Article Text

Abstract
Social media platforms are a massive source of information being used for monitoring and detecting various actual events such as natural disasters and disease outbreaks. This paper aims to present the experience of WHO, Regional Office for the Eastern Mediterranean in using social media for the detection and monitoring of COVD-19 pandemic alongside the other event-based surveillance tools. Over the period of 29 January 2020 to 31 May 2021, information was collected from social media and other media outlets (web news) as being the source of health information for early detecting and monitoring the situation of COVID-19 events. Signals were categorised into new events and event updates; where event updates captured from social media were categorised into official and unofficial. A total of 10 160 COVID-19 information were captured, out of which 95.8% (n=9732) were detected through social media. None of the information captured were discarded. 50.0% (n=11) of the COVID-19 events in the Eastern Mediterranean Region (EMR) were primarily captured from social media compared with 4.5% (n=1) primarily captured from other media outlets. Almost all (99.4%) of the event updates captured from social media were official updates. Real-time, transparent and relevant information posted on different social media platforms, especially the governmental official social media accounts, strengthened the early detection and follow-up of public health events in the EMR, especially during the current COVID-19 pandemic.
- COVID-19
Data availability statement
Data are available in a public, open access repository. Data are public and available on Twitter and Facebook.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
During the past few years, social media platforms have evolved to act as good communication channels that help every user connect, interact, share content and communicate with the globe.
With the emergence of the COVID-19 pandemic and the strict public health measures isolating everyone, social media provided the public health professionals the opportunity to get public health intelligence information from everywhere, even from remote and less accessible locations.
This article shares insights on the ability of different social media platforms to become a reliable and fast source of health-related information through a retrospective analysis of the information on COVID-19 collected at WHO Regional Office for the Eastern Mediterranean through internet media scanning between 29 January 2020 and 31 May 2021.
These insights include the potential use of social media in building a two-way dialogue between governments and the public to gain trust and communication messages, the integration of social media and other innovative and artificially intelligent tools for public health surveillance, and the need for further studies on the timeliness of social media detection in comparison to other sources of information.
Introduction
Coronavirus disease (COVID-19) is an infectious disease that is caused by the SARS-CoV-2 virus. On 31 December 2019, the WHO was informed of cases of pneumonia of unknown aetiology detected in Wuhan City, Hubei Province of China. On 07 January 2020, the Chinese authorities reported that the cases were due to a new type of coronavirus, and on 12 January 2020, they shared with the WHO the genetic sequence of the novel coronavirus (2019-nCoV). On 13 January 2020, the first exported case of laboratory-confirmed novel coronavirus was reported in Thailand and other countries started to report the importation of laboratory-confirmed cases.1 On 29 January 2020, the first imported cases in the Eastern Mediterranean Region (EMR) were reported by the UAE.2 On 30 January 2020, WHO declared the outbreak to be a public health emergency of international concern.3 On 11 February 2020, WHO announced ‘COVID-19’ as the name of this new disease,4 and on 11 March 2020, WHO characterised the COVID-19 epidemic as a pandemic.5 On 31 December 2020, the WHO approved on the emergency use of the COVID-19 messenger RNA vaccine.6 As of 31 May 2021, the cumulative number of confirmed cases reported globally reached nearly 197 million and the number of cumulative deaths has reached 3.5 million.7
Public health surveillance systems mainly rely on information that is collected and analysed using predefined case definitions by well-known sources such as health facilities which is known as indicator-based surveillance (IBS). With the increase of the vulnerability to high impact and fast-spreading outbreaks, event-based surveillance (EBS) was introduced to complement the IBS as it considers primarily unstructured, ad hoc information provided by a broader range of sources of information that can be external to the health system. Indeed, EBS includes all potentially relevant reporting sources such as communities, animal health or media.8 EBS is not based on the routine collection of data but rather on unstructured narrative descriptions and reports including media reports where, media scanning is an important source of information for EBS.9 10
In 2017, in coordination with WHO Headquarters and other WHO Regional Offices, WHO Regional Office for the Eastern Mediterranean (EMRO) has implemented the epidemic intelligence (EI) process that permits the early detection and the monitoring of public health events occurring in the region. The process is as follows: a daily triage takes place to decide if the information collected, either through IBS or EBS, is related to a situation representing a potential acute risk to human health, and therefore considered as a signal. After the verification process, the signal is either discarded or considered as an event, if it is a manifestation of a disease or an occurrence that creates a potential for disease as defined by the International Health Regulations (IHR). An event is considered to be risk assessed through a systematic process to assign a level of risk to human health. Risk assessment becomes a continuous process starting from the detection of the signal until the response to the event (see figure 1).8


Epidemic intelligence process.8 *Actions is related to the type of the event where its main purpose is to minimise and control any negative impact that might occur due to an event. The actions taken in an acute public health event is different from the ones taken in case of outbreaks of communicable diseases or an acute public health event of non-human health origins as epizootics, chemical, radiological accidents or natural disasters.8 EBS, event-based surveillance; EWAR, early warning, alert and response; IBS, indicator-based surveillance; IHR, International Health Regulations 2005.
Electronic means were introduced as complementary to other traditional data sources to ease the process of collection of health information from different sources mainly to support in the early identification of any event that might have an acute impact on public health.11 Information is actively searched in media are available on the internet. To automatise and improve the performance of the internet media scanning, WHO in collaboration with various public health stakeholders around the globe has developed, in 2017, the Epidemic Intelligence from Open Sources (EIOS) platform.12 EIOS complemented the use of other existing aggregator systems such as Global Public Health Intelligence Network (the first news aggregator used for public health intelligence in 1997),13 ProMED-mail,14 HealthMap15 and others.
However, until recently, EIOS was capturing only information provided by official traditional media on the internet that is publicly available. In the meantime, we have observed an increasing flow of information coming from different social media platforms in the region, such as Facebook, Twitter and Instagram, in line with the exponential increase in their usage in the current decade, moving from almost 1 billion users in 2010 to 4.2 billion users worldwide as of January 2021.16 Along with the increase of usage of social media platforms by the government entities and political parties to announce important information regarding decisions made at the national level and promote citizen engagement.17 18 Additionally, social media platforms proved the ability to perform as a source of health communication and to cover various topics along with those covered by traditional media sources.11
Since the COVID-19 pandemic started, the monthly active users of Facebook and Twitter increased by 19% and 8%, respectively.19 Social media has proven its effectiveness in reaching audiences, directing public opinion, sharing information and harnessing collaborations among online users.20–22
The significant advancement and popularity of social media have drawn attention to the potential it bears to strengthen public health surveillance.23 24 Indeed, as early detection and timely monitoring of public health events through EBS require direct and timely access to a broad range of informants, social media was considered as a reliable and timely source of information during the COVID-19 pandemic.17 This consideration was mainly to serve the purpose of public health intelligence (PHI) since it can permit millions of users across the globe to post information on a wide range of events including potential health events in real-time, even from remote places that are hardly accessible. Several studies were conducted to evaluate the ability of social media platforms to become a reliable and fast source of health-related information. Bosley et al concluded that Twitter can be used as a source for information sharing and seeking between the public and healthcare professionals about the cardiac arrest through examining and classifying more than 60 000 tweets mentioning specific keywords on cardiac arrest and resuscitation.25 In the period of January 2013 to April 2015, Lee and colleagues used text-mining techniques to collect more than 6.3 million tweets mentioning ‘allergy’ or ‘allergies’ to track the seasonal allergy patterns and were able to conclude that the allergy tweets data has a very strong relationship with the daily maximum temperature in the larger states of the USA.26 In 2014, Guidry et al studied the social media posts related to Ebola outbreak on Twitter and Instagram (a social networking service for photo and video sharing) and found that in times of global health crises, the Instagram platform can be used as a network for establishing a way of meaningful and interactive communication with the public.27 Between all these trials of the social media platforms to serve as a massive source of public health information, we cannot ignore the fact behind social media had a big impact on everyone in the world due to rumours and misinformation being shared and communicated especially during the COVID-19 pandemic28 This paper represents the experience of WHO EMRO in using social media to detect and monitor COVD-19 events in the EMR.
Electronic scanning tools
Since 2017, WHO EMRO has used electronic media scanning tools to conduct the daily EI work to rapidly detect and monitor acute public health events of any origin. First, the EIOS has been developed by WHO and partners to permit access to a broad range of media available on the internet. In September 2019, in EMRO before the COVID-19 pandemic started, we initiated the scanning of social media to search for information on public health events with an initial objective of accessing public and available information communicated by social media users in the community. The use of social media started from the manual search process on Facebook and Twitter, where four new events (dengue fever in Pakistan, Middle East respiratory syndrome coronavirus in Qatar, cholera in Sudan and civil unrest in Iraq) were primarily detected from Facebook and Twitter public accounts. After that, the detection through social media was taken over by artificially intelligent (AI) software, Sprinklr and Epitweetr.
In May 2020, after assessing the increasing use of social media for communicating information on COVID-19, WHO collaborated with Sprinklr, a company that develops a Software as a service customer experience management platform, to review, analyse in real-time and visualise the impact of the COVID-19 pandemic. This was achieved by using the publicly available content from different social media platforms and messaging channels.29 Sprinklr’s platform, which is powered by industry-leading AI, is an online tool that is used to listen and gain understanding from publicly available conversations. One of the main features of Sprinklr is the ability to send alert trends in real-time through AI-detected anomalies, which enabled rapid detection and subsequent addressing of different outbreaks needs.
In June 2020, WHO EMRO joined an expert workshop organised by the European Centre for Disease Prevention and Control (ECDC) to develop a tool for Twitter trend analysis for EI activities. In October 2020, ECDC launched Epitweetr which is an R-based tool that allows users to automatically monitor trends of tweets by time, place and topic to early detect public health threats using Twitter data.30 This tool (Epitweetr) can systemically collate publicly available data from Twitter to early detect public health events. Epitweetr aggregates the daily collected tweets and related metadata using Twitter Standard Search API V.1.131 categorises them according to the geolocation and collects information on the keywords within the collected tweets. Next, a signal detection algorithm identifies the number of tweets (by geographical location and topic) that exceeds the expected threshold for a given day. Then, Epitweetr sends alert emails to notify on these signals.
For the purpose of this paper, the information is categorised according to the type of information source: social media and other media outlets (web news), the nature of the event: new event or event update. A new event was defined as the first report of a COVID-19 case in a country; an event update was defined as any new information on the epidemiological situation or information on public health and social measures related to an on-going COVID-19 event in the region, and the origin of the information: official or unofficial source.
Social media as EI
From 29 January 2020 to 31 May 2021 a total of 10 160 information was captured, out of which 95.8% were detected from social media (n=9732). All the information captured were escalated to events as they were considered as related to a situation representing a potential acute risk to human health, and finally as manifestations of disease or an occurrence that create a potential for disease. A total of 9732 signals (95.8%) were captured from social media, out of which, 11 were new events and 9721 were event updates. A total of 428 signals were captured from other media outlets (web news), out of which, one was a new event and 427 were event updates (see table 1).
Distribution of information captured through electronic media scanning by type of information source, Eastern Mediterranean Region 29 January 2020 to 31 May 2021 (n=10 160)
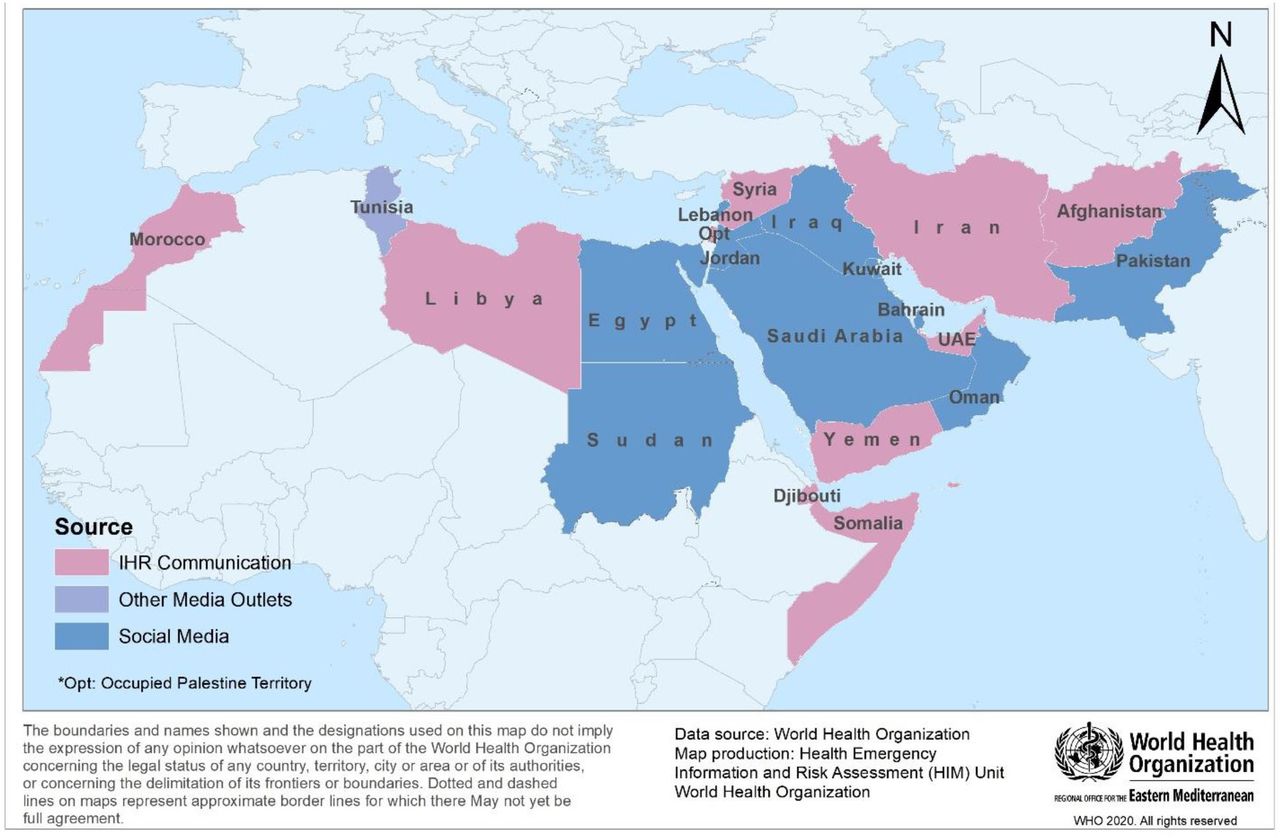
The 22 countries in the EMR region reported COVID-19. For 50% (n=11) of them, the detection of COVID-19 new events was done thanks to information primarily captured from social media while 4.5% (n=1) of the COVID-19 events in EMR were detected from information primarily captured from other media outlet. Ten COVID-19 events were directly reported to the WHO EMRO through the IHR reporting channels (see the geographical distribution presented in figure 2).
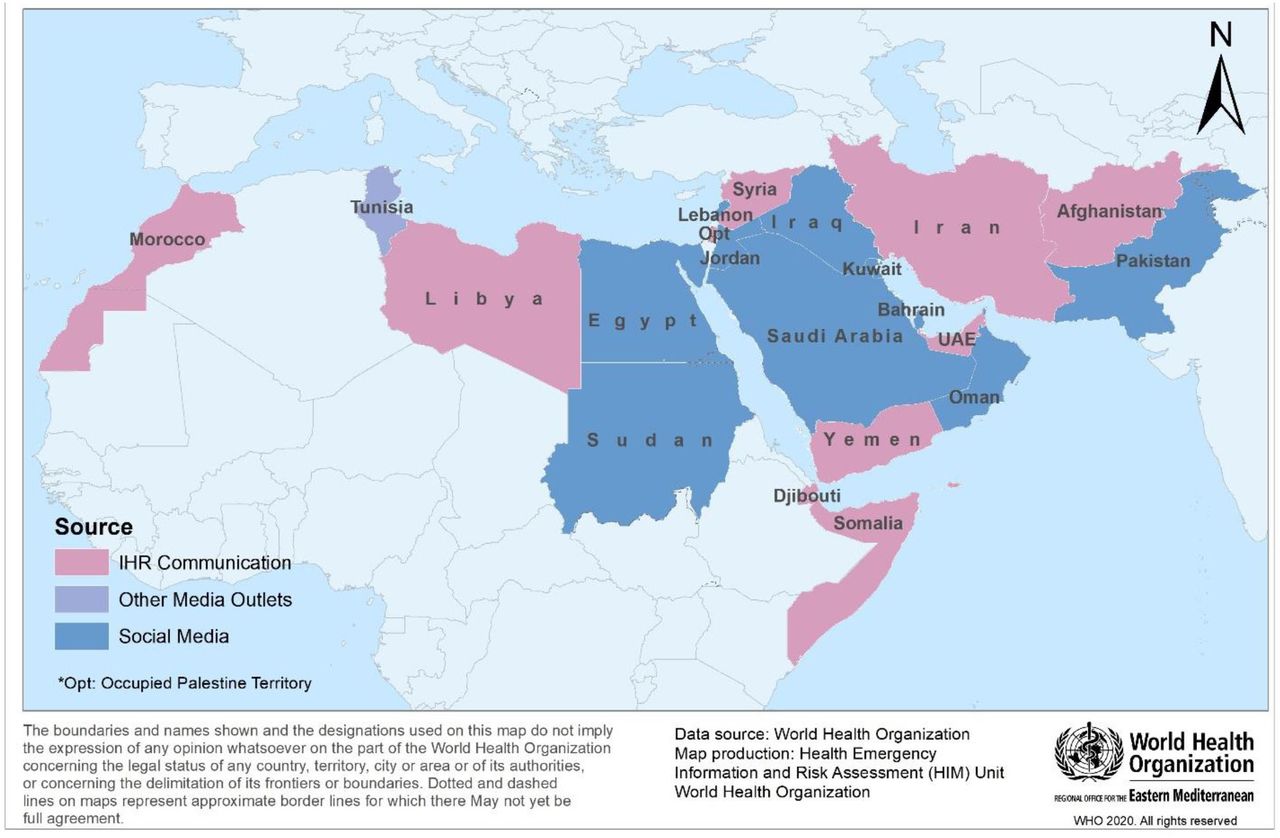
Distribution of new COVID-19 events by source of information, Eastern Mediterranean Region from 29 January 2020 to 31 May 2021. IHR, International Health Regulations.
Since the start of the COVID-19 pandemic, all the EMR countries, except Afghanistan, have reported their daily COVID-19 updates on their respective Ministry of Health’s (MOH) social media official accounts. As a result, 99.4% (n=9665) of the event updates captured from social media are considered official updates (table 2).
Distribution of social media event updates by origin of the information, Eastern Mediterranean Region from 29 January 2020 to 31 May 2021 (n=9721)
Lessons learned and ways forward
Since the start of COVID-19 pandemic, we have assessed that timely information on COVID-19 was mainly communicated through social media, which were not scanned by the EIOS. At the same time, MOH and governmental institutions realised the importance of using social media as a mean of communication with the public to share the daily updates and decisions related to the COVID-19 pandemic. Social media can provide a number of opportunities to build strong relationships, start engaging with the public, counterbalance the many rumours circulating on social media and demonstrate transparency to avoid social panic. In 2020, Kouzy et al were able to conclude, through a study that included 673 tweets, that misinformation and unverifiable information related to COVID-19 pandemic are being propagated at an alarming rate on social media.32
Social media was the first mean of communication used by 50% (n=11) of the EMR countries to announce the detection of initial COVID-19 cases. Additionally, some countries in the EMR (Oman, Somalia and Yemen) created COVID-19 only related accounts on Twitter, other than the MOH accounts, for the purpose of communication of the COVID-19 daily updates (online supplemental annex 1).
Supplemental material
In this regard, with the evolution of the pandemic in the EMR, instead of collecting information communicated by social media users in the community, most of the COVID-19 information collected was originating from official MOH Twitter and Facebook accounts. Over the period of 17 November 2019 to 17 March 2020, Rufai and Bunce tried to prove the power of Twitter as a communication tool by analysing the content of 166 informative tweets of the World leaders’ on Twitter in response to the COVID-19 pandemic and found that 28.6% of the collected tweets had web-links to government-based sources.33 Considering that social media might be an increasing source of information for the detection and monitoring of public health events, WHO EMRO has improved its capacity to capture information from them effectively.
In EMRO, monitoring of the COVID-19 pandemic was mainly done through the collection of information on social media. 95.8% of the COVID-19 updates were captured on social media where, almost all of the updates were communicated by MOH, leading to the establishment of social media platforms as the primary official channel of communication for public health events, for the first time. This might be because social media have been identified as an excellent communication mean to reach a 10s of millions of social media users.34 In 2021, Alomari et al used an unsupervised Latent Dirichlet Allocation topic modelling algorithm and was able to relate the increased activity on Twitter and high interaction in the Kingdom of Saudi Arabia with the quarantine concern that occurred on 21 March 2020, with the ‘Stay at Home’ campaign that was launched on Twitter by the Saudi Ministry of Health on the same day.35
This takes us to the lessons learnt from this paper where first, the information shared on social media about outbreaks are real-time, granular, detailed and can provide access to information that is not readily accessible through official sources data.36 37 Second, the informal sources like social media have improved timeliness and reporting of outbreaks. More than 60% of the first signals on new outbreaks come from such sources.37 38 Third, the increased interaction on different social media platforms tends to be more on news coverage and popular events, especially for novel health issues.39 In 2009, Keller et al analysed the timely sharing of information compared with an epidemic curve and supported the use of unstructured event-based reports from internet news and discussion sites for global surveillance of infectious disease surveillance (figure 3).36 Last but not least, we expect that in the future, we will also be able to capture more public health information provided directly by social media community users, before it is communicated by classical media or it reaches the health system and reported by the official sources. In return, it will strongly contribute to reducing the time of detection of public health events and will permit to provide a more rapid and effective response.

{kind=link}
{kind=link}
{kind=link}
Hypothetical timing of informal electronic sources available during an outbreak, by Keller et al.36
In the meantime, we are still facing some limitations as understanding public behaviour through analysing the data on social media is still limited and requires many more studies. In China, WeChat, a social application, was used to monitor changes in the COVID-19 trend through the public users’ behaviour, and Lu and Zhang predicted that, in the future, the public health authorities will rely more on social media to monitor the development of the epidemic or pandemic.40 Thus, the enormous publicly available data collected from different social media platforms could support PHI and decision-making.
Further work is planned to assess the performance of social media if it can detect public health events faster and more completely than traditional media sources publicly available on the internet so that we can analyse the impact of social media on the response to outbreaks.
Final remarks
Some questions and limitations remain about how to use the massive data of social media to inform the public health response. There are also major valid concerns about data protection and security. The use of social media in surveillance needs to be defined based on its purpose, scope of data and analysis. The widespread misinformation is still a challenge that needs to be taken into consideration, especially with the research and development happening to incorporate machine learning approaches for using social media in surveillance. Finally, there should be an inclusive platform that aggregates information for all the media including the popular social media platforms, such as Facebook and Twitter, which should be established to facilitate work in PHI worldwide.
Conclusion
In conclusion, real-time, transparent and relevant information posted on different social media platforms strengthens the early detection, monitoring and follow-up of public health events in WHO EMRO, especially during the current COVID-19 pandemic. Additionally, social media complements the sources of information used in the EBS at WHO EMRO.
Data availability statement
Data are available in a public, open access repository. Data are public and available on Twitter and Facebook.
Ethics statements
Patient consent for publication
Acknowledgments
The authors are very thankful to the WHO EMRO team at WHO EMRO for their valuable help in developing the process and conducting the work.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @ataboushady
Contributors HA, AK, AC and PN participated in the conception of the work. HA participated in the detection activities. HA collected the data. HA and AK contributed in the literature review. HA and PN conducted their analysis. HA and PN drafted the manuscript. HA, ATA, MT and PN reviewed and revised the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.