Article Text

Abstract
Introduction Tuberculosis (TB) treatment interruption remains a critical challenge leading to poor treatment outcomes. Two-thirds of global new TB cases are mostly contributed by Asian countries, prompting systematic analysis of predictors for treatment interruption due to the variable findings.
Methods Articles published from 2012 to 2021 were searched through seven databases. Studies that established the relationship for risk factors of TB treatment interruption among adult Asian were included. Relevant articles were screened, extracted and appraised using Joanna Briggs Institute’s checklists for cohort, case–control and cross-sectional study designs by three reviewers. Meta-analysis was performed using the random effect model in Review Manager software. The pooled prevalence and predictors of treatment interruption were expressed in ORs with 95% CIs; heterogeneity was assessed using the I2 statistic. The publication bias was visually inspected using the funnel plot.
Results Fifty eligible studies (658 304 participants) from 17 Asian countries were included. The overall pooled prevalence of treatment interruption was 17% (95% CI 16% to 18%), the highest in Southern Asia (22% (95% CI 16% to 29%)), followed by Eastern Asia (18% (95% CI 16% to 20%)) and South East Asia (16% (95% CI 4% to 28%)). Seven predictors were identified to increase the risk of treatment interruption, namely, male gender (OR 1.38 (95% CI 1.26 to 1.51)), employment (OR 1.43 (95% CI 1.11 to 1.84)), alcohol intake (OR 2.24 (95% CI 1.58 to 3.18)), smoking (OR 2.74 (95% CI 1.98 to 3.78)), HIV-positive (OR 1.50 (95% CI 1.15 to 1.96)), adverse drug reactions (OR 2.01 (95% CI 1.20 to 3.34)) and previously treated cases (OR 1.77 (95% CI 1.39 to 2.26)). All predictors demonstrated substantial heterogeneity except employment and HIV status with no publication bias.
Conclusion The identification of predictors for TB treatment interruption enables strategised planning and collective intervention to be targeted at the high-risk groups to strengthen TB care and control in the Asia region.
- Tuberculosis
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Tuberculosis (TB) is an infectious disease that remains one of the leading public health threats with two-thirds of global new cases mostly contributed by Asian countries.
Interruptions throughout the treatment period jeopardise the treatment outcomes that lead to widespread community transmission, the emergence of drug-resistant cases and mortality despite the effective therapy.
Many studies were conducted in Asian countries to explore the potential factors, leading to TB treatment interruption but generated variable and inconsistent findings.
WHAT THIS STUDY ADDS
This is the first systematic review and meta-analysis that established pooled estimates of the predictors with regards to TB treatment interruption in the Asia region based on collective results from 50 studies in 17 countries over 10 years from 2012 to 2021.
It systematically concluded seven significant predictors associated with increased risk of TB treatment interruption, namely, male gender, employment, alcohol intake, smoking, HIV-positive, adverse drug reactions and previously treated TB cases.
The issue of early treatment interruption in the Asia region was also highlighted as shown by the higher prevalence of 28% when compared with 10% as per ‘lost to follow-up’ WHO criteria.
Potentially alarming regions were Southern, Eastern and South East Asia regions.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The identification of high-risk groups enables heightened vigilance from the beginning of therapy to prevent treatment interruption with the eventual achievement of successful outcomes.
This could assist in regional interventional strategies planning and extend as a collaborative strategy to optimise TB management and strengthen TB control worldwide.
Introduction
Worldwide, tuberculosis (TB) is the 13th leading cause of death and the second leading infectious killer after the outbreak of the COVID-19 pandemic in the early year 2020.1 Although there has been a downward trend in TB incidence from 2015 to 2020, TB mortality has increased to approximately 1.5 million in 2020 during the COVID-19 pandemic, returning to its 2017 level.1 The unprecedented global pandemic had tarnished the hard gains in combating TB thus far, risking patients with TB due to disruptions to services and optimum management.
According to the WHO report in 2020, six out of eight TB-burdened countries accounted for two-thirds of global TB cases are located in Asia: India, China, Indonesia, Philippines, Pakistan and Bangladesh.1 Despite its high endemic problem, TB is curable and preventable. The standard TB treatment requires a minimum duration of 6 months for drug-susceptible cases, while the overall duration can span up to 2 years in drug-resistant cases.2 The lengthy therapy is, thus, the main challenge in ensuring therapy adherence, which is the cornerstone of successful TB treatment outcomes.3 Treatment interruption, default or non-adherence is complex, dynamic and attributed to many inter-related causes. Apart from treatment-related factors, other factors such as social-demographic, cultural, economic burden, patient’s knowledge, attitudes and beliefs, family, community and health system support are among the factors that could affect adherence status.4 5 As the influences of these risk factors differ across regions, countries and populations, many studies were conducted globally to understand the various aspects of treatment interruptions ranging from its aetiology to interventions, especially in high TB prevalence countries.4–6
Issues of early treatment interruption 2 weeks or more during the intensive phase have always been a concern among TB treatment providers as it warrants treatment to be restarted.7 However, WHO is advocating interruption of at least 2 consecutive months as per ‘lost to follow-up’ treatment outcome, which is rather a huge gap between early treatment interruption and outcome assessment.8 Knowing the risk of early treatment interruption, which can lead to unfavourable treatment outcomes, numerous studies have been conducted in an attempt to address the problems in the early treatment phase.9 10
Resulting from treatment interruption, a 10-fold increase in poor outcomes accounted for treatment failure mostly was reported.9 As TB is highly contagious, it poses a substantial threat to the health of the nation, given the greater risk to acquire drug resistance among the defaulters.11 This imposed high treatment costs, increased morbidity and mortality with the emergence of drug-resistant strains.12 The vicious cycle will never end as long as TB treatment interruption remains unresolved.
Given the high TB burden in the Asia region and considerable detrimental impacts of treatment interruption, there is a dire need to analyse systematically the prevalence and risk factors of TB treatment interruption, which varied across studies. This could assist in formulating tailored intervention strategies in the regional context to better manage treatment interruption issues.
Methods
Protocol development
A systematic review and meta-analyses were conducted by reviewing studies of TB treatment interruption in the Asia region. The review protocol was registered in the International Prospective Register of Systematic Review (PROSPERO) on 5 February 2022 bearing the registration number CRD42022295732. Each section in this article was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline.13
Study design
This review included primary quantitative studies. As factors with regards to TB treatment interruption were being assessed, only observational studies with the cohort, case–control and cross-sectional study design were reviewed. According to the NHMRC hierarchy of evidence with aetiology as the research question, prospective cohort, retrospective cohort, case–control and cross-sectional studies were ranked as levels II, III-2, III-3 and IV, respectively.14
Eligibility criteria
The eligibility criteria were delineated and classified based on the PECO acronym (Population, Exposure, Comparator, Outcome).
Population
Adult Asians on TB treatment with treatment interrupters forming a subset of the study population were included. Studies that focused solely on retreatment cases, latent TB, extrapulmonary TB and drug-resistant TB were not accounted for, given the complexity of the illness, substantial variation in the treatment regimen and/or treatment courses could potentially affect treatment adherence, which was the main outcome of interest in this review. Although pulmonary TB was the main focus of this study, studies with heterogeneous populations such as pulmonary with extrapulmonary TB, drug-sensitive with drug-resistant TB and studies with a combined cohort of children and adults were included.
Exposure
The exposure was risk factors of TB treatment interruption such as social demographic characteristics, lifestyle factors, comorbidities, disease or treatment-related factors.
Comparator
Patients without risk exposure served as the comparator in the included studies.
Outcome measures
This review was focusing on TB treatment interruption, which was defined as the discontinuation of medications, clinic visits or follow-ups either consecutively or non-consecutively throughout the treatment period. There should be an association or relationship of treatment interruption established in the studies with regards to the factors being investigated. Apart from predictive factors, the prevalence of treatment interruption based in different Asia regions was also analysed.
Search strategy
Articles were comprehensively searched through Ovid MEDLINE, Embase, CINAHL, Scopus and Web of Science databases that were published over the past 10 years from January 2012 to December 2021. Grey literature was searched using Google-Advanced (first 100 articles) and ProQuest Dissertations and Theses Global databases. References of identified articles were also screened to retrieve other potential studies that fulfilled the eligibility criteria. The PECO acronym was used to develop the key terms. The terms were: tuberculosis, factors, determinants, predictors, treatment interruption, treatment default, adherence, non-adherence and treatment outcome. The combination of the terms via Boolean operators “OR” or “AND” were used during the search process adapted to each electronic database (online supplemental table S1).
Supplemental material
Data screening and extraction
All records identified through research databases were exported to EndNote to remove duplicates. The first screening was done based on the title and abstract by the first reviewer (ALO). Full-text reviews of the included studies were then conducted thoroughly to assess the fulfilment of the eligibility criteria. Non-English articles were translated using Google Translate. Non-eligible studies were excluded during the full-text review process with explicit reasons stated.
The data such as author, year of publication, study design, geographical location, population characteristic, risk factor, number of subjects with treatment interruption, the total number of subjects included in the study and duration of treatment interruption were extracted in the standardised Excel spreadsheet. The risk factors recorded in binary outcomes encompassed sociodemographic (gender, age, marital, education and employment status and location of residence (urban vs rural)), lifestyle factors (alcohol intake and smoking status), commonly reported comorbidities (HIV and diabetes) and disease-related and treatment-related factors (types of TB cases, site of TB infection, sputum smear at baseline and adverse drug reactions (ADRs)). Both data screening and extraction were verified by the second reviewer (MM-B). In case there were disagreements, the third reviewer (FI) was consulted to solve for consensus which was regarded as the final decision.
Methodological quality assessment
The methodological quality assessment of included studies was carried out by two reviewers (ALO and MM-B) independently using Joanna Briggs Institute’s (JBI) critical appraisal checklist. The discrepancies were resolved on discussions or seeking an opinion from the third reviewer (FI). The checklists for cohort, case–control and cross-sectional studies comprised 11, 10 and 8 questions, respectively.15 The possible answers were ‘yes’, ‘unclear’, ‘no’ or ‘not applicable’ with one mark allocated for the fulfilment of each criterion or a zero mark otherwise. The total scoring was summed up in percentages to serve as a comparison to examine the methodological quality of the studies.
Data synthesis and analysis
The meta-analysis was performed using Review Manager software V.5.4 (Nordic Cochrane Centre). The prevalence for each study was derived from the number of subjects with treatment interruption to the total number of subjects included in the study. The pooled estimates of prevalence and predictors were analysed using the inverse variance method with a random effect model to generate ORs with 95% CIs. The heterogeneity of the studies was assessed using I2 statistic with its categorisation outlined as follows: 0–40% (not important), 30–60% (moderate), 50–90% (substantial) and 75–100% (considerable).16
Subgroup analyses for prevalence were carried out based on Asia regions (Southern Asia, Eastern Asia, South East Asia, Western Asia and Central Asia) and the duration of treatment interruption (≥2 months vs minimum<2 months). Region-based subgroup analyses were also conducted for predictors such as gender, marital status, and previously treated cases where appropriate. As there were substantial variations in the categorisation of age, two subgroups (age ≥60 and ≥65) were stratified. Sensitivity analyses were also performed by omitting studies with wide variations of the duration of treatment interruptions versus studies that specifically defined treatment interruption of ≥2 months to test whether there were substantial changes in the overall effect size for each predictor. The publication bias among studies was visually inspected using the funnel plot. This was performed for factors that showed statistically significant results with at least 10 studies included in the pooled estimation.
Results
The initial article search generated 9427 records. After removing duplicates and initial screening, 74 were eligible for full-text review. Out of these, 50 articles that fulfilled the eligibility criteria were eventually included for systematic review and meta-analysis. PRISMA guideline was adopted to present the flow of this review (figure 1). The reasons for studies exclusion are summarised in online supplemental table S2.

PRISMA flowchart of the review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Methodological quality assessment
This review comprised a majority of cohort studies (26), followed by cross-sectional (15) and case–control studies (9). Based on the JBI critical appraisal checklist for three study designs, 48 studies (96%) scored more than 60% with non-fulfilment of three criteria or below. The remaining two studies did not fulfil five criteria in the cross-sectional (3/8, 38%) and cohort (6/11, 55%) checklists, respectively. (online supplemental table S3).
Characteristics of included studies
The 50 eligible studies were conducted in 17 countries from five regions in Asia. Southern Asia (n=20) comprised the most with the majority from India (n=15), followed by Eastern Asia (n=15) with the majority from China (n=8) and South East Asia (n=7), which was mostly contributed by studies from Indonesia (n=4), while the remaining of the studies were from Western Asia (n=5) and Central Asia (n=3). The total number of participants included in this review was 658 304, with approximately three-quarters from the Eastern Asia region (n=4 79 986, 72.9%). There were substantial variations in defining TB treatment interruption across the studies, ranging from ≥1 day to ≥2 months. More than half, 28 out of 50 studies considered treatment interruption of ≥2 months based on the definition of ‘lost to follow-up’ in assessing TB treatment outcome by WHO (table 1).
Characteristics of the included studies based on the Asia region (n=50)
Prevalence of TB treatment interruption
Thirty-nine studies were accounted for pooled prevalence analysis, which included 32 020 treatment interrupters out of 654 872 populations in the study cohorts. All case–control studies and one cross-sectional study were excluded due to a fixed ratio sampling between treatment interrupters and non-interrupters,17–26 while another cross-sectional study included all interrupters in the study population.27 The overall pooled estimated prevalence for the Asia region was 17% (95% CI 16% to 18%). The highest pooled prevalence was noted in Southern Asia (22% (95% CI 16% to 29%)),28–42 followed by Eastern Asia (18% (95% CI 16% to 20%)),43–55 South East Asia (16% (95% 4% to 28%)),56–61 Western Asia (10% (95% 5% to 15%))62–64 and Central Asia (6% (95% CI 5% to 7%)).65 66 (figure 2) Subgroup analysis based on the duration of treatment interruption (36 studies, excluded non-defined duration of treatment interruption), demonstrated the pooled prevalence for ≥2 months interruption was 10% (95% CI 9% to 11%), which was much lower than another subgroup that considered the minimum duration of <2 months, 28% (95% CI 20% to 36%) (online supplemental figure S1).
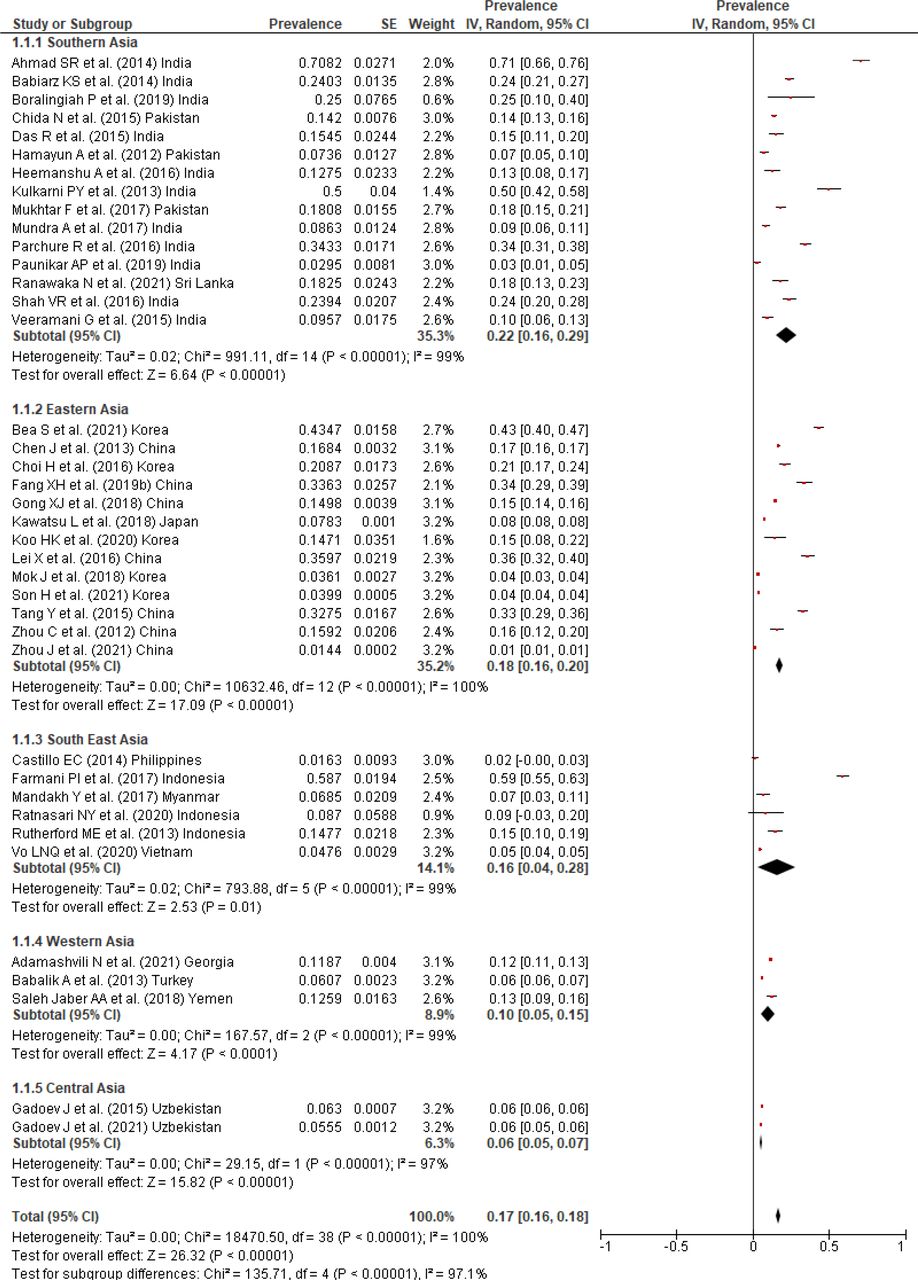
Prevalence of TB treatment interruption in the Asia region (n=39). TB, tuberculosis.
Predictors associated with TB treatment interruption
Out of 14 potential factors tested, 7 showed significant findings as follows, which were presented based on four major groupings such as sociodemographic, lifestyle factors, comorbidities and disease and treatment-related factors.
Sociodemographic factors
Gender
A total of 37 studies were included in the pooled estimation for treatment interruption associated with gender. The male gender was more likely to interrupt TB treatment as compared with the female gender (OR 1.38 (95% CI 1.26 to 1.51)) with a significant degree of heterogeneity between the studies (I2=79%, p<0.001). Region-based pooled estimates showed that male gender was consistently more prevalent towards TB treatment interruption in the Southern (OR 1.51 (95% CI 1.16 to 1.95)), Eastern (OR 1.19 (95%CI 1.06 to 1.32)), Western (OR 2.29 (95% CI 1.90 to 2.74)) and Central Asia (OR 1.46 (95% CI 1.20 to 1.77), except South East Asia region (table 2, figure 3).
Summary of the predictors of TB treatment interruption

Pooled estimate of the male gender as a predictor of TB treatment interruption. TB, tuberculosis.
Employment status
Employed TB patients showed a higher risk of treatment interruption by 43% as compared with those unemployed (OR 1.43 (95% CI 1.11 to 1.84)). No significant heterogeneity was observed among the nine studies (I2=23%, p=0.24) (table 2, online supplemental figure S2).
Lifestyle factors
Alcohol intake
Alcohol consumption posed an increased risk of TB treatment interruption as compared with no alcohol intake (OR 2.24 (95% CI 1.58 to 3.18)). There was significant heterogeneity noted across the 13 studies (I2=58%, p=0.004) (table 2, online supplemental figure S3).
Smoking
Patients who were known to be a smoker demonstrated a higher risk of experiencing TB treatment interruption as compared with non-smokers (OR 2.74 (95% CI 1.98 to 3.78)). However, significant heterogeneity was observed across the 14 studies (I2=66%, p<0.001) (table 2, online supplemental figure S4).
Comorbidities
HIV status
TB-HIV coinfection showed 1.5 times higher risk of treatment interruption as compared with negative HIV status (OR 1.50 (95% CI 1.15 to 1.96)) with homogeneous data in five studies (I2=1%, p=0.4) (table 2, online supplemental figure S5).
Disease and treatment-related factors
Types of TB cases
A comparison between new or previously treated TB cases demonstrated a higher risk of treatment interruption among those who were previously treated (OR 1.77 (95% CI 1.39 to 2.26)). Of note, data were heterogeneous among 13 included studies (I2=92%, p<0.001). There was no significant association in the subgroup analysis for the Southern and Eastern Asia region. However, about 2–4 times higher risk of treatment interruption was noted among previously treated cases in the Western (OR 3.70 (95% CI 2.34 to 5.85)) and Central Asia regions (OR 2.14 (95% CI 1.70 to 2.71)) without significant heterogeneity (I2=35%) (table 2, online supplemental figure S6).
Adverse drug reactions
Those who experienced ADRs secondary to TB medications were more likely to discontinue treatment (OR 2.01 (95% CI 1.20 to 3.34)). Heterogeneous data were noted across nine studies (I2=81%, p<0.001) (table 2, online supplemental figure S7).
Others
Other factors such as age, marital status, educational status, location of residence, diabetes, site of TB infection and sputum smear were unable to predict TB treatment interruption as shown by the overall pooled or region-based estimates (table 2, online supplemental figures S8–S14).
Sensitivity analysis
Seven predictors from the pooled estimates remained significant in sensitivity analyses that omitted studies with a wide range of treatment interruption duration but rather studies that specifically focused on ≥2 months treatment interruption were included. Of note, there were no changes in pooled estimates for HIV status and the subgroups of Western and Central regions as the same studies were accounted for in the initial pooled estimation and sensitivity analysis. The results for South East Asia were not estimated as all studies were excluded from the sensitivity analysis. (table 2).
Publication bias
Publication bias was visually inspected using funnel plots for significant predictors such as gender (figure 4), alcohol intake, smoking and previously treated TB cases (online supplemental figures S15–S17) that included more than 10 studies in the meta-analysis. All the data sets showed symmetrical distribution with the studies spanning on both sides of the dotted vertical line implying minimal publication bias.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot based on gender dataset.
Discussion
The fundamental goal of TB management is to ensure treatment success to cure the illness and curb disease transmission. Nonetheless, interrupted TB treatment remains the challenge over decades that prevent successful treatment outcome. In the year 2020, India topped the global TB incidence (26%), followed by China (8.6%) and Indonesia (8.5%),1 which corresponded to our review in which these countries contributed more than half (54%) of the included studies. This could plausibly explain the extensive studies being carried out in countries with a long-standing high TB burden to explore the contextual underlying treatment interruption issues for TB mitigation.
A wide range of duration has been used to define TB treatment interruption either by medication administration or clinic follow-up. In general, an event where a dose of medication is missed by more than 10% is considered treatment interruption or non-adherence.67 However, based on the TB treatment outcome assessment, ‘lost to follow-up’ was defined as interrupting treatment for at least 2 consecutive months.8 As such, the definitions varied across studies ranging from at least 1 day to 2 months in this review. The percentage of treatment interruption represented by the ‘lost to follow-up’ category among new and relapse TB cases in 2013 was around 5% in Asian countries based on the WHO global report.68 Nonetheless, a much higher pooled prevalence (17%) was noted in this review, which could be due to approximately half (44%) of the studies that considered minimum treatment interruption of fewer than 2 months, thus giving a higher chance of fulfilling the treatment interruption criteria. Specifically, looking at the interruption of ≥2 months as per WHO ‘lost to follow-up’ criteria, this review generated pooled prevalence of 10%, which was relatively higher than the 5% in the WHO global report, but much lower than the 28% that considered the minimum interruption of <2 months in this review. This was an alarming condition as early treatment interruption could lead to the subsequent loss of follow-up or default as highlighted by Jakubowiak et al.10 A more lenient higher default threshold by the WHO could create a false sense of complacency, letting the guard down among treatment providers to tackle interruption in the early treatment phase.
Gender-related disparities have been a known limiting factor for TB care and control. The differences in barriers experienced by women and men affect the responses to treatment that hinder early detection, diagnosis, treatment initiation and completion.69 The TB treatment success was noted as 20% higher among women in a meta-analysis that included studies worldwide.70 In contrast, gender, however, did not affect TB treatment outcomes in the African region.71 In this study, treatment interruption was more prevalent among men in all Asia regions except South East Asia. One reason for the higher treatment interruptions among men is that, in most cultures, men are breadwinners, and their busy lifestyle could have led to less time for treatment follow-up, despite having better access to TB treatment compared with women.72 The fear of losing jobs and incomes among those that are employed could be the main reason for defaulting long-term follow-up,28 34 which could also suggest employment as a significant predictor of TB treatment interruption.
Unhealthy lifestyles such as alcohol intake and smoking were shown to have an increased risk of treatment interruption in our meta-analysis. It was reported that non-alcoholics and non-smokers had 1.5 to 2 times higher probability of treatment success.70 This implied the detrimental effects of alcohol consumption and smoking on the overall TB treatment. The possible explanation was related to nausea and vomiting with excessive alcohol consumption, coupled with poor appetites and nutritional status among alcoholics, which resulted in patients stopping their medication leading to unfavourable outcomes.34 While smoking was shown to be the key contributor to defaulting treatment, it remains uncertain as to why the risk was higher among smokers than non-smokers. The engagement in unhealthy lifestyles was postulated as an excuse to rationalise other unhealthy practices which were shown by lower medication adherence, disease screening and reactive towards healthcare utilisation with more emergency versus primary care visits.73
TB-HIV coinfection has always been a concern as the double whammy increased mortality.74 In our review, patients with TB-HIV coinfection were shown to have 1.5 times greater risk of treatment interruption as compared with HIV-negative status. A similar risk of unsuccessful treatment outcome was also noted among TB-HIV coinfected patients in Africa,71 while Chaves Torres et al reported HIV-negative patients were two times more likely to be successfully treated.70 The management of TB-HIV coinfection posed a great challenge due to the complexity of the illness and medications that increased the likelihood of treatment-related problems.
Another great challenge in TB management was the occurrence of ADRs that led to treatment interruption.75 This was proven in our study, which revealed an increased probability of treatment interruption among those who experienced ADRs during the treatment period, which was concordant with a review in Ethiopia.76 In a global scenario, a wide range (8%–85%) of ADRs was reported among those who received first-line TB medications.77 Close monitoring with early detection and management of side effects, especially during the intensive treatment phase, is of utmost importance to prevent the progression towards severe adverse reactions, morbidity and mortality.77 78 Apart from ADRs, previously treated cases were also shown to be a predictive factor of treatment interruption as compared with newly diagnosed cases in the Asia region. This was in concordance with another study from Africa that showed significant 1.5 times higher risk of unsuccessful treatment outcomes among the previously treated cases.71 As such, counselling on TB treatment and follow-up shall be strengthened in TB management to prevent treatment interruption and ensure eventual treatment success.
Limitations
Given the variabilities in study designs, methodology and duration of treatment interruption, considerable high heterogeneity as denoted by pooled analyses of prevalence and predictors was observed. As such, the magnitude and degree of the significant predictors (except employment and HIV status) were not expressed numerically, but rather the direction of the predictors’ influences was reported. The random-effect model was, thus, selected in the meta-analysis that considered the variation of effect sizes across the studies.
Besides, the unstandardised categorisation of risk factors across the studies, for example, age, education level and income status, and the absence of the number of events in both risk exposure and non-exposure groups rendered studies to be excluded from the meta-analyses.
Strengths
Despite the limitations, this is the first systematic review and meta-analysis on the Asian population focusing solely on treatment interruption rather than unsuccessful treatment outcomes that incorporated default or loss to follow-up as one of the combined endpoints. Therefore, the identified predictive factors via pooled estimation from various studies in the Asia region could serve as a reliable reference to identify potential high-risk groups for treatment interruption. This information is particularly useful for regional interventional strategy planning for TB control. In addition, the findings which were in concordance with other regions could also assist in universal planning to tackle problems concerning TB treatment interruption that could potentially lead to unsuccessful treatment outcomes.
Conclusion
TB treatment interruption remains a potentially alarming problem. This was of particular concern in the Southern, Eastern and South East Asia regions, which demonstrated a high prevalence of TB treatment interruption. Significant predictive factors with higher risks of treatment interruption such as male gender, employment, alcohol intake, smoking, HIV-positive, ADRs, and previously treated cases were identified. Healthcare providers should focus their effort to improve TB treatment adherence in patients with these characteristics from the beginning of therapy, which is crucial to ensure treatment success.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We gratefully thank the Universiti Kebangsaan Malaysia librarian for their assistance in article acquisition and technical support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Senjuti Saha
Contributors ALO and MM-B conceptualised the study. ALO screened, extracted the data and assessed the methodological quality of relevant studies. MMB verified the data and conducted an independent methodological quality assessment. Disagreements were resolved by discussion with FI. The final data analysis and write-up were conducted by ALO and checked by MM-B, FI and ICKW. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication. MM-B is responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.