Article Text

Abstract
Introduction The COVID-19 vaccine donation process allegedly prioritised national interests over humanitarian needs. We thus examined how donors allocated vaccines by recipient country needs versus donor national interests and how such decisions varied across donation channels (bilateral vs COVAX with country earmarking) or exposure to foreign aid norms (membership status in the Development Assistance Committee—DAC).
Methods We used the two-part regression model to examine how the probability of becoming a recipient country and the volume of vaccines received were associated with recipient countries’ needs (disease burden and GDP per capita), donor countries’ interests (bilateral trade volume and voting distance in the United Nations General Assembly) and recipient countries’ population size. The analysis further interacted the determinants with channel and DAC status.
Results Donors preferentially selected countries with higher disease burden, lower GDP per capita, closer trade relations, more different voting preferences, and smaller populations. Compared with bilateral arrangements, COVAX encouraged more needs-based considerations (lower GDP per capita), less interest-based calculus (more distant economic relations and voting preferences) and larger population size. Compared with the DAC counterparts, the non-DAC donors focused more on politically and economically aligned countries but also on less economically developed countries. As for the volume of vaccines donated, countries received more vaccines if they had tighter trade relations with donors, more different voting patterns than donors, and larger populations. COVAX was associated with raising the volumes of vaccines to politically distant countries, and non-DAC donors donated more to countries with stronger trade relations and political alignment.
Conclusion Donors consider both recipient needs and national interests when allocating COVID-19 vaccines. COVAX and DAC partially mitigated donors’ focus on domestic interests. Future global health aid can similarly draw on multilateral and normative arrangements.
- COVID-19
- Health policy
- Health systems
- Vaccines
Data availability statement
Most data are available in a public, open access repository. Part of the data are obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Even though COVID-19 vaccines can save lives, there has been no quantitative examination of what drives donor countries to pick a certain country and, once decided, how many vaccines to give.
No previous study has examined whether COVAX mitigated donor interests despite significant hope that the COVAX initiative can improve global vaccine equity.
Literature on COVID-19 vaccine donation has also not quantitatively contrasted the donation determinants of the member states in the Development Assistance Committee (DAC) versus those that are not.
WHAT THIS STUDY ADDS
This is the first study to show quantitatively that (1) the decision to allocate COVID-19 vaccines is associated with recipient countries’ needs and donor interests; (2) COVAX increased donors’ focus on donating to economically and politically distant states; (3) DAC and non-DAC members considered similar factors, but DAC members focused less on domestic interests and (4) the allocation considerations differed across donors within and across DAC and non-DAC membership.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Establishing and supporting international aid allocation agencies such as COVAX can help insulate humanitarian aid allocation processes from national interests.
Implementing and encouraging international consensus on norms of donations that focus on recipient needs, as in the case of DAC, can also be helpful.
Introduction
Over the last several decades, global health aid has garnered increasing attention, as the amount of global health aid has increased dramatically. During this process, the role, content and structure of global health has increasingly transformed from solidarity in maximising human health and welfare to pragmatic foreign policies that enhance donor countries’ interests.1 The global health aid landscape thus often embeds a set of dual goals: on the one hand, donors value equity, in keeping with the ‘health for all’ principle; on the other hand, the allocation of global health aid may prioritise state objectives.2 Without genuine commitment to health and solidarity, preventable morbidity and mortality could escalate unnecessarily. It is thus crucial to objectively evaluate to what extent global health actors are dedicated to health improvement by piercing through the global health actors’ veil of rhetoric.
We leverage the context of COVID-19 vaccine donation to assess how donors balance their domestic interests against humanitarian considerations. Not only have critics expressed that donor countries’ interests have again tainted this humanitarian process,3 studying how the donors’ allocate their donations in this context offers two additional advances. First, because COVID-19 vaccines can prevent death more readily than monetary aid, the humanitarian concerns may outweigh the donor countries’ self-interests, highlighting the upper bound for the emphasis on humanitarian concerns. Second, because the initial set of COVID-19 vaccines was life-saving and could generate significant benefits for recipient countries’ government during a particularly dire situation, donor countries could buy much more goodwill via COVID-19 vaccines than traditional monetary aid. This consideration may thus highlight the upper bound of national interests as well. COVID vaccine donations thus highlight the upper bounds of both humanitarian and nationalistic determinants. Determinants that were not significantly associated with COVID-19 vaccine donation decisions are therefore unlikely to be significant determinants in other foreign aid situations as well, and the global health researchers can productively focus their attention elsewhere when examining determinants of foreign aid.
It is not enough to simply examine the extent to which such dual goals persist in global health. Identifying how specific arrangements can increase the weight of the humanitarian considerations relative to nationalistic tendencies can help the global health community learn how to set up global health aid in the future such that humanitarian considerations can outweigh nationalistic tendencies and move towards health for all.
The first possible arrangement is to establish a multilateral donation allocation process. Traditionally, donor and recipient countries negotiate bilateral agreements with each other, but these arrangements encourage donors to opportunistically target countries that serve domestic interests. During COVID-19, the leading global health organisations developed an alternative channel of vaccine donation. The COVID-19 Vaccines Global Access (hereafter ‘COVAX’) ensured that COVID-19 vaccines would be ‘distributed equitably, effectively and transparently’. However, COVAX nevertheless allowed donors to earmark vaccines for specific recipient countries (hereafter ‘COVAX specified’). In fact, such donations constituted the majority of COVAX-distributed vaccines. By October 2021, up to 75% of COVAX vaccines were earmarked.3 Studying the COVAX specified vaccines is more analytically advantageous relative to the non-earmarked COVAX vaccines. The non-earmarked COVAX vaccines are pooled together as a single pool of vaccines, so there is less readily identifiable origin and destination country. In contrast, the COVAX specified vaccines carry both origin and destination countries, so they can be readily compared against the traditional bilaterally donated vaccines.
The second setup stems from how the global community has historically mitigated national interests. The Development Assistance Committee (DAC) in the Organisation for Economic Co-operation and Development includes 30 of the world’s biggest donors. Even though some DAC donors have used global health aid to achieve diplomatic goals,1 the DAC targets their official development assistance to countries with lower income per capita. In contrast, donors not part of this group (non-DAC donors) do not adhere to a set of unifying guidelines that focus on recipient country needs. Such non-DAC donors are making up a formidable proportion of the global foreign aid, growing in absolute amount of donation for the last 50 years such that by 2016, they contributed to about 13.1% of the global financial aid.4 5 However, the lack of explicit norms have led critics to label these countries as being more focused on national interests when it comes to foreign aid6 even though the lack of guidelines does not necessarily confirm such tendencies.
Despite all the rhetorical differences, empirical support to distinguish the motivation between the two groups of donors is lacking. Only two studies have rigorously tested whether the determinants of bilateral development assistance allocation differed between the DAC and non-DAC donors, and they both suffer from methodological flaws. Dreher et al. found that both types of donors similarly allocated aid based on national interest and recipient countries’ merit,7 but due to data limitations, it did not include China and India, two of the largest non-DAC donors. Petrikova suggested that many non-DAC donors de-emphasised recipient countries’ merit relative to their DAC counterparts, but the study did not directly contrast between the two groups the influence of each determinant on donation behaviours.8
Overall then, this study addresses the primary research question: to what extent do the dual goals motivate the COVID-19 vaccine donations? To understand if and to what extent special multilateral global health aid arrangements can encourage humanitarian focus, the study explores two secondary questions. First, to what extent did COVAX mitigate donor interests? Second, how did the considerations differ between the DAC and non-DAC members?
Methods
Dataset
We used the UNICEF COVID-19 vaccine market dashboard9 and Airfinity10 to capture the recipient, donor, volume, and channel of vaccine donation. However, they did not include data on the non-DAC donors’ COVAX specified donations. We manually entered this data by examining the official government websites of the most significant non-DAC donors—China, India and Saudi Arabia. This approach only added India’s COVAX specified doses. Even though China joined COVAX on 8 October 2020 and delivered its first batches through COVAX to Pakistan and Bangladesh on 12 August 2021, data were unavailable. COVAX-related data for Saudi Arabia were similarly unavailable.
We restricted the analysis to the period before 31 December 2021, after which the much less lethal Omicron variant circulated widely. Studying this period thus maximises the weight of the humanitarian determinants. Restricting the analysis to this time period can also highlight the tension between the nationalistic and humanitarian considerations, as donors were also struggling to vaccinate their own citizens in this period.
Within the complete dataset, the analyses limited the donor countries to the countries whose volume of vaccine donation amounted to more than 1% of the total doses donated globally via either bilateral or COVAX specified channels by 31 December 2021. The cut-off considered the quantity of vaccine delivered rather than the declared supply since some donors may not follow through with the promises. Data from the Duke vaccine database showed large gaps between pledging and shipping, as high as 59% unshipped for some donors as of 15 September 2022.11 In total, the dataset captured a total of 12 DAC countries (USA, Japan, Poland, Germany, UK, Netherlands, Australia, South Korea, France, Italy, Spain, Canada) and 3 non-DAC countries (China, India, Saudi Arabia).
For recipient countries, we considered countries that could have received vaccine donations. We thus included the countries that received any donations from donors or belonged to the 135 low-income and middle-income countries group defined by the World Bank in 2020. Four territories (ie, Palestine, Taiwan, Kosovo and Serbia) were not included due to lack of data.
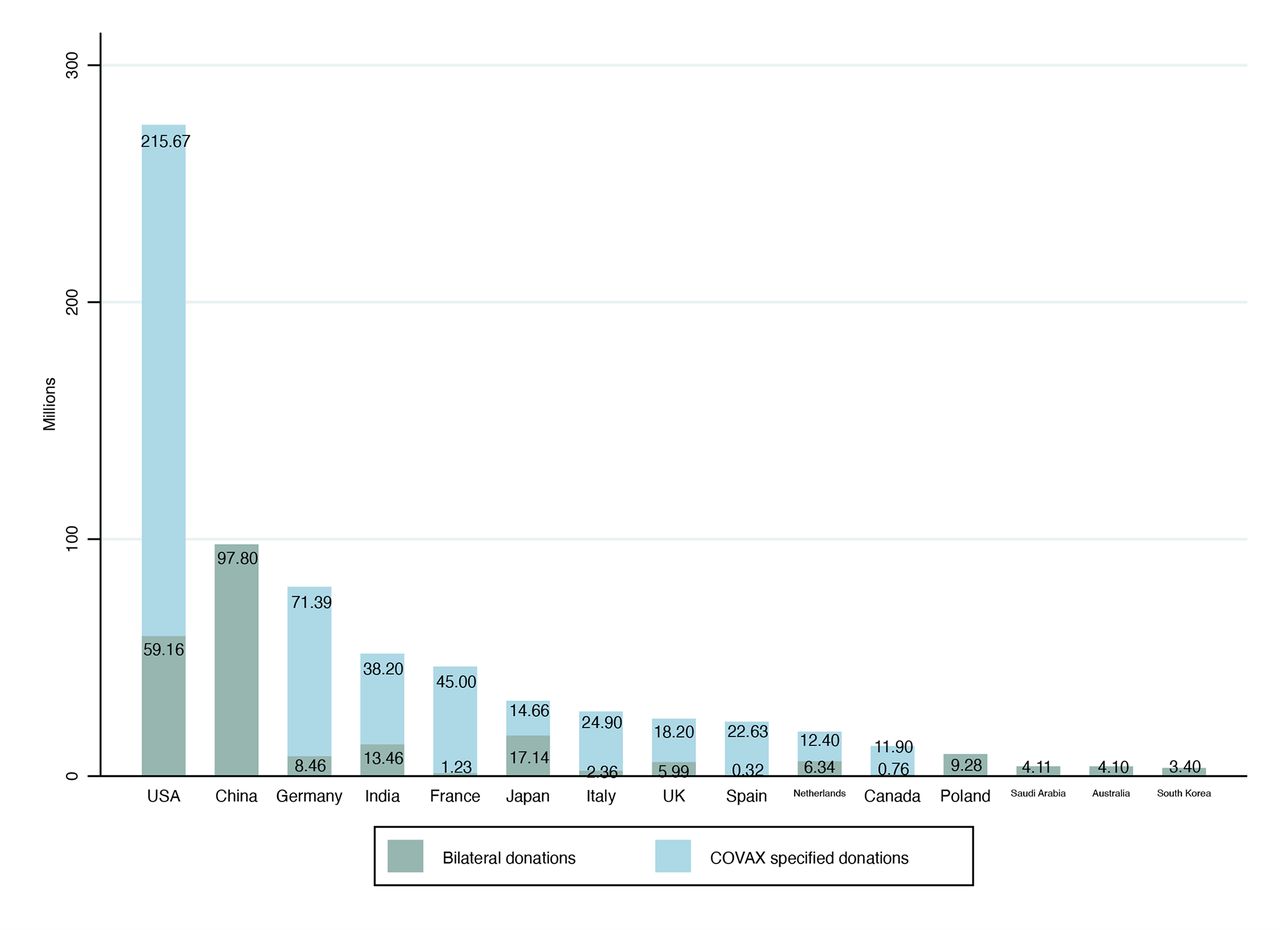
Figure 1 shows the distribution of the vaccine donation by country as of 31 December 2021. COVAX specified donations constituted a much larger proportion of the total donation than bilateral donations (474.9 million doses vs 233.9 million doses, or 67.0% vs 33.0%, respectively). The bilateral donations were roughly evenly split between the DAC and non-DAC donors (50.7% vs 49.3%, respectively). Of the countries that donated via bilateral channels, China donated the most (97.8 million doses), followed by the USA (59.2 million doses), and this rapidly dropped off by the third-highest country Japan (17.1 million doses) and fourth India (13.5 million doses). As for the COVAX-specified donations, 92.0% of them came from DAC donors.

{kind=link}
Vaccine donation of major countries as of 31 December 2021.
The recipient country characteristics drew from the WHO’s COVID-19 dashboard, which covers each country’s disease burden (ie, cumulative number of COVID-19 cases and deaths until 31 December 2021).12 The World Bank provided additional data on each country’s population size and Gross Domestic Product (GDP) per capita in 2019.13
The dataset on donor countries’ interests was based on the United Nations (UN) Comtrade data,14 which characterises the average volume of export from donor to recipient countries between 2017 and 2019. We also leveraged a dataset from Bailey et al15 that captured the alignment of voting preferences in UN General Assembly between 2017 and 2019. The voting alignment variable quantified the absolute distance between a pair of states’ foreign policy preferences, where smaller distances indicated higher voting alignment.
Outcome variables
The study measured two outcome variables, similar with the literature of development assistance.7 The first stage—gatekeeping—determines whether a recipient country will receive any vaccines from a specific donor country, measured via a binary variable (0 for no and 1 for yes). The second level-setting stage is measured by the number of vaccine doses that a recipient country received from a specific donor country.
Explanatory variables
Drawing on previous studies,7 16 17 we considered two categories of explanatory variables: recipient need and donor interest.
For recipient need, we included the cumulative COVID-19 cases and deaths until 31 December 2021. We also included the recipient countries’ GDP per capita. We expected that higher case or mortality level and lower GDP per capita to reflect strong needs of vaccines, as such countries may have higher disease burden or need more resources to quell COVID-19 outbreaks.
Donor interest was measured in terms of economic interest (bilateral trade volume) and political interest (voting alignment in the UN General Assembly). Higher bilateral trade volume indicates closer trade relations, and donations to economic partners may reinforce further trade relationships. Voting alignment connotes stronger political alignment, and donors may reward their allies with vaccines.18
We also considered the recipient countries’ population size though this variable carries a complex interpretation. It may reflect recipient country needs, because larger countries may require more vaccines to reach herd immunity. However, the variable may also reflect national interests. Donating to countries with smaller population size can buy the recipient countries’ goodwill more efficiently,19 as a smaller number of doses may foster proportionally greater political influence.20 Lastly, the variable may be contaminated by operational considerations. Smaller countries may be less well resourced, so the same amount of aid can generate more transformative effects,21 allowing the recipient country to reach herd immunity faster. Smaller countries may have less complicated bureaucracy, so the recipient can be more accountable.21 However, smaller countries may also have lower economies of scale19 and proportionally higher administrative costs, which may make them less attractive candidates. These varying considerations thus render this variable somewhat challenging to interpret as an explanatory variable.
We excluded the category of recipient merit, which reflects the ability for recipient countries to implement foreign aid. Conventionally, it includes variables characterising government effectiveness and, in this case, it can include variables such as vaccine distribution capacity. We excluded this category because the consideration of the recipient merit is not directly relevant to examining the contrast between humanitarian or nationalistic consideration.
We logarithmically transformed the explanatory variables on the number of cases and deaths, GDP per capita, trade volume and population size, as their distributions were skewed to the right. We used a logarithmic base of two to facilitate interpretation.
Estimation method
The analysis first descriptively differentiated the recipient countries’ needs and donor interests for vaccine allocation across the entire sample, as well as different channels and DAC statuses. The differences were tested using t test.
The analysis then used a two-part regression model to separately assesses (A) the probability of any vaccine donations (ie, gatekeeping) and (B) the number of vaccine donations that a particular recipient would receive from specific donors (ie, level setting). The separate modelling mirrors the two-stage donation decisions. This modelling technique is also often superior to the conventional estimation methods in its handling of the zero-inflated dataset.22 All regression models clustered the regressions at the level of donor countries, since each donor country likely had a specific set of considerations that influence its allocative decisions.
We estimated the gatekeeping outcome using equation (1):
 (1)
(1)
where the outcome variable Donation is a dummy variable indicating whether the recipient country i received any vaccine donations (one if yes, 0 otherwise). The log odds value of this outcome is estimated to be a function of a vector of explanatory variables X, which includes the level of needs (ie, number of cases and GDP per capita), donor interests (ie, trade volume and voting distance) and additional characteristics (population size) for recipient country i. We specified the disease burden needs as the total number of cases, because donor countries have explicitly targeted controlling the case load to contain the spread, conceptualised as ‘externality’ in the literature.23 In the case of COVID-19, lowering the evolution speed is also an important concern.24
We estimated the level-setting outcome using equation (2):
 (2)
(2)
where the logged number of doses of vaccine delivered to country i is estimated via the same list of variables in equation (1).
To examine whether the channel and DAC status influenced either of the outcomes, we repeated the equations (1) and (2) on the corresponding subsets of the data.
We then examined whether the channel differed in how they weighed the determinants by interacting COVAX with the vector of X variables, as shown in equations (3) and (4):
 (3)
(3)
 (4)
(4)
where the additional term non_DAC controls for whether the donations originated from non-DAC donors (1 if the donation originated from non-DAC donors and 0 otherwise). The key coefficients are the  coefficients, which would be significant if determinants considered in COVAX significantly diverge from bilateral donations.
coefficients, which would be significant if determinants considered in COVAX significantly diverge from bilateral donations.
To examine whether the vaccine origin from non-DAC donors influenced the donation allocations, we nuanced equations (3) and (4) by interacting the vector of explanatory variables X with the non_DAC variable, forming equations (5) and (6).
 (5)
(5)
 (6)
(6)
The key coefficients of interest are the  coefficients, which would be significant if the non-DAC donors’ considerations of determinants are significantly different from the DAC donors.
coefficients, which would be significant if the non-DAC donors’ considerations of determinants are significantly different from the DAC donors.
Robustness checks
We did two checks to ensure robustness. First, we specified recipient need using deaths instead of cases, as death counts may seem more pressing than case load. Second, we used the effective dose of vaccination to measure the quantity of donations. For example, the Janssen COVID-19 vaccine requires only one dose to be fully vaccinated, so we counted one dose from Janssen vaccine as one effective dose. For other vaccine types which require two doses, each dose was counted as half of an effective dose.
Subgroup analysis
Subgroup analysis focused on three countries—the USA, China and India, which all have mass manufacture capacities. The USA led the DAC donors’ donation efforts by far while China and India led the non-DAC donors. The analysis focused on understanding the determinants of these countries’ donation behaviours by substituting the non_DAC term in equations (5) and (6) with specific countries, such that the term would take on a value of 1 if the donation came from the specific country of interest and 0 otherwise.
Bias
Since there was little previous quantitative analysis on the determinants of vaccine donation, we based the selection of covariates on previous literature that examined the determinants of foreign aid.7 16 17 Residual confounding may persist to the extent that vaccine donation behaviours deviate from foreign aid behaviours. Also, GDP per capita—a recipient needs variable—is likely to be positively correlated with implementation capacity, which characterises the merit of a recipient country. Neglecting implementation capacity variables may thus overestimate the magnitude of the association between GDP per capita and outcome variables. However, excluding merit-based variables should not bias the estimate of the donor interest variables, as they should be independent of each other. Dropping the four territories might also bias our results though the few numbers of dropped observations should generate only minimal bias. Lastly, because the data could only consider the COVAX specified donations of India, the estimates around the determinants of COVAX specified donation may be biased.
Patient and public involvement
The design, conduct, reporting or dissemination of the research did not involve patients or the public.
Results
Descriptive results
The descriptive statistics in table 1 shows that in terms of the determinants of donation, the bilateral donations targeted countries with higher disease burdens, but the COVAX specified donations were preferentially allocated to poorer and more populous countries. Second, COVAX specified donations also mitigated donor interests, where doses were more often allocated to countries with lower volume of bilateral trade or more dissimilar political preferences. Lastly, the non-DAC donors allocated vaccines to countries with lower disease burdens, smaller population and more similar political preferences.
Descriptive characteristics of recipient countries’ characteristics across donation channels and types
Overall determinants of vaccine allocation
Table 2 shows the association of the determinants with the outcomes.
Regression analysis of determinants of COVID-19 vaccine donation across different channels and donor types
Using the pooled sample, as the recipient countries’ case load and trade volume with the donor country doubled, their odds of passing the gatekeeping increased by 1.05 and 1.39 times, respectively. Conversely, a doubling of the GDP per capita and population size lowered their odds by 0.68 and 0.80 times, respectively. More distant political preferences were also significantly associated with higher odds of passing gatekeeping, such that one unit increase in voting difference was associated with 2.11 times higher odds.
As for the level-setting stage, the only two determinants that retained the same direction of association were the bilateral trade volume and voting distance. A doubling of the trade volume was associated with 15% increase in the vaccine received, and one unit increase in voting distance was associated 37% with more vaccines received. The direction of association with population size flipped, such that a doubling of population was associated with 19% increase in the vaccine received.
Determinants of vaccine allocation by channels
The directions of association for bilateral donation remained the same as the pooled sample at the gatekeeping stage. The COVAX specified allocations, however, diverged, showing only significant associations with countries that had worse economic development, stronger trade relationships and further voting distance. Doubling the recipient countries’ GDP per capita and trade volume, and one unit increase in voting differences were associated with 0.59, 1.25 and 1.59 times higher odds of passing the gatekeeping, respectively. The COVAX specified donations were not significantly associated with the case load and population size in the gatekeeping stage.
Comparing the two channels showed that COVAX encouraged selection of countries on more humanitarian grounds. Recipients’ odds of passing gatekeeping decreased by 0.73 and 0.81 times when the recipient countries doubled their GDP per capita and trade volume with the donor countries, respectively. A doubling of the population size was associated with 1.60 times higher odds. Conversely, a one-unit increase in the recipient countries’ voting distance relative to donors was associated with 1.93 times higher odds of being selected.
The only conflicting finding to this trend is that COVAX was preferentially associated with countries with lower case load. A doubling of case load was associated with only 0.87 times the odds of passing gatekeeping.
At the level-setting stage, the patterns of significant determinants in bilateral and COVAX specified donations were generally similar to that observed for the pooled sample analysis. The main difference was that COVAX specified vaccines were significantly more associated with politically dissimilar countries, such that one unit increase in voting differences increased the volume of vaccines received by 23%.
Determinants of vaccine allocation by donor types
At the gatekeeping stage, the DAC and non-DAC donors demonstrated similar associations to countries with smaller populations, lower GDP per capita, and tighter trade relations. However, the non-DAC donors were more likely than their DAC counterparts to donate to less economically developed countries. A doubling of the recipient countries’ GDP per capita was associated with a drop of the odds of passing gatekeeping in non-DAC donors to 0.81 times. The non-DAC donors, however, also focused more on national interests. Relative to the DAC donors, the odds of passing the non-DAC donors’ gatekeeping increased by 0.19 times with a doubling of the trade volume with the donor country and decreased by 0.29 times with a one-unit increase in voting difference relative to the donor country. The non-DAC donors also favoured smaller countries more—a doubling of the population size decreased the odds of passing gatekeeping to 0.72 times.
At the level-setting stage, both DAC and non-DAC donors generally used similar criteria as gatekeeping. In both cases, however, the population size became positively associated with more COVID-19 vaccine delivery. A doubling of population size increased the number of vaccines received from DAC and non-DAC donors by 27% and 19%, respectively.
When comparing the two directly, the non-DAC donors were significantly more likely to donate more vaccines to countries with higher bilateral trade volume and closer political preferences. The number of vaccines increased by 11% with a doubling of the trade volume and decreased by 31% with a one-unit increase in political preference.
Robustness checks and subgroup analysis
The findings were generally supported in robustness checks (online supplemental appendix tables A1 and A2). However, disease burden specified in terms of deaths was not a significant determinant for gatekeeping, and the focus on lower economically developed countries was also less consistently significant.
Supplemental material
The subgroup analysis suggested different countries showed divergent priorities (online supplemental appendix table A3), but the pattern of recipient needs versus donor interests remained similar.
Discussion
Our study is among the first to quantitatively demonstrate that despite the humanitarian call to equitably distribute COVID-19 vaccines for life-saving purposes, donor countries nevertheless balance humanitarian contribution against foreign policy interests. This is also the first study to quantitatively demonstrate that COVAX and DAC membership mitigated the donors’ tendencies to prioritise nationalistic interests.
Determinants of donations
The study confirmed that worse caseload and lower economic development are generally associated with higher probability of passing gatekeeping and, in some cases, higher volume of vaccines donated.
Donors’ economic interests matter as well. Consistent with the development assistance literature,25 26 higher bilateral trade volume is associated with both greater probability of passing gatekeeping and larger volumes of donations. The existing theory suggests that donors may wish to reinforce their extant commercial ties with the recipient countries.27 Foregoing such donation may undermine future economic relationships. Another possibility is that the extant institutions used for trading may improve the efficiency of the donation process. Countries that frequently trade with each other may take on similar organisational structures and norms,28 which might lessen the bureaucratic burden for donation processing.
Political differences also factored into donor considerations. Contrary to the conventional wisdom that countries preferentially reward their allies,18 the donors were more likely to pick countries which voted differently from them in the recent UN voting history and donate more vaccines to such countries. This pattern was consistent across donation channels and donor types.
In terms of how donors consider the importance of population size, we found a paradoxical phenomenon. When recipient countries have larger populations, they have lower probability of passing the gatekeeping stage, but if they do pass it, they may receive higher levels of volumes of vaccines. Previous research has demonstrated such small country biases in bilateral and multilateral donations,25 29 as well as in the health aid,21 but there remain some conflicting interpretations about the margins at which such small country biases ought to manifest.19 This is as far as we know the first empirical documentation of such sharply demarcated dichotomous finding within a single episode of donor aid. The findings suggest distinctive considerations at the two stages. Perhaps when donors determine the target of donation, it considers the marginal gain for political influence and vaccine impact, but at the level-setting stage, it focuses on the economies of scale and maximising the humanitarian aid.
COVAX specified versus bilateral donations
Even though we studied the COVAX vaccine donation using earmarked vaccines, the findings nevertheless suggested that COVAX mitigated some nationalistic interests. First, at the gatekeeping stage, COVAX specified donations were significantly less associated with economically developed countries. Second, COVAX moved donors to focus more on countries that are less developed. Third, COVAX eliminated the population bias in the gatekeeping stage. Last, COVAX further strengthened donations towards countries whose voting behaviours were different with donors. The only negative finding of COVAX specified donation relative to the bilateral donation channels is that COVAX was less likely to be associated with disease burden than bilateral donations. This might have stemmed from COVAX’s prioritisation of equitable vaccine distribution across countries with less emphasis on disease burden.30
The findings thus suggest that even in a suboptimal situation where COVAX allowed earmarking donations, it could be helpful. In the scenario that donor countries are not able to fully give up their opportunities to use foreign aid for domestic interests, striking the middle ground of using multilateral agencies to administer foreign aid may prove a feasible and effective compromise.
Comparison across groups of donors
The study showed that generally, non-DAC and DAC donors were associated with a similar panel of determinants. The main difference was that the non-DAC donors were more likely to choose and donate more vaccines to countries that demonstrated tighter trade relations and similar voting patterns. This suggests that the DAC donors may be focusing less on their own domestic needs though these factors still impact their decisions. It is noteworthy that at the gatekeeping stage, non-DAC donors targeted poorer countries more than the DAC counterparts, which indicates that there may be alternative reasons beyond DAC norms that can encourage focus on lower economically developed countries. Also, this pattern may not apply across all member states within either of the groups. The subgroup analysis suggested that countries within both the DAC and non-DAC groups may demonstrate significant heterogeneity as indicated in the literature of development assistance.7 31
Practically, the differences suggest that the norms established within the DAC may be helpful in guiding its membership states towards less nationalistic considerations. Ideally, the principles that guide DAC countries’ donation can also generate interest from other major donors. Theoretically, the heterogeneity also offers a unique opportunity for subsequent in-depth comparative case studies to understand why certain countries preferentially value certain determinants.
Stages of donation
This study showed that the determinants were not homogeneously significant across the different stages of vaccine allocation. Future development can develop a more nuanced model of the allocation process so that future research, advocacy, and policy recommendations can be more targeted. Such a model could capture at least the following stages: shortlisting the recipient countries, deciding on the recipient countries, determining the volume of donation, and delivery of the actual vaccines.
Limitations
First, the data only allowed static assessment of the donation behaviours, which may miss the changes in donor countries’ intentions across different stages of the pandemic. Our study nevertheless provided novel evidence on the determinants of the initial vaccine donation, during which time the conflict of recipient needs and self-interests should have been especially prominent. Second, we did not differentiate between the types of vaccines, though we considered the effective doses as a robust check. The efficacy, safety, and cost vary, and more granular data may better distinguish the various donors’ trade-off considerations. Lastly, the study quantitatively examined the association between the determinants and decision outcomes, but this design is unable to illustrate why the countries valued certain determinants as specific stages. Future case studies of the decision-making processes can provide in-depth illustrations about the dynamics of foreign policy considerations.
Conclusion
The donor countries’ decision to donate COVID-19 vaccine was associated with the recipient countries’ needs, as well as their intensity of economic interaction and political alignment with the donor countries. COVAX partially mitigated donors’ self-interests, even when it allowed donors to target specific recipients. The DAC donors showed somewhat milder nationalistic tendencies though the pattern of significant determinants differed within the groups of DAC and non-DAC countries and across different stages of the donation process.
Practically, foreign aid arrangements in the future can draw on multilateral allocation approaches such as COVAX or use normative arrangements like DAC to mitigate nationalistic tendencies for foreign aid. Theoretically, as demonstrated by the conflicting association of population sizes with gatekeeping versus level setting, more detailed understanding of allocation decision processes can help the global health community better identify the mechanisms driving the donation process, target advocacy efforts and improve aid effectiveness.
Data availability statement
Most data are available in a public, open access repository. Part of the data are obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank Professor Nozaki Shinjiro from the WHO Regional Office for the Western Pacific for his valuable insights. His thorough and critical comments for the initial versions of the manuscript were very helpful. We are also grateful to the anonymous reviewers for their insightful comments on the previous versions of the paper, which have helped us sharpen the methodology, interpretation, and contribution of this manuscript significantly.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @YianFang2, @SianTsuei
Contributors SH-TT and MW led the study. YF and TM originally conceptualised the study and collected the data. YF, TM and SH-TT contributed to the study design and methodology. YF conducted the analysis. YF drafted the manuscript with substantial revision and comments from TM, MW and SH-TT. YF and SH-TT jointly serve as the guarantor of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.