While we made sure to collect qualitative data from these contexts through other virtual means, we recognise that fieldwork and observations are an important source of evidence, and important to understanding midwifery associations working in challenging contexts.
Conclusion
Investments in the midwifery profession will be necessary in order to address the pressing need for quality SRHR services globally. Our framework supports the development of evidence-informed CEI for midwives using gender transformative approaches and reinforces midwifery associations as an important strategy to strengthening the profession across health and political system arrangements and improving inequities.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Hamilton Integrated Research Ethics Board (HiREB, protocol number 7489) at McMaster University in Hamilton, Ontario, Canada and Laurentian University’s Research Ethics Board (LUREB protocol number 6018380) at Laurentian University in Sudbury, Ontario, Canada. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to first and foremost thank our dear esteemed colleague Sebalda Leshabari RN/M MPH, PhD, who sadly passed away before this manuscript was produced. Her contributions to our research included reviewing the proposal, facilitating data collection and member checking in Tanzania and reviewing initial results. Her dedication to midwifery and leadership in her country of Tanzania have greatly advanced her profession and overall access to SRHR. Thank you, Dr Leshabari. We would also like to thank our colleague from the South Sudan Nurse and Midwifery Association, Achiga Patrick. Achiga Patrick supported data collection within South Sudan and contributed greatly to our association’s strengthening study and manuscript. This work allowed us to continue the development of this manuscript. Your contributions and support for the midwifery association strengthening research, the companion to this study, was an important contribution to the development of this second study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Stephanie M Topp
Twitter @DrKirstyBourret, @MattisonPhD, @LizDarlingRM
Contributors KB: is acting as the guarantor, co-developed the research proposal, co-conducted the critical interpretive synthesis with CM as well as all other sources of data collection. KB led the team in the analysis of all sources of data; prepared the initial synthesis, concepts and framework and incorporated the team’s feedback and revisions; prepared the initial draft of results for research team and incorporated feedback and revisions; prepared initial draft of manuscript and incorporated feedback and revisions. CM: co-developed research proposal, co-conducted critical interpretive synthesis with KB and other sources of data collection; participated in analysis of all sources of data; revised and reviewed the synthesis of data, initial concepts and framework; created the images of the frameworks; conducted the first revision of results and manuscript and worked extensively with the research team on the finalization of results, framework and manuscript. EH: participated in team meetings and work to refine and develop the analysis of all sources of data; participated in the development of framework and concepts; revised and translated the results to French; revised the manuscript. AK: reviewed and approved the research protocol; oversaw and facilitated data collection (interviews, focus groups, observations, document collection) in the Democratic Republic of Congo; co-facilitated member checking of framework; participated in meetings to revise framework and results in French. SS: supported data collection in Tanzania (interviews, focus groups, observations, document collection); reviewed framework and concepts as well as contributed to manuscript. MC: reviewed and contributed to synthesis of the initial results; participated in team meetings to review the framework and manuscript. ED: supported proposal development and collaboration with CAM; participated in the analysis of the results and reviewed manuscript. JR: co-developed research proposal; organized collaborations and in-country data collection plans in Democratic Republic of Congo and Tanzania as well as distance data collection in South Sudan and Haiti; reviewed the concepts and framework; contributed to the writing of the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.