Article Text

Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Improvements in access to healthcare are fragile in politically unstable countries, especially in Mali.
The primary factors that continue to limit women’s access to healthcare after user fee abolition are distance to health facilities.
Repeated attacks aggravate insecurity and are further detrimental to maternal healthcare.
WHAT THIS STUDY ADDS
A large number of events, especially in the more remote parts of the Bandiagara district, would not impact the number of assisted deliveries.
Populations move to less exposed areas and to efficient centres to access maternal care.
CsCOM performance is associated with an increase in assisted deliveries.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Non-governmental organisation prevention efforts contribute to an increase in assisted deliveries.
The use of mixed methods with a spatial approach allows to improve knowledge at fine local scales.
Introduction
Healthcare systems are often severely affected by armed conflict.1 2 In sub-Saharan Africa and the Sahel in particular, by disrupting access to care and the availability of human and financial resources, these conflicts contribute to high maternal mortality rates3 and a low rate of deliveries in health facilities.4 Although there are rich literature on the connections between5 conflict and access to healthcare, studies that estimate their impact on the use of maternal healthcare are still rare.6 These studies mainly address the impacts of armed conflict on maternal health, miscarriage or other adverse pregnancy outcomes.7 In Burkina Faso, studies suggest that armed groups have an immediate impact on the organisation of care8 and various indicators of maternal care, including the number of antenatal care visits, assisted deliveries and caesarean sections.9 The frequent and repeated attacks, which are temporally and geographically close, aggravate insecurity and undermine access to maternal care in the affected regions. Thus, they are a barrier to access to care4 when it should be a priority in humanitarian and fragile contexts.10 In addition, the use of health facilities for skilled birth attendance can be irregular within a single Sahelian country and within health districts.11 It is important to conduct analyses at local scales to avoid ecological errors that mask these disparities.
Armed groups generate a sense of insecurity among the general population, and health workers working in local health centres.12 This feeling can have a negative impact on the functioning and performance of the health centre, which in turn will also affect the use of healthcare.13 Thus, in the context of this article, it is also a question of considering the fine scale of the health centres, in order to take into account this feeling of insecurity and performance, the geographical distribution of which is heterogeneous, in order to understand possible differences in the impact of conflicts on the rates of assisted deliveries.
Insecurity in the Sahelian zone is causing population movements. While these displaced persons are sometimes accommodated in camps with health resources, many move to other cities, creating a large influx of people for already limited healthcare capacities. Health facilities often cannot care for patients, their inputs are exhausted, and there is a shortage of medical supplies.14 Since January 2012, Mali has been facing a security crisis initiated by an armed rebellion organised by an alliance of Tuareg independence groups and jihadist groups, mainly located in the north of the country. In 2015, groups of jihadist fighters formed in central Mali, where social and political tensions were already high. Since 2016, a new conflict has emerged in the south and southeast of the Mopti region (districts of Mopti and Bandiagara). This area is now considered the ‘epicentre of violence’ in Mali.15
The main objective of this study is to understand how assisted deliveries are being reorganised in the context of the security crisis in Mali. There are three secondary objectives: (1) to analyse the geographical distribution of assisted deliveries in the health districts of Mopti and Bandiagara; (2) to evaluate whether the performance of health centres is one of the factors explaining differences in the use of assisted deliveries and (3) to assess the impact of conflict on the number of assisted deliveries in health centres.
Method
The study design is explanatory sequential16 (quantitative analyses (QUAN)-QUAL). The objective is to explain the results of phase 1 (QUAN), which is a statistical and geographical analysis of deliveries in primary health centres (CsCOMs) and attacks by armed groups, using the results of phase 2 (QUAL). Phase 2 analyses in-depth interviews with managers of these CsCOMs and two agents of international institutions involved in the study area.
Study area
The study area is central Mali in the Mopti region and the two health districts of Mopti and Bandiagara (figure 1). The Mopti health district is composed of health areas (a collection of villages). It has 2 hospitals (1 public and 1 private), 26 CsCOMs and 15 communes that do not correspond to the health areas. The Bandiagara district has 21 communes, 1 hospital and 31 CsCOM. The total population of the Mopti district is 492 174, and 424 665 for Bandiagara.17 Bandiagara is to the east of Mopti and is bordered in its western part by the Bandiagara cliff. The district is rural and not served by major roads (figure 1). The Mopti health district is crossed by National Road 6, which links Bamako to Gao. The localities located west of this road are in the Niger Delta and are partially cut-off for long periods of the year.
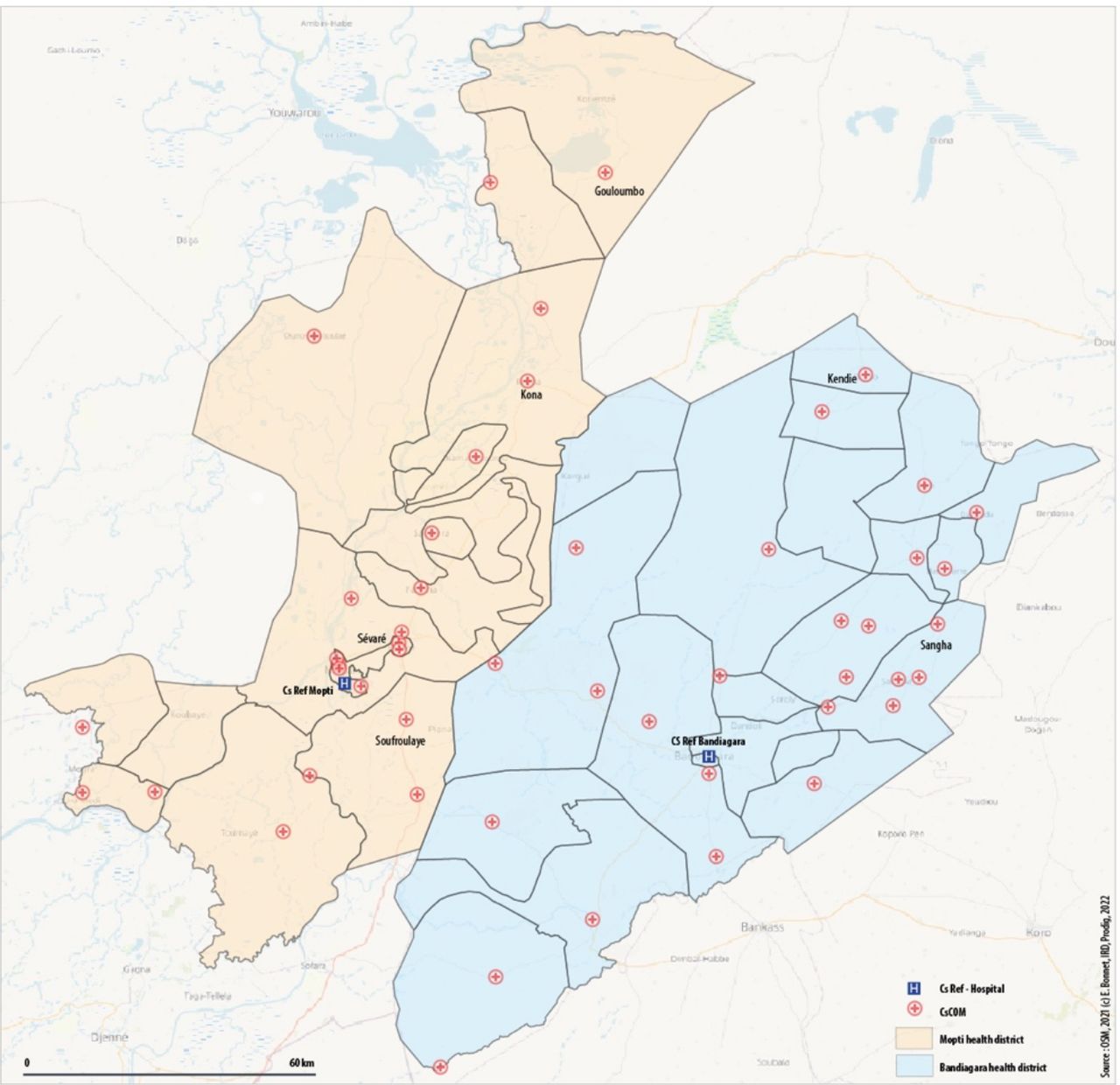
Study area: healthcare supply in the health districts of Mopti and Bandiagara.
Quantitative approaches
Data collection
We used monthly data from the Data Health Information System on the number of assisted deliveries and prenatal consultation by CsCOM from 2017 to 2019. The DIHS2 data in this region were well captured because of the presence of various programmes, including the capitalisation of the programme to support health and social development in the Mopti region.18 The year 2017 corresponds to the beginning of a phase of intensification of the security crisis in the Mopti region.19 For data on attacks and incidents, we used the political violence database produced by the non-governmental organisation (NGO), The Armed Conflict Location & Event Data Project (ACLED).20 These data contain the dates, geographical locations and actors involved in the events. The database lists 819 events between 2016 and 2019.
Geographical analyses of assisted deliveries
We conducted several QUAN. The first is a descriptive and spatial analysis of the dynamics of assisted deliveries by commune since the geographical breakdown of the health areas is inaccurate in available geographical databases. It consists of an aggregation of the number of deliveries per commune and its evolution over the study period.
To examine spatial and temporal trends in assisted deliveries at a finer scale than that of the communes, that is, at the CsCOM level, we calculated a global spatial autocorrelation. This calculation allows us to determine whether there is a correlation between the number of assisted deliveries in the CsCOM and the metric relationships between these CsCOM. To take into account neighbouring values, we used the Moran index21 index. It is defined as the average of the products of the normalised values of pairs of points, weighted by the distance between two points. We performed this calculation on the whole area.

Where i,j=spatial unit; n=the number of spatial units; xi is the value of the variable in the unit i; x is the average of x and wij are the elements of the spatial interaction matrix to define spatial contiguity, distances or shared borders.
A second analysis consisted of understanding the spatial heterogeneity of assisted deliveries at the CsCOM level. We used spatial scan statistics.22 The principle is to cover the study area using scanning windows in the shape of circles and to determine the area that contains an abnormally high number of assisted deliveries using the log-likelihood ratio test.23
Analysis of CsCOM performance
To account for the different performances of the CsCOM, we selected five output indicators as they are the most frequently used for this type of analysis and correspond well to maternal and child health issues:
The rate of births attended by a skilled health professional.
Prenatal consultation rate (prenatal consultation 1).
The rate of postnatal visits.
The rate of curative consultations.
The rate of care utilisation for children under 5 years of age.
To evaluate the performance of the CsCOM at the beginning of the period under consideration, we performed a hierarchical ascending classification based on a distance matrix calculated using Ward’s method. The interest is in conducting a contextualised analysis (a CsCOM appears to be performing well in relation to its environment) and thus, by defining performance in a relative manner, to avoid the need to decide on thresholds.24 Finally, to measure the evolution of inequalities between CsCOM in terms of performance, we calculated the IQR for each month of the period for three attendance indicators for which we had monthly data: the rate of assisted deliveries, the rate of prenatal consultations, and the rate of curative consultations for children under 5. This is a robust dispersion index, particularly with respect to extreme values.
Analysis of insecurity
For the conflicts, each event (differentiated by ACLED)20 attacks on civilians, fighting against armed groups/FDS (Force de sécurité / security force), ImprovIsED ExplosIvE DEvIcEs (IED) explosions) was georeferenced and integrated into a GIS. We mapped an analysis of the spatial distribution of these events and the number of casualties. We counted the number of attacks, their frequency, and the number of victims within 10 km, 20 km and 50 km of the CsCOM. A smoothing map of the data25 produced a map of the exposure of the CsCOM to attacks. This map provides a framework for analysis of the evolution of the use of assisted deliveries
We used R software for statistics, QGIS for GIS and mapping, and SatScan for cluster analysis.
Qualitative approaches
Sampling
We based the selection exclusively of resource persons from the CsCOM interviewed on the results of the QUAN. We identified the CsCOM with contrasting numbers of assisted deliveries between those with higher-than-expected numbers and those with lower numbers. These selections were made in the two districts of the Mopti region: Bandiagara and Mopti. We then asked the members of the district management teams in the districts to identify the resource persons in these CsCOM to meet. In January 2020, we conducted semistructured interviews, informal discussions in each of the selected CsCOM. We conducted 22 interviews with the centre technical directors (DTC) (n=15), maternity ward managers (n=3), midwives (n=2), and international institutions (n=2); 12 interviews were conducted in Motpi and eight in Bandiagara. The health professionals interviewed were mainly managers (DTC, midwife) and had been in post for an average of 10 years. Research assistants conducted interviews on-site (n=2) or by telephone (n=20) when security conditions made on-site travel impossible. The research assistants have a strong background in fieldwork and qualitative studies. They produced verbatim transcripts of the interviews. They conducted the interviews using a thematic guide based on quantitative results and discussions with experts. The questions for the qualitative study stemmed from the results of the quantitative study on the evolution of the assisted delivery indicators during the study period. We compared them to the other CsCOM in the two health districts. We used these results to ask the DTCs what elements could explain the changes in the use of assisted deliveries that we observed in their CsCOM, or the significant geographical differences observed in one district between all the CsCOM, or between the two districts, depending on the year. We also asked them about the dates of arrival and presence of displaced persons in the commune, their healthcare conditions, and the use of the commune’s CsCOM by these refugees. We conducted the 20 interviews by telephone, with simultaneous note-taking. The assistants used the data to answer the various questions asked, under the supervision of the researcher, who was responsible for organising the qualitative study. The interviews lasted approximately 1 hour, and the notes were systematically transcribed.
Data analysis
We manually processed the observation and informal interview reports and the transcripts of the semistructured interviews using a classic content analysis method based on a series of themes and questions that had been previously identified following the initial geographical and quantitative processing of the attendance and security data.
Integration in mixed methods
The results of phase 1 QUAN inform phase 2 QUAL. Results on the distribution and spatial heterogeneity of assisted deliveries guided QUAL data collection to understand heterogeneity at the CsCOM level. Thus, the QUAL results contribute to the interpretation of the QUAN results.
Patient and public involvement statement
Patients were not included in this study.
Results
Contrasting dynamics of assisted deliveries
The spatial distribution of changes in the number of assisted deliveries over the entire period shows a decline in the number of deliveries per commune or stability in most of the study areas. However, we can identify two communes with high trends (Bandiagara in orange and Soroly in red) surrounded by communes with high declines (figure 2).

Change in the number of assisted deliveries between 2016 and 2019.
Contrasting concentrations of assisted deliveries at the CsCOM level
The Moran index was high over the 4 years. This result means that the study area is very heterogeneous and that there are clusters of CsCOM, that is, groups of CsCOM that are geographically close, that have a lower or higher number of assisted deliveries than expected. We observe that the Moran index increased from 0.41 to 0.49 between 2016 and 2019. Thus, there is an increase in heterogeneity in the number of assisted deliveries across the territory. In other words, as the years go by, there are more clusters of assisted deliveries (low and high).
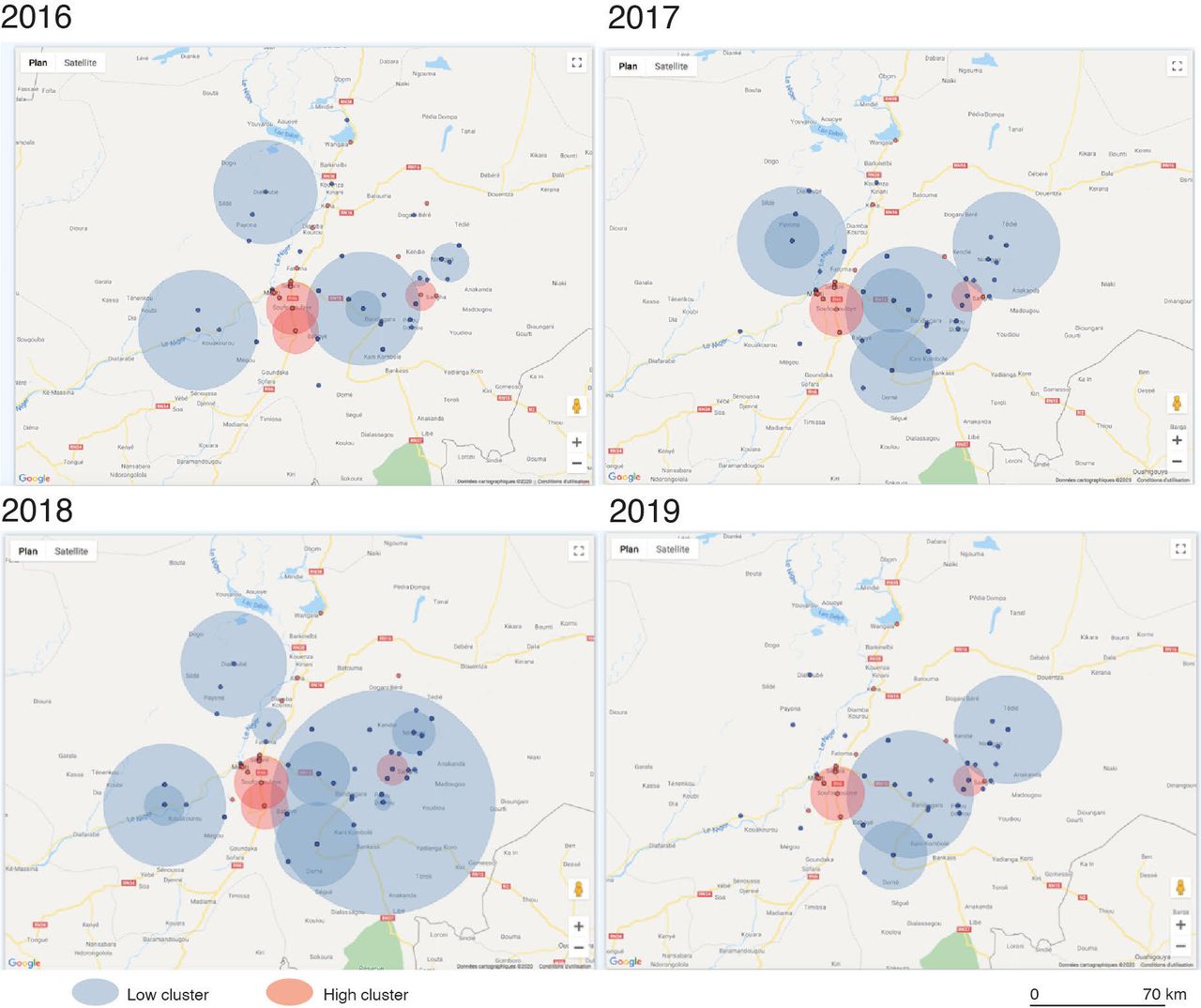
The spatial scan shows that it is always the same CsCOM that remain clustered over time. There is no major change except for a CsCOM west of Sio, which becomes a recurrent cluster only from 2018. However, fewer clusters with high values can be distinguished in 2017 and 2018. On the other hand, the number of clusters with low values is increasing, particularly in the commune of Bandiagara, where one cluster includes practically all the CsCOMs.
There were 10 recurrent high cluster CsCOM (in red) over the 4 years (figure 3). The average relative risk of these clusters is high (r=2.16). The probability of having more deliveries in these CsCOM is four to five times higher than expected. In detail, 8/10 CsCOM (Gouloumbo, Konna, Sokoura, Sévaré 2, Toguel, Medina Coura, Soufroulaye, Samadougou) are located in the commune of Mopti, 2/10 (Kendie and Sangha) in Bandiagara and 7/10 are CsCOM. We also note that two high cluster CsCOM are recurrent over 3 years (2016, 2017, 2019) and one high cluster CsCOM is recurrent over 3 years (2016, 2018, 2019).

Spatial clusters of the number of assisted deliveries per year.
In other words, deliveries are concentrated in a small number of CsCOM that are generally close to each other and the other CsCOM in the districts are less and less frequented. This phenomenon tends to intensify during the period under consideration.
Divergence of CsCOM in terms of attendance
To explain the existence and persistence of high assisted delivery clusters, we proposed an analysis of the level of performance (ratio to outputs) of the different CsCOM.
The hierarchical ascending classification makes it possible to identify three classes of CsCOM according to their performance in 2017 (figure 4). A first class is characterised by low performance (green), a second class is characterised by rather high performance (orange) and a third class is composed of two outsiders with exceptional performance (purple). Table 1 shows that the high assisted delivery clusters identified above are essentially CsCOM classified as rather and exceptionally efficient, apart from Soufroulaye, Toguel and Konna. Of these last three, only one shows really poor performance, while the other two show moderate results in 2017 and show a clear progression over the period. This analysis of performance confirms that the high clusters identified earlier appear around the high-performing CSCOMs in 2017.
Level of performance of the CsCOM in the upper cluster

Representation of the hierarchical ascending classification.
This inequality in CsCOM performance tended to increase during the period under consideration, as indicated by the change in the IQR of rates of assisted deliveries per CsCOM, prenatal consultations and curative consultations for children under 5. The increase in this gap indicates a divergence, for each of the three indicators, between the 25% of CsCOM with the lowest attendance and the 25% with the highest attendance. In short, the gap is gradually widening between the lowest and highest performing CsCOM. The appearance of clusters indicates a more general movement of divergence in performance.
Evolution of the security situation and geography of violent events
In order to improve our understanding of the appearance of clusters, we are interested in the geographical distribution of security events. On the one hand, we note that the evolution of the security situation deteriorates sharply at the beginning of the period. On the other hand, that insecurity is unevenly distributed over the territory considered. Regarding the evolution of the security situation between 2016 and 2019, there were 819 attacks in Mali with 1875 victims. From 2017 onwards, conflicts intensified, mainly in the districts of Douentza, Koro and Tenenkou (further north in the study area), and gradually spread to the districts of Mopti and Bandiagara considered in this study. In these two districts, there were 184 events and 366 victims (figure 5). The number of events and associated victims increased between 2016 and 2019. Regarding the spatial heterogeneity of insecurity, we note that, counterintuitively, assisted deliveries are not located in the areas furthest from the violent events.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Violent events in the districts of Mopti and Bandiagara.
At the level of the two districts, the number of assisted deliveries in the CsCOM increased from 2016 to 2018 but decreased by nearly 20% in 2019. We note that the areas (figure 5) where the number of assisted deliveries is significant in 2019 (red colours) is associated with a significant number of events since 2016 (red proportional points). This is particularly the case in the Bandiagara health district and in some CsCOM located near Mopti. The CsCOM identified as high-performing clusters are thus found. We note that a high number of events, particularly in the most isolated parts of the Bandiagara district, would not impact the number of assisted deliveries. A similar phenomenon was observed in Mopti. However, the geographical contexts are different. In Mopti, the CsCOM are located near one of the country’s major traffic arteries, whereas in Bandiagara, the CsCOM are landlocked, particularly in the eastern part of the district.
These analyses do not establish a causal link, but help to better understand the security context in the vicinity of the CsCOM and at fine scales.
Qualitative analysis
The impact of population displacement on the healthcare system
The interviews with participants shed light on the trend towards strengthening the abovementioned clusters. Three explanatory elements can be advanced for the low clusters. First, population displacement partly explains the decrease in the number of deliveries. As the security situation worsened, particularly in the Bandiagara district, it gradually led to massive departures of the population. Second, for the population that remained in the area (or returned after a temporary displacement), insecurity tends to reduce the income of families (and thus their inclination to use paid care) and encourages them to limit travel to the CsCOM, particularly for women who live several kilometres away. Third, analysis revealed that qualified health workers often refused to go to practice, or were absent, particularly in the Bandiagara district, for security reasons. In these areas, people are also less likely to use services because of poor quality and availability of care.
The CsCOM in rural areas were kept active by relying on health workers with little or no qualifications and recruited locally (matrons, warehouse managers, nurses, volunteers) whom the population does not fully trust for deliveries. In addition, the rural maternity units of the Bandiagara CsCOMs did not function normally in 2019 because of the jihadist attacks.
On the high cluster side, insecurity has generated massive population displacements in the Mopti region, particularly towards the city of Mopti, which probably explains in part the increase in the number of assisted deliveries. The displaced have settled in the communes of Mopti, Socoura, Fatoma and Sio in the Mopti district and Doucombo, Sangha, and Timiniri in the Bandiagara district.
Prevention actions of NGOs in refugee camps
Other factors contributing to increased assisted deliveries are the contraceptive awareness campaigns conducted by some NGOs in the framework of family planning since 2016 and the free healthcare programmes, particularly for deliveries, for displaced persons since 2018. Free healthcare supported by an NGO was effective for all displaced persons from 2020.
Discussion
We conducted this study in the health districts of Mopti and Bandiagara between 2016 and 2019 on the evolution of the number of assisted deliveries and the use of maternal and infant care in general. It reveals strong territorial heterogeneity. While the majority of the communes in the region show zero or negative rates of change, a few communes, including Bandiagara, stand out with an increase in the rate of assisted deliveries of more than 200%. At the CsCOM level, the analysis identifies 10 CsCOM with high rates of assisted delivery, eight of which are in the Mopti district alone. Like the Bandiagara CsCOM, these are located near recurrent security events. The difference could be explained by the better connectivity to national transportation networks in Mopti and the fact that the Bandiagara district is very isolated. Several arguments can be advanced to explain the appearance of these clusters. First, these CsCOM appear to be performing well in 2017 and have high rates of assisted deliveries, but also high prenatal and postnatal follow-up and high use of healthcare in general. This coincidence suggests that clusters appear where CsCOM have a high level of functionality. It can be hypothesised that the most performant ones also become the most resilient in the sense of maintaining services for women. Second, fluctuations in the number of assisted deliveries in CsCOM can be explained mainly by massive flows of displaced persons, reducing the number of deliveries in the zones of departure and increasing them in the reception areas where NGOs are active, particularly if these have awareness-raising and free-of-charge programmes. Four of the 10 CsCOM belong to the single urban entity of Mopti, which is the largest city in Mali. Four of the six rural CsCOM are located on the only road leading to the north of Mali (BamakoMopti-Gao axis). Finally, elsewhere, in more remote areas, the persistence of large numbers of assisted deliveries can be explained by the maintenance of dynamic, performant CsCOM, as well as the non-hostility of armed groups to maintain care, as stated by the health personnel interviewed.
Most studies of maternal and reproductive health utilisation take a generally macro approach in which the minimum unit of analysis is the district or region.24 26–29 By focusing on a finer geographical scale, this analysis shows that conflict-affected areas are heterogeneous. These territories are unevenly affected by conflict because of their physical geography, the location of urban areas and road infrastructures, and the dynamics of conflict and population displacement. This study highlights that the administrative or health mapping of a territory, while useful for planning purposes, is not necessarily a relevant analytical framework for understanding the impacts of a conflict situation on the use of healthcare.
The analysis of the level of performance of health centres was used on an exploratory basis and on a small number of indicators. However, it offers interesting avenues for a rapid methodology for evaluating the relative performance of a homogeneous group of health units (health centres, health regions, etc). It provides a simple alternative to analytical frameworks inspired by the evaluation framework proposed by the WHO.30–32 Another advantage is that it proposes a relative evaluation, since performance is only identified within the sample considered. This characteristic limit the possible uses of this method, but it avoids the need to decide on a threshold to define performance levels. Jackline Odhiambo and her colleagues highlighted this challenge in their assessment of the resilience of the southern Sudanese health system: ‘The challenging question concerns how to set the threshold of the percentage of indicators to detect improvement or even how to set a health system coverage target in the first place. These considerations are essential for measuring a country’s health system resilience’.24
The results of this study add to our knowledge of the impact of conflict on assisted deliveries and the use of healthcare in general. It shows that not all services are affected in the same way, whereas other studies in Burkina Faso show the opposite.9 In contrast, in South Sudan, which was heavily impacted by violent events, there was a low use of assisted delivery during the conflict between 2013 and 2017. However, there are rare locations where service delivery was functional. These corresponded to camps in which health development, coordination and humanitarian efforts were most prominent.26 We observe a similar phenomenon. Some clusters correspond to CsCOM located near camps where humanitarian NGOs offer additional services and prevention campaigns. Humanitarian organisations are, therefore, fundamental to maintaining basic services, including in the Centre de Santé Communautaire (CsCOM) of the Malian health system. Although humanitarian aid has increased since 2019, it remains insufficient and still below the needs of the population. For example, in October 2022, an estimated 23% of the funds needed for health needs were allocated across Mali.33 In 2019, it was 3%.34 There are now 28 international and national NGOs in the Mopti region, the majority of which are in the larger towns. Due to the lack of functional infrastructure and insecurity, the most isolated sites, remain difficult to access, including for NGOs, which explains their weak presence. The consequence is an unequal presence of NGOs in the Mopti region, which is reflected in the gap between the high and low clusters identified in the study. Should we fear, as in southern Sudan, that the prolonged violence in the area will affect the availability of humanitarian providers? It is imperative that all governments and partners working in the health sector ensure that essential health services are accessible to all people living in conflict zones, that they operationalise the Humanitarian-Development-Peace nexus defined in 2016 at the first world humanitarian summit, and that they work together to help rebuild local and national health systems.35
Improving assisted deliveries in conflict zones remains a significant challenge, particularly in the isolated rural areas of African LMICs. Indeed, in these places, the low level of assisted deliveries is primarily associated with the legacy of several decades of health system dysfunction (absenteeism, lack of resources, refusal of assignments in isolated areas) and structural difficulties (scattered population, accessibility, means of travel). The implementation of interventions to improve assisted deliveries in these conflict contexts difficult and rare. The main obstacles identified in several literature reviews on this topic in LMICs36 37 included lack of security, lack of trained health workers, lack of financial resources and the influence of international donors on intervention choices and locations.38 However, actions do exist and are the result of the creativity of the humanitarian system,39 which has developed new modes of delivery to improve maternal health in particular. Some of these interventions could be appropriate to the situation in the Mopti region. One example is the recruitment and training of community health workers, including community health workers and traditional healers. Examples from the Democratic Republic of Congo and Somalia have proposed transferring or sharing certain tasks with these new agents to strengthen health training. Elsewhere, in Syria, midwifery capacity-building programmes have been implemented in response to the population’s preference for home deliveries, in part because of the sense of insecurity felt inside hospitals, which are often the target of attacks.40 In other situations, NGOs have directly negotiated with armed groups to agree to maintain the health system.13 Reinforcing the image of neutrality in health can, therefore, help to secure health centres and their workers.
Limits
One of the limitations of this study is that it did not include the opinions of healthcare users. The security conditions in the study area did not allow for lengthy interviews or focus groups. We focused our analysis on the DTCs who were familiar with the functioning of their CsCOM.
Conclusion
This research demonstrates the need to study healthcare use at the finest possible scales. Our results confirm that combining methodological approaches is essential to explain significant use in the local context. The analysis of the number of assisted deliveries in conflict zones must consider the number of procedures, the nearby security context, the number of internally displaced persons and the presence of camps in which humanitarian organisations offer programmes.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by 34/2018/CE-INRSPof Participants gave informed consent to participate in the study before taking part.
Footnotes
Handling editor Seye Abimbola
Twitter @mavalo76, @dansinediarra, @ValeryRidde
Contributors The study was carried out with the fair participation and collaboration of the international researchers (French: EB, VR, TL and Malians: LT and DD), and the research assistants (YD and SD). The research assistant (YD and SD) was trained and supported by LT in data collection and analysis. All results were interpreted by the MISELI leaders who participated in the writing of the article. The order of authorship reflects a fair distribution of the intellectual contribution of the coauthors in the research process. EB and VR coordinated the overall research in collaboration with the coauthors. EB took the lead in writing the article, TL writing the section of performance but all authors participated in writing and validating the content and VR was the final author. EB is guarantor of this paper.
Funding This work was supported by Agence Française de Développement.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.