Article Text

Abstract
Introduction Malaria and malnutrition are key public health challenges in India. However, the relationship between them is poorly understood. Here, we aimed to elucidate the potential interactions between the two health conditions by identifying the areas of their spatial overlap.
Methods We have analysed the district-wise undernutrition and malaria data of 638 districts of India across 28 states and 8 union territories. Data on malnutrition parameters viz. stunting, wasting, underweight and anaemia, sourced from the fourth National Family Health Survey (2015–2016), and malaria Annual Parasite Index (API) data of the same year (i.e, 2015), sourced from National Center of Vector Borne Diseases Control were analysed using local Moran’s I Index and logistic regression.
Results Among all the malnutrition parameters, we found underweight in children and anaemia in men to co-occur with malaria in the districts of Chhattisgarh, Jharkhand, Madhya Pradesh and Odisha. Further, districts with more than 36% underweight children (OR (95% CI): 2.31 (1.53 to 3.48)) and/or more than 23.6% male population with anaemia (OR (95% CI): 2.06 (1.37 to 3.11)) had higher odds of being malaria endemic districts (ie, Annual Parasite Index >1).
Conclusion Malaria and malnutrition co-occur in the malaria-endemic parts of India. The high prevalence of undernutrition in children and anaemia among men may contribute to malaria endemicity in a particular region. Therefore, future research should be prioritised to generate data on the individual level. Further, malaria control interventions could be tailored to integrate nutrition programmes to disrupt indigenous malaria transmission in endemic districts.
- malaria
- nutrition
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Undernutrition compromises immunity and predisposes humans to a plethora of infections. Malaria, a mosquito borne infectious disease, has been on a persistent decline in India. The National Family Health Survey round 4, conducted in 2015–2016 under the aegis of the Ministry of Health and Family Welfare, Government of India, reveals that many parts of the country are affected by child and adult undernutrition. The association between malaria and undernutrition has been investigated in several malaria-endemic countries, but studies show mixed results.
WHAT THIS STUDY ADDS
This study underscores the association between malnutrition and malaria in the endemic states of India. It is evident that chronic malnutrition and anaemia co-occur with malaria and their prevalence beyond a certain threshold is likely to enhance the risk of persistent malaria in a region/district.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The study provides a path for generating evidence to corroborate the malaria–malnutrition association and its risks to humans. It further advocates focused interventions targeting both undernutrition and malaria in endemic areas.
Introduction
Undernutrition is a major risk factor for under-5 mortality and health loss worldwide. As per WHO estimates, undernutrition accounts for ~45% of deaths among under-5 children and the burden is most prominent in low/middle-income countries.1 Malnutrition is fairly widespread in India, with more than 68% of deaths in children under 5 years old attributable to malnutrition.2 As per the fourth National Family Health Survey (NFHS-4) conducted during 2015–2016, more than 35% of children below 5 years of age in India suffered from chronic malnutrition in the form of stunting (low height for age) or underweight (low weight for age), while more than 20% of them were wasted (low weight for height). Over 50% of children and women were anaemic across the country.3 Similarly, a significant proportion of the adult population was undernourished (body mass index <18.5 kg/m2).3 In the recently conducted fifth round of NFHS (NFHS-5; 2019–2021), the nationwide prevalence rates of stunting, underweight, and wasting are 35.5%, 32.1%, and 19.3%, respectively.4 Although there is a slight improvement in the undernutrition indicators, the prevalence of anaemia among children and women seems to have risen in a few districts in the last 5 years (67.1% of children (age group 6–59 months) and 59.1% of all women (age group 15–49 years) were anaemic in the NFHS-5 vs 58.6% children and 54.1% women in NFHS-4).4 Undernutrition is prominent among the rural and tribal sections of India, which are also burdened with several infectious diseases that include waterborne diseases, respiratory infections, pneumonia, reproductive tract infections, tuberculosis (TB), leprosy and malaria.3 5–8
Malaria is a challenging infectious disease in India but has been in a declining phase since 2002. Globally, India is the leading contributor to the malaria burden in the WHO Southeast Asia Region (SEAR). As per the World Malaria Report 2021, India accounted for 83% of all malaria cases and 82% of all malaria deaths in the WHO SEAR.9 India has a diverse topography, ecology and climate which support malaria transmission in almost all states/Union Territories (UTs) with varying intensities and transmission windows.8 In 2015, there were eight states, namely Mizoram, Meghalaya, Odisha, Tripura, Chhattisgarh, Arunachal Pradesh, Jharkhand and Madhya Pradesh where malaria API was more than 1 and these contributed to 77% of the total malaria burden in India. Incidentally, except for Mizoram, all these states also had a large and persistent burden of undernutrition.3 As resistance to infections is intricately linked to the nutritional status of individuals, it becomes important to understand the potential influence of malnutrition on malaria morbidity in the Indian context. Studies conducted elsewhere highlight a complex relationship between malaria and undernutrition with divergent findings on the effect of malnutrition on malaria and vice-versa. While some suggest protective or no effects of undernourishment,10–15 several others highlight increased susceptibility to malaria in malnourished individuals.16–19 Nonetheless, the association between chronic malnutrition and disease severity is reported to be rather consistent where the former is likely to enhance disease severity in terms of parasitaemia and associated anaemia.16 20–22
Undernutrition is also shown to lower the anti-malarial bioavailability of drugs which may further support recurrent and severe infections in malnourished children.16 21 22 Prevalence of anaemia in a population is also an indicator of its poor nutritional status, and in high malaria transmission settings, it has been seen that this disease is inevitably associated with some degree of anaemia through enhanced removal of circulating red blood cells and suppressed erythropoiesis due to bone marrow suppression.23 In India, associations between malnutrition and malaria are inadequately studied. In a preliminary study, Ghosh et al concluded that malnutrition does not palliate malaria in children.24 A few other sporadic studies provided indirect and weak evidence of the malaria–malnutrition association by assessing the serum concentrations of micronutrients such as retinol, tocopherol, riboflavin, etc in patients with malaria.25 26
Thus, malnutrition can affect the immunity of individuals by making them more susceptible to the disease or by raising disease severity in individuals. Identifying co-occurrences of these two factors can enable the national programme to target them in conjunction and customise the control interventions in areas where malnutrition and malaria coexist at the individual level. The present study dissects the linkages between malaria and malnutrition in India where both malnutrition and malaria are important public health challenges.
Methods
About the data
NFHS is a nationally representative large-scale survey conducted under the aegis of the Ministry of Health and Family Welfare, Government of India. It was initiated in the year 1992–1993 for providing information on key aspects of health, family welfare and nutrition. These include district and state-level indicators of fertility, infant and child mortality, maternal and child health, reproductive health, nutrition, anaemia, and health and family planning services. So far, five rounds of NFHS (NFHS-1–NFHS-5) have been completed. NFHS uses a uniform sample design in which districts are stratified into rural and urban areas, and primary sampling units (PSUs) in each urban/rural stratum are identified. Within each PSU, a fixed number of households are selected using equal probability systematic sampling for conducting surveys.27
In 2019–2021, India implemented the NFHS-5, but complete data were still not in the public domain at the time of these analyses. Therefore, data from the NFHS-4, conducted in the year 2015–2016, were used to study the association of malnutrition with malaria. Malaria data of the same period (ie, 2015) were taken from the National Center for Vector Borne Diseases Control (NCVBDC).
Variables of interest
Malnutrition parameters: stunting, wasting, underweight, anaemia in women, anaemia in men and anaemia in children were taken from a subset of NFHS-4 that focused on the nutrition status of the population. The API was used as an indicator of malaria burden, taken from NCVBDC’s data on malaria. The NCVBDC collects data for the continuous active and passive surveillance of malaria in the country and is meant to be a reliable representation of the actual malaria burden. The API can be defined simply as the total number of malaria cases per 1000 population. Owing to the large variation in malaria incidence across the country, NCVBDC stratifies the states and districts in India into different phases of malaria control based on the API, that is, states with less than 1 API in all districts are placed in the elimination phase, states with less than 1 API but with some districts reporting more than 1 API are placed in the pre-elimination phase and finally, states that have more than 1 API are placed in the intensified control phase.28 Based on this, we categorised all districts of India into two categories of API (<1 and >=1).
Study design
This is an ecological study where data were analysed at the district level.
Statistical analysis
The local Moran’s I (Anselin) cluster and outlier analysis was performed to assess whether malnutrition parameters are randomly distributed over the country or follow some patterns. The local Moran’s I Index is a local spatial autocorrelation statistic that can be summarised by the equation:

where xi is the magnitude of the variable x at location i; xj is the value of the variable at all other locations; ẍ is the average of x; n is the number of samples; Si2 is the variance of the variable of interest; and wij is the weight computed as the inverse distance between locations i and j. The Moran’s I divides a geographical region into different clusters/outliers as discussed below:
High-high clusters or hotspots: hotspot clusters represent those areas of a geographical region where the prevalence of a particular condition (in our case, prevalence of malnutrition parameters) is high in that area as well as its surroundings (ie, neighbouring districts).
Low-low clusters or coldspots: coldspot clusters represent those areas of a geographical region where the prevalence of a particular condition (in our case, prevalence of malnutrition parameters) is low in that area as well as its surroundings (ie, neighbouring districts).
Outliers (high-low or low-high): Moran’s I also marks some areas as outliers which implies that the value of a particular condition is high in a particular area but low in its surrounding areas (called high-low outliers) or vice-versa (called low-high outliers).
Further, to assess the association or co-occurrence between malaria and malnutrition parameters, we identified cut-off values for each of the malnutrition parameters taking the malaria status of a district as dichotomous (API ≥1 and API <1) by using receiver operating characteristic (ROC) curve. We calculated sensitivity and specificity at each point, and the point where sensitivity and specificity are fairly comparable was considered the cut-off value (online supplemental tables 4–9). Different cut-off values were obtained for different malnutrition parameters as given below:
Supplemental material
Stunting (≤37 and >37).
Wasting (≤20 and >20).
Underweight (≤36 and >36).
Anaemia in women (≤54 and 54).
Anaemia in men (≤23.6 and 23.6).
Anaemia in children (≤60 and 60).
Once the malnutrition parameters were converted into binary, the association of each of these malnutrition parameters was assessed with malaria endemicity (API ≥1 and API <1) using simple logistic regression followed by multivariable logistic regression. All analyses were carried out using Stata V.15.0, R V.3.4.4 and Esri ArcGIS V.10.2 software, and a p value less than 0.05 was considered statistically significant.
Limitation
A limitation of this study is its design, that is, it is an ecological study. The association which was assessed in this study is at the district level and may not be applicable to the individual level. Still, this work remains very important as it identifies regions where a significant burden of both these health conditions coexists. This analysis will be helpful in the context of malaria elimination.
Results
The NFHS-4 (2015–2016) was carried out in all 29 states and 6 UTs of India, with a total sample size of 568 200 households constituting 625 014 women, 93 065 men and 265 653 children below the age of 5 years.3 The NFHS-4 data revealed that malnutrition was widespread in India in 2015–2016, with a large part of the country having ‘very high’ levels of stunting, wasting and underweight children as per the cut-offs for public health significance defined by the WHO29 and provided in the online supplemental table 1.
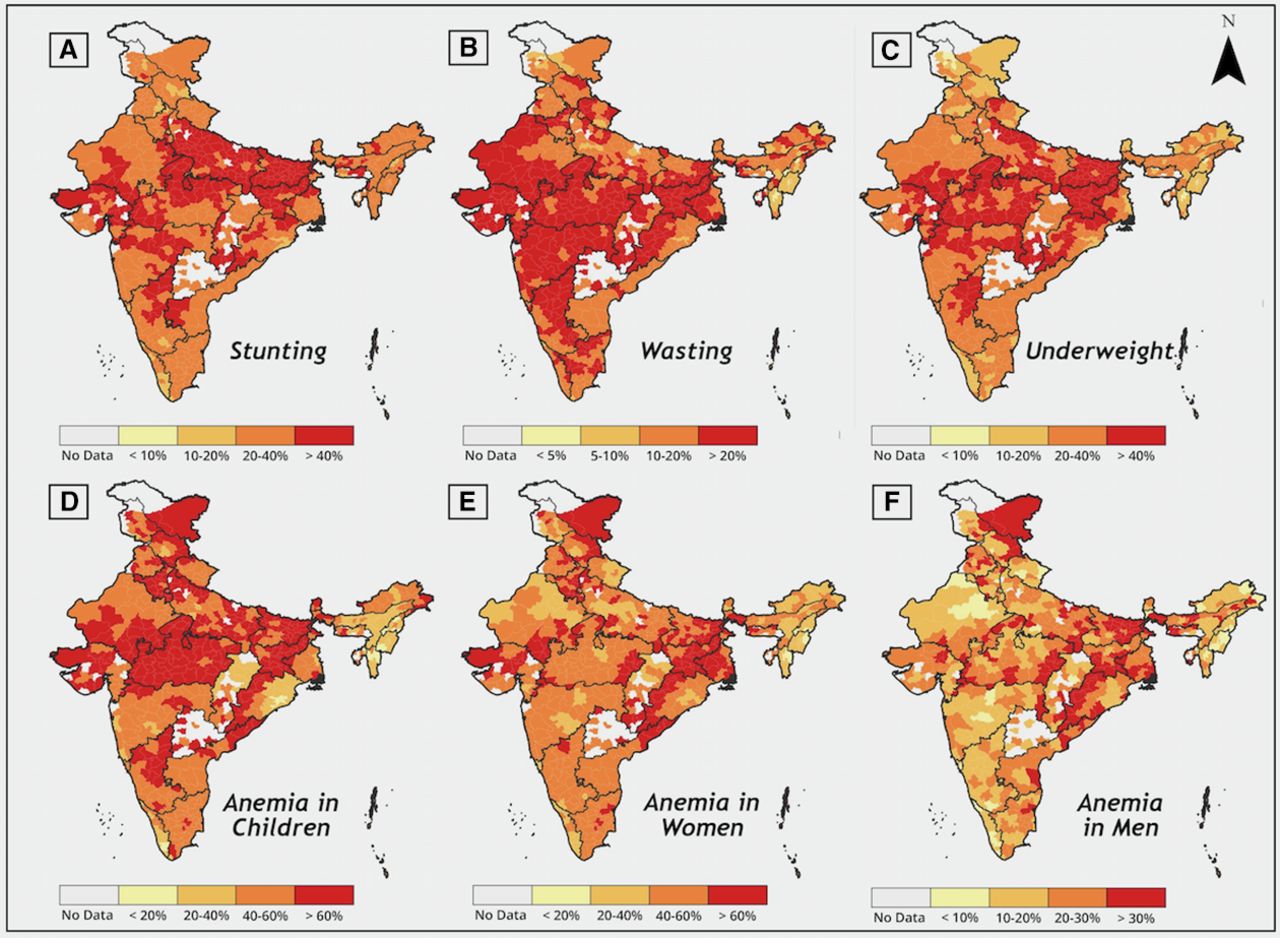
Out of all the states, Jharkhand was the most affected by malnutrition with a very high prevalence of the malnutrition parameters, that is, stunting (45.3%), wasting (29%) and underweight (43.9%). Jharkhand was also highly endemic for malaria, and despite significant reduction still ranked among the most malarious states (online supplemental table 2). Chronic malnutrition manifesting as stunting and underweight among under-5 children was also fairly widespread in the states of Bihar (48.3% and 43.9%, respectively), Uttar Pradesh (46.3% and 39.6%), Gujarat (38.5% and 39.3%), Madhya Pradesh (42% and 42.8%) and Rajasthan (39% and 36.7%) (figure 1A,C). On the other hand, wasting was most prevalent in Karnataka (26.1%), Maharashtra (25.6%), Rajasthan (23%) and West Bengal (20.3%), besides Jharkhand (figure 1B). Jharkhand and Bihar also had a significantly large proportion of children (69.9% and 63.5%, respectively), women (65.2% and 60.3%) and men with anaemia (29.9% and 32.2%). Similarly, Haryana had a high incidence of anaemia in both children (71.7%) and women (62.7%), whereas West Bengal and Andhra Pradesh had a high incidence of anaemia in women (62.5% and 60%, respectively) and men (30.3% and 26.9%) (figure 1D–F). The south Indian state of Kerala as well as the northeastern states, particularly Mizoram and Manipur, fared the best in terms of malnutrition and anaemia, with less than 25% of the population affected. A noticeable deviation from this trend was observed in the northeastern state of Meghalaya which had a fairly high level of stunting (43.8%). Among the northeastern states, Meghalaya was the second most endemic for malaria in 2015 (online supplemental table 3).

Distribution of malnutrition parameters: (A) stunting, (B) wasting, (C) underweight, (D) anaemia in children, (E) anaemia in women and (F) anaemia in men in India.
Since 2002, India has achieved a steady decline in its malaria burden and by the year 2015, high endemicity for malaria was restricted to only a few states. By 2015, a major part of the country fell under the pre-elimination or elimination phase of malaria control, with an overall state malaria API of less than 1. By 2015, only 10 states were classified as category 3 for malaria control (state API ≥1), namely: Maharashtra, Madhya Pradesh, Chhattisgarh, Odisha, Jharkhand, Meghalaya, Tripura, Mizoram, Arunachal Pradesh, and Andaman & Nicobar Islands. However, despite the gains in malaria control, five of these states were still endemic for Malaria (Chhattisgarh, Odisha, Tripura, Meghalaya and Mizoram) and regularly reported higher APIs .28 A probable cause for the high endemicity in these states could be the prevalence of certain chronic conditions that may render the populace more vulnerable.16 It has been observed from our analyses that every district with high malnutrition status does not necessarily have a high incidence of malaria; however, the converse is often true, that is, highly malarious regions often have moderate to high levels of stunting, wasting, underweight and anaemia status.
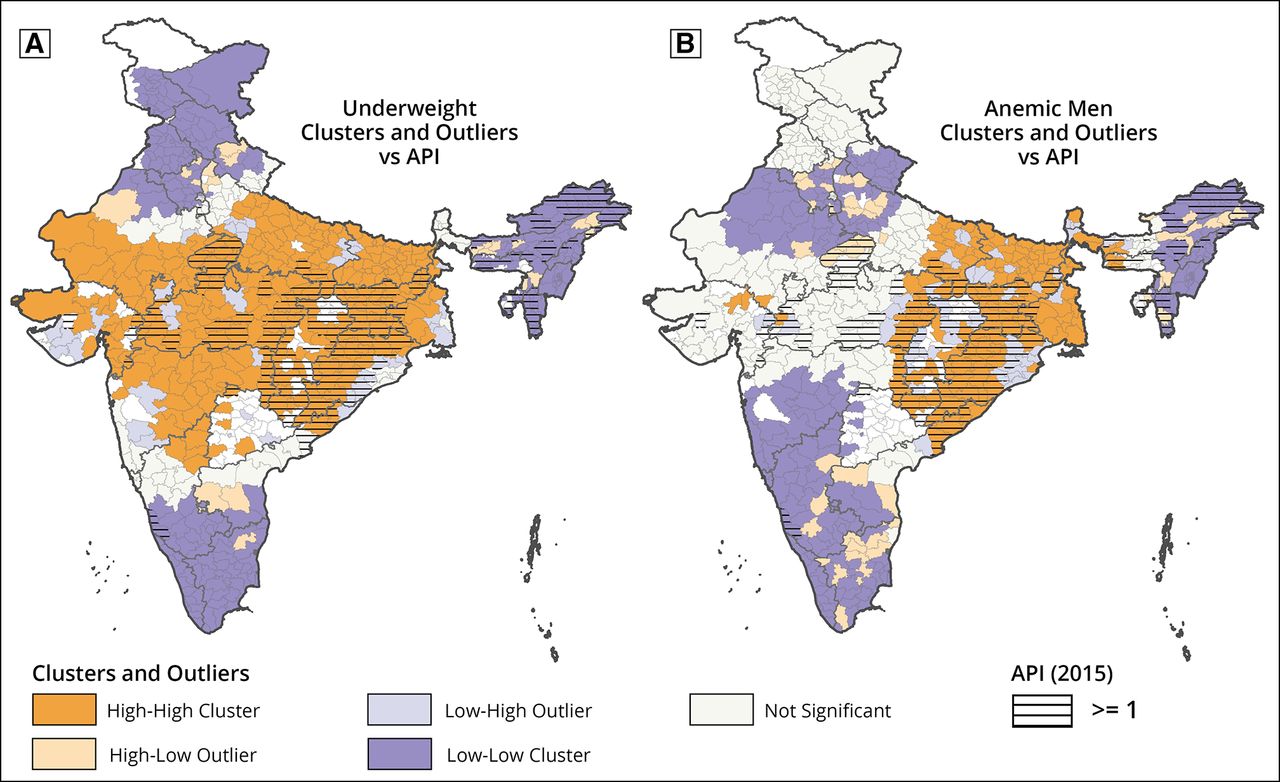
To investigate further, spatial clustering in malnutrition parameters and malaria was identified using Moran’s I statistic which signifies the co-occurrence of two malnutrition parameters (viz. underweight and anaemia in men) and malaria. In most parts of India, high incidence of malaria (≥1 API) co-occurs with high-high clusters and some low-high outliers of underweight, whereas the results are quite contrary in the northeast, where high malaria incidence (≥1 API) coincides with low-low clusters and high-low outliers of underweight. High-high clusters of underweight are observed in most parts of Gangetic Plains, Central Highlands, semiarid/arid desert regions as well as the northern parts of the Deccan Plateau. Among these Madhya Pradesh, Chhattisgarh, Odisha and Jharkhand are the major states which are highly malaria endemic. On the other hand, the southern peninsular region, Northern Himalayan regions, Punjab, Haryana and the northeastern parts of the country exhibit low-low clusters of underweight. Apart from the northeastern region, the malaria API is low (API <1) in all the low-low clusters of underweight. Several districts in northern India (such as Bikaner, Kaithal, Saharanpur, Ambala, Panipat, Balaghat, Muzaffarnagar, Tehri Garhwal and Uttarkashi) as well as a few in the northeastern parts (namely Dhubri, Barpeta, Bongaigaon, Goalpara, Darrang, Tinsukia, Dibrugarh) are outliers and have a high incidence of underweight in children despite significantly lower incidence in the neighbouring districts. As similar to underweight, high malaria endemicity coincides with high-high clusters of anaemia in men as well, with northeastern states once again behaving differently, that is, despite the low prevalence of anaemia in men, endemicity for malaria is fairly high in this region (figure 2).
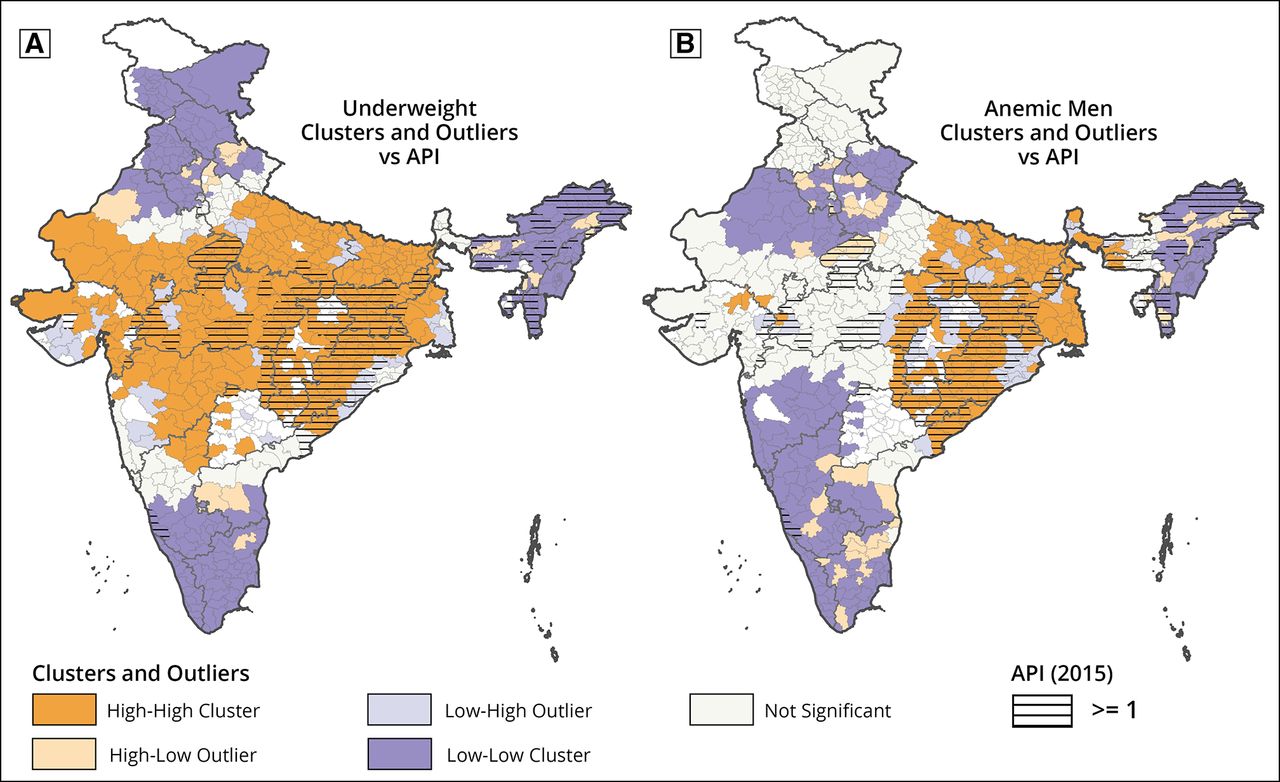
Co-occurrence of malaria (API >1) and malnutrition parameters: (A) underweight and (B) anaemia in men in India by clusters creation using Moran’s I statistic. API, Annual Parasite Index.
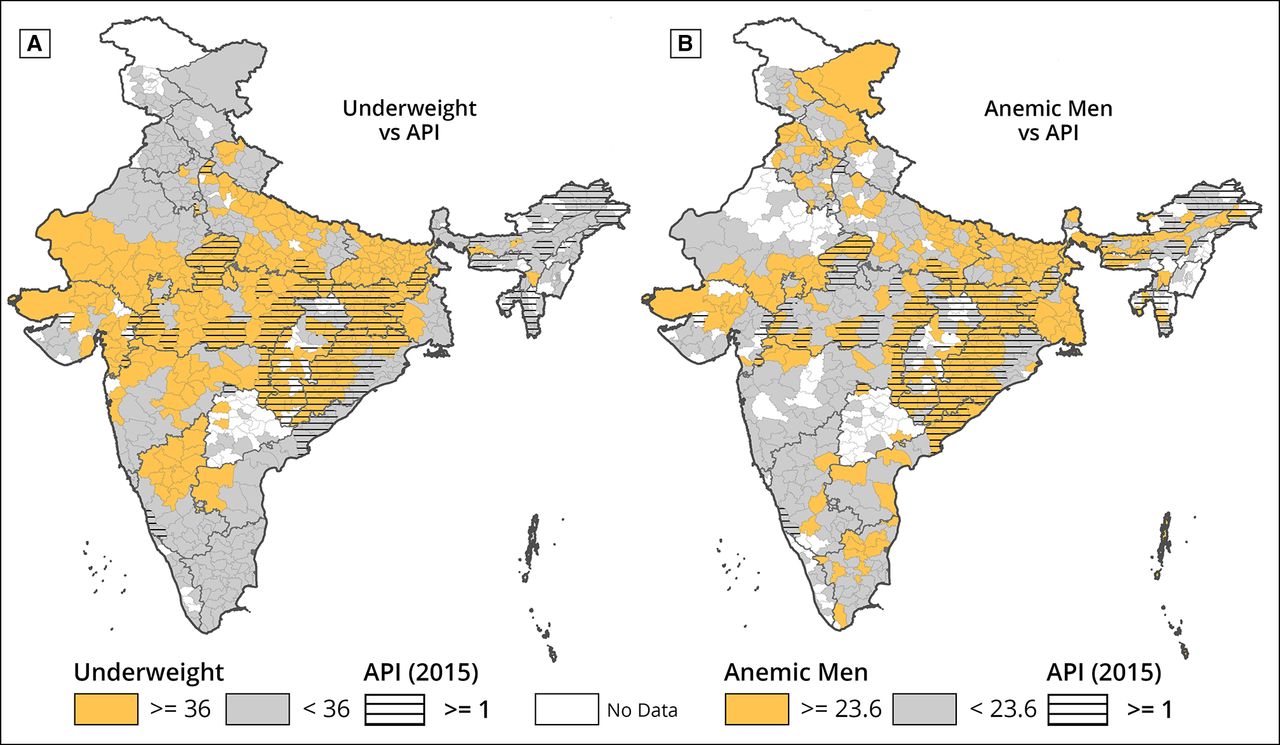
To establish a robust statistical association between malnutrition parameters and malaria burden, we categorised each of the malnutrition parameters into two categories based on the ROC curve and then logistic regression was implemented to assess the relationship between malaria and malnutrition parameters. The malnutrition parameters show a significant association with malaria endemicity at the district level in the bivariable analysis and multivariable analysis using simple logistic regression and step wise logistic regression respectively (table 1). At the end of the multivariable analysis, only two malnutrition parameters viz. underweight in children and anaemia in men were found to be statistically associated with malaria API. A district with more than 36% underweight prevalence status is likely to have 2.46 (95% CI 1.53 to 3.48) times higher odds of having a high incidence of malaria (API >1) as compared with districts where underweight prevalence is below or equal to 36%. Similarly, if the prevalence of anaemia in males in a district is more than 23.6%, it is likely to have almost two times higher odds of having high malaria (OR (95% CI): 2.06 (1.37 to 3.11)) (table 1 and figure 3).

{kind=link}
{kind=link}
{kind=link}
Cross-classification of malaria API (≥1 and <1) and malnutrition parameters: (A) underweight (≥36, <36) and (B) anaemia in men (≥23.6, <23.6), in India.API, Annual Parasite Index.
Malnutrition parameters associated with endemicity of malaria using logistic regression analysis
Among the 272 Indian districts (out of 638; 42.6%) where the prevalence of underweight is 36% or more, 80 of these districts (ie, 31%) had malaria API of 1 or more. These 80 districts predominantly belong to four states, namely Chhattisgarh, Jharkhand, Madhya Pradesh and Odisha. On the other hand, 188 out of the 638 districts (equivalent to 57.4%) of India had an underweight prevalence lower than or equal to 36%, and among these only 52 (ie, 15.4%) districts have malaria API 1 or more. These districts belong to over 14 different states in India and out of these, Arunachal Pradesh, Meghalaya and Mizoram are endemic to malaria. The second malnutrition parameter, which was statistically associated with malaria, is anaemia in men. A high prevalence of anaemia in men can be observed in central eastern parts of the country such as the eastern part of Madhya Pradesh, the southeastern part of Uttar Pradesh, Bihar and Odisha, some parts of Andhra Pradesh and West Bengal. Among these, the majority of the regions/states are highly malaria endemic.
Discussion
Malaria is a declining infectious disease in India with foci of stable disease transmission often coinciding with the rural and tribal belts where communities are socioeconomically marginalised. Using retrospective data analysis, we demonstrate that malaria and malnutrition are highly correlated in endemic regions. We first examined the distribution of malnutrition parameters viz. stunting, wasting, underweight and anaemia among children, men and women across the Indian states. We found that many parts of India are affected by varying degrees of adult and child malnutrition. It is important to note that many central, eastern and a majority of western states had the highest prevalence of chronic undernutrition (stunting and underweight prevalence >30%) vis-à-vis remaining parts of India. Several states in these regions, which include Jharkhand, Chhattisgarh, Odisha, Madhya Pradesh and Maharashtra, are highly malaria endemic and cumulatively reported more than 0.743 million cases in the year 2015. A significant prevalence of wasting was also observed in these states. The malaria-endemic states of the northeast, however, were better nourished despite perennial malaria transmission. Except for Meghalaya, the levels of malnutrition were comparatively low in Arunachal Pradesh, Mizoram and Tripura. Cultural and dietary differences may account for better nutrition in the northeast.30 Further, Meghalaya, Mizoram and Tripura share international borders with Bangladesh and Myanmar which are malaria endemic. Cross-border malaria along with poor surveillance and high climatic suitability are major drivers of malaria transmission in these states.31 Recent studies have been unable to find a clear association between malnutrition and malaria in high malaria-endemic districts in the northeast.32
The endemic states exhibited considerable district-wise heterogeneity in their malaria caseload/API. We observed that underweight children form high-high clusters and these clusters were spread uniformly in the eastern, central and western states of India, and overlapped with highly malaria-endemic districts (API >1)—Chhattisgarh, Jharkhand, Madhya Pradesh, Maharashtra and Odisha. Anaemia among men exhibited spatial clustering in the eastern and to some extent in the northeastern states of the country. Strikingly, several districts within these states are highly endemic for malaria. As malnutrition remains prevalent in India, this analysis enabled us to specifically identify the districts where malaria and malnutrition co-occur. In districts where the levels of underweight or anaemia in men crossed particular cut-offs (36% for underweight and 23.6% for anaemia among men), the odds of having high malaria (API >1) doubled. In other words, the high prevalence of underweight and anaemia among men emerged as risk factors for high malaria in a district. Our findings are in line with previous studies which showed that stunting and being underweight enhanced malaria risk in malnourished children.20 33 34 Underweight can arise from both acute and chronic malnutrition. While chronic malnutrition is demonstrated to increase susceptibility to clinical malaria and relapses, acute malnutrition may promote fatal outcomes and mortality in malnourished children.14 16 17 35 Consequently, underweight children may be more vulnerable to malaria infections and increased malaria incidence due to their weak immune systems.36 37 Malnutrition, both acute and chronic, is known to affect innate and adaptive immunity, and the immune system in malnourished individuals may be compromised at various levels. Severe acute malnutrition in infants and under-5 children is associated with thymus atrophy resulting in reduced T cell numbers and consequently maldevelopment of peripheral lymphoid organs, that is, spleen and lymph nodes.38–40 Innate immune defects such as impaired skin and gut immunity, defective antigen presentation due to reduced numbers of circulating dendritic cells, reduced microbicidal activity of granulocytes etc are observed in malnourished individuals.38 41 On the other hand, reduced levels of soluble IgA, low numbers of circulating B cells, atrophy of lymphoid organs and reduced delayed-type hypersensitivity responses constitute some of the adaptive immune defects attributed to malnutrition.41 With chronic malnutrition, long-term immunological defects such as reduction in the number of white cell count (leucopenia), decreased ratio of CD4/CD8 functional T cells, excess of undifferentiated lymphocyte numbers and low serum complement activity are observed.42 A deficiency of micronutrients such as vitamins A, B, C and E, zinc, carotenoids and folic acid is also shown to tip the balance in favour of malaria pathology.43 Therefore, underweight children may exhibit multiple immunological defects and consequently may not be able to mount appropriate immune responses to defend against malaria parasites. On the other hand, anaemia is mostly present as an obligatory manifestation of malaria in high-transmission settings.44 Anaemia is usually well described in children and women; however, its high prevalence among men residing in endemic districts is particularly intriguing and thus far is an overlooked public health issue. In India, the prevalence of anaemia is high in the age group 15–54 years.45 Anaemia among men in India is multifactorial with age, poverty, poor diet, tobacco consumption and being underweight as some of the contributing factors among many.45 A rural residence is also a risk factor and we speculate that the occupational practices such as agriculture, labourers, etc in such areas might enhance exposure to vectors and finally lead to malaria and associated anaemia.45
This is a pioneering study that highlights existing knowledge gaps in our understanding of malaria and malnutrition correlations in the Indian context. The current analysis indicates that all districts with malaria had a significant proportion of undernutrition. The populations are trapped in the well-known vicious cycle of malnutrition and infectious diseases, which is reflected in this analysis as well. There is an urgent need to generate evidence on the predisposition of malnourished people to malaria and their therapeutic responses to standard doses of anti-malarial drugs. In addition, the public health national programme needs to take into cognisance the presence of malnutrition in malaria-endemic areas and take steps to address both simultaneously as is being done in TB in the Indian TB programme.
Overall, the study underscores malnutrition and anaemia as important confounders influencing malaria epidemiology in the endemic states of central and eastern India. The mal–mal relationship dissected here calls for a comprehensive approach to malaria control that includes integrating nutrition programmes with disease control interventions in these regions.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval is not required for this study as it is an analysis of secondary data.
Acknowledgments
We are very thankful to the Directorate of NCVBDC for providing data and ICMR-NIMR for all logistical support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Alberto L Garcia-Basteiro
CPY, SSAH, SP and SS contributed equally.
Contributors AS (guarantor) conceived, designed, supervised and reviewed the study. CPY, SSAH,SP & SS extracted data, analysed the data and wrote the manuscript equally. MR and PKB critically appraised the paper, analysed the data and cowrote the manuscript. All authors participated in finalising the draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.