Article Text

Abstract
Introduction Implemented in 2013 in Senegal, the Programme National de Bourses de Sécurité Familiale (PNBSF) is a national cash transfer programme for poor households. Besides reducing household poverty and encouraging children’s school attendance, an objective of the PNBSF is to expand health coverage by guaranteeing free enrolment in community-based health insurance (CBHI) schemes. In this paper, we provide the first assessment of the PNBSF free health insurance programme on health service utilisation and health-related financial protection.
Methods We collected household-level and individual-level cross-sectional data on health insurance in 2019–2020 within the Niakhar Population Observatory in rural Senegal. We conducted a series of descriptive analyses to fully describe the application of the PNBSF programme in terms of health coverage. We then used multivariate logistic and Poisson regression models within an inverse probability weighting framework to estimate the effect of being registered in a CBHI through the PNBSF—as compared with having no health insurance or having voluntarily enrolled in a CBHI scheme—on a series of outcomes.
Results With the exception of health facility deliveries, which were favoured by free health insurance, the PNBSF did not reduce the unmet need for healthcare or the health-related financial risk. It did not increase individuals’ health service utilisation in case of health problems, did not increase the number of antenatal care visits and did not protect households against the risk of forgoing medical care and of catastrophic health expenditure.
Conclusion We found limited effects of the PNBSF free health insurance on health service utilisation and health-related financial protection, although these failures were not necessarily due to the provision of free health insurance per se. Our results point to both implementation failures and limited programme outcomes. Greater commitment from the state is needed, particularly through strategies to reduce barriers to accessing covered healthcare.
- health insurance
- health services research
- health economics
- health policy
- maternal health
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Providing free or heavily subsidised health insurance to the indigent population is viewed as a core strategy for achieving universal health coverage in low-income and middle-income countries.
Various evaluations of the free of heavily subsidised health insurance programmes on health service utilisation and financial protection—which are needed to inform policy—have been conducted, reporting mixed results.
WHAT THIS STUDY ADDS
We provide the first evaluation of the effects of the Senegalese free health insurance programme, which is part of the Programme National de Bourses de Sécurité Familiale.
Unlike studies investigating only one outcome and one dimension of Universal Health Coverage, we investigate the effects of the free health insurance programme on a series of outcomes pertaining to both health service utilisation and health-related financial protection.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We believe our study will help inform policymakers on the concomitant strategies to implement for the free health insurance programme to effectively reduce both the unmet need for healthcare and the health-related financial risk among the Senegalese indigent population.
Introduction
Universal health coverage (UHC) is at the heart of the Sustainable Development Goals (2015–2030), as it represents a cross-cutting challenge to improve the health of populations by guaranteeing access to care for the greatest number while reducing socioeconomic inequalities. Many low-income and middle-income countries (LMICs) are moving towards UHC, mainly through the implementation of health insurance systems and of free healthcare programmes for specific population groups. Existing health insurance systems vary widely in terms of supply-side and demand-side characteristics, for instance, the territorial level (from community-based health insurance (CBHI) schemes to national health insurance), the operational capacity (degree of professionalisation, cooperation with local health facilities, etc), the terms and conditions of enrolment (voluntary or compulsory, at the individual or household level, etc), or the premium payment system (fixed or sliding-scale premiums, sometimes free or partly subsidised).1
Over the past two decades, Senegal consolidated the free healthcare programmes and developed and implemented at least one CBHI scheme in each rural community, with the objective to expand health coverage to people in the informal sector and to rural populations, and thereby move toward UHC.2 However, voluntary enrolment rates remain very low.3 4
In 2013, Senegal initiated a national cash transfer programme for poor households conditioned on income, the Programme National de Bourses de Sécurité Familiale (PNBSF).5 6 Besides reducing household poverty and encouraging children’s school attendance, a secondary objective of the PNBSF is to help improve health coverage by guaranteeing de jure free enrolment (ie, fully subsidised, publicly financed) in a CBHI scheme to all members of the indigent households eligible to the PNBSF.7 8
A large number of studies examined the effects of health insurance—mainly voluntary CBHI schemes or national health insurance—on health service utilisation and health-related financial protection.9–13 Thus, health insurance has generally been found to improve access to healthcare in LMICs. In parallel, studies reported mixed results as to whether health insurance provides health-related financial protection.
In contrast, fewer studies investigated the effects of free or heavily subsidised health insurance programmes (see for instance the studies conducted in China,14 Colombia,15 India,16 Indonesia,17 Peru18 and Thailand19), even though such studies are needed to inform policy. To focus on studies in sub-Saharan Africa, the few available studies on free health insurance programmes for the poor—which were mainly focused on maternal care—reported mixed results. Free health insurance enrolment increased maternal care service use in Ghana and Rwanda.20 A study in Tanzania found no effect on maternal service use, although the free health insurance programme reduced the amount paid for antenatal and delivery care.21 A randomised experiment among informal workers in urban Kenya highlighted that free health insurance did not favour health service utilisation.22
In this paper, we provide the first assessment of the Senegalese PNBSF programme in its health coverage dimension, based on primary data collected in 2019–2020 in the rural area of Niakhar (Fatick region). More specifically, we investigate the effects of the free PNBSF CBHI enrolment on individual-level and household-level outcomes pertaining to the two fundamental dimensions of UHC: health service coverage (ie, that everyone can receive healthcare when needed), and financial protection (ie, that the use of health services, when it occurs, does not lead to financial difficulties).
Methods
The Senegalese free health insurance programme for the poor
The PNBSF programme provides quarterly cash transfers of 25,000 CFA Francs to the country’s poorest households.5 The programme also provides free (fully subsidised) insurance premiums for households beneficiaries of the PNBSF cash transfer to enrol in their local CBHI scheme. This free health insurance is supposed to be provided to all members of beneficiary households, who are issued a CBHI membership card on registration. Once enrolled, copayments of medical expenses for services included in the benefits package are supposed to be fully covered by the PNBSF.
Besides the free CBHI enrolment provided by the PNBSF programme, regular enrolment in Senegalese CBHI schemes is voluntary, with the possibility to enrol individually. After having paid a lump sum of 1000 CFA francs for the household to register with the CBHI organisation, a fixed premium of 3500 CFA francs has to be paid per individual/year to benefit from the CBHI package (the Senegalese State subsidising the same amount, for a total premium of 7000 CFA francs per individual/year). Then, the beneficiaries’ healthcare costs are covered at 50% (in private pharmacies) or 80% (in public facilities and for generic drugs).
To be covered, all CBHI beneficiaries must first obtain a so-called letter of guarantee (lettre de garantie in French) at the office of their CBHI. They must also seek care only at local health facilities which have an agreement with the CBHI. The benefits package includes primary care and preventive consultations, drugs, hospitalisations, deliveries, complementary exams, special care and evacuations.
The CMUtuelleS survey
We used primary data from the CMUtuelleS survey, which we conducted in 2019–2020 in the Niakhar area (Fatick region, Senegal), a rural area of 203 km2 located 135 km east of Dakar. This area of 30 villages comprises four primary health facilities, and residents may enrol in two CBHI depending on their village of residence. The nearest secondary hospital is the Fatick regional public hospital (located about 20 km from the Niakhar area).
The CMUtuelleS survey aimed at investigating various dimensions of UHC.4 Given the low CBHI enrolment rates in Senegal,2 3 the sample was stratified into three groups of households depending on the health insurance status of their members: (1) not having any CBHI member, (2) having at least one member who voluntarily enrolled in a CBHI and (3) having at least one member who benefited from the fully subsidised CBHI enrolment through the PNBSF. Detailed information on the CMUtuelleS survey design and implementation is provided in online supplemental appendix A2.
Supplemental material
Our sample was constituted of 1001 households (about one-third of households in the Niakhar area) and 1787 adults.
The survey data were also matched with the Niakhar Population Observatory23 to obtain additional demographic and socioeconomic characteristics of all individuals and households. The Niakhar Population Observatory is a Health and Demographic Surveillance System which collects prospective data on all individuals in the area of 30 villages in which the CMUtuelleS survey was conducted.
A reflexivity statement on our international partnership between high-income and LMICs is provided in online supplemental appendix A3.
Data and descriptive analysis
The main variable of interest (ie, the ‘treatment’ variable) was the health insurance status, measured at the individual level (ie, not enrolled in a CBHI, enrolled voluntarily, or enrolled through the PNBSF programme) or at the household level as previously defined.
We first conducted a series of descriptive analyses to fully describe the application of the PNBSF programme in terms of healthcare coverage. In all summary statistics, data were weighted using sampling weights to be representative of the study area.
All variables used in the present study are defined in online supplemental appendix A4.
Catastrophic health expenditure was defined as out-of-pocket payments for health accounting for 40% or more of a household’s capacity to pay (ie, the income remaining after subsistence needs are met).24 We also considered two alternative thresholds of catastrophic health expenditures (namely, out-of-pocket health expenditures ≥30% and 20% of non-food expenditures, respectively).
Econometric analysis
We estimated the effects of health insurance enrolment—either voluntary or fully subsidised through the PNBSF programme, as compared with having no health insurance—on a series of outcomes and populations. Because CBHI enrolment is not randomly distributed in the population, we used multivariate logistic and Poisson regression models within an inverse probability weighting (IPW) approach. More specifically, we estimated the average treatment effect (ATE) of a given treatment (in our case being registered in a CBHI either voluntarily or through the PNBSF programme) by weighting the ‘treated’ individuals by the inverse of the probability of being their group, thereby reducing biases due to covariate imbalances between treatment groups. In our case, there are three treatment groups of individuals or households (ie, with no, voluntary (ie, who paid the premium voluntarily), or free PNBSF-subsidised health insurance). Details on IPW with multivalued treatment can be found in Wooldridge.25 26 In the first step, we estimated the probability of health insurance enrolment using multivariate multinomial logistic models (at the individual and household levels). In the second step, we estimated a series of multivariate logistic and Poisson models weighted by the inverse probability of treatment obtained in the first step, to identify the factors associated with each outcome and obtain the ATEs of voluntary and PNBSF-subsidised CBHI-enrolment (both vs no enrolment). The outcomes considered were measured on different populations, at the individual or household level.
First, we investigated whether CBHI enrolment increased individuals’ health service utilisation, based on the population of individuals who had a health problem in the last 2 months. The dependent variable was whether the individual consulted in a health facility (model 1), using a logistic regression adjusted for demographic and socioeconomic characteristics, the perceived quality of health services, the distance to the nearest health facility, and the duration and severity of the health problem considered.
Second, we examined whether health insurance enrolment favoured maternal health service utilisation, based on the population of women who had a live birth in the last 2 years. Two dependent variables were considered: the number of prenatal care visits (model 2), and whether the woman gave birth in a health facility (model 3). Models 2 and 3 were estimated using Poisson and logistic regressions, respectively, both adjusted for demographic and socio-economic characteristics, the perceived quality of health services, and the distance to the nearest health facility.
The third set of analyses was performed at the household level. We assessed whether health insurance enrolment protected households against the risk of forgoing medical care and against the risk of catastrophic health expenditure. Five logistic models were estimated on the whole sample of households, with the following dependent variables: whether the household had to forgo medical consultation (model 4) and medical treatment (model 5) in the last 12 months due to financial hardship, and whether the household had catastrophic health expenditures using the 40% (model 6), 30% (model 7) and 20% (model 8) thresholds, respectively. All models were adjusted for households’ and household heads’ demographic and socio-economic characteristics, and the distance to the nearest health facility.
Robust standard errors were computed for all regressions. Household-level clustered standard errors were calculated in all individual-level regressions to account for intra-household correlation. The study area comprises 30 villages, which is too few to calculate village-level clustered standard errors.27 All regressions were weighted by the product of (1) the inverse probability of treatment obtained in the first-step multinomial logistic model of health insurance enrolment at the individual level (models 1–3) or household level (models 4–8) and (2) the sampling weights to be representative of the study area.28 All analyses were performed using Stata/SE version 16.29
For all regressions, we provide tables with average marginal effects. The marginal effects for the health insurance status variable are the ATEs of CBHI enrolment on each outcome. Relative risk ratios (RRR), OR and incidence rate ratios (IRR) are also provided for multinomial logistic, logistic and Poisson regressions, respectively, along with their graphical representation.
Results
Summary statistics
In the study area, 55% of households reported being beneficiaries of the PNBSF cash transfer programme (ie, they have received the cash transfer from the PNBSF at least once, including all generations of beneficiaries). Individual-level health insurance statistics indicated that 87% of the adult population in the area were not registered in a CBHI, with free PNBSF-subsidised and voluntary CBHI enrolment representing 9% and 4% of the adult population, respectively. Thereby, 82% of the households did not have any member covered by health insurance, with only 11% and 7% of the households having at least one PNBSF-subsidised and voluntarily enrolled CBHI member, respectively (online supplemental appendix A4).
Summary statistics on the whole sample of individuals and households, and on each sub-population considered, are provided in table 1. Online supplemental appendix A5 presents these summary statistics stratified by health insurance status. Online supplemental appendix A6 presents additional results on the knowledge of CBHI by health insurance status and by whether the individual’s household was a beneficiary of the PNBSF cash transfer programme.
Summary statistics
Among individuals belonging to a household that received at least once the cash transfer from the PNBSF and were not members of a CBHI, 69% did not know about the existence of CBHI before the survey. Among the 31% who had already heard of CBHI before the survey, 47% had heard about them through an information campaign of the CBHI, 45% through a relative, 19% through a CBHI member, and 17% through the media (figures not mutually exclusive).
Among the 11% of individuals both receiving the PNBSF cash transfer and being actually registered for free in a CBHI, the level of knowledge of health insurance was surprisingly low. Among these individuals, 46% have even been registered in the CBHI without their knowledge.
The adult population—54% of which were women—was 53 years on average. 10% were not in a union at the time of the survey (either single, divorced or widowed), 84% had no formal education, 58% had poorer self-rated health and 71% had a lower perception of the quality of healthcare services in their area. On average, individuals lived 5.5 km and 3.2 km away from the nearest CBHI and health facility, respectively.
Among the adult population, 23% (n=418) had, in the 2 months preceding the survey, a health problem that prevented them from carrying out, partially or totally, their daily activities. Among these 418 adult individuals, only 33% had a medical consultation in a health facility. Nevertheless, 70% of these reported health problems lasted for 3 days or more (with an average of 10 days) and were experienced as severe in 17% of cases.
Among the women of reproductive age (15–49 years), 36% (n=197) had a live birth in the 2 years preceding the survey, of whom 83% did not have any type of health insurance, and 6% and 11% were enrolled in a CBHI through the PNBSF programme and voluntarily, respectively. They had three prenatal care visits on average, but only 54% gave birth in a health facility.
At the household level, household heads were aged 57 years on average, 7% of them were women, and 15% were not in a union. The highest level of formal education was primary education for 16% of the household heads and secondary or higher education for 5% of them. A household had 12 adult equivalents on average. There was a poverty rate of 51% (calculated based on equivalised household expenditure data). The incidence of catastrophic health expenditures in the area was estimated to be 6.2%. Due to financial hardship, 35.6% and 24.0% of the households had to forgo medical consultation or treatment of one of their members, respectively.
The Strengthening the Reporting of Observational Studies in Epidemiology checklist for observational studies is provided in online supplemental appendix A7.
Results of the econometric analysis
Concerning the individual-level analyses, the results of the first-step multinomial logistic model of health insurance enrolment are presented in online supplemental appendix A8, along with the graphical representation of the RRR. A covariate balance table is provided in online supplemental appendix A9, with results indicating good balancing properties across treatment and control groups.
Compared with not being enrolled in a CBHI, the free PNBSF CBHI enrolment was associated with being older, being female, not being in a union, living closer to the nearest CBHI, and living in a household with fewer adult equivalents. Voluntary CBHI enrolment (ie, having paid the premium voluntarily) was associated with being younger, having a higher level of formal education, having poorer health, being in the richest wealth quartile and living in a household with more adult equivalents.
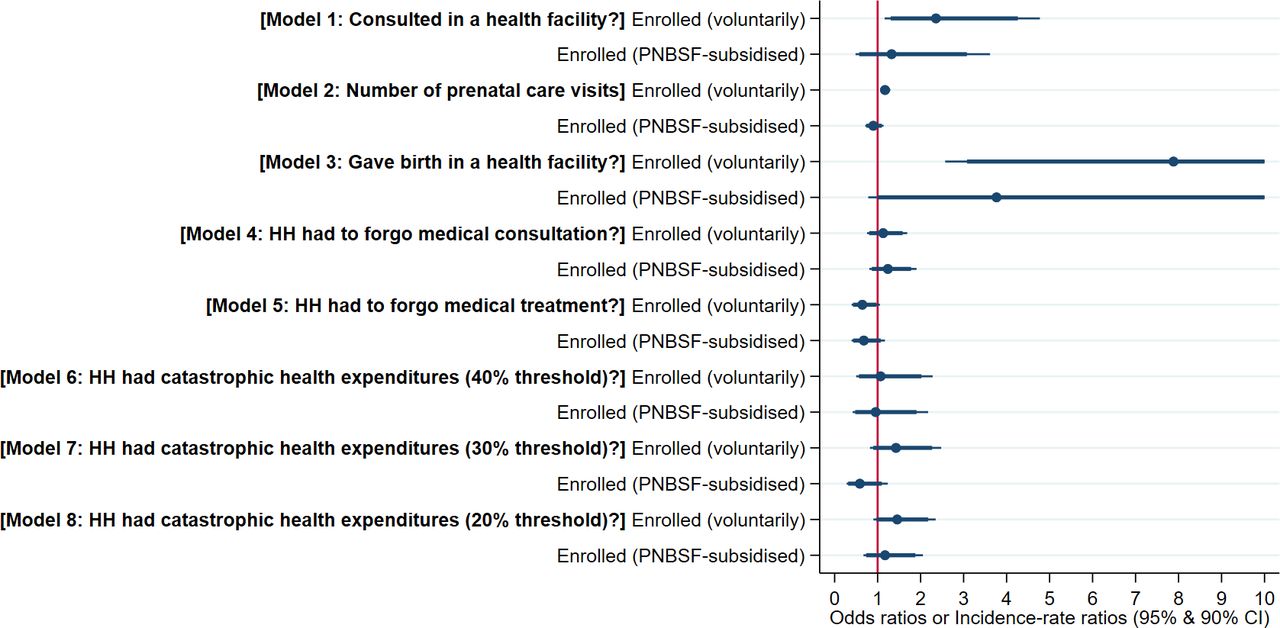
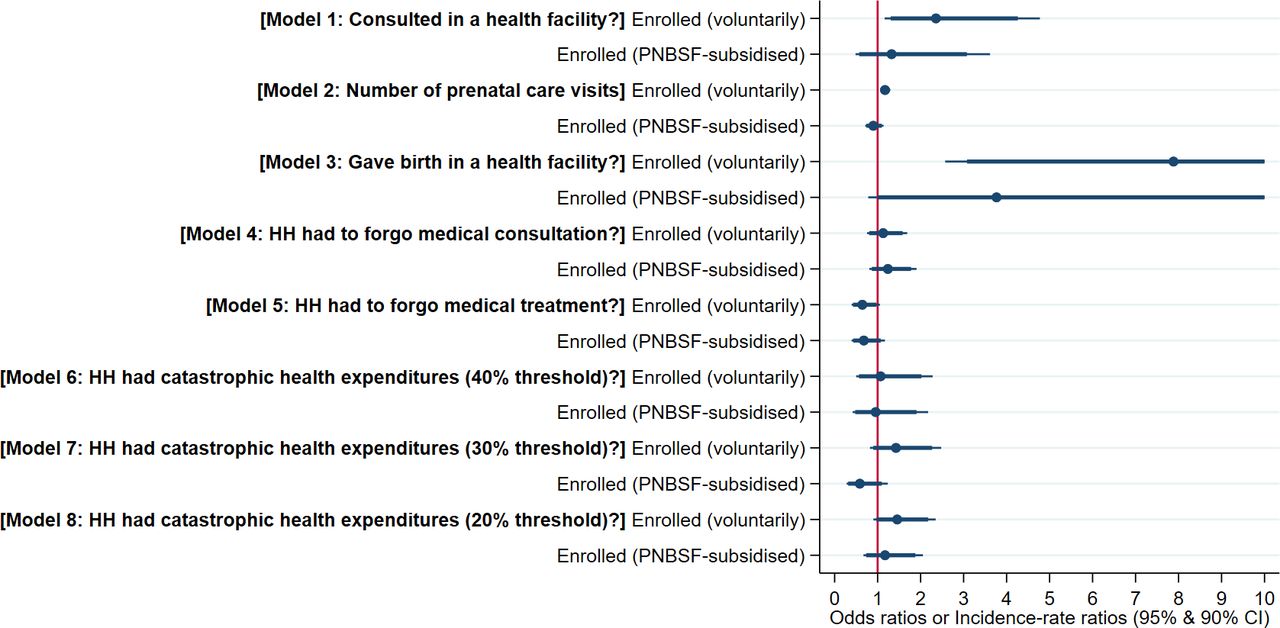
The main results of model 1–8—that is, the effects of CBHI enrolment on each outcome—are presented in table 2 (OR or IRR, ATE and predictions) and depicted in figure 1 (OR or IRR).
{kind=link}
Inverse probability weighting regression results of models 1–8: effects of voluntary and PNBSFsubsidised CBHI-enrolment on each outcome. Notes: In all regressions, the reference group was individuals or households not enrolled in a CBHI. ORs are provided for logistic regressions (models 1 and 3–8), and incidence rate ratios for Poisson regressions (model 2). Upper CI limits for model 3 are truncated for readability (upper 95% CI were 24.2 and 18.1 for voluntarily and PNBSF-subsidised enrolled, respectively). Full results for each model are provided in online supplemental material. CBHI, community-based health insurance; HH, household; PNBSF, Programme National de Bourses de Sécurité Familiale.
Summary of the inverse probability weighting regression results of models 1–8: effects of voluntary and PNBSF-subsidised CBHI-enrolment and predictions for each outcome
The effect of the free PNBSF CBHI enrolment was first assessed concerning an adult’s probability of consulting in a health facility following a health problem that occurred in the last 2 months (model 1). Full results and graphical representation of the OR are provided in online supplemental appendix A10. When compared with having no health insurance, benefiting from the PNBSF-subsidised CBHI enrolment was not associated with a higher probability of consulting in a health facility in case of health problems (36.0% vs 31.5%, p=0.591), while on the other hand having voluntarily enrolled in a CBHI increased the probability of consulting in a health facility by 14.4 percentage points (45.9% vs 31.5%, p<0.05).
Regarding women who had a live birth in the 2 years preceding the survey, results of model 2 showed that, compared with not having any type of health insurance, benefiting from the free PNBSF CBHI enrolment was not associated with having a higher number of prenatal care visits (2.9 vs 3.3 visits, p=0.361), while on the other hand having voluntarily enrolled in a CBHI increased the average number of prenatal care visits by 0.6 (3.8 vs 3.3 visits, p<0.01), that is, by 17%. Full results of model 2 are provided in online supplemental appendix A11. Nonetheless, results of model 3 indicated that, compared with having no health insurance, being enrolled through the PNBSF programme increased the probability of health facility delivery by 23.8 percentage points (68.1% vs 44.3%, p<0.10). See online supplemental appendix A12 for the full results of model 3. This was also true—to a greater magnitude—for voluntarily enrolled women, who had a 34.9 percentage points higher probability of health facility delivery compared with women not insured (79.2% vs 44.3%, p<0.01).
Turning to the household-level analyses, the results of the first-step multinomial logistic model of household-level health insurance enrolment are presented in online supplemental appendix A13, along with the graphical representation of the RRR. Results showed good balancing properties across treatment and control groups (see the covariate balance table provided in online supplemental appendix A14).
At the household level, being enrolled in a CBHI through the PNBSF programme did not significantly reduce the households’ probability of forgoing medical consultation (model 4, with full results presented in online supplemental appendix A15) and of forgoing medical treatment (model 5, with full results presented in online supplemental appendix A16), compared with not being covered by health insurance. The only significant effect of health insurance was found for voluntarily insured households, whose probability of forgoing medical treatment was reduced by 7.2 percentage points compared with households not insured (18.9% vs 26.1%, p<0.10).
Our results also revealed that benefiting from the free PNBSF-subsidised health insurance enrolment did not protect households against the risk of catastrophic health expenditure (of note, this was also true for households having at least one voluntary-enrolled member). Indeed, there was no significant difference between the three groups of households in the probability of catastrophic health expenditure (model 6, with full results presented in online supplemental appendix A17). This result was robust to the use of alternative thresholds of catastrophic health expenditures, namely, out-of-pocket health expenditures ≥30% (model 7, as also presented in online supplemental appendix A18) and ≥20% (model 8, as also presented in online supplemental appendix A19) of non-food expenditures.
Discussion
Our results point to failures of the PNBSF free health insurance programme, with almost no significant effect on any of the outcomes pertaining to health service utilisation and health-related financial protection. How to interpret these puzzling results? It is important to distinguish between programme implementation and programme outcome assessment.30 31 Our results suggest the presence of both implementation failures and limited programme outcomes, although both dimensions are generally difficult to disentangle.
Flaws in the implementation of the PNBSF free health insurance programme
Our study point to a series of barriers to effective health coverage through the PNBSF programme. First, in the Niakhar area, there was a large gap between the proportion of households benefiting from the PNBSF cash transfer programme (55%) and the proportion of households who had at least one member who benefited from the PNBSF free health insurance enrolment (11%). Besides confirming the low health insurance enrolment rates usually reported in Senegal (voluntary health insurance coverage was even lower),2 3 and in sub-Saharan Africa in general,32 33 this suggests a dysfunction of the PNBSF, which is supposed to provide fully subsidised membership to all members of households registered in the programme (ie, receiving the cash transfer). Even more problematically, our results indicated that, among those individuals belonging to a household that received at least once the cash transfer from the PNBSF and were not members of a CBHI, 69% did not know about the existence of CBHI before the survey (and therefore had no information about their right to free PNBSF-subsidised CBHI membership). A study in Ghana on the impact of a programme pairing cash transfers with a premium waiver for health insurance enrolment also found that large enrolment gaps remained.34 These gaps were likely due to insufficient communication and misunderstanding of the integration of the cash transfer and premium waiver provision.
Surprisingly, the level of knowledge of health insurance was low even among individuals registered in the PNBSF programme and actually registered for free in a CBHI. Paradoxically, 46% of these individuals have been registered in the CBHI without their knowledge, and thereby have not been informed of their free registration and their rights. Hence, the lack of significant programme effects could be linked to the presence of ‘virtual membership,’ which can themselves be a way for CBHI organisations to attract additional capital inflow.35
This is in line with a recent study analysing the universal health insurance models in Africa—including that of Senegal—which highlighted a paradoxical situation, with an apparently high health insurance coverage of the indigent population nationwide (ie, 19% in 20182) but who tend to be not effectively covered.1 This was partly explained by the delays in the payment of subsidies by the Senegalese government, forcing CBHI organisations to restrict access to covered healthcare.1 Similarly, partly due to failures in the implementation of performance-based financing (eg, delays in reimbursements of health facilities),36 possessing a user fee exemption card did not increase health service utilisation among the ultra-poor in Burkina Faso.37
Another evaluation of a free health insurance programme—targeted at poor pregnant women in Tanzania—found that its effects were limited by demand-side and supply-side constraints affecting implementation, in particular, poor awareness of the programme among providers and—as also observed in our study—beneficiaries.21
Altogether, these implementation dysfunctions were likely to account for a large part in the apparently poor results of the health dimension of the PNBSF programme on UHC, potentially more than the free health insurance per se. Thus, one should not wrongly conclude that it is the free health insurance system itself that is ineffective in improving health coverage.38
Nevertheless, it should be noted that our results indicate that benefiting from the free PNBSF CBHI enrolment was generally associated with being more socially vulnerable. PNBSF CBHI enrolees had social characteristics broadly similar to that of the rural indigent population in Burkina Faso,39 suggesting that the targeting was likely based on effective selection strategies.
Limited effects of the PNBSF free health insurance programme
Our results suggest that there was no effect of free health insurance on health service utilisation following a health problem, as also found in a randomised experiment among informal workers in urban Kenya.22 It is worth noticing that, in our study, the observed proportion of the population that reported a health problem was similar to that of a national-level study also conducted in 2019 in Senegal (ie, 23%).40 However, we observed a much lower proportion of the population that consulted in a health facility following a health problem (33% vs 61%), a gap that may be related to the high poverty rate in the rural area of Niakhar.
As regards maternal care, we found no effect of the programme on the number of antenatal care visits. We nonetheless found a significant effect of free health insurance on health facility deliveries (compared with home deliveries), which seemed to have been favoured by the free CBHI enrolment compared with not benefiting from any type of health insurance, yet with a lower magnitude than for voluntary CBHI enrolment. This is all the more important since health facility deliveries were shown to be associated with lower maternal and neonatal mortality,41 42 including in Senegal.43 Our results are in line with that of a study in Ghana and Rwanda,20 which found a much more consistent impact of free health insurance on facility-based delivery than on the use of antenatal care. The study in Tanzania, however, found no effect of free health insurance for poor pregnant women on maternal care utilisation.21 That being said, it should be noted that free or heavily subsidised health insurance programmes are highly context-specific, and comparisons should be made with an appropriate degree of caution.
As expected, the incidence of catastrophic health expenditures—which we estimated at 6.2% in the Niakhar area—was higher than the national-level estimate for the same year (ie, 1.1% in 2019, though with a more than three times higher risk in rural areas).40 Also at the national level in 2019, spending on medicines accounted for 52% of households’ out-of-pocket health expenditures.40 In this study, we found no effect of either free or paid health insurance on health-related financial risk protection measured by catastrophic health expenditures. This absence of effect might be related to the fact that the burden of health expenditure borne by households—mostly due to spending on medicines—remained high even after CBHI enrolment. Due to the regular shortages of medicines in public health facilities, CBHI organisations tend to further control prescriptions and restrict the list of medicines covered to remain financially sustainable.44 Also in line with our results, a study in Burkina Faso revealed that indigents had to pay a significant amount of out-of-pocket expenditure to receive supposedly free-of-charge health services at public health facilities.45
Commenting in detail on the results concerning voluntary CBHI enrolment is beyond the scope of the present study. Nevertheless, our results that suggest an overall positive effect on health service utilisation are in line with those from other studies in LMICs.9 13 The absence of health-related financial protection that we observed contrasts with other studies in LMICs that rather highlighted a protective effect,9 12 13 although it is not uncommon to find studies reporting no or even detrimental effect of voluntary health insurance on financial protection indicators.14 46 47
Study strengths and limitations
Our study is the first to analyse the effects of the free PNBSF-subsidised health insurance enrolment. Such studies were needed to inform policy.48 Furthermore, while studies often rely on only one dimension of UHC and only one outcome (a given type of health service or a given health-related expenditure), we estimated the effect of the free CBHI enrolment on the two dimensions of UHC and on different populations: (1) access to healthcare services (health facility consultations in case of a health problem, access to maternal health services and overall forgone medical consultation and treatment) and (2) health-related financial protection (catastrophic health expenditure). Considering both healthcare-seeking behaviours and out-of-pocket health expenditures is crucial when assessing the effect of health insurance, since, for example, a low incidence of catastrophic health expenditure may be due to better financial protection, but also to an unmet need for care.
Our main study limitation is the impossibility to account for supply-side factors influencing the capacity of the PNBSF programme to guarantee better access to health services and to better protect individuals or households against the financial risk associated with healthcare. Important factors may be the presence of financing shortfalls of the PNBSF programme, the lack of professionalisation of the Senegalese CBHI management,49 or the operational capacity of the CBHI organisations.50
Questions may be raised about considering the Niakhar area as being representative of rural Senegal. This area has a long research history of research activity, mostly in the social sciences and medical fields.23 The possible territorial heterogeneity in the implementation of the PNBSF programme also limits the generalisability of results.
From a statistical standpoint, a limitation is related to the potential risk of bias in the estimation of the effects of the free PNBSF-subsidised CBHI enrolment policy. Although we used the IPW method to address issues related to sample selection and stratification, and controlled for other observed factors that may have influenced each outcome, we cannot exclude a risk of omitted variable bias due to unobserved confounders, which is a common limitation. More generally, the cross-sectional nature of our data prevented us to estimate strictly causal effects of the free health insurance programme. Therefore, we acknowledge that estimated between-health insurance group differences may not be solely attributable to differences in health insurance status. Moreover, in the models of catastrophic health expenditure, we did not account for the potential endogeneity bias that may arise if the decision to seek care was correlated with the expected healthcare expenditure (ie, a potential selection bias due to care-seeking decisions).51
Conclusion
Overall, our study reveals the presence of dysfunctions at different levels, preventing an effective application of the PNBSF programme in terms of protection against the risk of forgoing healthcare and the financial risk related to healthcare in rural Senegal. Our results suggest that the limited effects of the free health insurance programme on health service utilisation and health-related financial protection were more likely due to implementation issues than to the provision of free health insurance per se. Nevertheless, although our results seem to point to a poor PNBSF implementation process, this ought to be investigated in an in-depth qualitative study, as was done for instance for the case of performance-based financing in Burkina Faso.36
Greater commitment from the State is needed to remove existing barriers—observed at different levels—to effective health coverage within the PNBSF programme, and thereby effectively reduce both the unmet need for healthcare and the health-related financial risk.
Encompassing better communication strategies within the health-related dimension of the PNBSF programme would narrow the gap between de jure eligibility to free health insurance and actual free enrolment in CBHI schemes. Then, among households/individuals aware of their eligibility to free health insurance, concomitant efforts should be made to remove supply-side and demand-side barriers to accessing covered health services. For example, there seems to be a challenge in combining the free health insurance programme with strategies to improve patient navigation and, thereby, overcome the barriers PNBSF beneficiaries face in accessing care. A recent review of patient navigation interventions in low-income countries highlighted that no intervention specifically targeted indigents.52
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The CMUtuelleS survey was approved by the Senegalese National Ethical Committee for Health Research (no 000037/MSAS/DPRS/CNERS and no 0000118/MSAS/DPRS/CNERS). Informed consent was obtained from all subjects. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank the study participants, the staff at the Niakhar Health and Demographic Surveillance System, and the members of the UNISSAHEL programme. A complete list of members of the UNISSAHEL Study Group is given in online supplemental appendix A1. We also thank Valéry Ridde and Bruno Ventelou for their useful comments and suggestions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Contributors M-QB: conceptualisation, supervision, methodology, formal analysis, investigation, visualisation, writing- original draft preparation, writing- review and editing. PD: Formal analysis, investigation, writing- review and editing. GàDT: formal analysis, investigation, writing- review and editing. J-YLH: conceptualisation, investigation, supervision, methodology, writing- review and editing. RL: funding acquisition, conceptualisation, investigation, project administration, supervision, methodology, writing- review and editing. All authors approved the final version of the manuscript for submission and agreed to be responsible for all aspects of the work.
Funding This research is part of the UNISSAHEL programme (Universal Health Coverage in Sahel), funded by the Agence Française de Développement (AFD).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.