Article Text

Abstract
This case study analyses a health project that focused on peacebuilding in addition to service provision, and the impacts of this dual focus in contested territories of Southeast Myanmar. The Swiss-funded Primary Health Care Project provided equal funds to both ‘sides’ in a decades-long conflict, and brought people together in ways designed to build trust. The case study demonstrates that health can play a valuable role in peace formation, if relationships are engineered in a politically sensitive way, at the right time. Whereas much of the literature on ‘health as a bridge to peace’ focuses on the apolitical in health, here the explicitly political approach and the deliberate adoption of neutrality as a tool for engaging with different parties were what enabled health to contribute to peace, using a political window of opportunity created by ceasefires and the beginnings of democratic transition in Myanmar. We argue that this approach was essential for health to contribute to bottom-up processes of peace formation—though the scope of the gains is necessarily limited. Crises like the COVID-19 pandemic and military coup in Myanmar can undermine the resilience and limit the impacts of such endeavours, yet there is reason to be hopeful about the small but significant contributions that can be made to peace through politically sensitive health projects.
- maternal health
- child health
- public health
- COVID-19
- health policy
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
In Southeast Myanmar, the Swiss-funded Primary Health Care Project provided equal funds to both ‘sides’ in a decades-long conflict, bringing people together in ways designed to build trust.
In-depth-interviews with health workers and other stakeholders suggest the explicitly political approach and adoption of neutrality as a tool for engaging with different parties enabled this project to contribute to peace, using a window of opportunity created by ceasefires and the beginnings of democratic transition in Myanmar.
Ties formed during the project between ethnic and government providers promoted resilience and helped to preserve gains in service delivery and referrals despite the sequential crises of the COVID pandemic and Myanmar military coup.
Though the scope of the gains is necessarily limited, the case study demonstrates that health can play a role in peace formation, if relationships are engineered in a politically sensitive way, at the right time.
Introduction
Proponents of ‘health as a bridge to peace’ commonly argue that health transcends political divisions, uniting opponents around shared goals. Collaboration through joint health activities can humanise the ‘enemy’ and build trust.1 Yet, health systems and service delivery are shaped by political factors and health programmes can become a domain of political contestation. In Southeast Myanmar, conflict and structural violence constrained access to state health services for many ethnic groups who came to rely on non-government systems affiliated with armed non-state actors,2 and attempts to reform health systems were deeply politicised. If health does not necessarily transcend politics, how can it become a ‘bridge to peace’?
In contested territories of Southeast Myanmar, the Primary Health Care Project (PHCP) funded by the Swiss Agency for Development and Cooperation (SDC) provided equal funds to both ‘sides’ in the conflict, bringing people together in ways designed to build trust. Together with the adoption of neutrality as a political tool, this enabled health to contribute to peace formation. Neutrality—the idea that humanitarian actors ‘may not take sides in hostilities or engage at any time in controversies of a political, racial, religious or ideological nature’3—is often interpreted as meaning that aid agencies must remain outside of political disputes. Yet, the PHCP adopted an approach to neutrality that meant not only engaging equally with both ‘sides’, but also encouraging project partners to recognise and grapple with this strategy’s political implications and outcomes. Drawing on a review of transcripts from interviews conducted in January–February 2019 with 48 non-government, government and international actors as part of research on ‘health as a bridge to peace’ (approved by the Office of Research Ethics and Integrity, the University of Melbourne), and of project documents, we analyse outcomes and challenges of the PHCP as a neutral, politically sensitive peacebuilding-through-health initiative.
Context: conflict, health systems and other international approaches
The Karen ethnic group was among the earliest to take up arms against the Myanmar (then Burma) government in 1949, and southeastern areas bordering Thailand where Karen comprise the majority of the population have endured fluctuating levels of conflict for over six decades.4–7 Large areas of Karen (Kayin) State remained outside of government control, and in the absence of national government services, the Karen National Union (KNU)—largest Ethnic Armed Organisation (EAO) in Karen State—and other local groups developed health systems in Karen communities. The Ethnic and Community-Based Health Organisations (ECBHOs) include Ethnic Health Organisations (EHOs) and Community-Based Health Organisations that often work in partnership with EHOs. Although not officially recognised in Myanmar and often targeted by the military, ECBHOs in KNU-controlled and mixed administration areas were the only trusted source of healthcare for many communities, receiving funding from major international donors throughout the 1990s–2000s.
From 2012, as military leaders issued rhetorical commitments to transition towards civilian rule, donors increasingly focused on building relationships with the Myanmar government. In this context arose the claim that continued support for ECBHOs could prolong conflict. In one study frequently cited by international donors and aid agencies, cross-border aid agencies (as ECBHOs and other groups using a management base in Thailand to support services in Myanmar were called) were described as ‘humanitarian wings of armed ethnic groups’, which ‘risk[ed] serving to legitimise the latter in the perception of recipients’, thereby fuelling conflict.8 In other words, looking specifically at health groups, this was an argument that health could be a barrier to peace. The perceived non-neutrality of ECBHOs became an articulated rationale that donors used to justify withholding or withdrawing funding from such groups and increasing funding for state-sanctioned approaches inside Myanmar.9 These approaches were, ironically, far from ‘neutral’ themselves. Considered in concert, they disproportionately favoured systems administered or sanctioned by the state.
Over the 4 years of Thein Sein’s quasi-civilian government in Myanmar, funding shifted away from the border and towards centralised mechanisms and state-sanctioned systems. A number of internationally funded programmes and projects were established that focused explicitly on building peace or social cohesion, and several education and livelihood projects embraced peace as a concurrent objective.
In the health sector, although major pooled funding mechanisms gave rhetorical support to peace promotion, they were headquartered in Yangon (former capital) and prioritised a model for development and peace led by the central government. This government-centred approach reflected the contemporary emphasis on liberal peace frameworks that prioritise state building, formal institutions, and elite-level processes and that have been criticised for potentially reinforcing systemic inequalities, denying self-determination, and bolstering anti-democratic processes in contested states like Myanmar.10 11 Such limitations call for alternative approaches that recognise non-state actors and attempt to address systemic inequalities.
The PHCP: window of opportunity and project novelty
The SDC prepared its PHCP in 2013 and 2014, launching it in 2015. As one SDC representative put it, it used the ‘window of opportunity’ provided by the 2012 preliminary ceasefire agreement between the KNU/Karen National Liberation Army and government to ‘[bring] together the different stakeholders which usually sit on the opposite side in the peace process’. After PHCP initiation, the 2015 Nationwide Ceasefire Arrangement, the National League for Democracy electoral victory and other peacebuilding programmes in Karen State further boosted confidence among project stakeholders and contributed to project feasibility.
To demonstrate donor neutrality and increase cooperation between implementing partners historically divided by conflict, SDC mandated equal funding (‘50:50’) for government and non-government actors, for the same objectives. SDC selected international non-governmental organisations (NGOs) to lead two consortia: Save the Children led a consortium of government service providers, and community-based and religious organisations; Community Partners International worked with a consortium of ECBHOs.
The PHCP began in May 2015 with an initial plan for an 8-year project period, through 2022. Like many projects funded by major bilateral donors in Myanmar, it supported universal healthcare (UHC) goals to deliver a basic package of health services to all township residents (figure 1). However, it differed from other health projects in three respects.

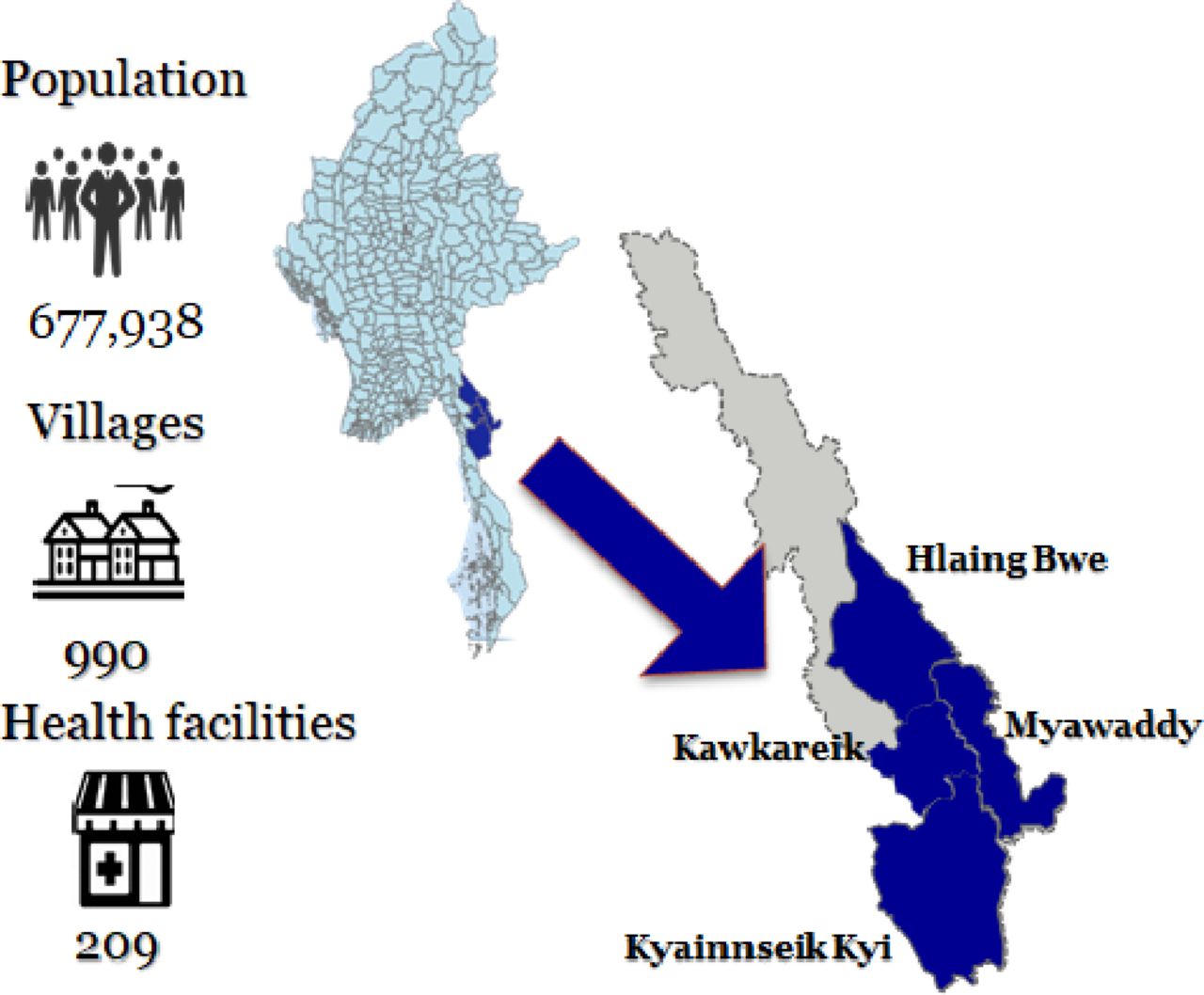{kind=link}
SDC Primary Health Care Project, key figures across consortia. SDC, Swiss Agency for Development and Cooperation.
First, it explicitly recognised both the government and ECBHOs as legitimate providers operating in a contested governance landscape, with intercalated services targeting a complex map of beneficiary villages. Second, the project sought to build trust between health workers and communities from opposite ‘sides’ of the conflict, working from the local level upwards. Third, the SDC supported a flexible budget line item that project partners could allocate to fund an evolving suite of ‘convergence’ activities.
Project outcomes: what worked and what did not
If health is a bridge to peace, then the SDC PHC project is the engineer. (interviewee, 2016 PHCP Midterm Review)
Engineering a bridge to peace
Project stakeholders explained that health could bring together actors from opposite ‘sides’ of the conflict around shared, apolitical goals, thereby ‘building trust, building social cohesion on the ground’. Yet, the project was far from the traditional model that considers health as a ‘bridge to peace’ because it somehow transcends politics.12 13 Although officially, many project actors verbalised that ‘health is not political’, few considered this to be the case.
For ECBHO members, ‘convergence’ with state health systems was linked with aspirations for self-determination and self-administration within a federal model. As one ECBHO member stated, “our convergence vision is based on our political goals.” Government health workers, in contrast, continued to operate within a highly centralised model, meaning that ‘as soon as EHOs are involved, it gets very politicised’—an SDC representative explained. Each aspect of coordination was therefore understood to be politically loaded, with this acknowledgement being vital to the project’s ability to build trust and achieve outcomes.
Political sensitivity was built into the project from the outset. For example, there was discussion about the 50:50 allocation of funds to both sides. ECBHOs argued that to achieve equity in outcomes (and not simply equality in funds disbursed), historically marginalised non-government groups should receive a disproportionate share of project funds. Although the 50:50 split was preserved, it nevertheless brought non-government service providers to the table on a more equal basis with government counterparts than would otherwise have been possible (and more than was possible in other donor-funded health programmes).
Peace formation outcomes
The project design and incorporation of joint planning promoted understanding, collaboration and trust. At first, there were disputes over which villages to include in respective government and non-government target areas. However, coverage maps were agreed to after 1 year—an allocation never reached elsewhere in the country, despite receiving priority under interim ceasefire frameworks. Initially, semiannual planning meetings were sparsely attended by both sides; by project year 3, the two consortia were able to meet for Coordinated Township Health Planning on a quarterly basis, and reported in a combined format.
Joint planning meetings paid for project partners to convene on a more level playing field and forge unprecedented relationships with counterparts on the ‘other side’ of the conflict. One ECBHO medic explained, “All are coming together, both sides, and joined the meeting. … We discussed about the project side, building relationship and cooperation.”
Relationships between government and non-government actors were also built at local levels through joint training, immunisation campaigns and study trips. In Kawkareik Township, for example, 31 ECBHO Maternal and Child Health workers (midwife-equivalent cadre for ECBHOs) were trained by the Ministry of Health and Sports (MoHS) in coordination with Community Partners International (CPI), International Rescue Committee and ECBHOs. This was the first joint training between the two ‘sides’ for this type of health worker. It enhanced acceptance of ECBHO skills by government actors, while building relationships and trust. Immunisation campaigns were also jointly planned by ECBHOs and government actors. In the 2018 Japanese encephalitis campaign, ECBHOs received transport funds from the MoHS for the first time. Finally, government and ECBHO staff felt that annual study trips to Switzerland afforded an informal means to get to know each other and, over time, build trust.
Multiple stakeholders identified the establishment of patient referral networks linking non-state and state systems as one of the most meaningful project impacts, both in terms of health outcomes and the development of relationships. Although ECBHO clinics could handle presentations of common illnesses, complex cases required referral to a higher level of care. Before the project start, CPI estimated that around 70% of ECBHO referrals were to the Thai side of the border, with only 30% going to Myanmar government facilities. By 2019, 59% of referrals went to government facilities (this proportion continued to increase during COVID-19 as travel restrictions reduced international referrals to Thailand). This shift suggests increased trust in government facilities among ECBHO patients and staff. ECBHO staff perceived positive synergies between better coordinated referral systems and the understanding developed through PHCP activities:
At the beginning, when we came to be based here, we had difficulties in referring patients to the Kawkareik Hospital because [government staff] don’t recognise us and they said we are just curing the patients without guidelines. … There are less complaints coming from the hospital after SDC project implemented.
On the national policy level, SDC leveraged its position as a major bilateral donor to advocate, alongside CPI, for EHOs’ inclusion in the National Health Plan (NHP) forged by the National League for Democracy in 2016. The NHP’s development was ‘a uniquely inclusive process in the context of Myanmar, as the committee for developing the NHP included government officials as well as representatives from civil society and EHOs’.14 In the resulting plan, EHOs were mentioned 34 times and acknowledged as ‘service providers’ in Myanmar’s ‘ethnic’ areas.15 This highlights the government’s recognition that UHC, which the plan aimed to achieve by 2030, necessitated collaboration with EHOs.
Challenges and limitations
Stakeholders highlighted flexibility as key to the project’s peacebuilding aims. Rather than assigning fixed annual targets listed in logframes that rapidly became antiquated in a constantly shifting environment, the flexible line item dedicated to ‘convergence’ activities allowed consortia to target areas where cooperation was possible. This flexibility may reflect why such schemes are rare. The SDC project trades the typical donor emphasis on readily quantifiable annual process and impact indicators for less easily measured results that accrue over longer time frames. It demonstrates the feasibility of a flexible model managed by one donor for a fraction of its funds; however, a more substantial shift in priorities is likely necessary to be embraced at scale by a pooled bilateral fund or the Global Fund.
Additionally, the project’s aims were inevitably limited in terms of peacebuilding. For one, the joint planning meetings described above were not a panacea. Based on the Township Health Working Group model established in the NHP, they were perceived to give greater power to government over non-government actors. Furthermore, the rapid turnover of government staff undermined the ability to nourish personal relationships on which trust is built. ECBHO members lamented that ‘we have to build the relationship, again and again’ and speculated that this turnover was a legacy of previous military government strategies to maintain divisions between ‘us’ and ‘them’.
Actors at all project levels recognised that wider peace depended on actors and forces beyond their control. Nevertheless, local-level health workers are vital community members who may determine social cohesion within a village or township. Although health programmes may not produce nationwide political breakthroughs, they can contribute to bottom-up processes of peace formation,11 with the everyday diplomacy16 engineered through the PHCP building bridges between groups divided by conflict and contributing to a culture conducive to peace at a local level. Targeting the community level, however, leaves a project exposed to winds of change blown from the capital city and headquarters of armed organisations that may shift the terms of cooperation quickly. This may always be the case for health projects aiming to build peace, but is worth acknowledging. Health alone is unlikely to redress a century of history or to guard against a unilateral seizure of power by a military dissatisfied with election results.
Resilience in times of crisis: COVID-19 and the 2021 military coup
In the last year, two crises have rocked Myanmar and this project: the global SARS-CoV-2 pandemic and the military coup. COVID-19 strained health services to the breaking point, and the coup rekindled active fighting between the Myanmar junta and ethnic Karen forces—with further limitations and successes of the PHCP highlighted by these external crises.
COVID-19 offered a test for the cooperation built between ECBHOs and government health services. However, the severity of the health challenge may have prevented the project’s gains from having significant impacts. Even before the coup, COVID-19 responses were escalated right to the top of government, to the State Counsellor and EAO leaders. Policy decisions related to travel restrictions, quarantine and isolation were made by state and non-state authorities, not the health sector. Joint planning meetings and training were stalled and travel restrictions created barriers to referral. Arguably this is not unique to Myanmar—across the world, many heads of state orchestrated COVID-19 responses with relatively little regard for public health expertise, and in many countries the risk of COVID-19-related mortality was decoupled from the overall strength of health systems.
The 2021 military coup struck a second blow to the PHCP, which now looks unlikely to persist in its previous form. Most ECBHOs remain reluctant to engage with the junta, and many government clinicians have participated in the national Civil Disobedience Movement (CDM). Faced with the option of working for a government they did not vote for, many left their positions, with MoHS clinics and township health departments much depleted. To date, few donors and international NGOs have cooperated with the junta.
Despite these challenges, the PHCP’s 7-year (to date) investment in peace continues to yield positive impacts. For one, SDC support further strengthened ECBHO systems, contributing to their continued operation in the acute-on-chronic crisis. ECBHO resilience is evident in their successful referral of 463 emergency cases in 2020, the most referrals of any year to date and more than twice as many cases as in 2016.
Moreover, relationships created through a shared desire to serve local communities have survived and thrived since the coup. Clinicians participating in the CDM are considered enemies of the junta,17 and many have fled for their lives. Many have turned to former PHCP colleagues for protection; some are now working scalpel-to-scalpel with ECBHO colleagues to deliver health services within Myanmar’s current political and humanitarian emergency. Among these ECBHO and (former) government staff, health has served as a bridge to peace, forging solidarity amidst surrounding political upheaval and armed conflict.
Conclusion
The PHCP demonstrates that health can play a role in building peace, when relationships are cultivated with political sensitivity. The project’s success was linked to its embrace of an approach to neutrality which entailed equal engagement with both ‘sides’ of the conflict and which explicitly supported activities that acknowledged and accounted for political implications and outcomes of this strategy. The ‘window of opportunity’ created by ceasefires and the beginnings of democratic transition in Myanmar contributed to the project’s feasibility—highlighting the need to consider contextual factors. Limitations to peacebuilding outcomes as well as generalisability show that it is important not to overstate possible impacts of such projects. Despite these caveats, the PHCP demonstrates that health can play a valuable role in peace formation, if relationships are engineered in a politically sensitive way, at opportune times. Politically sensitive health programming alone may not produce nationwide peace, but it can build bridges at the community level, which are essential for long-term peacebuilding.
Politically sensitive engineering is especially important in situations where health workers operate in a context shaped by profound structural inequalities. Within unequal playing fields, it is difficult for health interventions to contribute to peace.1 3 This case study demonstrates how, through careful engineering and with international actors using the leverage that their funding affords, the playing field can to some extent be levelled (at least within a health project and although imperfectly), creating a situation more conducive to health contributing to peace. And while we must remain humble about their potential outcomes, we can nevertheless be hopeful about the small but significant steps that politically sensitive health projects can make in contributing to bottom-up processes of peace formation.
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Office of Research Ethics and Integrity (University of Melbourne 1853127.1). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the PHCP partners and other stakeholders who shared their candid perspectives on convergence during interviews in 2019, and the SDC staff and ECBHO leaders who provided constructive comments on a draft manuscript.
Footnotes
Handling editor Seye Abimbola
Twitter @tom_traill
Contributors AD and TT contributed equally to this paper and jointly serve as guarantors: they accept full responsibility for the work, had access to the data, and controlled the decision to publish. AD and TT jointly conceived the study design, conducted and analysed the interviews, reviewed project documents, and drafted and edited the manuscript. ST shaped the study design and critically reviewed the manuscript. AR conceived the study design, reviewed project documents, and critically reviewed and edited the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests AR is Senior Technical Advisor and a Member of the Board of Directors of Community Partners International (CPI). He did not receive any compensation in relation to this manuscript. ST and TT are employees of CPI.
Provenance and peer review Not commissioned; externally peer reviewed.