Article Text

Statistics from Altmetric.com
Summary box
While responding to the COVID-19 pandemic, other high-impact respiratory viruses with epidemic or pandemic potential such as influenza and the Middle East Respiratory Syndrome Coronavirus (MERS-CoV) were left ‘unattended’ in many settings, including in the WHO Eastern Mediterranean Region.
Integrated surveillance of high-impact respiratory viruses using (influenza) sentinel surveillance has the advantage to optimise the use of material and human resources for multiple viruses, hence maximising efficiency and sustainability and fostering preparedness for future pandemics.
Advocacy and technical guidance are needed to foster recognition by public health authorities of the essential role of sentinel surveillance for influenza and other high-impact respiratory viruses in anticipation of the emergence of a new pandemic virus.
Whereas the occurrence of future pandemics or epidemics caused by emerging or re-emerging high-impact respiratory viruses is virtually inevitable, the causal agent remains hard to predict. The COVID-19 pandemic has exposed the weaknesses to respond effectively to the emergence of a new viral pandemic threat. To prevent the next pandemic a formal global viral surveillance network which is agnostic of the pathogen and fosters greater use of multisectoral approaches to deal with emerging and re-emerging respiratory viruses is needed.1 Such a formal network, although new, would build on existing platforms and ‘leverage systems and capacities that are already operational’.1
Undoubtedly, the COVID-19 pandemic response already leveraged existing epidemic and pandemic preparedness capacity built for other high-impact respiratory viruses. For instance, influenza has served as a model pathogen against which countries have developed, tested, and sustained capacities for epidemic and pandemic preparedness.
Nonetheless, the COVID-19 pandemic response also negatively impacted the performance of existing surveillance and associated response systems for other pathogens with epidemic and pandemic potential. This negative impact was particularly severe in, but not limited to, resource-limited settings, including countries in the Eastern Mediterranean Region (EMR).
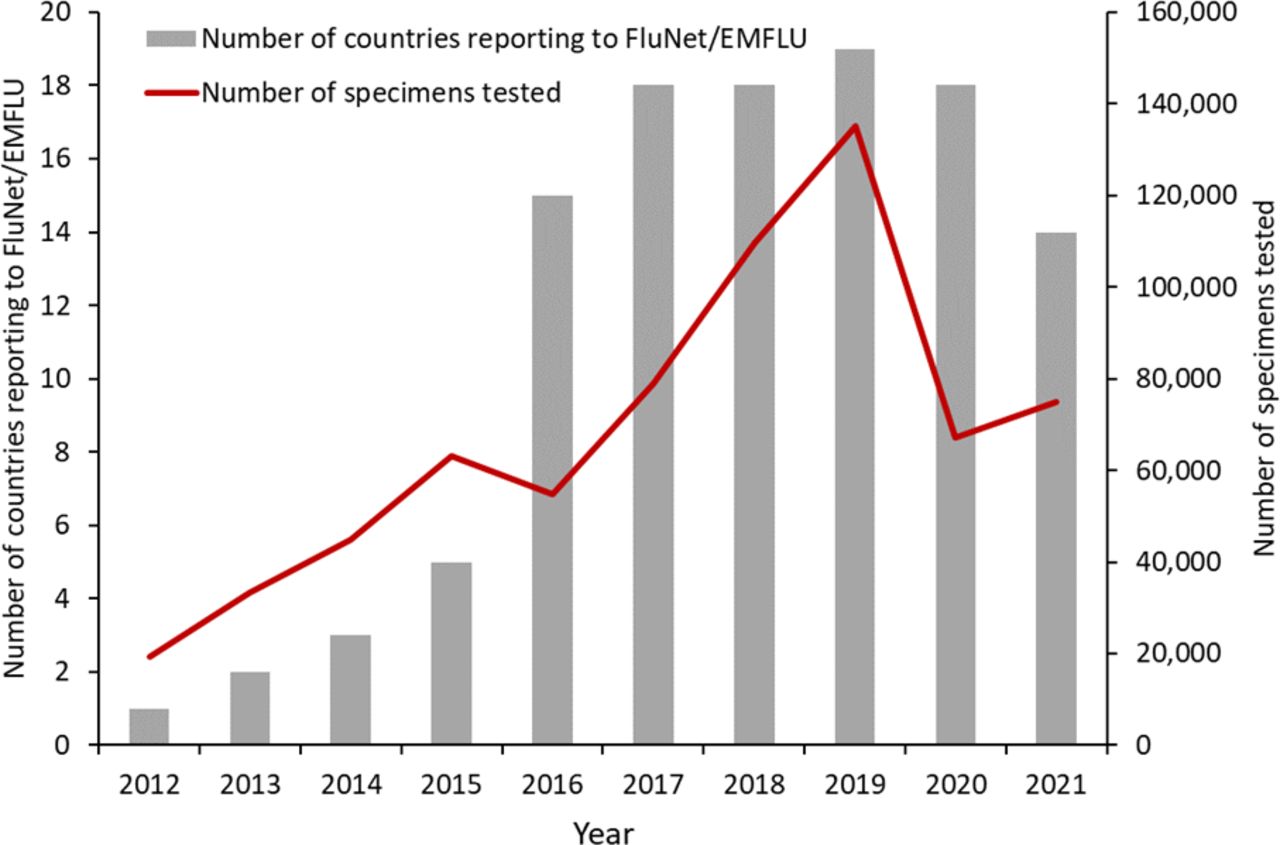
In the EMR for instance, prior to the COVID-19 pandemic the capacity for influenza sentinel surveillance grew steadily over the years, resulting in 19 out of 22 countries having functioning influenza surveillance systems and reporting influenza data to the Global Influenza Surveillance and Response System (GISRS) (figure 1). However, the established and functioning influenza surveillance systems have been impacted during the COVID-19 epidemic, resulting in a substantial decline of samples collected and tested during 2020–2021 (figure 1). A similar situation was observed for the Middle East Respiratory Syndrome Coronavirus (MERS-CoV) surveillance. The mean annual number of laboratory-confirmed MERS-CoV cases in the EMR declined from 271 during 2015–2019 to 39 (86% reduction) during 2020–2021.2 De facto, while responding to the COVID-19 pandemic other high-impact respiratory pathogens with known epidemic or pandemic potential were left ‘unattended’ or were at least partially neglected in many settings, including in the Eastern Mediterranean countries.

{kind=link}
Number of influenza specimens tested and reported to FluNet/EMFLU (World Health Organisation global and Eastern Mediterranean Region influenza reporting platforms) and number of reporting countries (n=22) in the Eastern Mediterranean Region, 2012–2021.
Especially in resource-limited settings, the disruption of sentinel surveillance activities for influenza and other high-impact respiratory viruses has been largely attributed to the need to redirect limited human and financial resources and infrastructures to the COVID-19 pandemic response. One of the lessons learnt during the pandemic is the importance of expanding the scope of the influenza sentinel surveillance systems to detect and monitor other respiratory viruses with epidemic and pandemic potential using integrated surveillance approaches.
The use of influenza surveillance to monitor other respiratory viruses with epidemic potential is not new. For instance, WHO-led pilot studies for respiratory syncytial virus surveillance nested within existing influenza sentinel surveillance systems have been ongoing for a number of years, including in five countries in the EMR.3 4 In addition, surveillance for multiple respiratory viruses within the influenza sentinel surveillance systems has been successfully implemented in different parts of the world.5–8 At the time of writing, the WHO GISRS+ platform is being conceptualised for the integration of surveillance for influenza and other respiratory viruses with epidemic and pandemic potential within existing sentinel surveillance networks, with priority initially given to the integration of influenza and SARS-CoV-2 surveillance.9 10 The selection of additional viruses for integrated surveillance is not fully defined and may vary across regions and countries within regions.
Globally, during the past 20 years, a number of high-impact respiratory pathogens affecting humans have emerged or re-emerged, including several zoonotic influenza A viruses such as influenza A(H5N1) in 2003; the pandemic influenza subtype A(H1N1)pdm09 in 2009 and influenza A(H7N9) in 2013 as well as three novel zoonotic coronaviruses, namely the SARS coronavirus in 2003; MERS-CoV in 2012; and the pandemic SARS-CoV-2 in 2019. In the EMR, highly pathogenic avian influenza A(H5N1) and A(H9N2) as well as MERS-CoV are endemic in the susceptible animal population and have caused sporadic human infections and outbreaks for decades.11 Novel influenza viruses and coronaviruses have proven capability to cause large epidemics or, even more importantly, pandemics and, as such, they warrant dedicated attention.
Whereas an integrated surveillance for high-impact respiratory viruses is one of several components needed for effective pandemic preparedness and response, it is both a necessity for and an enabler of epidemic and pandemic preparedness in the EMR; a region where several countries have been affected by ongoing protracted conflict and political instability that resulted in chronic weaknesses in health systems, including poorly functional disease surveillance.
Khan et al in their commentary on ‘Preparing for future pandemics in the Eastern Mediterranean region’ highlighted that ‘pandemic preparedness is political, resource intensive, and highly contextual’ and that, as a corollary in the context of the EMR, the following elements are pivotal to better prepare for future pandemics: (1) Strengthening leadership capacity in evidence-driven decision-making; (2) Sustaining commitment by the national authorities and the international community on building and maintaining functional health systems, especially in conflict affected countries; and (3) Voicing the perspective and the necessities of Eastern Mediterranean countries, particularly those affected by conflict, in the context of the new pandemic framework convention.12
The establishment or strengthening of integrated surveillance for high-impact respiratory viruses in the EMR has a role to play in achieving all identified pivotal pandemic preparedness elements by (1) Providing ongoing evidence to leadership for better decisionmaking, (2) Substantiating needs to foster commitment by national authorities and the international community to build and/or maintain health systems based on measured public health burden of high-impact respiratory viruses, and (3) Generating evidence for context-specific epidemic and pandemic preparedness needs.
In addition to the establishment of adequately resourced systems, communication and advocacy are needed to foster recognition by public health authorities of the essential role of sentinel surveillance systems for influenza and other high-impact respiratory viruses in the event of the emergence of a new pandemic virus. Such recognition would assist to prevent the negative impact on the existing epidemic and pandemic surveillance systems during the next pandemic as observed during the COVID-19 pandemic in several settings, including that in the EMR.
We consider integrated surveillance of influenza and other respiratory viruses with epidemic and pandemic potential as a necessity for better epidemic and pandemic preparedness in the EMR. As such, at the time of writing, efforts are ongoing by the WHO Regional Office of the Eastern Mediterranean to develop a framework, with inputs from Member States and stakeholders, built on the GISRS+ ambitions and to promote governance and leadership commitment for integrated surveillance of high-impact respiratory viruses in the Region.
Data availability statement
Data are available in a public, open access repository.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Handling editor Seye Abimbola
Contributors ST and WK conceived the study. ST drafted the manuscript. All coauthors provided critical review. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.