Article Text

Abstract
Nationalism has trumped solidarity, resulting in unnecessary loss of life and inequitable access to vaccines and therapeutics. Existing intellectual property (IP) regimens, trade secrets and data rights, under which pharmaceutical firms operate, have also posed obstacles to increasing manufacturing capacity, and ensuring adequate supply, affordable pricing, and equitable access to COVID-19 vaccines and other health products in low-income and middle- income countries. We propose: (1) Implementing alternative incentive and funding mechanisms to develop new scientific innovations to address infectious diseases with pandemic potential; (2) Voluntary and involuntary initiatives to overcome IP barriers including pooling IP, sharing data and vesting licences for resulting products in a globally agreed entity; (3) Transparent and accountable collective procurement to enable equitable distribution; (4) Investments in regionally distributed research and development (R&D) capacity and manufacturing, basic health systems to expand equitable access to essential health technologies, and non-discriminatory national distribution; (5) Commitment to strengthen national (and regional) initiatives in the areas of health system development, health research, drug and vaccine manufacturing and regulatory oversight and (6) Good governance of the pandemic prevention, preparedness and response accord. It is important to articulate principles for deals that include reasonable access conditions and transparency in negotiations. We argue for an equitable, transparent, accountable new global agreement to provide rewards for R&D but only on the condition that pharmaceutical companies share the IP rights necessary to produce and distribute them globally. Moreover, if countries commit to collective procurement and fair pricing of resulting products, we argue that we can greatly improve our ability to prepare for and respond to pandemic threats.
- Public Health
- Health policy
- Health systems
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
To date, more than 6 million people have died from the pandemic (with COVID-19-period excess mortality much higher) and some estimate that a more equitable distribution of vaccines could have saved 61% of the deaths.
The world has agreed to strengthen the International Health Regulations and to thrash out a potentially legally binding instrument that would set targets and responsibilities for various stakeholders involved in pandemic preparedness and response.
To help everyone access essential counter-measures in pandemic times, we propose a six pronged approach that argues for an equitable, transparent, accountable new global governance structure that oversees the replacement of the financial incentives of intellectual property exclusivities by rewards for research and development but only on the condition that pharmaceutical companies share the intellectual property rights necessary to produce and distribute essential health technologies globally.
We also argue for the global governance structure to oversee collective procurement, and support investments in regionally distributed research and development and manufacturing capacities, and strengthened health systems.
Our proposal makes actionable key ideas in section 5 of the International Panel on Pandemic Preparedness and Response’s recommendations and provides to the Intergovernmental Negotiating Body drafting the pandemic prevention, preparedness and response accord an outline of how an accord that supports equitable access to essential health technologies for all might be implemented.
If countries commit to collective procurement and fair pricing of resulting products, we argue that we can greatly improve our ability to prepare for and respond to pandemic threats
Introduction
The global response to the COVID-19 pandemic faltered: Nationalism trumped solidarity despite a call for joint action against this and future pandemics signed by 25 heads of state and several international organisations.1 The joint call made a plea for an international treaty for pandemic preparedness and response. The 1-year period following that call has seen significant progress and exposed some stark political realities. The world has agreed to strengthen the International Health Regulations and to thrash out a potentially legally binding convention, agreement or an international instrument (provisionally called the “pandemic prevention, preparedness and response accord”) that would set targets and responsibilities for various stakeholders involved in pandemic preparedness and response.2 This is good news. But this pandemic has also revealed that solipsistic sovereignty and self-interest trump existing treaties or agreements if they are not legally binding.
Whether or not the proposed accord will live up to global expectations for fairness and solidarity remains to be seen, however, as currently formulated, it does not address international and national intellectual property (IP) regimens (patents, copyrights, industrial designs, trade secrets and data rights) that negatively impact equitable access to pandemic health technologies. This means that pharmaceutical firms will continue to enjoy IP exclusivities that pose direct obstacles to increasing manufacturing capacity, and ensuring adequate supply, affordable pricing, and equitable access to COVID-19 and future pandemic vaccines, diagnostics, therapeutics and other health products in low-income and middle-income countries (LMICs). Within the World Trade Organization (WTO) framework, despite a push for a temporary waiver of IP rights on COVID-19 medical countermeasures by many LMICs, the recent WTO Ministerial Decision offers only a highly conditional compulsory licensing (CL) solution for patents that only covers export of vaccines to eligible developing countries.3 4 Though there was an initial 6-month window to extend the ‘solution’ to diagnostics and therapeutics, including the outpatient antivirals now widely available in the global North, this deadline was not met and has been further extended. Thus, the current state of affairs falls far short of the vision of a world that works together to fight global health emergencies through IP waivers and technology transfer (TT) initiatives that support alternative producers in poorer countries in making vaccines, diagnostics, therapeutics and other medical countermeasures and providing them equitably and affordably to their populations.5 Moreover, we support investments in basic health systems to buttress other aspects of pandemic preparation and response—from surveillance, testing, treatment, tracing and isolation capacity for a variety of potential pandemic threats, to investments in new manufacturing sites—and detail how representative governance at the global level can advance not only procedural justice and legitimacy but also enhance efforts for equitable allocation and uptake of these technologies. Our proposal makes actionable key ideas in section 5 of the International Panel on Pandemic Preparedness and Response’s recommendations.6
Because the WTO Ministerial Decision does not directly provide a solution for future pandemics, the proposed pandemic preparedness and response accord is our next chance to pre-emptively remove IP barriers to what should be global public goods. Now is the time for the international community to work together to ensure that the proposed treaty includes a robust regimen for the development of, and access to, essential health technologies required for the effective management of any pandemic; such a treaty must also enable health systems strengthening so that pandemic countermeasures can actually be delivered to all in need. In our opinion, Perehudoff et al offer the best worked out proposal for ensuring access to essential health technologies. They suggest that a global treaty should be guided by the ethical principles of solidarity, transparency and inclusive governance, and propose seven areas for action in order to support global sharing of IP, know-how, and technology for equitable access to medical countermeasures.7 We agree with these authors, but go beyond their proposals in specifically responding to the question ‘what provisions or mechanism(s) might ensure that the pandemic accord ensures equitable access to essential health technologies for all?’ Specifically, we suggest licences for new technologies be vested in a well-governed international organisation and that funding for research and development (R&D) of essential health technologies at the international level be tied to strong access conditions well before the declaration of a pandemic of international concern. We also advocate for collective procurement with fair pricing so that the international community can help recoup investment costs in R&D and support future development and basic health systems. Finally, we detail how representative governance efforts can advance not only procedural justice and legitimacy but also enhance equitable allocation and uptake of essential health technologies.
Our proposal
We propose an enhanced global mechanism embodied in the pandemic prevention, preparedness and response accord that holds everyone accountable (see figure 1). This mechanism should be well-governed and requires pooling IP and data, patent, trade-secrets and copyright waivers, and TT in return for a reward for innovation in order to speed up R&D of, and fair access to, essential health technologies. By fair access we mean ensuring a robust, affordable, and equitable supply chain of public health related technologies, through collective procurement, among other provisions, where we take equity to mean ensuring alignment of health resources with needs.

Key provisions of the proposed agreement. R&D, Research and Development.
In our opinion, each of these provisions is interlinked and essential for our proposal to work. As we have seen in the COVID-19 pandemic and the monkeypox outbreak, IP rights, while providing incentives for innovation, have also posed obstacles to equitable access, with a handful of companies with the IP rights retaining technological knowhow, and the capacity to manufacture vaccines and therapeutics without addressing the majority of the world’s needs. We propose an alternative regimen to overcome these barriers. But alternative incentives and funding mechanisms that support pooled IP and shared licensing can also fail, if the technologies developed through these mechanisms cannot be shared efficiently and equitably with all. That is why pillars one and two need to be supported by the third and fourth pillar. For a faster and more coordinated response, and to reduce duplication and fragmentation, innovation hubs that are interconnected, and share data and knowledge must be distributed around the world. Such innovation hubs will necessarily require support and funding from international organisations and funders, but unless host countries and regions take ownership of these innovation hubs, and take responsibility for supporting them, such top down initiatives may fail. That is why our fifth pillar is so important. National governments’ and the international community must commit to strengthening not only basic health systems to ensure equitable access to developed health technologies, but also health research systems, including manufacturing and regulatory structures, to support the establishment of innovation hubs mentioned in the fourth pillar. The running of such an interconnected system is however fraught with challenges. Entities that have the knowledge and the data need assurance that their data and expertise will be used responsibly and ethically. Including a neutral and trusted broker such as the World Health Organization (WHO) or any other similar entity in the deals—our sixth pillar—gives confidence and assurance to everyone that sharing expertise, knowledge, and the fruits of that knowledge will be universal and equitable.
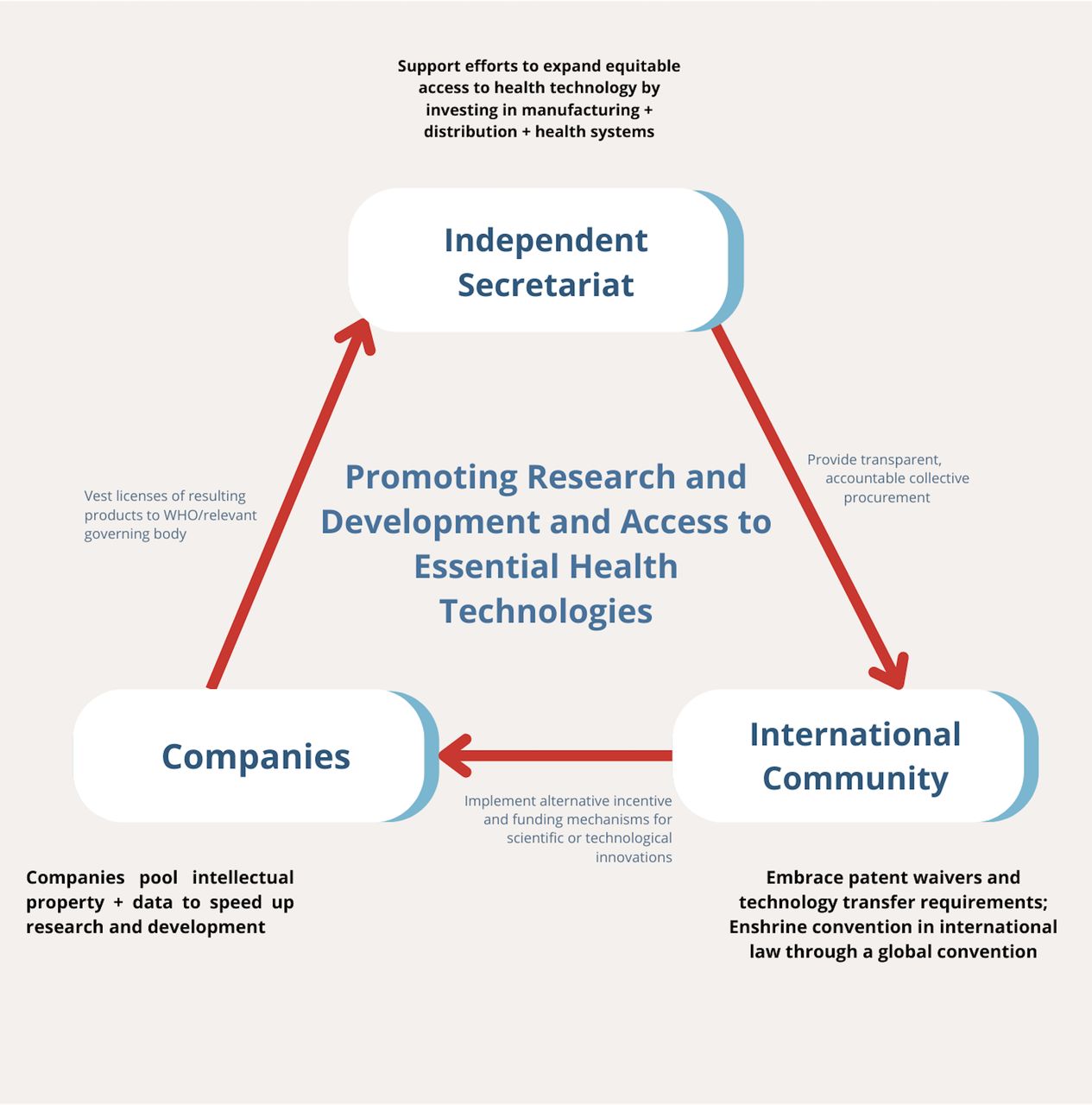
If countries agree to this proposal in negotiating a pandemic prevention, preparedness and response accord, they have ultimate responsibility for implementing its provisions but, to do so effectively, they must not only create a representative governance structure for guiding these efforts, the agreement should specify an international health organisation or organisations responsible for implementing its provisions. This organisation (or these organisations) would have responsibility for creating target product profiles for new products and negotiating agreements with industry, working with collective procurement organisations and funding hubs, etc. including liaising with pharma and biotech companies (see figure 2). Below, we detail each provision in turn.
{kind=link}
{kind=link}
Structure of the proposed mechanisms for promoting R&D and access to essential health technologies. R&D, Research and Development.
Implement alternative incentive and funding mechanisms to develop new scientific innovations to address infectious diseases with pandemic potential
The idea is to replace the rewards of IP exclusivities with alternative funding for essential health technologies for priority conditions on the WHO list of pandemic threats, including disease X and influenza, where current incentives and funding are insufficient to generate R&D and guarantee equitable and affordable access to resulting products. We also believe that all diseases and conditions, on which there are insufficient incentives and innovation, such as antimicrobial resistance, HIV, tuberculosis, and malaria should automatically gain eligibility for alternative funding and incentives.
The incentives for R&D might come in many forms, be tailored to different circumstances, and include both ‘push’ strategies—like direct funding and grants—and ‘pull’ strategies—like lump sum or milestone payments or prize funds—for new R&D.
We suggest that R&D funding be linked to the many different proposed, and, current innovative financing mechanisms for pandemic preparedness, wherein a proportion of these funds are earmarked for R&D on health technology innovations with a shared vision on scope.8–10 Fiscal bonds, levies on airlines tickets or internet-based products, etc., revolving funds from donor countries, social impact bonds are all instruments that are already being used for specific health programmes, including for R&D and could be reimagined for pandemic preparedness and response.11 12 The World Bank has recently set up the Financial Intermediary Fund which might designate resources for the same purpose.10 Andrew Lo, an economist from Massachusetts Institute of Technology, has proposed a subscription-based funding model, where countries would be required to pool a small amount per citizen in exchange for access to vaccines developed from those funds.13 Voluntary contributions from philanthropic organisations and compulsory contributions from signatories to any agreement implementing this proposal might also help generate the needed funds. Funding costs for developing multiple treatments range from US$50 to US$680 billion—much less than the estimated cost of the pandemic.14
Voluntary and involuntary initiatives to overcome IP barriers
The international community should, at a minimum, embrace IP waivers and TT requirements along the lines of the unsuccessful India/South Africa proposal for a temporary waiver on IP protections on COVID-19-related health technologies.15 An expert group has recently published seven key recommendations for overcoming IP barriers to address future pandemics with which the authors agree.7 In addition to these more systematic reforms, the WTO’s Agreement on Trade-Related Aspects of Intellectual Property Rights allows CL of patents on multiple grounds, including, with expedited procedures, for public health emergencies. CL guarantees ‘adequate remuneration’, i.e. incentives for innovation, but it should also be interpreted to allow CLs on trade secrets and confidential information. However, country-by-country, product-by-product compulsory licences are often administratively burdensome and politically risky. Therefore, rules streamlining and broadening CL procedures and removing export restrictions should be adopted and mechanisms for coordination of CLs should also be pursued.
Since IP barriers and TT refusals should not stand in the way of equitable access, we also recommend that rewards/incentives mentioned above be conditional on pooling IP, sharing data, and vesting licence for resulting products in a globally agreed entity. Existing international health initiatives and organisations demonstrate that it is possible to provide compensation for IP-free technology acquisition at reasonable rates.16 17 However, as a condition of receiving the incentives, it is essential that companies share IP and all the other relevant knowledge and data relevant to development (including preclinical and clinical trial results) and manufacturing, and vest the licence in the WHO COVID-19 Technology Access Pool (C-TAP) (reorganised as a Pandemic TAP, P-TAP) or as specified by a global agreement (though for the remainder of this article we will suppose the selected organisation is C-TAP or P-TAP). This will encourage and empower companies to build on each other’s scientific research and support and speed up production of new vaccines and technologies.18 C-TAP or its P-TAP alternative would then be able to licence out production to alternative (eg, generic) manufacturers, including those in LMIC regions as proposed through C-TAP, the WHO mRNA Tech Transfer Hubs, and the Medicines Patent Pool (MPP) for COVID-19 technologies. P-TAP can licence production on specified access (affordable cost and equitable distribution) conditions.
Current estimates of R&D drug costs range from US$43.4 to US$4200 million.19 To ensure that the incentives are appropriate to guide future R&D investments, companies must share data on current R&D costs. Incentives for new innovations must cover these costs, the risks of failure and the risk of not being the first to produce a product fulfilling a specific profile, but calculating the exact size and methodology of awarding incentives is beyond the scope of this paper. Modelling of disease infectivity rates, estimates of pandemics’ likelihood, and information on interventions’ effectiveness from clinical trials and treatment access may inform rewards for preventative treatments. Incentivising companies in this way delinks companies’ profits from sales and ties them to good health consequences instead. Moreover, some suggest rewarding pharmaceutical companies and other R&D organisations for new innovations based on their health impact. To this end, good measures of health impact exist.
Transparent and accountable collective procurement to enable equitable distribution
The proposed pandemic accord should support a rational procurement system that includes pooled procurement, but under an equitable allocation framework. This framework should ensures equitable, timely, and global distribution according to allocation principles and at price points in LMICs established by C-TAP or P-TAP. Procurement efforts should involve pooled contracted negotiation on prices of essential health technologies globally as well as information sharing on budgeting, pricing, forecasting and the legal landscape. However, collective procurement may also include pooled contracting, acquisition, logistics, and delivery of these technologies where helpful to support country efforts and may involve a gradual scale up of UNICEF, regional procurement organisations such as the African Medicines and Supplies Platform, and/or related distribution efforts.20 We propose C-TAP or P-TAP licence the products to manufacturers with licensing fees and conditions that support collective procurement efforts and at price points that allow them to recoup the costs of investment and support the development of new manufacturing capacity, investments in cold chains, and other aspects of demand and supply development necessary for vaccine deployment and uptake.
Investments in regionally distributed R&D capacity and manufacturing and basic health systems to expand equitable access to essential health technologies and ensure non-discriminatory national distribution
For technologies to be accessible, available, affordable and adapted for use in LMICs, manufacturing capacity for all necessary medical countermeasures such as vaccines, therapeutics, diagnostics, personal protective equipment, basic medical supplies, etc. must be distributed globally. This requires global efforts to strengthen and use LMIC research capacity and regionally distributed biopharmaceutical and diagnostic manufacturing capacity. A very promising initiative that includes both of these features is the WHO mRNA TT Hub. The Hub is developing a Moderna-like mRNA vaccine (an improved, more heat stable version of the same), and additional applications of mRNA technologies to address other pressing health needs.21 The Hub’s innovations, commercial manufacturing know-how, and clinical trial data will be shared with at least 15 spoke companies in other underserved LMIC regions who will be authorised to clone the relevant technologies. The model combines open access initiatives to expedite and coordinate research and to share knowledge with a commitment to democratise supply and ensure more equitable access to more affordable medical countermeasures.
Commitment to strengthen national (and regional) initiatives in the areas of health system development, health research, drug and vaccine manufacturing and regulatory oversight
To be party to the proposed pandemic prevention, preparedness and response accord, countries should commit to strengthening their health and community systems, including their health delivery systems, with external assistance to help develop health service capacity in lower income countries. Without such a commitment, countries risk perpetuating a colonial model of neglect for health technology delivery. Strong health systems require a robust policy environment, strong health governance and leadership, and coordination mechanisms at country, regional and global levels. They also require investments in data, monitoring, evaluation and surveillance systems, and importantly, in both skilled and community health workers. Priority in many LMICs should go to expanding, and strengthening community systems and community-led interventions such as health information, education and communication strategies, demand generation and outreach.
Finally, countries must commit to non-discriminatory national delivery of pandemic-related health services, reaching most-vulnerable and hard-to-reach populations and ensuring gender equity. The least developed countries may not have adequate capacities even for strengthening their health systems. The proposed legally enforceable pandemic accord must include language that requires establishing regional centres of excellence to support health systems development in the least developed countries of that region, taking into consideration their sociocultural needs and economic background. These centres could also provide support to the more advanced countries in the area of drug and vaccine R&D, and manufacturing, including regulatory oversight.
Good governance of the pandemic prevention, preparedness and response accord
The existing global response architecture is not fit for purpose, because it does not represent the interests of all those affected by pandemics. A pandemic accord should be supported by good governance and enforcement mechanisms to create the proposed incentives for new product development and ensure collective procurement and equitable access to essential health technologies.
The governance for the coordination mechanism, or independent secretariat, that we propose should embrace decolonisation at its core and fully represent the interests of the global population, especially LMICs; it should be accountable, transparent and representative of a wide set of stakeholders such as, but not limited to, patient groups, healthcare provider representatives, civil society, philanthropic organisations, and policy makers, both in high-income countries (HICs)s and LMICs.22 Countries negotiating the agreement should be bound to act in the common interest rather than primarily as representatives of their own populations. The secretariat must have proportional representation of LMIC governments and experts not only in leadership roles and throughout the governance structure, but at all levels; not just as tokens but in ways that are meaningful and numbers that are proportionate to LMIC populations and diverse LMIC perspectives. Experts and civil society organisation (CSO) voices that represent marginalised populations, minorities, populations across the life-cycle continuum, and diverse gender perspectives must also be included in the governance mechanism; not only towards the end of the process but early on—for example, in setting priorities for effective pandemic preparedness and response. The secretariat must be responsive to indigenous and community-based knowledge and beliefs, equitable and effective, and transparent and accountable. Terms of reference should be devised for this purpose, stating clearly who will be entitled to participate in the mechanism’s design, as well as how the processes of deliberation and decision will take place.23 Ideally, LMIC stakeholders will have sufficient power and control over resources so that the most affected have the largest voice and influence over decisions and outcomes. It is not enough to be ‘consulted’, or merely ‘informed’, about predetermined decisions. Nor should stakeholders be manipulated, placated, or expected to engage in implementing decisions over which they have no effective influence. Rather, representatives should have full and equal rights to meaningful participation and co-creation, which will engender trust, catalyse political buy-in, and help stimulate demand for—and uptake of—new technologies.
The Global South has strong grounds for distrusting continuing colonial practices and attitudes given the consistent failure of the Global North to share resources and decision-making rights. If the international community embodies true inclusion, participation and governance rights in the pandemic prevention, preparedness and response accord, it can enhance solidarity and trust. If government and CSO representatives are involved from the beginning, and make contributions that are reflective of the beliefs and knowledge of the people in the community, rather than being pressured to simply endorse the status quo, they can advance equitable access to essential health technologies.
The accord must also be backed by enforcement mechanisms consistent with existing and evolving international law.24 Mechanisms might include penalties for non-compliance, and benefits for participation, such as capacity building support for LMICs in strengthening basic health systems, and TT before the onset of major pandemics so that they are prepared to respond. Though tax and trade penalties and overcoming IP barriers may require modifying existing rules under the WTO, it also requires countries willing, and able, to enforce such measures. Civil society may help secure countries’ participation and address breaches of the agreement by informing public opinion, be part of decision-making processes, and contribute important grass root perspectives.24
Cooperation to develop preventive measures and treatments in non-pandemic times may make it easier to sustain cooperation in future pandemics. A well-designed legal agreement can help provide clarity on what is required by member states prior to and during a pandemic, whether they are conducting themselves in line with their commitments, and possibly even foster avenues for correcting deviations. It can provide a process for resolving disagreements, helping to get people to the table. Moreover, it may be more difficult to deviate from procedures as they become ingrained in many other systems.
Defending the proposal: global cooperation, solidarity and human rights
Principles of solidarity (which we take to be the sympathetic and imaginative enactment of collaborative measures to promote everyone’s flourishing and specifically, in this context, equitable access to essential health services), human rights (as articulated in the Universal Declaration of Human Rights and other international treaties and instruments), and justice (which at least requires fair distribution and access to essential health technologies), all provide strong ethical reasons to implement our proposal. As the recent pandemic has shown, lack of preparedness, cooperation and solidarity leads to unequal distributions of healthcare technologies and, partly for this reason, inequities in the health impact of the disease. In order to reduce the impact of pandemics in the future, we must strengthen our pandemic preparedness and response in a way that recognises the mutual responsibilities of all stakeholders. Our proposal provides a path forward for such preparations.
Moreover, previous global health initiatives provide some reason to believe that the international community can make the kind of agreement we propose. Some global health organisations like Drugs for Neglected Disease Initiative and Medicines for Malaria Venture have succeeded in securing licences and good access terms in their R&D investment agreements.16 17 Others like the MPP have secured significant licences sharing IP as well as other data and knowledge necessary to ensure access to essential health technologies.25 The MPP estimates that its licensing efforts will have saved 36 million patient years by 2027 by yielding lower cost treatments.26 Likewise, in 2021, UNICEF delivered approximately 45% of the vaccines for children under five globally, and other pooled procurement mechanisms—from the WHO Procurement Platform, Pan American Health Organisation, UNICEF, the Global Fund, and the African Medicines and Supplies Platform—also provide access to essential health technologies with significant cost-savings.27–29
Some might suggest that instead of supporting our proposal to remove IP barriers through voluntary and involuntary measures, the international community could just provide more funds for pandemic-related R&D and still let pharmaceutical companies keep the patents, trade secret protection, and maintain other exclusive rights on their technologies. They will point to the rapid development, and scaled-up production, of COVID-19 vaccines, diagnostics and therapeutics to argue that the current IP-based incentive system produces consistent results by providing stable incentives for innovation and contract manufacturing agreements. More recently, they might point to the International Federation of Pharmaceutical Manufacturers’ Association’s Berlin Declaration, where industry promises to take additional steps to scale-up supply to LMICs if a stable IP system is preserved and if donors provide guaranteed funding for low-profit or no-profit sales to the poorest countries.30
The rhetoric that the R&D system works well and we just need to solve the access problem ignores evidence that the status quo system has consistently produced rampant health inequality precisely because of the incentives it creates. The current R&D system works well for the wealthy, but it almost always fails to serve the poor. Even during the current pandemic, with minor and recent exceptions, most pharmaceutical firms simply did not voluntarily join C-TAP, the WHO mRNA Tech Transfer Hub, or the MPP.31 This pandemic has demonstrated that companies are perfectly willing to accept public funds through Operation Warp Speed, the Coalition for Epidemic Preparedness Innovations, and other public and philanthropic funders, take additional government money to derisk their pandemic-related R&D and expand, fill and finish capacity that they control, and then just sell their technologies to the highest bidders. Moreover, historically, pharmaceutical companies have not invested enough in R&D addressing future pandemic threats. We believe public funding must come with stringent access conditions. We cannot leave it up to companies whether or not to share their technology and data, whether to expedite and expand supply, whether to lower prices, or whether to sell on anything other than a first-come, higher-price basis. We must make the rewards proportionate to companies’ actual investments and conditional on their sharing technology and data to ensure adequate supply, affordable pricing and equitable access.31
Yet others might argue for alternatives to our proposal that we believe are demonstrably worse. For instance, some may advocate for allowing bilateral supply deals within limits and for dose reallocations.32 Unconstrained bilateral purchasing contributed to vaccine and therapeutic nationalism and supply shortages in less powerful and less wealthy countries. Similarly, dose reallocation deals led to highly inequitable outcomes, perpetuating dependencies and the colonial model of global health. Vaccine reallocations were often delayed, sporadic, and unplanned for and involved disfavored vaccines and near expiry doses. Poor countries that simply did not have the time to distribute the doses before expiry sometimes received sanction for destroying them as directed by the WHO. While sharing innovations with countries that do not currently have the capacity or resources for manufacturing vaccines and therapeutics supports solidarity, the international community must also strengthen the agency of populations living in LMIC by supporting the development of national or regional innovation hubs in these regions.
Some may worry that a fully multilateral approach along the lines we advocate will require too much cooperation and that we ignore the self-interested power of HICs.32 33 Rich countries have undue influence over international health organisations because they pay a great proportion of their budgets and can also exercise significant influence over pharmaceutical companies within their boundaries. They may simply exit or renege on international agreements and, when it is in their best interest to engage in bilateral deals, pressure pharmaceutical companies to provide them priority access, or issue export prohibitions to secure scarce supplies.
For countries, feasibility of our proposal will be determined by the terms of the pandemic accord, but we believe that it is in the interest of all countries to collaborate and to implement the mechanism proposed here. As we have seen in this pandemic—‘No one is safe till everyone is safe’.34 The COVID-19 pandemic has shown that status quo approaches, where rich countries protect the interests of the biopharmaceutical industry and support existing trade rules, have actually prolonged and intensified the pandemic and its social, economic, and political impacts. Whether our proposal is feasible will also depend on countries’ ability to reign in unbridled corporate power, but there is reason for optimism. Expanded public expenditure on R&D, clinical trials, expanded manufacturing capacity, and advance purchase agreements all derisk or actively subsidise R&D, registration, and supply. Implementing these investments in conjunction with collective procurement and the other aspects of our proposal would obviate the need for companies’ to invest significantly in marketing and demand creation, lowering their costs. Moreover, our proposal secures the benefits of transparency and knowledge-sharing—saving time and resources throughout product development and across the supply pipeline. If the rewards for innovation are sufficient and threats of involuntary measures to secure equitable access are credible, pharmaceutical companies’ reluctant acquiescence is more likely. Agreeing to provide pandemic-related health technologies at set price points need not threaten their ability to develop and sell technologies for non-pandemic-related conditions in normal markets. Moreover, companies should be willing to forego potential future profits in pandemic times at reasonable rates as these profits are discounted by the uncertainty of a pandemic eventuating for which any particular product might be useful. In any case, this is an opportune moment to push for more radical change in governments’ regulation over the pharmaceutical sector. Significant civil society action may help get sign on and cooperating countries can use trade, tax and other incentives to encourage participation.
Some simply assume that the approach we advocate is not feasible, but we believe that what we can achieve together as an international community is up to us. Significant civil society action may help get sign on and, as noted above, countries can use trade, tax, and other incentives to encourage cooperation. Moreover, even the sceptics highlight the importance of many parts of our proposal and acknowledge that it is important to articulate principles for investments in essential health technologies that include reasonable access conditions, especially given the public funding provided for these technologies. They also stress the importance of transparency in negotiations, ensuring productive investments are made in manufacturing capacity, supply chain resilience, and sharing technical knowledge.33 Even aspirational or normative proposals that are not fully effective, such as an ideal of collective procurement and R&D guided by global health interests, can be important in practice—setting standards that allow criticism and civil society action for reform—even if they are never fully implemented.
To date, more than 6 million people have died from the pandemic (with COVID-period excess mortality much higher) and some estimate that a more equitable distribution of vaccines could have saved 61% of the deaths.35 36 Some predict that COVID-19 crisis will cost the world US$12.5 trillion over the next 2 years.37 Others estimate that vaccine nationalism alone has cost the world US$1.2 trillion.38 So, moving beyond bilateral deals and greatly enhancing the global preparedness and response architecture has the potential to save millions of lives and trillions of dollars.
Conclusion
What we can achieve together as an international community is up to us. We believe that every human being has a stake in the effective management of the next pandemic, and everyone—from states and the private sector to civil society—must work together and be held accountable. Absent this, adequate pandemic preparedness and response will remain a distant hope, and securing equitable distribution of pandemic-related health technologies to all people of the world, a dream. It is important to articulate principles for deals that include reasonable access conditions and transparency in negotiations. Unfortunately, in the current pandemic, wealthy nations have unethically bought most of the world’s COVID-19 vaccine and therapeutics supplies despite having a small proportion of the global population, leaving many countries with late and limited access to vaccines and medicines. Even those who can access the countermeasures often lack other health system resources they need to effectively combat the virus. Moreover, future pandemics may prove much more devastating without global cooperation. We have argued for an equitable, transparent, accountable new global agreement to provide rewards for R&D but only on the condition that pharmaceutical companies share the IP rights necessary to produce and distribute them globally. Moreover, if countries commit to collective procurement and fair pricing of resulting products, we have argued that we can greatly improve our ability to prepare for and respond to pandemic threats. We must work together to overcome the nationalism undermining our current global response plans to adequately address and prevent future pandemics.
Patient and public involvement
This paper did not involve patients or the public because the paper focuses on all potential pandemic diseases. However, it is the result of a year-long collaboration with scholars and public health practitioners from around the world and across the disciplines of law, bioethics, public health, and economics on pandemic preparation and response. Since there were no patients involved, the development of the research question and outcome measures were not informed by patients’ priorities, experience and preferences.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable
Acknowledgments
The authors gratefully acknowledge the financial assistance provided for this publication through the University of Gothenburg. We would also like to thank the Binghamton University Philosophy Department for their support. Moreover, we deeply appreciate the feedback we received from Kaushik Basu, Larry Gostin, Pedro Villarreal, Steven Hoffman, Johnathan Wolff, and José Szapocznik as well as audiences and colleagues at Drugs for Neglected Disease Initiative, the Pandemic Action Network, Rutgers Center for Population Bioethics, Cornell University, CRADLE/ Institute of Economic Growth (Dehli) Roundtable on Law and Economic Development, Bowling Green State University, Regis University, Oxford University, Merrimak College, and a series of virtual workshops organized in conjunction with the Blavatnik School of Government at Oxford University, Center for Global Development, and IRG-GHJ (https://www.irg-ghj.org/). Finally, we would like to thank Milan Patel, Diana Dedi, Julia Match, Annie Nguyen, and the Global Health Impact (https://www.global-health-impact.org/) team for their organization and research assistance.
Footnotes
Handling editor Seye Abimbola
Twitter @SaxenaBioethics, @atuire
Contributors All authors contributed to the conceptualisation of the manuscript. AS, BKB and NH contributed the majority of writing as lead authors. All authors helped shape the analysis, research and manuscript and provided critical feedback on drafts. NH led the discussions, organised the group, and is ultimately responsible for the article's content, as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.