Article Text

Abstract
Background ‘Resilience’, ‘self-reliance’ and ‘increasing country voice’ are widely used terms in global health. However, the terms are understood in diverse ways by various global health actors. We analyse how these terms are understood and why differences in understanding exist.
Methods Drawing on scholarship concerning ideology, framing and power, we employ a case study of a USAID-sponsored suite of awards called MOMENTUM. Applying a meta-ethnographic approach, we triangulate data from peer-reviewed and grey literature, as well as 27 key informant interviews with actors at the forefront of shaping these discourses and those associated with MOMENTUM, working in development agencies, implementing organisations, low-income and middle-income country governments, and academia.
Results The lack of common understanding of these three terms is in part a result of differences in two perspectives in global health—reformist and transformational—which are animated by fundamentally different ideologies. Reformists, reflecting neoliberal and liberal democratic ideologies, largely take a technocratic approach to understanding health problems and advance incremental solutions, working within existing global and local health systems to effect change. Transformationalists, reflecting threads of neo-Marxist ideology, see the problems as inherently political and seek to overhaul national and global systems and power relations. These ideologies shape differences in how actors define the problem, its solutions and attribute responsibility, resulting in nuanced differences among global health actors in their understanding of resilience, self-reliance and increasing country voice.
Conclusions Differences in how these terms are employed and framed are not just linguistic; the language that is used is reflective of underlying ideological differences among global health actors, with implications for the way programmes are designed and implemented, the knowledge that is produced and engagement with stakeholders. Laying these distinct ideologies bare may be crucial for managing actor differences and advancing more productive discussions and actions towards achieving global health equity.
- health policy
- health systems
- public health
- qualitative study
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is a rich body of scholarship that seeks to advance application, measurement and strategies for improving resilience, self-reliance and increasing country voice in global health policy and practice.
WHAT THIS STUDY ADDS
This study problematises the assumption that global health actors understand these common terms in the same way, finding that differences in understanding are reflective of two distinct perspectives in global health, which are shaped by threads of neoliberal and liberal democratic ideologies on one hand and undercurrents of neo-Marxist ideology on the other.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The existence of conflicting perspectives on how these terms are understood—and the deeper ideologies that animate these differences—likely reflect more fundamental contestations among global health actors on the nature of the underlying problems in the field, the solutions that should be advanced, and how and which actors should be engaged and assume responsibility.
Background
‘Resilience’, ‘self-reliance’ and ‘increasing country voice’ are widely used buzzwords in global health. However, the terms are understood in diverse ways by various global health actors. Use of these terms has been constrained by a ‘linguistic crisis’1 or a lack of ‘conceptual maturity’2—insufficient clarity or consistency on what they mean. The lack of coherence may be a reflection of an actor’s uncritical application, a function of variations in interests or experiences, or more fundamental belief differences that actors hold about global health—its purpose, the processes for health advancement and the role of involved actors. An examination of the way in which actors employ common terms in global health provides an avenue for making broader perspective differences clear. Through ‘constructive destruction’3—taking apart different meanings these words have acquired as they have come to be used in global health discourse, we analyse how ‘resilience’, ‘self-reliance’ and ‘increasing country voice’ are understood across various global health actors and why differences in understanding exist. These terms were chosen for two reasons. First, the terms collectively articulate ideas that many actors in global health see as critical for improving population health outcomes and equity: building responsive (resilient), self-sustaining (self-reliant) and inclusive (increased country voice) health systems and governance structures. Second, they are central pillars of the MOMENTUM awards suite, which served as a case for this analysis. We seek to not only bring into view the dissonance between meanings of each term, but also what animates the differences that various actors in global health ascribe to them—a necessary step for engaging in meaningful debate and ultimately advancing global health’s agreed on goals.
Frames, power and underlying Ideologies in global health
A growing body of scholarship examines the role and importance of framing in global health policy in shaping the categorisation and understanding of health issues, policy responses, and global health priorities and governance.4–7 However, little scholarship has examined the ideologies that underlie and structure competing frames in global health.8 9 Ideology is a coherent and well-ordered rational system of beliefs about the social world and how it operates.10 Wilson (1973)11 advances three structural elements of ideology, which have subsequently been adopted in the framing literature12–14: diagnosis, concerning the problem definition or how things got to be how they are; prognosis, referring to the solution definition or what should be done and potential consequences; and rationale, relating to who should do it and why.
Ideology underlies frames, serving as a ‘mediatory’ that connects framing and power structures.15–22 Frames draw—either implicitly or explicitly—on broad ideational paradigms of health as well as the international system’s power distribution, highlighting how a mixture of power, ideas, agency and structure shape the frames that are produced, and ultimately the global health policies that are advanced.4 This ‘deep core’ ideology shapes what is sayable, doable and thinkable in global health.4
Scholars have identified three distinct ideologies in global health: neoliberal, democratic liberal, and neo-Marxist. Some argue that neoliberalism, which prioritises market-based policy responses, liberalisation of healthcare, privatisation and idealisation of risk and responsibility, is a ‘deep core’ ideology that has dominated global health over the last three decades.23–26 Those embracing a democratic liberal ideology believe that healthcare should be a right for all people, equitably financed and implemented through a social insurance system providing universal health coverage.27 Despite neoliberal and democratic liberal ideology differing in the value placed on efficiency versus rights, respectively, both see value and possibility for change within the current power structures.
This is in contrast to neo-Marxist ideology, which is fundamentally dissatisfied with existing political, economic and social systems that maintain divisions between the most and least powerful.28–30 Historically, neo-Marxist ideology was largely reflected by the efforts of national leaders, writers and activists who fought for independence and sovereignty, seeking to dismantle colonial empires and liberate countries from western control.31–40 More recently, elements of neo-Marxism are reflected in calls to ‘decolonise global health’,41–45 where proponents demand a transformational change in global and national health practice.
Fundamentally, these ideologies differ on the value and legitimacy of current global and national structures, and the extent to which actors should work within or upend existing power structures in advancing global health goals. While neoliberal and democratic liberal ideologies see the value of and seek to work within current structures, neo-Marxist ideology questions the very legitimacy of these structures and wish to dismantle them.
Methods
Data
We employed a case study of the MOMENTUM suite of awards—a U.S. Agencyy for Internationl Development (USAID) sponsored, 3 year (2021–2024) project that seeks to accelerate reductions in maternal, newborn and child mortality and morbidity in high-burden countries. The MOMENTUM awards are applied in low-income and middle-income countries (LMICs) in East, West and Southern Africa, as well as South and South-East Asia. Collectively, the MOMENTUM awards seek to build on existing evidence and science to develop new ideas, partnerships and approaches, and strengthen health systems. USAID funded this project, which encompassed a number of studies,46–48 given the three terms’ centrality to the aims and strategic interests of the MOMENTUM suite of awards, and their frequency in partner organisational and strategy documents. For example, some of the awards specifically aim to develop health resilience to counter the effects of fragility, strengthen local and country voices, expand global technical leadership, or support leadership of health systems and institutions. Beyond MOMENTUM, this analysis is relevant to a boarder global health audience given the diversity of global health actors involved in the MOMENTUM case—a bilateral donor, key implementing organisations located in high-income countries (HICs) and LMICs, and LMIC governments and service providers— working on a common global health issue.
We triangulated data from peer-reviewed and grey literature to examine discourses in both research and practitioner global health circles respectively, as well as key informant interviews (KIIs). To examine the peer-reviewed literature, three interrelated search strategies were developed and executed on 6 October 2020 using the search terms in online supplemental annex 1 in PubMed, Embase, Ovid Global Health databases. The search strategy development was iterative using the three words and guided by index articles to select related words that were pulling articles relevant to our inclusion criteria. We retrieved 4694 articles from the peer-reviewed literature and uploaded into RefWorks for review (3364 for self-reliance, 769 for resilience, 531 for decolonisation with links to increasing country voice, and 102 articles for more than one term). Three researchers conducted a title and abstract review in RefWorks, with one researcher reviewing each title and abstract. Through the review process, we subsequently significantly narrowed the number of article included to those that contained one of the three specific words of interest. Online supplemental annex 2 outlines the criteria used to select the articles. In line with the ethnographic nature of the literature search,49 criteria were developed iteratively as literature was reviewed. Online supplemental annex 3 provides a table for the articles remaining after the title and abstract review. While the ‘increasing country voice’ literature search began from a ‘decolonisation’ angle, the subsequent narrowing of the articles was limited to those that explicitly focused on ‘increasing country voice’ given the research team’s discovery that the two terms held substantially different heritages and purposes. Moreover, the recent decolonisation discourse was likely influencing and/or reflective of some of the understandings across all three terms, not just increasing country voice. Following the initial search, a second search for relevant grey literature was conducted via Google for each of the three terms, using the search terms used in the initial search. For the ‘increasing country voice’ term we were intentional about identifying grey literature that was not necessarily linked to decolonisation, which was the focus in the initial search. Additional peer-review and grey literature was also identified using snowballing approaches from the reference list of articles, including relevant publications prior to 2000 and after 2020.
Supplemental material
In addition, 27 semistructured KIIs (tables 1 and 2) were conducted with leaders within the MOMENTUM awards suite, leaders in other global health organisations, and leaders shaping respective term discourses. Using a purposive selection strategy, we identified these individuals through the organisational chart of the MOMENTUM consortium, our literature review and interviewee input. KIIs occurred via zoom between 2 February 2021 and 29 April 2021, each lasting for an hour, transcribed on permission, deidentified and password protected. Each respondent was asked about the origins of one or more term(s) in global health discourse and their evolution over time, how they defined and understood it, any challenges to and/or critiques of their dominant understandings they observed in global health and any practice or policy implications of their understanding on power distribution in global health. We continued interviews until we reached theoretical saturation.50
Key informant organisational affiliations
Key informant characteristics
Data extraction and analysis
A data extraction form was developed in Microsoft Excel to review and analyse the collected data. Terms on the extraction form (online supplemental annex 4) corresponded to a series of subquestions developed from the overall research questions and drawn from the power, ideology and framing literatures.6 51–53 This document summarised: the (1) definitions used; (2) origins and evolution of the term in global health; (3) nature of the problem; (4) operationalisation(s); (5) measurement and (6) practice and policy implications. The research team regularly discussed emergent themes and collectively identified two distinct perspectives—reformist and transformational—given their orientation to the nature of the problem, its solutions and motivational rationale. These two perspectives were then probed for key ideational principles, including the value of current systems, structure of relations and the nature of involvement of key stakeholders.
Respondent and public involvement statement
Respondents or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research given the nature of this research.
Results
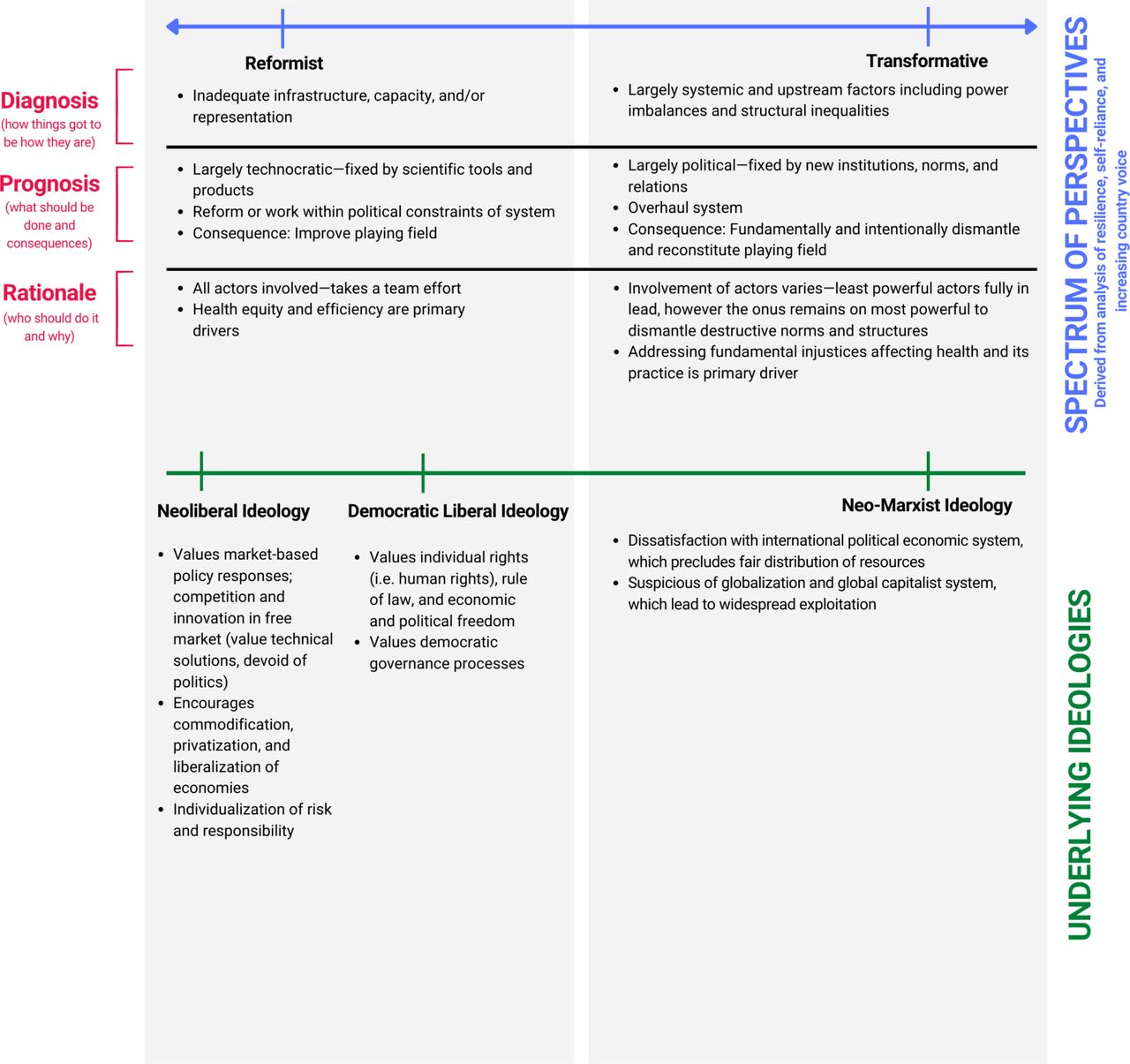
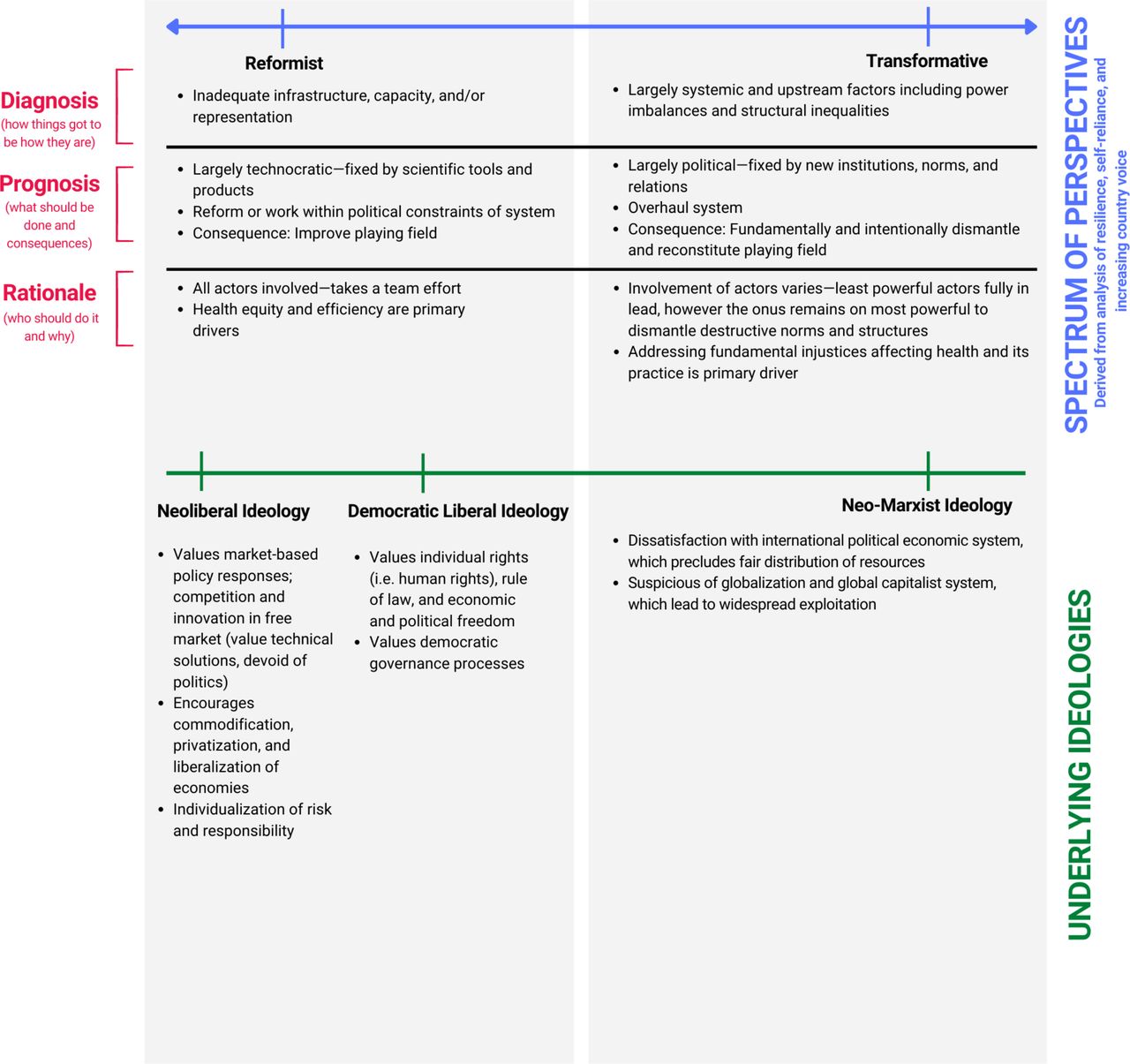
The differences in understanding of ‘resilience’, ‘self-reliance’ and ‘increasing country voice’ are reflective of the two contrasting perspectives: reformist and transformational. These differences are animated by distinct ideologies: the former reflects threads of neoliberal and democratic liberal ideologies while the latter contains undercurrents of neo-Marxist ideology. The ideas encompassed by the spectrum of reformist-transformational perspectives and their underlying ideologies are summarised in figure 1; these are derived from an analysis of ‘resilience’, ‘self-reliance’ and ‘increasing country voice’. Online supplemental annexes 5,6 and 7 examine each of the terms respectively across the diagnostic, prognostic and rationale dimensions. Across the three terms, those who hold a primarily reformist perspective conceptualise the problem as predominantly down-stream and addressed via largely technocratic solutions. They embrace market-based and/or democratic orders with a desire to incrementally reform or work within current power structures. In contrast, transformationalists describe the problem as predominantly upstream and fundamentally demand a different system as the solution. They reject the existing international economy and seek to overhaul existing power structures.
{kind=link}
Summary of ideas encompassed by the reformist and transformational perspective spectrum, as well as their underpinning ideologies.
These perspectives are not binary but rather lie on a spectrum. We detected variance not only among but also within individuals and organisations in terms of their embrace of reformist and transformational perspectives. For example, sometimes individuals articulated a transformational perspective in their understanding of the nature of the problem, but then advanced solutions that were reformist in nature. We present each term—resilience, self-reliance and increasing country voice— in turn, examining the ways in which reformist and transformational perspectives are reflected along diagnostic (how the problem is defined), prognostic (which solutions are advanced) and rationale (who is responsible) dimensions.
Resilience
In defining resilience, global health actors differ in what they see as the root problem and the predominant nature of ‘shock(s)’ that affects the health systems, the extent to which software versus hardware elements should be engaged for the solution, and who takes responsibility for building resilient health systems. These distinctive perspectives—along the reformist-transformational spectrum—reflect underlying ideological differences.
Diagnosis
Those holding a reformist perspective consider the root problem of inadequate health system resilience to be insufficient self-reliance (ie, specifically, a lack of funding and/or capacity) (I4, I9) and/or deficient health security (I4, I7). Accordingly, resilience is a means to strengthen health security, ensuring that countries are able to withstand and adapt to shocks.54 Furthermore, reformists, while acknowledging a range of possible shocks, consider shocks to the system as primarily acute and often catastrophic in nature.55–57 Examples include disease outbreaks,58 59 insecurity,60 and natural and man-made disasters.61 62 This is emphasised in USAID’s Global Health Resilience BluePrint, underscoring the agency’s experience in ‘preventing, preparing for, responding to and recovering from a range of infectious disease outbreaks’, including the global HIV epidemic, the Ebola outbreak in West Africa, and the COVID-19 pandemic, that ‘provided lessons to inform health resilience efforts’.63 This perspective is also reflected in a majority of systematic and scoping reviews of empirical literature on the subject of health resilience.
In contrast, those holding a transformational perspective describe the root problem to be structural, such as historical colonial legacies, as well as current trade, tax, health insurance and aid systems and policies.64 Resilience is thus a means to address structural crises weakening the system, deeply embedded health inequalities and the deliberate choices that shape inadequate health system responses to structural crises and health inequalities.60 65 66 Furthermore, they tend to conceptualise shocks as chronic, slower-burning and occurring over a longer time-span. These include LMICs’ regular health systems challenges resulting from human error, dynamic political environments, dysfunctional and unclear policies, limited funding, inadequate human resource capacity and high levels of disease.67–70 There is also emphasis on shocks and disturbances arising from intentional choices made by international, national and local actors, resulting in deliberate and inadvertent consequences. These include donor conditionalities and trade agreements at the global level; election promises, government reforms and regulatory changes at the national level; and changes to citizen voice mechanisms and organisational instability at the local level.64
Prognosis
In discussing health system resilience solutions, reformist and transformational perspectives differ on the extent of cruciality of technical or political strategies. Reformists tend to focus on technical solutions for fostering resilience, most of which lie within health or closely adjacent sectors including emphasising community mobilisation, disease surveillance, integration or collaboration of sectors, partners and services.63 Some respondents emphasised how the words fragility analysis, crisis sensitivity and complexity-aware monitoring frequently overlapped discussions of health system resilience among donors and implementing partners, underscoring the technocratic approach employed (I4, I6, I9). Accordingly, reformists give priority to hardware resilience building blocks—a bias more broadly reflected in the field of global health71—including finances, infrastructure and governance understood as organisational structures and legislation (ie, hospitals, standards and surveillance systems).72 Reformists tend to stress health system stability as the ultimate goal, emphasising maintenance, control, recovery, learning and/or ‘bouncing back’ to be the key resilience outcomes73–78 (I4, I6, I7, I19). Furthermore, they stress ‘preparedness’ as a strategy (I4, I7, I9, I12). They see crises as permanent; actors thus have to be continuously prepared for the worst. The focus is on anticipating how, where and when crises will happen (ie, preparation) and what sorts of responses are pragmatic and acceptable in those extreme circumstances. A respondent working in an intergovernmental organisation explained the rationale for strengthening preparedness in countries as it relates to advancing resilience:
You know a flood is going to happen; so be prepared so that once it happens, you have the structures to respond to it and be back at where you were before the flood as quickly as possible (I7).
In contrast, transformationalists see that any approach to resilience necessitates long-term commitments to finding socioeconomic and political solutions that tackle the roots of structural violence, challenge leaders of ‘weak’ states that maintain power by controlling interactions between their country and the rest of the world, and other reasons that put populations at risk.69 Accordingly, strategies and solutions advanced for creating resilient health systems cannot be divorced from meaningful assessment of the political economy and power dynamics that produced or shaped the health system crises.64 68 69 73 79 Transformationalists tend to stress the importance of software elements—’the ideas and interests, values and norms, and affinities and power that guide actions and underpin the relationships among system actors and elements’.80 These include leadership capacity, power relations, values, relationships and organisational culture.68 Transformationalists also highlight the commitment to address a range of interconnected issues that often extend beyond the health sector (I11). Instances include, an LMICs’ dependent position in the world economy, the ‘brain drain’ of medical and other professionals because of externally promoted austerity measures, and policies that uphold user fees for medical services and medicines.69 Furthermore, those with transformational ideology question if maintenance or ‘bouncing back’ to a health system’s baseline functioning prior to shock is the right goal, given that it is likely to ignore existing challenges and deficiencies and assume that the system was in an ‘adequate’ state prior to the shock or that it even existed to begin with.81 Finally, transformationalists are wary of the constant focus on anticipating a crisis, since it likely stymies the capacity or willingness of involved actors to have a bold vision (ie, fundamentally changing power relations in the governance of health). Undue continuous anticipation of catastrophe distracts attention from deeply embedded health inequities, the choices that shape health system responses, and the ‘hard grind’ of responding to chronic stresses that do not manifest as acute shocks.82
Rationale
Reformists and transformationalists also differ on who is responsible for ensuring health system resilience; the former values equal engagement across various stakeholders and communities impacted, while the latter puts the responsibility on the most powerful. Reformists are more inclined to see the importance of engaging all relevant stakeholders, especially communities and individuals, in creating health system resilience. USAID, for example, advances a ‘whole of society’ approach in building resilience by building partnerships across public, private and non-governmental sectors. Respondents with this perspective place particular emphasis on empowering communities to have agency in building resilience:
Resilience transports us back to the community…. Resilience is only built when communities own their health and they are able to…set aside resources and able to access health facilities, clean and safe delivery, family planning methods, [and] immunization. [They] are able to demand it and find ways and be creative [to secure it] (I13).
An expert in disaster risk reduction and international development explained:
A focus on resilience means putting greater emphasis on what communities can do for themselves and how to strengthen their capacities, rather than concentrating on their vulnerability to disaster or environmental shocks and stresses, or their needs in an emergency (Twigg, 2009 in83).
A LMIC government representative underscored an individual’s agency in a resilience approach:
Resilience is the ability of bouncing back after having the worst of scenarios, like an experience that puts you down so hard and all of a sudden, even with the pain and suffering, you dust yourself and stand up (I19).
In contrast, transformationalists tend to be critical of the dominant ‘whole of society’ approach employed in resilience discussion by donors and implementing partners—cautious that it is translated in practice as coping, with more powerful actors putting undue burden on the poor and disadvantaged, expecting them to ‘draw on their internal strengths and resources’ to make up for health system weaknesses.66 Such operationalisation of resilience masks the fact that resources are far from equally shared among states and within communities.84 These actors seek to change the loci of power and foster new governance structures and relations rather than reinforcing existing, dysfunctional health systems.66
Self-reliance
The way that self-reliance is framed and the actors that employ the term have varied over time.47 While a transformational perspective of self-reliance was historically employed by LMIC actors, a reformist perspective of the term was introduced by international donors around the 1990s, eventually evolving into the current understanding of self-reliance embraced by major donor institutions (including USAID’s recent ‘Journey to Self-Reliance’ branding under the Trump administration) and implementing partners. In contrast, national governments and country non-governmental organization (NGO) staff are more likely to articulate a transformational perspective. The two perspectives differ on the problem being largely grounded in national (ie, lack of health system capacity) or global system (ie, unequal trade power) deficiencies; whether solutions necessitate improved domestic resource mobilisation and distribution or fundamentally different approaches that re-centre an LMIC’s agency; and if responsibility for self-reliance includes HIC agencies.
Diagnosis
From the reformist perspective, the implicit problem is that countries require, or are perceived to require, external support from bilateral donors in order to reach a goal. Many respondents articulated a problem definition that aligned with this perspective (I4, I8, I18, I11, I10, I21). These respondents from HICs explained:
I think, my understanding of self-reliance…means you no longer need a donor. I mean, that’s the way they [donors] understand it, because…at some point the support should end; you can’t keep on supporting a group of communities or a country forever on the same thing (I13).
…Mov[ing] us towards a situation where the countries are doing all this themselves without our external support (I11).
We used to call it decades ago when I started off in the sector as self-sufficiency, right? And then OECD [Organization for Economic Co-operation and Development] came in [and] they started using the word sustainability. And now we’re talking self-reliance. All the same things. And it’s the whole idea of getting rid of dependency (I21).
In articulating the problem, respondents holding reformist perspectives tended to attribute the dependence on external resources to national system level deficiencies, including a country’s low domestic health spending, inadequate capacity and/or lack of political will. As a respondent from a donor agency explained:
The perfect example might be [informant gives two country examples in Africa] where we know [there is] corruption or government issues… [while] there’s a lot of development that goes into those two countries, [there is] very little commitment from the governments themselves to take on some of that work that they do have…[so its about] increasing country commitment and promoting domestic resource optimization and transparency and mutual accountability between donors and country partners (I14).
In contrast, transformationalists see the problems underlying self-reliance to be generally focused on liberal, capitalist models of development, structural inequities in the world economic and political system, and the resulting, unequal power dynamics manifested in the ‘first world’ and the ‘third world’.85–88 These structural inequalities, in addition to trade and power imbalances, have resulted in financial outflows from poorer countries that are at least US$3 trillion per year or 24 times that of incoming aid.89 These outflow calculations include debt with interest, profit repatriation from foreign direct investment and capital flight, and are likely underestimated given additional, unaccounted costs associated with slave trade, climate change and the commercial determinants of health that are disproportionately shouldered by poorer countries.90 91 Several respondents residing in or originally from LMICs connected self-reliance to the independence of their countries and/or recent efforts by national champions and governments to counter the costs of global political economy on local human development (I8, I9, I18, I19).
Prognosis
Reformists emphasise working within the existing system to resolve the identified problems by fostering localisation of funding, subawards, domestic resource mobilisation, private-sector engagement and commitment from country actors. One respondent related the term to countries ‘driving the train’, where external assistance can still provide support but countries are in control of their development trajectories (I11). Historically, reformist efforts to advance self-reliance were reflected in structural adjustment programmes devised by the International Monetary Fund, which made loans to indebted countries conditional on privatisation, economic liberalisation and reductions in public expenditures;89 the proclaimed aim was to increase government spending for healthcare and innovations to enable borrowing countries to protect health spending from broader austerity measures.92
Respondents holding reformist perspectives advanced a number of solutions for advancing self-reliance, including working through local organisations, staffing local country offices with national rather an international workforce (I1, I11, I17, I20), and gradually working towards ‘graduating from assistance’ so that as a donor’s ‘funding drops off, [a country’s] domestic resources and their advocacy…increases…[enabling them to] ‘graduate out’ when they're able to cover their own costs for that area’ (I2). This perspective embraces social entrepreneurship as part of the solution—fundamentally embracing a political economy that emphasises individual agency.89 Respondents also emphasised capacity building as part of the solution to building self-reliance (I1, I2, I4, I9, I10). One from a bilateral donor commented:
We really need to make sure that we're building an organization’s capacity to be our partners, to handle the logistics and the funding that we have or to be at a place where they don't need to have our funds…[but] I don't think that there is a need to completely erase what we've started and start over. (I10).
In contrast, transformationalists desire a system overhaul and uprooting of entrenched power dynamics, including redefining trade terms (especially historically) and developing country strategies that focus on national leadership (especially presently). The solutions proposed are fundamentally emancipatory in nature. Nationally and historically, this is reflected in a call for community-led development approaches and self-reliance of individuals—particularly rural communities—from dependency on government support.93–96 LMIC leaders like Julius Nyerere, the first President of Tanzania, advocated for wealth transfer across and within nations. They advanced that the uneven tolls of the global political economy must be equalised for true empowerment of the Global South.89 More recently, LMIC leaders such as China’s President Xi Jinping and India’s Prime Minister Narendra Modi have called for self-reliance with the latter, for instance, calling for import restrictions and local manufacturing bolstering (Patel, 2021). At the international level, this is reflected in calls to change the terms of economic markets, trade and finance in an effort to rebalance global economic and political power dynamics in the postcolonial era.96–98 For example, this practically could include ‘debt cancellation, providing predictable, unearmarked budget support to enable recipient governments, and the people to whom they are accountable, to finance health systems they imagine’.89 This entails a complete reclaiming of agency and the narrative by country actors. One respondent with origins from an LMIC explained:
I use expressions like self-reliance, get them out of our country. Get them to stop doing stupid things in [a particular LMIC]. Can’t we take control of the narrative in [a particular LMIC]? (I26).
Rationale
Reformists acknowledge the need to put LMIC actors in the ‘driver’s seat’ while articulating a role for HIC actors in achieving self-reliance in LMICs by helping strengthen individual and government capacity and accountability. One HIC NGO respondent noted this:
As you strengthen that [individual capacity], you [also] strengthen government…I think international donors have put more pressure on governments to be responsive as well, and to take responsibility (I9).
In contrast, transformationalists see responsibility for advancing self-reliance to rest squarely on LMIC actors, whether national governments or local communities.99 Unless fully dictated by LMICs, HICs and agencies can’t have a role, especially not one that detracts from an LMIC’s agency. Several respondents from HICs working in donor agencies or NGOs explained how some LMICs have exhibited this approach:
Ethiopia is a good example. They’ve thrown most donors out of the country, they have their own plan for being a middle income country by 2030, upper middle income country by 2030. Now granted, they’ve got a lot of problems but at least they have their own vision that they own…. (I11).
Ethiopia and Rwanda are able to hold donors accountable and say: ‘You were committed to the Paris declaration, you said one plan, one monitoring framework, one report, etcetera…You need to live up to it and if you don’t, we don’t sign any agreement and you are out of the country’ (I9).
Increasing country voice
In their calls for ‘increasing country voice’ global health actors understand the term fundamentally differently. Reformists describe a lack of inclusiveness and democratic engagement in global health as a problem whose solution includes improving local representation and ownership with engagement by all involved actors to better understand local contexts and ultimately improve programme efficiency and health outcomes. In contrast, transformationalists see the problem rooted in racial hierarchy and capitalism with the solution being transformation of power structures with the most vulnerable voices—recipients of services—fully dictating how to best prioritise human well-being.48
Diagnosis
A reformist sees suppressed LMIC voice in global health as the absence of inclusiveness in global health governance, which includes imbalances or complete exclusion from agenda setting processes, study and programme design, and knowledge creation (I1, I23, I25).100 This stems from differential access to funding, knowledge, networks and educational opportunities.101 102 Those embracing this perspective highlight how key decision-making bodies and forums in global health are mostly represented by academics, donors, and implementing agencies in HICs like North America and Europe, with few individuals from LMICs (I14). This is in large part a result of significant differences in economic power (I5, I22) given those ‘who ha[ve] the dollar hold the power’ (I5). It is also in part driven by the need to produce quick results in-country, as well as existing project and funding proposal structures that privilege HIC actors who are most familiar with navigating the complex funding application submission and reporting systems, and leave many LMIC actors at a comparative disadvantage (I14, I22).
From a reformist standpoint, the lack of country voice is a result of little ‘local buy in and local ownership’ and inadequate efforts to ‘understand what the locals need’ given the ‘really poor understanding of the local context.’ (I15). Several respondents noted how the majority of members of the working groups of global health initiatives are white males from Europe and North America, representing donors and research organisations. One donor agency respondent described their personal experience:
We had an initial meeting and I realized that there wasn’t a single person in that meeting from any of our partnering countries and, like this is absolutely ridiculous; like why are we all coming together trying to decide what we should be focusing on and why are we not listening to our colleagues who are on the front lines and dealing with post-partum hemorrhage on a daily basis? (I14).
In contrast, transformationalists describe the problem as stemming from racialised hierarchisation of humanity and health systems, sexism, environmental racism as well as exploitative neoliberalism and the predatory nature of capitalism.41 102 103 Accordingly, seen and unseen racism, and its intersections with other systems of oppression fundamentally underlie suppression of voices with the least decision-making power.
Prognosis
Reformists view better LMIC representation in global health agenda-setting forums and shifting the decision-making locus to LMIC offices to increase country voice, as reflected by one respondent from an HIC NGO:
Elevating country voices means more [LMIC] representation in different global fora, more research where they [those from LMICs] are primary authors, more interaction with them, [and] they are in leadership positions where they can state their own opinion (I5).
Reformist ideas around how to facilitate increased local leadership is represented, for example, in Oxfam America and Save the Children’s Local Engagement Assessment Framework, which has been adapted by donor and NGO agencies working in health and other development sectors.104 It presents a spectrum of approaches that donors, partners and communities can engage in working together to shift agenda-setting and decision-making power into the hands of local actors. These range from consulting local actors on their views and preferences, to embedding them into a system that sees them as formal partners, to encouraging them to lead within jointly agreed parameters. Similarly, a Panel of Movers under the auspices of the Global Health Decolonisation Movement in Africa advances pragmatic approaches to increasing country voice.105 For example, their framework recommends global health organisations use holistic review methods when recruiting employees to reduce hiring bias against Africans and other persons who are under-represented in global health.106
In contrast, transformationalists view current operationalisation efforts of ‘increasing country voice’ to be insufficient where: ‘people have figured out the right things to say, and few actually go through the process of getting local ownership and getting the perspectives of the people on the ground’ (I5). From a transformational perspective, democratising global fora by increasing LMIC representation alone is an unhelpful goal because tokenism rather than representation is achieved. As one respondent working in a donor agency noted, one or a few people invited to join the discourse may not truly represent the country, and is more likely to reflect the voice of the most privileged in LMICs:
I don’t think that having one person is representative of the country… but again, we checked the box, right? (I10).
Rather, recent scholarship on decolonising global health describes the solution to be the removal of all forms of supremacy within all spaces of global health practice, within countries, between countries and at the global level.107 Efforts should be dedicated to creating a political economy that genuinely prioritises human well-being. This fundamentally requires ‘decolonisation of the mind’36—directly addressing the structural drivers of discrimination and barriers to self-determination that have led some HIC actors to feel superior and some LMIC actors to feel inferior.43 Such principles are encompassed in the efforts of groups like Campaign Against Racism, which seek to uncover and dismantle ‘historical connections between racism and capitalism to radically imagine a future in which sociocultural, political and economic systems work towards health equity, rather than against it’108 Specifically, this entails, for example, organising people to practice social medicine and collectivising their actions for structural change, transforming health education to make social medicine the norm for health professionals, and developing local leadership in LMICs that prepares people to lead and be change agents.109 It also necessitates creating new learning platforms in global health that safeguard reciprocal knowledge flows, with contributions from LMICs driving discussions and practice, both locally and globally.41 Other scholars drawing on Freire’s110 The Pedagogy of the Oppressed advance the need to move away from the Eurocentric cultures that insist on “‘professional’ dress, presentation of speech, modes of argumentation and ‘correct’ formats and literature to be used when disseminating ideas”.103 Rather, increasing voice requires ‘reparations, repatriation of indigenous land, abolition of oppressive systems and more’.103
Rationale
Reformists see the responsibility for increasing LMIC voice on HIC donors and actors, as noted by one HIC respondent working in a UN agency:
Richer countries and donors have to be able to provide the means that actually ensure that those voices are at the table (I11).
Several respondents embracing this perspective employ justifications that are instrumental in nature. Specifically, they advance that practices intended to ‘increase country voice’ will lead to a ‘better way to do development’ (I1). One respondent clarified this rationale, rooted in business economics:
Global health is a business with competition with people competing for dollars, and it’s expensive, we have large organisations that have operation costs and management fees and all kinds of things (I1).
Others call for ‘metrics,’ ‘checklists’ and a ‘road map’ to hold global health organisations based in HICs accountable in redressing wrongs and creating space and voice for the less powerful.111
Transformationalists, in contrast, see the onus on powerful actors to ‘lean out’ on an individual, national and institutional level to stop reproducing racist and colonialist ideologies,112 and more fundamentally transform their perspective on global health work. Specifically, seeing it as an act of justice instead of saviorism. A thought leader of the decolonising global health movement explained:
Instead of thinking about fixing the problems of people in poor countries, they [HIC actors] [need to] think of what they’re doing as an act of justice. And if you begin from thinking of it as an act of justice, then you don’t think about even saving someone else. You think about saving yourself… (I26).
Transformationalists also emphasise the agency of LMIC actors in advancing their voice. An LMIC scholar provides guidance for other investigators in low-income countries on ‘navigating the violent process of decolonisation in global health research’113:
I have tried to distill what I have seen, witnessed, experienced, or heard accounts of over the past 12 years into workable guidelines, for I have also seen that the extent of violence depends on the degree of power imbalance.
Discussion
Several articles have appeared in the past decade pointing to the inconsistency of definitions and/or calling for common definitions in the field of global health.114–116 In fact, several definitions of global health itself have been offered,117–120 with scholars varying in their articulation of and focus on the field’s aspirations, methods of research and practice, intervention strategies, geographical area and nature of the relationship between its practitioners and its recipients. This analysis builds on this literature, finding that the lack of clarity and consistency in understanding common terms in the field of global health may at least in part be driven by ideological differences among its actors.
Across all three terms, there are two distinct perspectives. A reformist perspective embraces liberal democratic or neoliberal ideologies. Those embracing the former believe in democracy as an ethical form of governance and hold human rights as an ethical paradigm; those embracing the latter value a market-based allocation of resources and the role of the private sector, and of the capitalist system more broadly. Despite differing emphases on the value of market-based economics and human rights, both ideologies embrace the idea of individual choice and the right of the individual to decide for him or herself what is best. Furthermore, both ideologies seek to achieve better health outcomes and equity by working within existing political and power constraints of global and national systems. Reformists often: articulate the problem as largely a matter of inadequate infrastructure, capacity and/or representation; propose incremental, scientific and technical solutions; and see a range of actors as ultimately responsible for improving global health outcomes. This perspective is reflective of the current dominant discourse, largely manifested in the reports, strategies and research produced by organisations within major global health donors, implementing partners and academia in HICs— relatively powerful actors in global health.
In contrast, transformationalists have neo-Marxist ideology leanings, seeking to fundamentally overhaul existing power structures. This ideology shapes the transformationalist’s framing of the problem as largely systemic and upstream. They are more likely to propose solutions that are political in nature and directly address past and current power imbalances. The transformational perspective is largely embodied by supporters of the decolonise global health movement and champions of economic nationalism in LMICs, who are uncomfortable with the status quo and highly critical of the dominant global health discourse. The former tend to be based in HICs, with many originally from LMICs and working within academic institutions; the latter tend to be representatives in LMIC governments or local organisations working closely with these governments. This perspective tends to be held by those relatively less powerful in global health.
The existence of conflicting perspectives on how these terms are understood—and the deeper ideologies that animate these differences—likely have significant implications on the acceptability, uptake and sustainability of global and national health policies and programmes. For example, a global health actor with a reformist perspective is likely to face difficulty securing buy-in and engagement with partners and stakeholders holding a transformational perspective. These underlying clashes may not only lead to confusion and misalignment, but also resentment and distrust. Such conflicts, among and within donors, implementing and government partners, researchers and population targets, are likely to result in, and indeed may explain why particular policies and programmes in global health achieve non-optimal acceptability, effectiveness and health outcomes.
We do not seek definitional consensus on the three terms examined in this analysis. In fact, given our findings, we believe this to be a futile exercise—and perhaps even undesirable given the value of perspective plurality. These definitional differences are at least in part driven by deep-seated ideological differences, which are difficult to alter. Rather, this paper highlights three key takeaways. First, it is crucial to be aware of the spectrum of beliefs present in global health and the key ideas that underly their differences. The ideologies uncovered in this analysis point to distinct ideas about the underlying problems, solutions and who is responsible for their addressal in global health. These belief patterns go beyond understanding definitional differences in three commonly used terms in global health; they underlie and offer clear perspective on the very different ways global health actors think about the nature of the problems, the policies and programmes they believe should be advanced, and who bears responsibility to improve population health outcomes and equity.
Second, an actor’s ideology interacts with and is shaped by power, which manifests, for example, in an actor’s location of residence, control over resources, perceived decision-making capacity, place and type of training, as well as the institutional and societal structures that he or she must operate within. This has implications for why particular understandings get advanced (or not) and by whom. Dominant understandings of terms—advanced by those in power—shape the way interventions are designed and implemented, the knowledge that is produced, and the nature of interactions and engagement across stakeholders in global health. These become institutionalised over time. Accordingly, we must recognise these words as power and value-laden—not merely technical terms.
Finally, and perhaps most crucially, actors in global health must become more intentional and critical about how they employ key terms. What do we actually mean in seeking to improve resilience, support self-reliance and increase country voice? Explicit and clear communication of our own understandings provides an avenue for making perspectives differences across the reformist-transformational spectrum clear. This clarity opens up the possibility for productive dialogue on how to effectively manage actor differences, rather than seek or force consensus. The process of productive deliberation is necessary for optimal decision-making and collective action, which may ultimately help improve global health’s existing fragmentation and dysfunction.
This analysis has several limitations. It has limited generalisability given that most of the KIIs are affiliated with the MOMENTUM suite of awards and/or those working in academic circles. None of the interviews were conducted with members of marginalised populations benefiting from development programmes, non-traditional partners, advocacy groups or civil society. Furthermore, we conducted 27 interviews, which is an insufficient number to make strong generalisations about the extent to which certain perspectives are represented by certain actors (ie, those working in USAID, those residing/working in an LMIC); however, supplementing interviews with extensive literature helped address this. Also, the initial literature search around ‘increasing country voice’ began with a ‘decolonisation’ angle, which limited the number of articles that were included and reviewed. The research team subsequently sought to address this by conducting a supplementary literature search that examined ‘increasing country voice’ more broadly, without linkages to decolonisation or the decolonising global health movement. Finally, we did not review non-English literature, which may have excluded key perspectives.
Conclusion
The field of global health would benefit from a closer examination of the terms used and how they are understood by its actors. The various meanings that a word takes on may be driven by distinct actor ideologies, which are hidden and often only discussed implicitly at most in studies of global health policy and governance. Laying these ideologies bare offers actors the opportunity to collectively reflect and debate how to achieve better health outcomes and equity.
By analysing three commonly employed terms in global health and through an examination of a microcosm of global health actors—those working within and around the MOMENTUM suite of awards, this study reveals the ideological spectrum that likely exists in the global health field. We find that ideological differences shape the various understandings that ‘resilience’, ‘self-reliance’ and ‘increasing country voice’ take on. However, more than just explaining differences in how the three terms are understood, these distinct ideologies are most likely driving more broad and fundamental contestations among global health actors on the nature of the underlying problems in the field, the solutions that should be advanced, and how and which actors should be engaged and assume responsibility. While ideological differences among actors are unlikely to be eliminated, it is through awareness of their existence and productive deliberation that it may be possible for fundamental disagreements to be effectively managed in ways that enable advancements in global health’s agreed on goals: improvement of health outcomes and equity.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but Institutional Review Board Office of Johns Hopkins Bloomberg School of Public Health. Communication of exemption was on 29 September 2020. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors to wish to acknowledge Johns Hopkins Welch Medical Library librarian Rachael Lebo for her assistance in developing and executing the comprehensive search strategy for this study. The authors also thank the anonymous reviewers, Jim Ricca, Cory Wornell and Zema Mirza for reviewing a draft of this manuscript and providing constructive comments, as well as the key informants that participated in this study for the time and valuable insights they provided. Editing assistance was provided by ReVision: A Scientific Editing Network at Johns Hopkins University.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @yrshawar
Contributors YRS and JS conceptualised the project. YRS conducted the interviews; MM jointly conducted a portion of the interviews. YRS, RN, MK and MM developed and conducted the literature search and extraction. All authors participated in the analysis and interpreting the results. YRS wrote the first draft; RN, MK, MM and JS provided extensive feedback on the paper.
Funding This study was made possible by the generous support of the American people through the US Agency for International Development (USAID) under the terms of the Cooperative Agreement #7200AA20CA00002, led by Jhpiego and partners.
Disclaimer The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government.
Competing interests The second author was an independent consultant for MOMENTUM on a different topic during a portion of this study. There are no conflicts of interest for the other listed authors.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.