Article Text

Statistics from Altmetric.com
Summary box
Libya has experienced decades of armed conflict and political instability.
Non-communicable diseases (NCDs) are particularly vulnerable to long-term disruptions in health services and policymaking processes.
Conflict indirectly drives the escalating burden of NCDs, which can stoke civic unrest and propagate further violence and political instability.
This reciprocal of this vicious feedback loop has been demonstrated by sustained NCD policymaking efforts spanning political factions.
Recent data collection, health service reform and NCD guideline development activities that have served East and West populations without distinction are contributing to the building of a collective civic identity.
The stability and cooperation fostered by these activities could potentially help to build small but important bridges towards peace; however, we do not have sufficient evidence to confirm a causative association.
Introduction: conflict, peace and health
It has been argued that peace and its reciprocal—conflict—are macrodeterminants of health. Nowhere has experienced greater conflict than the Middle East in recent decades.1–3 The experience of Libya offers potent lessons on the bidirectional relationship between peace and health that extend beyond the immediate violence-related health impacts of civil war.
Context: Libya’s political instability
Since the toppling of Muammar Ghaddafi in 2011, numerous political factions have vied to exert control, often backed by competing foreign nations with clashing interests over oil, regional influence and migration. International agencies have largely been working with two competing governments based in Benghazi and Tripoli, respectively. In March 2021, a new Government of National Unity was formed through a UN facilitated process, and formal elections are slated for l2022. The UN Human Rights council estimates that 10 000–15 000 people died in the civil war between 15 February and 9 June 2011,4 and the Global Burden of Disease Collaborative Network estimate that a further 11 355 people have been killed by fighting in the last decade.1
We are a group of World Bank health specialists and Libyan policymakers who are working together to bolster Libya’s national response to non-communicable diseases (NCDs). These conditions account for over 80% of all deaths in Libya and 78% of disability-adjusted life years.5 We have been focusing on the 12 WHO-recommended NCD ‘best buy’ policies (summarised in the online supplemental appendix) that include tobacco and alcohol taxation, reformulation of trans and saturated fats, child junk food marketing regulations and basic medicines for cardiovascular diseases.6 These highly cost-effective, population-level policies were unanimously endorsed by all WHO Member States in 20137 and again in 2017 at the World Health Assembly.6 Recent work has shown that countries based in the African continent are among the least likely to have implemented the NCD best buys.8 Libya has only implemented five of these 12 policies, placing it in the bottom third of all countries.9 Libya has yet to implement a multisectoral action plan or national targets. A number of nascent cross-departmental NCD policies are in development, but they cannot progress until a legitimate deliberative body, elected with an appropriate mandate, officially endorses these activities and releases the required resources. Libya is unusual in that big tobacco, big food and big alcohol are not major barriers to policy implementation. Almost all tobacco products are produced illegally and sold on the black market; alcohol is illegal; and the lack of credible food reform has led major manufacturers to largely ignore the country.
Supplemental material
In the course of our collaboration, we have performed literature reviews, analysed domestic policy documents and interviewed a range of government policymakers in order to understand how Libya can move forward to implement more of these life-saving policies. Several themes have emerged around the direct and indirect impact of conflict on NCDs.
Conflict as an indirect driver of morbidity and mortality
Peace is identified as the initial ‘fundamental condition’ for health in the Ottawa Charter,10 and Levy11 has argued that ‘without peace, there can be no health’. Conflict and the absence of peace are intuitively associated with violent deaths, and Libya provides ample evidence for the direct impact of fighting on human lives. The quarterly civilian casualty report from the UN Support Mission in Libya enumerates five different categories of mortality: improvised explosive devices, targeted killings, airstrikes, small arms and heavy weapons.12
However, conflict can also lead to great harm long before and after physical violence, creating divisions that undermine political solidarity, governmental legitimacy and authority.11 Conflict also indirectly damages health through disruptions to supply lines, human resources deployment, fractured financing and the provision of healthcare services,13 and all of these outcomes have been directly observed in Libya.14 15 Approximately one-third of Libyan primary health facilities have been destroyed in fighting,16 and ongoing hostilities frustrate the country’s ability to train and deploy doctors, nurses and allied health staff with geographic equity.17 Libya’s gross domestic product (GDP) fell by two-thirds in the five years following 2011 and has still not recovered.18 Disruptions to state oil production; a fractured economy; and the emergence of multiple overlapping authorities constrain the nation’s ability to finance and run a functioning public health system. A recent survey of Libya’s health worker diaspora showed that economic collapse brought about by the conflict was the main reason for emigration and that health system reform is the most important factor for inducing future return.19 There are no estimates for the epidemiological burden stemming from the indirect impact of conflict, but Libya’s health performance indicators are far below what would be expected for an upper-middle income country with such a well-educated population.
The unique relationship between conflict, peace and NCDs
While infections, maternal and neonatal care, and nutritional health problems all require functioning health systems, chronic diseases are acutely vulnerable to disruption.20 The long-term management of diabetes, cancers, chronic lung disease and cardiovascular diseases requires special attention to coordinated and longitudinal care. As NCDs are driven by upstream economic and political conditions, housing, education, transport, food, international trade policy, etc, the effective prevention and control of these conditions is dependent on a health in all policies approach, led by multisectoral committees at the highest levels of (functioning) government.21 22 WHO places great emphasis on the importance of convening stakeholders from different areas of government to develop and implement national NCD strategies23 24 and monitors progress in this area for all 194 Member States.9
Through our work, we have found that one of the most commonly reported barriers to tackling NCDs in Libya is the inability to pass policies and regulations at the national level. During a decade of conflict, there has not been a single, unified deliberative body either in existence or that possesses the legislative capacity to address NCDs. High morbidity and mortality rates, ballooning levels of obesity, a booming tobacco black market and unregulated junk food sales and marketing are no secret,5 25 but these significant health problems have—understandably—not been prioritised by successive short-lived governments. This legislative lapidification has forced NCD departments to focus on less impactful ‘downstream’ service delivery strategies and small-scale public awareness and education interventions.
Even if national NCD policies—such as tobacco taxes—were to be endorsed by a legislative body, conflict and instability also present major barriers to implementation and enforcement. As things currently stand, the interim government is working to develop a multisectoral committee to draw up targets and a national strategy; however, even this endeavour has been undermined by the disruption to national surveillance efforts, including a planned second WHO NCD ‘STEPS’ survey. Reinstating disease monitoring systems and epidemiological surveys is essential for understanding the baseline risk profile and epidemiological burden faced by contemporary Libyan society.
The cycle of conflict
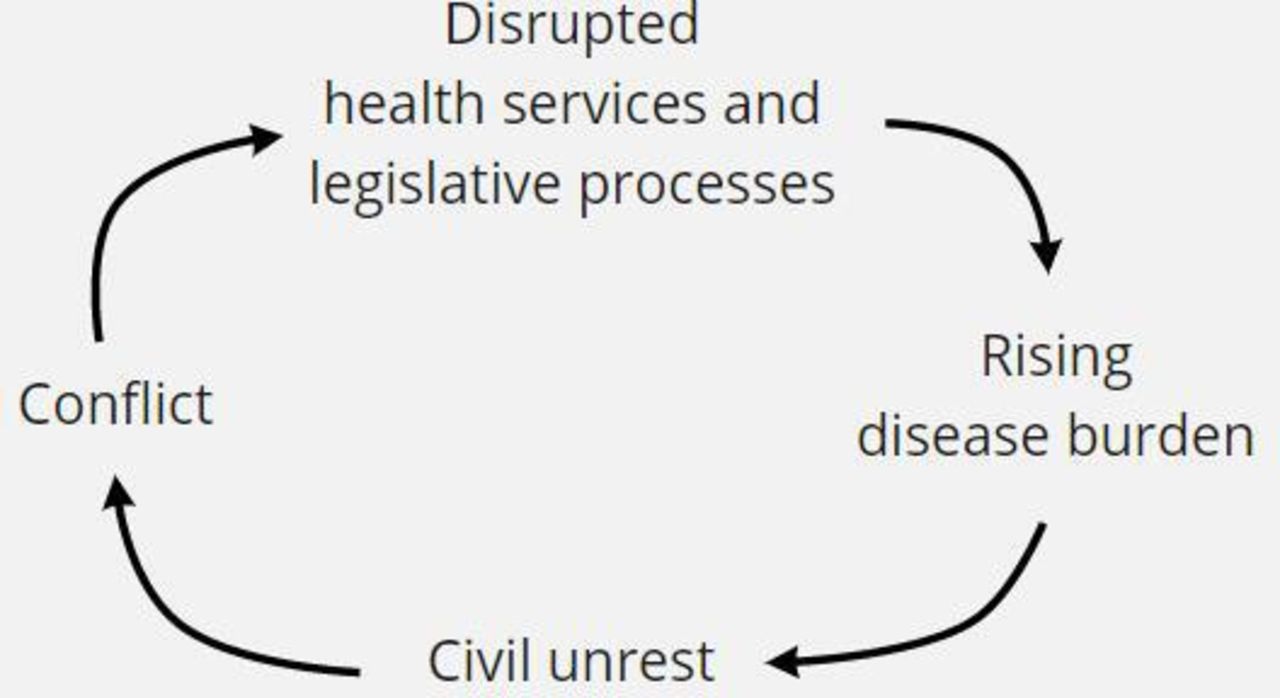
The relationship between conflict and health service disruption in Libya’s experience can be examined using system thinking.26 Building on the work of Yusuf et al27 and Arya28 in 2004, Santa-Barbara and MacQueen29 presented a cyclical conflict model that illustrates the phases of war and opportunities for prevention, built around a reinforcing feedback loop. They identify public grievances as a key driver of the cycle of violence and argue that it can be broken with ‘primordial prevention’27 efforts. Poor health has long been identified as an important grievance that can stoke civil unrest and subsequent violence, acting both as an important issue in itself and as a marker for other grievances such as human rights abuses and inequitable resource allocation.11 30 Although we do not have direct evidence that the rising NCD burden is directly stoking civil unrest in Libya, previous research has found that the rising incidence of various diseases is strongly associated with the risk of a country becoming engaged in armed conflict.28 31 32 Based on our experience, we postulate that weak, unequal and inadequate NCD policies and service delivery has contributed to the rapid rise in NCD morbidity and mortality. We also believe that patients and the general population perceive government action to be inadequate and that this represents a public grievance that contributes to civil unrest. Decades of experience from other fragile settings shows that a rising burden of preventable disease can undermine state legitimacy,33 34 and this can seed the conditions for further conflict and political instability.35 We have already seen that conflict and political discontinuity undermines health services and obstructs the passing of health policy. As the burden of NCDs rises, the health-related cost of conflict continues to rise. This can lead to a reinforcing feedback loop (figure 1), which must be broken.

{kind=link}
A simplified reinforcing feedback loop between conflict and non-communicable diseases.
Breaking the cycle
This special issue highlights how health can build bridges towards peace. Libya’s experience provides case study level evidence for the reverse; how conflict, political instability and fragmented governance can directly and indirectly impede progress in tackling a country’s most pressing disease burden. We also argue that conflict and NCDs can become self-sustaining, via health service disruption and civil unrest. The issues that we have documented in Libya are generalisable to other settings where conflict and the absence of peace undermine the ability of national authorities to develop, approve, implement and enforce effective health policies.
In 2000, MacQueen and Santa-Barbara identified five mechanisms through which health workers can build peace; conflict management (via medical diplomacy); solidarity (supporting those working to build peace); strengthening the social fabric (using healthcare delivery to serve diverse groups); dissent; and restricting the destructiveness of war.36 Our work on NCD policymaking has provided several examples of how health workers contribute to strengthening the social fabric by working with and providing services to East and West populations, irrespective of ethnicity, ideology or any other sociodemographic characteristic.
First, the National Centre for Disease Control’s office for NCDs have continued to produce national reports and guidance for the East and West governments throughout the past decade. Second, their epidemiological reports are based on intelligence from primary care centres located throughout the entire country, serving all population groups. Third, efforts to reform the primary care-based NCD health service delivery system have been based on a commitment to serving all Libyans, and fourth, the development of new national NCD guidelines have been drawn up with broad representation from across the East and West. These policy decisions contribute to the building of a ‘collective civic identity’29 and have been further supported by non-state actors operating within the health system: WHO have convened numerous health system workshops that engage representatives from East and West, as well as international and national stakeholders that work to provide services across the country. Aiming to sustain continuity in the leadership and human resources of the national Centre for Disease Control (CDC) and NCD Office is an excellent starting point for the Government of National Unity. The existence of health departments that serve the entire country supports unifying peace-building efforts around a common objective. Health investments that distribute benefits among competing actors is a relatively low-hanging fruit that can foster broader, multisectoral cooperation in the longer term.
United against a common enemy
Libya’s security concerns and interrelated short-term humanitarian crises leave little room for the slow-motion disaster of rising NCDs on the legislative agenda. However, tackling NCDs provides a precious opportunity for unification around a common cause, potentially uniting disparate factions against a common enemy. The statecraft required to tackle NCDs makes these conditions especially vulnerable to conflict, but by the same token, the requirement for coordinated and cohesive governance may also provide a rallying point for the building of stable governance and a more enduring peace.
Given that addressing NCDs is a strategically important but long-term process, the government has been looking for ‘quick wins’ by identifying maximum-yield NCD interventions. Our current work is part of a broader support package that includes providing analytical and advisory support to develop institutional capacity for data analysis, policymaking, implementation, enforcement and service delivery for NCDs, complementing ongoing efforts by WHO and other development partners. Ongoing cross-party efforts to develop and deliver population-wide services can continue to make a modest but important contribution towards rebuilding a united state. There are potent similarities with NCD prevention in that peacebuilding is necessarily a ‘multi-level’ and ‘whole of society’ endeavour.29 37 38
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @drlukeallen, @Giulia_Loff
Contributors LNA conceived the piece and wrote the first draft. All other authors provided conceptual contributions and revised subsequent drafts of the manuscript.
Funding This study was funded by World Bank Group.
Competing interests MA and HE work at the Libyan Centre for Disease Control.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.