Article Text

Abstract
Introduction Poor access to water, sanitation and hygiene (WASH) services threatens population health and contributes to gender and social inequalities, especially in low-resource settings. Despite awareness in the WASH sector of the importance of promoting gender equality and social inclusion (GESI) to address these inequalities, evaluations of interventions focus largely on health outcomes, while gender equality and other social outcomes are rarely included. This review aimed to collate and describe available research evidence of GESI outcomes evaluated in WASH intervention studies.
Methods We applied a systematic mapping methodology and searched for both academic and grey literature published between 2010 and 2020 in 16 bibliographic databases and 53 specialist websites. Eligibility screening (with consistency checking) was conducted according to predetermined criteria, followed by metadata coding and narrative synthesis.
Results Our evidence base comprises 463 intervention studies. Only 42% of studies measured transformative GESI outcomes of WASH interventions, referring to those that seek to transform gender relations and power imbalances to promote equality. A majority of studies disaggregated outcome data by sex, but other forms of data disaggregation were limited. Most included studies (78%) lacked a specific GESI mainstreaming component in their intervention design. Of the interventions with GESI mainstreaming, the majority targeted women and girls, with very few focused on other social groups or intersectional considerations.
Conclusion The review points to various areas for future primary and secondary research. Given the potential contribution of WASH to GESI, GESI considerations should be incorporated into the evaluation of WASH interventions. Regular collection of data and monitoring of GESI outcomes is needed as well as developing new and testing existing methods for monitoring and evaluation of such data.
- Review
- Public Health
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Globally, interest in improving and promoting equality and inclusion is growing. However, this interest has not completely translated into explicit attention to evaluating gender equality and social inclusion (GESI) outcomes in water, sanitation and hygiene (WASH) and existing reviews largely focus on health outcomes.
WHAT THIS STUDY ADDS
This review collates the literature on a myriad of GESI outcomes in the context of WASH interventions and highlights knowledge gaps and clusters in the evidence base. We further emphasise the ways that WASH interventions can lead to transformative outcomes, which is an increasing area of focus in global health, including related development interventions.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This systematic map was not set to evaluate the impacts of WASH interventions on GESI outcomes, but the evidence collated in this work provides a basis for such investigations. Future research can use the evidence base collated in this map to determine which WASH interventions work as intended for GESI outcomes. This will help to fully realise the potential returns of WASH investments and will better equip us to challenge harmful gender norms and power relations that hold societies back from achieving gender equality and other forms of social inclusion.
Introduction
Poor access to water, sanitation and hygiene (WASH) services threatens public health and contributes to gender and social inequalities.1 2 Due to gendered norms and practices related to water, women and girls bear the burden of water fetching and management within the household in many countries.3 4 This is linked to health outcomes such as musculoskeletal injuries,5 psychosocial stress6 7 and gender-based violence.8 This unpaid work can also be extremely time-consuming, constraining time for productive, educational or leisure activities.9 10 Women and girls also face cultural taboos, discriminatory norms and health risks related to poor sanitation, particularly in the case of menstrual hygiene management.11–13 This is a barrier to girls’ participation in educational opportunities and negatively impacts dignity and self-esteem.14 Despite disproportionate impacts, women and marginalised groups often have less say in the delivery and management of WASH services.15
In addition to gender, inequalities related to accessing safe WASH services arise based on disability, age, ethnicity, caste, religion and other social identities.16–19 People with disabilities often face significant challenges accessing WASH services18 and people experiencing homelessness are often denied their rights to safe water and sanitation.17 These inequalities can be particularly pronounced when gender and other social identities intersect,13 19 such as in the case of displaced women and girls seeking safe and private facilities for menstrual hygiene management.20 Recognition of these inequalities has translated into attention to gender equality and social inclusion (GESI) mainstreaming in WASH programmes, thought to contribute to both more sustainable WASH services, as well as (women’s) empowerment.21
In the context of this review, we focus on ‘inclusive’ and ‘transformative’ outcomes. Inclusive outcomes seek to address the different needs of girls, boys, women, men and other social groups, ensuring access for all. These can be seen as accommodating gender or other social differences as they do not explicitly seek to redress gender inequalities or social exclusion. Transformative outcomes explicitly focus on how power relations are challenged, and how stereotypes, harmful gender attitudes and social norms are changed to promote GESI,22 23 such as through increasing women’s meaningful participation in WASH decision-making processes (see the review protocol24 for more details).
Despite the potential contribution of WASH to achieving gender equality and social justice, WASH interventions are often evaluated using a narrow range of health outcomes, such as diarrhoea and child growth.25 26 This has created a ‘knowledge silo’ overlooking a wide range of potential impacts related to time savings, livelihoods and broader health and well-being.27 Additionally, a lack of data disaggregation by sex and other social identifiers has been highlighted as a barrier to better understanding the wide-ranging impacts of WASH interventions.2
A comprehensive mapping of evidence of GESI outcomes related to WASH interventions is therefore a first step towards incorporating GESI considerations into WASH intervention design, implementation and evaluation.27 28 However, a comprehensive overview of existing evidence on GESI in the WASH sector is not yet available.21 29 Existing reviews about WASH largely focus on health outcomes. Review authors that do pay attention to GESI tend to have a relatively narrow scope. Recently, a systematic review provided a synthesis of evidence on water and sanitation and women’s and girls’ empowerment as one of the GESI outcomes.30 A WASH evidence gap map was conducted across a broad range of WASH outcomes, but without including qualitative evidence or lacking an in-depth focus on GESI outcomes.29
With this review, we collate and describe evidence of inclusive and transformative GESI outcomes associated with WASH interventions. Specifically, the review question is: What evidence exists on the GESI outcomes of WASH interventions in low-income and mid-income contexts?
This review is timely as the Lancet Commission on WASH and health is reconceptualising WASH as not only foundational to public health but also key to gender equality and social and environmental justice.31 There is also a growing interest in gender-transformative programmes more broadly.32
Methods
Detailed methodology is available in a previously published protocol.24 However, no critical appraisal and data extraction was conducted in this review. We undertook a systematic mapping of the primary research studies instead.33 34 Metadata coding was followed by a narrative synthesis to describe the evidence base. The mapping process facilitates the discovery of research and highlights knowledge gaps and clusters. EPPI-Reviewer Web,35 a review management software, supported almost all stages of the review process including assembling a library of search results, deduplication, screening and metadata coding.
Search strategy, eligibility criteria and screening process
Search strategy
All searches were conducted for literature published between January 2010 and November 2020. Fifteen bibliographic sources were searched for English language literature. Additionally, the websites of 57 organisations suggested by experienced stakeholders in the field (collected via workshops and an open consultation process) were handsearched using simplified English (56 websites) and Spanish (12 websites) language search terms. Stakeholders were also invited to suggest unpublished, relevant literature. Bibliographies of 46 reviews identified during searching were also checked for relevant literature. Detailed search records are available in online supplemental tables S1–3. Search results from bibliographic databases were collated into a library, with duplicates removed before the screening.
Supplemental material
Supplemental material
Supplemental material
To assess sensitivity and increase the comprehensiveness of searches, a benchmark list of 32 articles of known relevance to the review was screened against search results and search strings were amended accordingly.
Eligibility criteria
Studies were included irrespective of publication status and electronic availability. All study designs including qualitative, quantitative and mixed-method studies were eligible. Commentary and theoretical papers, as well as modelling studies, were excluded. All types of study participants were included but restricted to those in low-income to middle-income countries (LMICs) (defined by World Bank 2020 classification).36
All types of interventions to promote improved WASH were eligible for the review, including behaviour change programmes, provision of WASH infrastructure and technologies, and economic and marketing-based approaches. Belcher and Palenberg’s definition of intervention was used, specifically, ‘a set of activities organised within a project, programme or instrument,’37 with clearly defined aims and sufficient details about implementation (including defined target population, intervention location and implementation duration). Studies without a clear and detailed description of the intervention were not eligible, as well as other types of water interventions such as irrigation or water resources management. WASH interventions implemented in households, schools, health facilities, community spaces and workplace settings were considered eligible for this review.
All GESI outcomes resulting from a WASH intervention were eligible. Health outcomes related to GESI and arising from gender roles and social norms were eligible, including musculoskeletal injuries and reduced nutritional status linked to water-carrying infections from poor menstrual hygiene management, and psychosocial stress associated with inadequate sanitation facilities. Other health outcomes, such as diarrhoea and stunting, were not considered.
During the review planning and protocol stage, a theory of change was co-developed with stakeholders to assemble a list of all potentially relevant interventions and outcomes, and to hypothesise links between them (see online supplemental figure S1).
Supplemental material

Screening process
The screening was conducted in two stages by a team of seven reviewers, with expertise in WASH, gender and systematic evidence synthesis methodology. First, titles and abstracts were screened together. Second, records were screened in full text (following retrieval). Consistency checking was performed on a subset of records at the beginning of each of the two screening stages. All disagreements were discussed in detail, with further consistency checking if the level of agreement was below 80%. The level of agreement between reviewers was between 88% and 95% for 600 titles and abstracts, and 78%–95% for 132 full texts.
Following the initial consistency checking exercise, EPPI-Reviewer Web’s machine learning tools—priority screening and bespoke classifiers—were used to increase title screening efficiency. Priority screening places items predicted to be more relevant at the begging of the screening queue. It predicts the likely relevance of a given record during the screening process and it increases the accuracy of predictions in interactions with a reviewer and the number of screened items. Bespoke classifiers organise items according to their probability of relevance, based on a training dataset (of included and excluded items). Each classified item is given a ‘probability of being relevant’ score. The scores are represented as decile bands of probability (from 0%–9% to 90%–99% likely to be relevant).38
Priority screening was used to support manual screening. Bespoke classifiers were used to identify an empirically informed screening cut-off point (after which no manual screening was done) as follows. First, 14 040 records (22.5% of all identified deduplicated records) were manually screened, a quarter of which (3642) were screened by at least two reviewers. Two data subsets were created at random from the manually screened records. The first was a training set (80% or 11 234 records) and the second was a test set (20% or 2806 records). A subset of 11 234 records used for training was assumed to be large enough to avoid hasty generalisation bias.39 Several bespoke classifiers were built and tested for satisfactory performance and class balance40 during the screening process. The two classifiers with the highest recall (a performance indicator showing a rate of true positives) were applied to a test subset of records and the number of incorrectly classified records was assessed. The model with the lowest number of false negatives (ie, with only 0.6% of ‘includes’ incorrectly classified into the lowest three decile bands of relevance probability) was applied to all non-screened items. Classified items (titles) within the highest seven decile bands of relevance probability (30%–99%, see online supplemental figure S2) were then screened manually and by all reviewers independently (9011 titles). Items classified into the lowest three decile bands of relevance probability (0%–29%) were excluded from the review (39 091 titles).
Supplemental material
Metadata extraction and synthesis
Extracted metadata included bibliographic information, study location, research type and analytical approach, details about intervention and implementation, the population descriptors and outcome themes. Outcome themes were coded both deductively (using the theory of change, see online supplemental figure S1) and inductively (drawing directly from reviewed literature). The coded outcome themes are thereafter classified into inclusive and transformative. A distinction between the inclusive and transformative types of outcome themes is often overlapping, as without asking individuals to reflect on their own personal and collective outcomes it is difficult to make this distinction with confidence. Nevertheless, we draw the distinction as a means to assess the extent to which reported outcomes align with transformative ideals. A list of definitions of each outcome is available in online supplemental table S4. The protocol24 includes a detailed overview of all the theoretical assumptions used to build our theory of change, including definitions of inclusive and transformative approaches.
Supplemental material
Consistency checking for metadata extraction was performed on a subset of 132 records independently by all reviewers across three rounds of consistency checking to assure the repeatability of metadata extraction. All disagreements were discussed, and the coding scheme was clarified where needed. The metadata from each record was then extracted by a single reviewer and the metadata was then narratively synthesised to assess frequencies and trends in the evidence base.
Role of the funding source
The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Public involvement
To take into account policy, research and practice needs and priorities as well as to increase potential policy uptake of review findings,41 international stakeholders (including representatives from academia, funding agencies and non-governmental organisations working in WASH implementation) were engaged throughout the review process. Together with these stakeholders (first via two workshops, followed by a public consultation process), we co-created a theory of change that facilitated review scope definition and later led a metadata coding exercise (more details in the protocol24). Moreover, stakeholders were shown preliminary review findings during a dedicated event at the World Water Week in Stockholm (August 2021, https://www.sei.org/events/world-water-week-evaluating-gender-and-social-equality-in-wash/) and asked for input on the clarity and relevance of the findings.
Results
The evidence base included 499 publications in total across 463 studies (66 publications described 30 studies). Publications were deemed to be part of a study if they were based on the same dataset or analysis, produced by the same (group of) authors, examining the impacts of the same intervention(s) at the same study site(s) (including pilot intervention testing in different locations). Figure 1 shows the flow of information through the different phases of our systematic mapping process. A list of excluded full texts with reasons for exclusion is available in online supplemental table S5 and all included studies with coded metadata are available in online supplemental table S6.
Supplemental material
Supplemental material
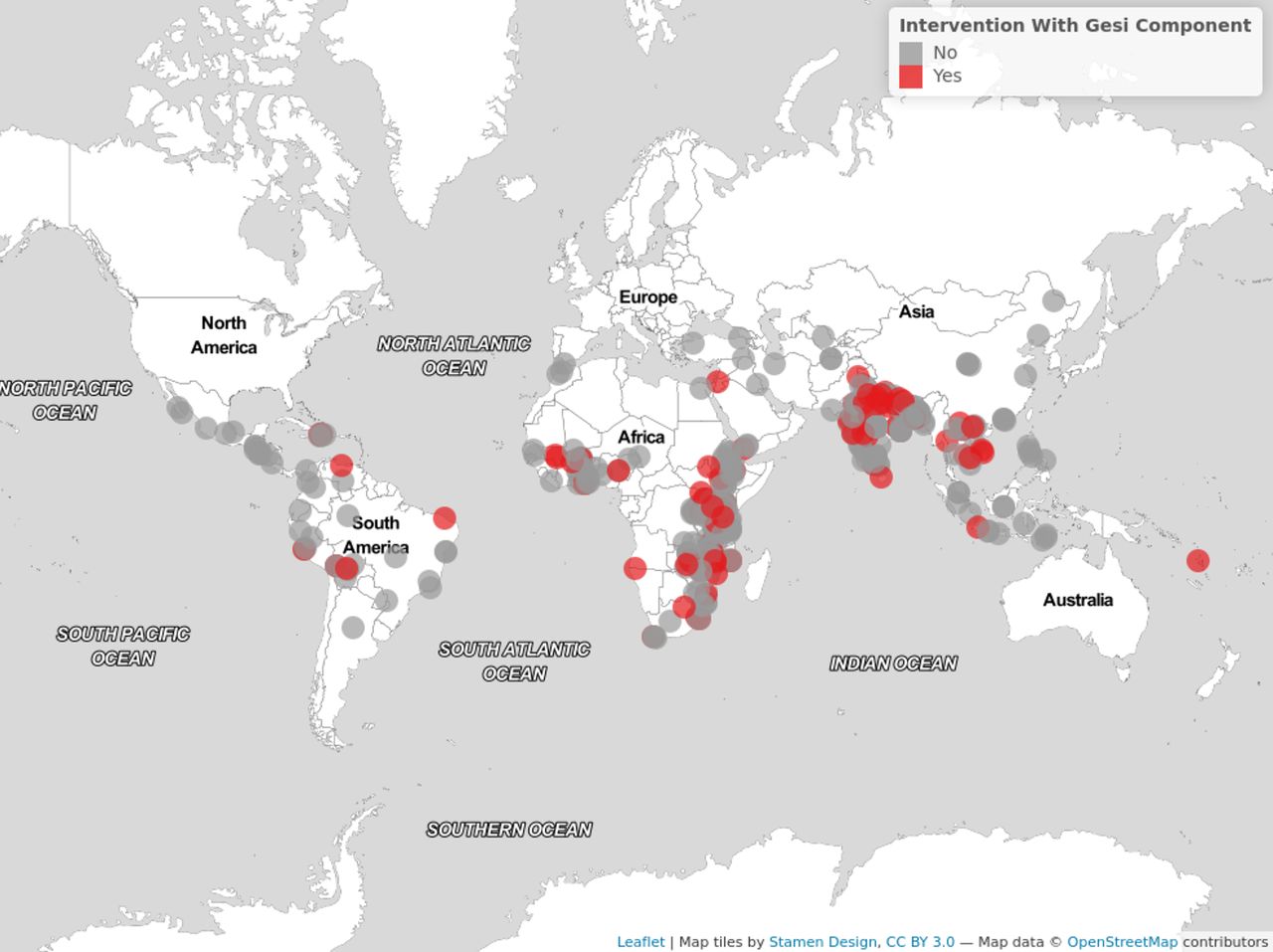
Overall, the literature on GESI outcomes of WASH interventions is considerable and steadily growing (online supplemental figure S3). Eligible studies from 62 LMICs were identified, including 23 least-developed countries. Sub-Saharan Africa and South Asia were the most frequently studied regions. India (represented in 81 studies), Kenya (62) and Bangladesh (49) were the most frequent research locations (figure 2, online supplemental table S7, online supplemental figure S4).
Supplemental material
Supplemental material
Supplemental material

A snapshot of the evidence atlas (visualised with EviAtlas59). The interactive version: https://sei.org/wp-content/uploads/2022/08/eviAtlasMap2022-08-22.html.

Distribution of outcome themes across studies. Transformative outcome themes are represented with grey bars and inclusive with blue. HWF, hand-washing facility; MHM, menstrual hygiene management.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of studies across (A) Types of GESI components designed for WASH interventions and (B) gender, age (between 5 and 10, or above 65) and other social groups targeted by interventions with GESI components. GESI, gender equality and social inclusion; WASH, water, sanitation and hygiene.
Quantitative research was prevalent (240 studies), followed by qualitative (122) and mixed-methods research (104) (online supplemental figure S5A). Included studies were evaluations of intervention impacts (373), followed by process evaluations (74) (online supplemental figure S5B). Our evidence base included 95 randomised experiments (including randomised control trials), 61 experiments without randomisation (including quasi-experiments) and other quantitative observational designs (178 studies) (online supplemental figure S5C). Most qualitative designs included studies without an explicit reference to a particular qualitative methodological approach (142 studies), followed by case studies (42 studies), ethnographies (19), phenomenology (18) and grounded theory (2) (online supplemental figure S5D).
Supplemental material
A little over half of the studies in the evidence base focused on water supply (55.3%), followed by sanitation (43.4%) and hand-washing (32.6%). Over half of all water supply studies were about water quantity (51.5%), and the rest focused on water quality (online supplemental figure S6).
Supplemental material
Most studies (68.9%) described interventions implemented in rural settings, followed by urban settings (17.5%) and slums and informal settlements (9.3%) (online supplemental figure S7A). Interventions were mostly implemented at the household level (56.8%), followed by the community level (25.3%), school (19.4%) and individual (10.8%). Interventions implemented at the service provider level (3.7%), in healthcare facilities (1.9%), government offices (0.9%), local markets (0.2%) or similar were less common (online supplemental figure 7B). A little over half of all studies involved behaviour change interventions (50.5%), followed by interventions that provided WASH infrastructure (40%) and training and capacity building (24.8%) (online supplemental figure S8A,B). The majority of behaviour change interventions focused on awareness building or messaging (80.7%), in comparison to triggering (eg, Community Led Total Sanitation approach) (27.7%) (including combinations of two approaches).
Supplemental material
Supplemental material
GESI outcome themes
We mapped 25 GESI outcome themes, including 12 inclusive and 13 transformative themes. A total of 435 studies reported inclusive, while 194 studies reported transformative outcome themes (online supplemental figure S9). Inclusive outcome themes, which focus on improving access and use of WASH for all users, encompassed equitable access and use of safe water supply (41.3%), sanitation (31.1%) and hand-washing facilities (27.2%), knowledge of safe WASH (32.2%), service quality (29.4%), attitudes towards safe WASH (23.5%), affordability of WASH services (19.9%) and similar (figure 3, blue bars). Transformative outcome themes, related to changes in existing gender norms, roles or other power relations, included change in time use (related to WASH activities or time available for leisure, work or schooling and similar) (15.8%), participation in WASH-related decision-making activities (10.2%), education (8.9%), economic and livelihood opportunities (8.6%), empowerment and agency (8.2%), non-discrimination and equality (6.9%), gender attitudes and norms (6.3%), self-confidence and self-efficiency (6.3%) and others (figure 3, grey bars).
Supplemental material
The top three research locations (India, Kenya and Bangladesh) together featured the highest proportion (51%–67%) of the following outcome themes: GESI mainstreaming of service providers, mobility, economic opportunities, non-discrimination and equality, education opportunities and time use. The only outcome theme not reported at all in the top three research locations was social capital (online supplemental table S8). All transformative outcome themes were relatively consistently reported across water supply and sanitation sectors, in contrast to hand-washing or hygiene where there are frequent gaps in the evidence base (online supplemental table S9). Both inclusive and transformative outcome themes had consisently high frequencies in rural settings (online supplemental table S10). No transformative outcome themes were reported for interventions targeting healthcare facilities. Moreover, transformative outcome themes were proportionally underrepresented in studies describing interventions targeted at schools, individuals, service providers, governments and markets (online supplemental table S11).
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Only 266 studies (57.5%) reported disaggregated outcomes, and specifically across age, sex or other social categories (including disability status, caste, ethnicity or religion). Studies mostly reported outcomes disaggregated across only one of these three categories (online supplemental figure S10) and mainly by sex (online supplemental figrue S11A). Outcomes were mostly reported in relation to women (173 studies), men (87), 11–18 years old girls (71), 5–10 years old children (64) and 11–18 years old boys (43). Only a small number of studies reported outcomes related to specific caste, ethnicity or religion (17), people with disabilities (10) and adults above 65 years of age (7). No studies reported outcomes related to sexual or gender minorities (online supplemental figure S11B).
Supplemental material
Supplemental material
Interventions with GESI mainstreaming components
Out of 463 studies in the evidence base, only 22% (104 studies) studied interventions that included GESI mainstreaming components. The majority of these components involved capacity building and training (including individual and group mentoring of women) (40.4%), followed by the provision of participation and leadership opportunities (such as activities to improve financial independence or inclusion in decision-making) (25%), WASH infrastructure (19.3%) (such as female friendly toilets), product provision (eg, water filters, pads, hygiene kits) (18.3%) or financial support (such as the provision of tariffs, loans and subsidies) (13.5%) (figure 4A).
Interventions with GESI components mostly targeted specific gender identities (77.9%), including women (51.9%) and girls (24%), followed by men (1.9%). Other social categories, such as people with disability status, those who are chronically ill (9.6%), and other marginalised social groups (6.7%) accounted for an additional 19.2% of all targeted categories in total. Interventions with GESI components in our evidence base very seldomly targeted children (3.8%) or adults above 65 years old (2.9%) (figure 4B and online supplemental figure S12).
Supplemental material
Interventions with GESI components were reported in all eligible regions except Europe and Central Asia (0 out of 3 studies), Latin America and the Caribbean region had proportionally the lowest number of studies with GESI interventions (7 out of 50) and East Asia and Pacific (12 out of 47) and sub-Saharan Africa (63 out of 238), the highest (online supplemental figure S13.
Supplemental material
Some transformative outcome themes, such as participation opportunities, empowerment and agency, self-confidence, and efficacy, were proportionally more frequently reported in studies evaluating interventions with GESI components (online supplemental figure S14A,B).
Supplemental material
Discussion
Our systematic map identified a large range of GESI outcome themes across different types of interventions (entire browsable dataset is available in online supplemental table S6). However, transformative outcome themes were reported in comparatively fewer instances, indicating this is not often a focus of WASH intervention evaluations and highlighting the important evidence gap in the WASH sector. Measuring (transformative) social change is complex, non-linear, context-specific and slow.42 Yet, this should not prevent the research community from collecting evidence about transformative outcomes, especially as tools to measure GESI outcomes in the WASH sector are emerging and have the potential to address this gap.43–45 While addressing gender inequalities is often described as a key aim of WASH programmes, regular collection of qualitative46–49 and quantitative gender and equality data and monitoring should be mainstreamed by practitioners to ensure this aim is achieved and to improve understanding of both the extent and direction of change.
The WASH community should broaden reporting of GESI outcomes beyond a focus on women and girls. Disaggregated outcome-related information across sex and other social categories in our review was provided in only a little over half the studies, and mostly related to women and girls. Very little was reported for other social categories, including disability status or ethnicity, and we found no information on sexual and gender minorities. As noted in other reviews,22 30 more research is needed to understand the impact of WASH interventions (and especially those with GESI components) for various gender and social identities. Future research should explore outcomes of WASH interventions using an intersectionality lens and for (as a minimum) sex and gender minorities,50 different age or socioeconomic categories, people with disabilities and other identity markers. This will allow for a better understanding of the pathways through which WASH leads to gender and socially transformative change for all users, and opportunities to address the multiple and intersecting structural barriers that prevent equality.
Our review highlights that further research should explore GESI outcomes in a more diverse range of settings beyond the household. A study on the maternal and reproductive health priorities of women around the world found that WASH services and facilities were the top priority after respectful and dignified care.51 However, only nine studies in our review’s evidence base examined GESI outcomes in healthcare facility settings. The lack of studies about the service provider context is also concerning, as increasing gender and social equality requires change beyond the individual, but at the institutional and structural levels too.30 52 53
In terms of geographical distribution, knowledge clusters are notable in India, Kenya and Bangladesh. Nevertheless, more than half the world’s LMICs were absent from the evidence base. This highlights a need for a more even distribution of rigorous research of GESI outcomes globally, particularly due to the ways in which gender and social relations vary by cultural context.
Similarly to other sectors,54 55 the WASH community needs comprehensive evaluations of WASH interventions. Future research should identify the most effective WASH interventions that can facilitate transformative change. Furthermore, our systematic map found that interventions with GESI mainstreaming components were under-researched. Nevertheless, regardless of whether a WASH intervention includes intentional GESI mainstreaming, it will still result in social and gendered (positive or negative) outcomes.56 This demonstrates the importance of careful planning to ensure that interventions have a positive GESI impact, and the need to influence WASH intervention design in the direction of inclusion and equality, rather than risking harm. Evidence from the broader development sector further supports this and shows that incorporating gender equality and women’s empowerment components into intervention design is associated with improvements in development and health outcomes.54 Overall, more interventions should use an intersectional approach in their design and implementation, going beyond gender and extending understanding of interconnected systems and power structures that might create or maintain inequalities or exclusion. Moreover, future research is needed to evaluate the impact of inclusion of GESI components in the WASH intervention designs, and to understand what leads to the most transformative change for all.
Our systematic mapping has some limitations. We conducted extensive academic literature searches in English, and grey literature searches in Spanish and English. We used diverse search sources, terms and languages to avoid selection bias and increase comprehensiveness. However, the search was limited to literature published between 2010 and 2020 and studies from low-income and middle-income contexts. Academic searches could be extended by using non-English search terms and expanding to high-income contexts. We only included research about WASH interventions, but literature that does not include (well-described) WASH interventions is informative for a general understanding of GESI outcomes in the WASH context and could be examined in future. The list of excluded full texts with reasons for exclusion compiled during the mapping process could be used to facilitate this undertaking (see online supplemental table S5). This systematic map was also not set to evaluate the impacts of WASH interventions on GESI outcomes, but the evidence collated in this work provides a basis for such investigations. Future research can use the evidence base collated in this map to determine which WASH interventions work as intended for GESI outcomes. This will help to fully realise the potential returns of WASH investments and will better equip us to challenge harmful gender norms and power relations that hold societies back from achieving gender equality and other forms of social inclusion.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Acknowledgments
This work was funded by the Centre of Excellence for Development Impact and Learning (CEDIL) which is supported by UK aid from the UK Government. We are thankful to George Njoroge, Audinisa Fadhila and Molly Hanson for their support during various stages of the review process. Thanks to our advisory board members for their invaluable insights and advice: James Thomas, Lewnida Sara, Louisa Gosling, Hugh Waddington, Naomi Carrard, Karin Hannes and Marni Sommer. We are also extremely grateful to all stakeholders for their input and feedback provided at various stages of the review process.
References
Footnotes
Handling editor Seema Biswas
Twitter @biljana_macura, @carliera, @AdrianaSoTru, @_ariannaorlando, @laura_delduca, @naomicarrard, @KarinHannes, @marnisommer, @sarahdickin
Contributors BM: guarantor, conceptualisation, funding acquisition, project administration, methodology, analysis, visualisation, writing—original draft preparation, writing—review and editing. EF, CL, AS, AO and LDD: data collection, writing—review and editing. NC, KH and MS: validation, writing—review and editing SD: conceptualisation, funding acquisition, analysis, writing—review and editing. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Funding The Centre of Excellence for Development Impact and Learning (CEDIL).
Competing interests None declared.
Patient and public involvement The public was involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.