Article Text

Abstract
Soon after detection of the first COVID-19 case in Lebanon, a testing strategy was developed aiming to early detect new cases and identify close contacts in order to implement isolation and quarantine measures, thus limiting disease transmission. Field-testing activities were initiated in March 2020, focusing on suspected cases and close contacts. The objective of this paper is to present data collected between the 1st and the 35th week of 2021 and discuss challenges and lessons learned. During the study period, testing activities were conducted in field sites covering all Lebanese districts and following a fixed schedule. Testing was provided free of charge for suspected/probable patients with COVID-19 and close contacts of positive cases. Nasopharyngeal specimens were collected and sent to designated laboratories for reverse transcription polymerase chain reaction testing. Results were received on a timely manner, within 48 hours. From the 1st to the 35th week of 2021, 1244 field-testing activities were conducted with an average of 37 testing activities per week. During this period, 71 542 samples were collected with an average of 2104 specimens per week. On average, activities covered 78% of the Lebanese districts. The average positivity rate for this period was 24% (15%–33%) in line with the virus circulation levels in the country. Timely development and implementation of a testing strategy is crucial during epidemics. The success of Lebanon’s field-testing experience was mainly due to the timely adapted approach that covered all national territories, targeting all residents as well as high-risk groups in suburbs and remote areas.
- COVID-19
- public health
- descriptive study
Data availability statement
All the data relevant to this study are included in this article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Since the beginning of the COVID-19 pandemic, WHO urged all countries to develop testing strategies in order to guide and monitor public health control measures.
Soon after detection of the first COVID-19 case in Lebanon, a testing strategy was developed aiming to early detect new cases and identify close contacts in order to implement isolation and quarantine measures, thus limiting disease transmission.
Field-testing activities were initiated in March 2020, providing free of charge COVID-19 testing for suspected cases and close contacts.
The success of Lebanon’s field experience was mainly due to the timely adapted approach covering all national territories targeting all nationalities and the close collaboration between the Ministry of Health and the different stakeholders and partners.
Introduction
Since the beginning of the COVID-19 pandemic, WHO urged all countries to increase their level of preparedness and response, enhance their laboratory capacity and develop testing strategies in order to guide and monitor public health control measures.1 According to the European Centre of Disease Prevention and Control, testing strategies have five objectives: controlling the transmission of the disease, monitoring SARS-CoV-2 transmission rates and severity, mitigating the impact of COVID-19 in healthcare and social care settings, detecting clusters and outbreaks and maintaining COVID-19 elimination status once achieved.2
In Lebanon, since the first case of COVID-19 was diagnosed on 21 February 2020, the epidemic in the country is still evolving. Up to 2 April 2022, the cumulative number of confirmed cases reached 1 092 807 cases and 10 311 deaths with a total of three waves. In April 2022, a decrease in the number of cases was reported, reaching around 300 cases per day.3 With the first few cases reported in the country, testing was limited to a national reference laboratory. However, with the increase in the number of cases, both public and private hospitals/laboratories started testing for COVID-19. The most commonly used diagnostic techniques were the real-time reverse transcription polymerase chain reaction (rRT-PCR). Field-testing activities implemented by the Ministry of Public Health (MoPH) were initiated in March 2020, soon after the start of the epidemic in the country. Field teams were deployed to the different localities that were reporting clusters of cases. With the WHO support, the MoPH developed a strategy for COVID-19 testing, aiming to cover suspected/probable cases and close contacts of positive cases in all provinces.
The goal of this strategy is to limit the spread of the disease through early detection and isolation of new cases as well as identification and quarantine of close contacts. This strategy’s main objective is to make testing available and accessible for all residents inside the country, not leaving behind hard-to-reach settings and vulnerable populations. In this practice article, we will describe and present data collected during Lebanon’s 2021 COVID-19 field-testing activities between the 1st and the 35th week of 2021, highlighting lessons learnt and addressing challenges faced.
Preparation and facilitation of field-testing activities
Field-testing activities have evolved since their initiation in Lebanon in March 2020, where they initially aimed to test clusters in neighbourhoods, closed settings such as hospitals, informal tented settlements (ITSs), refugee camps, elderly homes and large companies dealing with public services to limit the virus transmission and implement isolation/quarantine measures in timely manner. In later stages, at the declaration of community transmission in the country, targeted testing has been aimed to test close contacts of cases. In June 2020, a testing strategy was organised where fixed field-testing points covering all Lebanese districts were assigned in different sites. In each district, one or two sites were selected in collaboration with the local municipalities. The testing points included public and private hospitals, health centres, public venues and gardens. Each field team included a trained nurse to collect specimens, a data operator and a driver. Trainings for field teams on specimen collection techniques, proper personal protective equipment (PPE) use and appropriate handling of specimens were conducted on a regular basis. Supervision of field teams was done by MoPH coordinators. Field teams were mobilised to the different sites based on a weekly fixed schedule, that was developed and coordinated in collaboration with local municipalities and partners.
Testing was provided for free in the field-testing sites for symptomatic patients fitting the case definition of suspected/probable patients with COVID-19 and for individuals who were close contacts of positive cases. A clinical suspected patient with COVID-19 was defined as any patient presenting with any of the following: (1) fever and cough and (2) acute onset of any three or more of the following signs or symptoms—fever, cough, general weakness/fatigue, headache, myalgia, sore throat, coryza, dyspnoea, anorexia/nausea/vomiting, diarrhoea and altered mental status. A probable case was a person with recent onset of anosmia or ageusia in the absence of any other identified cause. A contact of a positive case was identified as any family member/colleague/friend being in close contact with the positive case in the 2 days preceding the symptoms (or the laboratory test for asymptomatic contacts) or during the case’s illness. Initially, contacts were tested if symptomatic. Then, all contacts were tested: immediately for symptomatic contacts and household members or starting day 7 for other contacts.
Referral for testing was done through four channels: (1) the COVID-19 call centre receiving calls from suspected cases or contacts of positive cases, (2) surveillance and MoPH teams while conducting case investigation and contact tracing, (3) municipalities and (4) UN agencies supporting displaced populations (the United Nations Relief and Works Agency (UNRWA) United Nations Relief and Works Agencyand Palestinians and the United Nations High Commissioner for Refugees (UNHCR) for Syrians).
Prior to the field activity, arrangements included: (1) designation of a field team, (2) designation of a site and local partners, (3) preparation of the material for specimen collection and personal protective equipment, (4) preparation of the list of beneficiaries, (5) designation of the team in charge of specimen referral and (6) designation of a referral laboratory.
At the field site, the team was distributed at three points: (1) first point for crowd management usually supported by local partners, (2) second point for registration where the names were checked in the list, identity documents were verified, additional data were collected on Microsoft Excel and specimen tubes were labelled and (3) third point for specimen collection, where nasopharyngeal swabs were collected, and preserved in a viral transport medium, and maintained in zipped bags and an ice box with ice packs to maintain a cold chain . At the end of the activity, specimens were transported to referral laboratories by the Lebanese Red Cross or other partners. Moreover, drive thru service was provided in selected sites. rRT-PCR tests were performed, and results were received on a timely manner from the designated laboratories, within 48 hours of collection, including positive, negative and inconclusive results.
Confirmed cases were informed by MoPH surveillance teams, by calling them to collect needed information and complete the investigation. During the call, contacts were identified, advised on proper quarantine practices and offered an appointment at field-testing sites. Negative results were shared by local municipalities. Patients with inconclusive results were advised to repeat the test after 48 hours. In addition, designated laboratories preserved the positive samples for later genomic surveillance.
Along with data reported from other sources, like COVID-19 public and private laboratories, data collected through field-testing activities were entered on the District Health Information Software 2 (DHIS2) platform, feeding to the national COVID-19 database.
Data were analysed using Microsoft Excel 2016. Descriptive analysis was performed. Frequencies and percentages were computed, and tables and graphs were generated. The following indicators were monitored: number of field activities per week, number of specimens per week, positivity rate and geographical coverage of field activities. Positivity rate was computed by dividing the number of positive tests by the total number of performed tests. The district coverage of field-testing activities was computed by dividing the number of districts with field-testing sites over all districts (26 districts in Lebanon). A field-testing activity was defined as any visit conducted by a team to a specific location to collect COVID-19 specimens from suspected/probable cases and contacts of positive cases.
On a weekly basis, a report was issued by the Epidemiological Surveillance Programme documenting the activities and results of the field-testing sites. The report was included in the national COVID-19 daily surveillance report.
This is an observational study using aggregated deidentified data collected through surveillance activities. Though no ethical approval was required, ethical principles were followed throughout the data collection process like beneficence and justice through providing free of charge testing for Lebanese residents of different nationalities living in all districts in addition to respect of beneficiaries which was assured by providing regular training for field teams.
Field-testing outcomes
Field activities
From the 1st to the 35th week of 2021, 1244 field activities were conducted for a total of 71 542 tests and an average of 37 activities per week. With time, the number of activities increased progressively from week 1 to week 3. Between week 3 and week 17, the weekly number of sessions reached 50 with a peak of 58 activities on week 8. Starting week 17, progressive decrease was observed till week 29 with 18 weekly activities. Starting week 30, the number of activities increased progressively reaching 42 activities in week 33. The distribution of activities by weeks is presented in figure 1.

Number of sessions for field testing, Lebanon, January to August 2021.
Geographical coverage
The district coverage reached 78% for the period between week 1 and week 35. This indicator reached 100% during 3 weeks: 8, 9 and 12 as shown in figure 2. The majority of the districts were covered by field-testing activities as shown in figure 3.
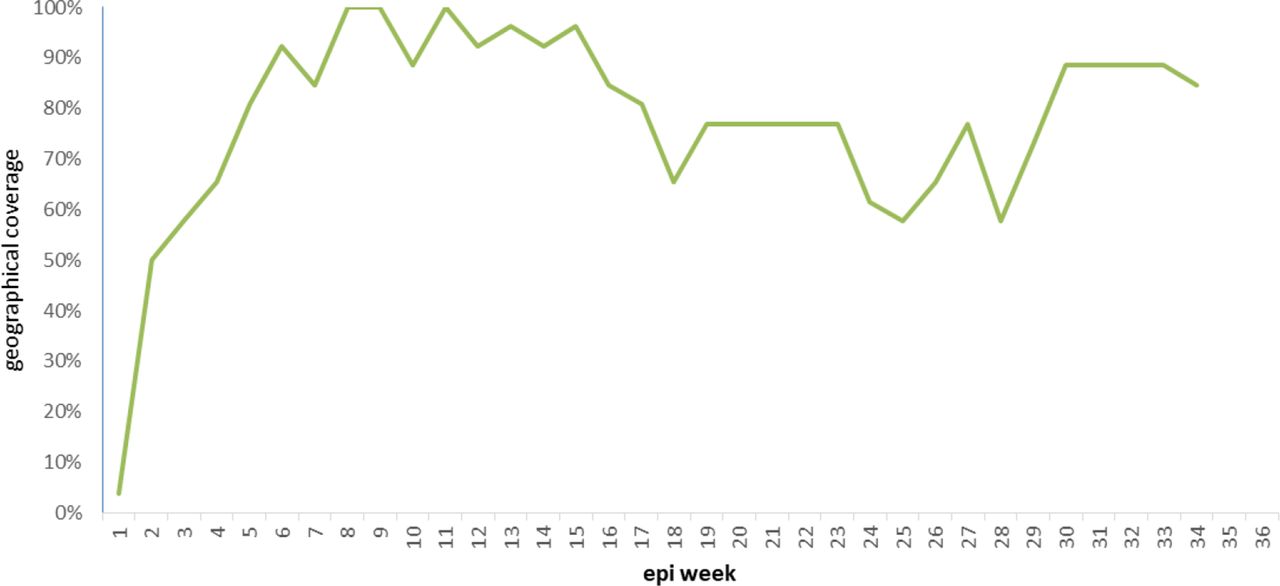
Geographical coverage for all 26 districts by week, Lebanon, January to August 2021.
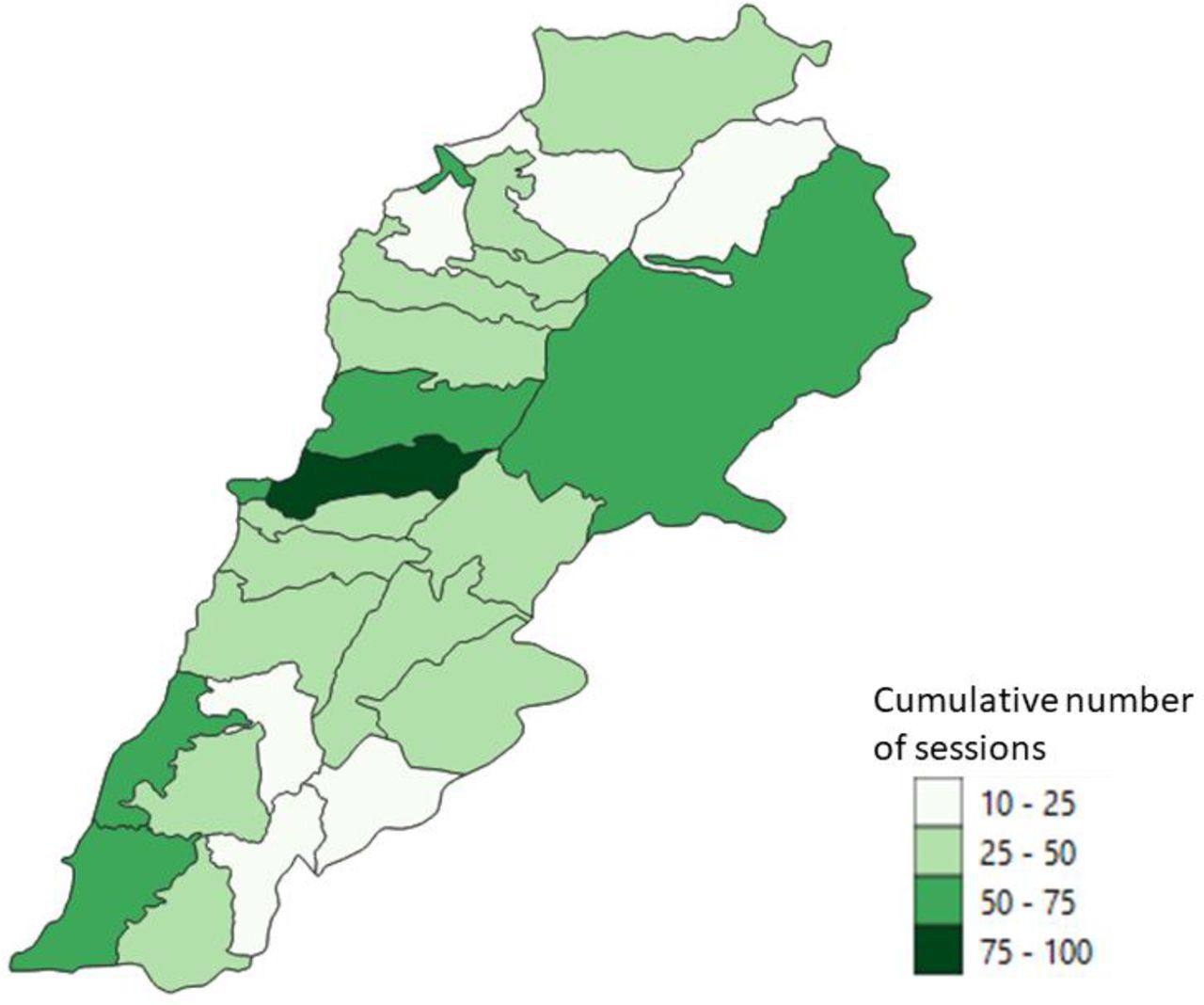
Distribution of field-testing sessions organised by the Epidemiological Surveillance Programme, January to August 2021.
Partnerships
Organisation of the field-testing activities was based on strong partnership between MoPH, local authorities like municipalities and international and national non-governmental organisations (NGOs), in addition to hospitals (from both public and private sectors) and schools, in order to secure the needed staff and the location of the field site. For the studied period, sessions were mainly supported by NGOs (55%), municipalities (24%) and the Ministry of Health staff (14%) in addition to hospitals (6%) and schools (1%). Five NGOs were involved in the field testing: Amel Association, Médecins Sans Frontières, Islamic Health Society, Armenian Cross and the International Orthodox Christian Charities.
Samples
During the aforementioned analytical period, 71 542 samples were collected from suspected/probable cases and contacts during the field activities with an average of 2104 specimens per week. By time, the number of collected specimens increased progressively from week 1 to week 3. Between week 4 and week 16, an average of 3785 specimens was weekly collected, with a peak of 4545 in week 8. Starting week 17, the total number of collected specimens decreased progressively till week 26 with 258 specimens. Starting week 31, an increase was observed with an average of 1781 specimens per week. The distribution of the number of collected specimens per week is presented in figure 4.

Number of collected samples and positivity rate from field testing, Lebanon, January to August 2021.
COVID-19
Out of the collected specimens, 18 976 tested positive for COVID-19 with an average of 558 positive tests per week. The cumulative positivity rate for this period was 26% and the average positivity rate was 24%, ranging between 15% and 33%.
Two waves were observed in the positivity rate curve. The first wave, from week 1 to week 19, had an average positivity of 27% and a peak of 33% at week 3 and week 8. The second wave, starting week 27, had an average positivity of 24%. The distribution of the positivity rate by weeks is presented in figure 4.
Close settings
The field activities included testing in close settings like elderly homes, long-term care facilities, orphanage homes, ITSs and refugee camps. From January to August 2021, 33 activities were conducted in close settings, where 1480 samples were collected with positivity rate of 42% (628 cases).
Lessons learned and overcome challenges
COVID-19 epi curve in 2021
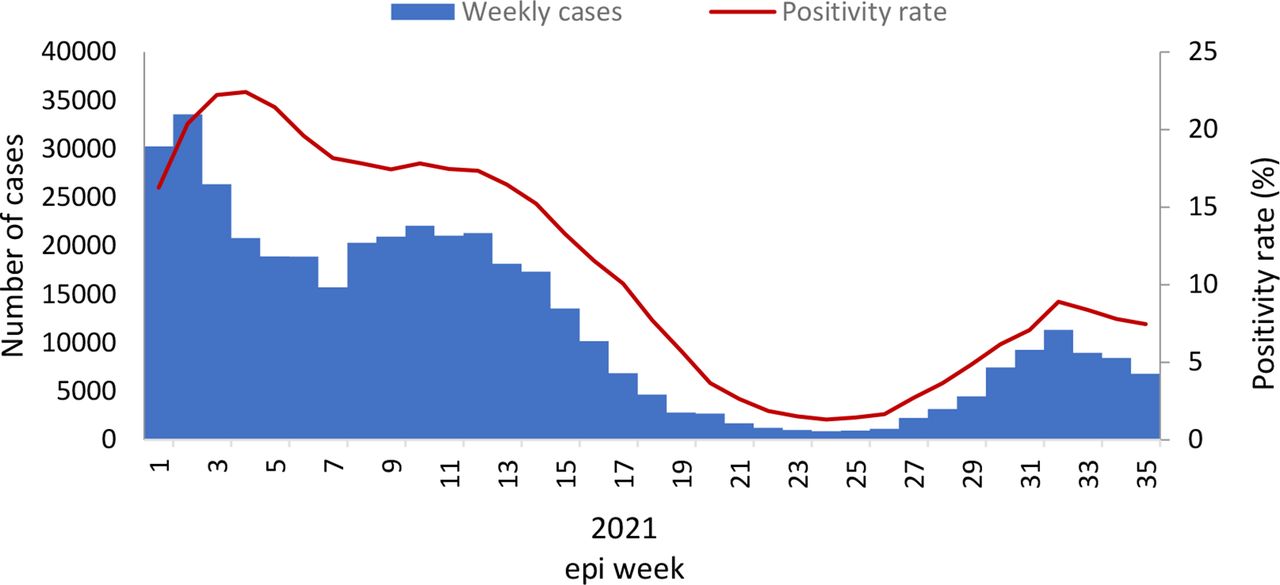
From January to August 2021, Lebanon witnessed two waves of COVID-19 cases (figure 5). The first wave was between January and April with 344 756 confirmed cases reported and 5470 deaths with a peak of cases reaching 6154 cases on the 14th of January and a peak of mortality reaching 98 deaths on the 4th of February. As per genomic surveillance findings, the dominant variant was alpha during this period.4
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
COVID-19 epi curve and positivity rate, Lebanon, January to August 2021.
Between June and mid-July 2021, the number of cases decreased and maintained stable levels. Starting mid-July, a new wave emerged, with 53 807 reported cases and 179 deaths (up to 31 August 2021). For the latter wave, genomic surveillance identified delta and delta-like variants in positive samples.4 The observed increase in the number of field activities and collected specimens were concomitant with the COVID-19 waves. This highlights the importance of the collected field-testing data during the different stages of the COVID-19 outbreak in the country. However, there was a difference in the positivity rates of field testing compared with the national positivity rates which is due to the fact that field testing targeted only symptomatic patients and contacts of positive cases; this could explain the higher and steady values of field-testing positivity rates compared with the national positivity rates which included the systematic testing for hospital admission, travelling, attending workplaces and so on.
Access for free testing for close contacts and suspected/probable cases
COVID-19 field-testing activities in Lebanon were initiated by the MoPH in 2020 soon after the reporting of the first few cases of COVID-19 in the country. These field-testing activities were maintained up to October 2020; however, these activities were disrupted between November and December 2020 due to saturated laboratory capacity at designated laboratories. In early January 2021, with the large increase of COVID-19 cases, hospitals and emergency rooms as well as laboratories were overwhelmed with patients with COVID-19 and contacts requesting COVID-19 testing. Consequently, the field-testing activities were reimplemented, building on lessons learnt from the field-testing experience of 2020. MoPH managed to reactivate the field-testing activities in order to provide a free service for the large number of close contacts identified during case investigation and symptomatic individuals calling the COVID-19 call centre and requesting COVID-19 testing. Field-testing activities were maintained during the study period and after that till March 2022, despite that the number of COVID-19 cases dropped between week 17 and week 28, 2021 (as shown in figure 1). In April 2022, with the decrease in the number of cases, field-testing activities were suspended, to be reactivated with any surge in COVID-19 cases.
Despite the challenges faced, mainly the limited public adherence to isolation/quarantine measures, the plan succeeded in providing free testing for a substantial number of residents in all Lebanese regions amidst the country’s economic crisis and their inability to cover testing fees. Thus, the testing plan contributed to limiting the spread of the disease,
Testing in specific settings
Testing in close settings like elderly homes is of great importance given the high risk of COVID-19 complications and death in these settings and the importance of early detection to reduce the transmission.5 Testing in informal settlements and refugee camps is also important in light of the large number of Syrians and refugees in the country living in poor conditions which increases the risk of communicable disease transmission in these settings.6 These activities are crucial to guide on proper prevention measures to be implemented.
Geographical coverage
The geographical coverage of these activities ensured that residents of different nationalities living in the different Lebanese districts are having equal access to free COVID-19 testing. This led to a greater health equity which is an important component of the testing strategy.7 Although universal coverage (100%) of field testing for all the 26 districts was not reached during all the weeks, all districts had the capacity of setting a field-testing site. The main criterion for organising a field-testing activity was to have a minimum number of beneficiaries attending the field-testing activity. If the number was not reached, the suspected/probable cases and close contacts were referred to nearest activity point outside their district of residence. The decrease in the geographical coverage observed between weeks 17 and 28 was concomitant with the low circulation of the virus in the country during this period, as shown in figure 5.
Collaboration between the different stakeholders
Throughout this field-testing experience, close collaboration was ongoing between different stakeholders including the field teams responsible for specimen collection and transportation, laboratories and local communities. Effective coordination between the different stakeholders ensured a proper implementation of the activities. It also helped in the timely management of any challenge faced by field teams at all levels. This networking is considered a key element for the success of any public health activity and more specifically for ensuring a successful and effective response to emergencies8
Contribution to genomic surveillance
Given the importance of genomic surveillance during the current COVID-19 pandemic, it was important that MoPH maintains a system for collecting COVID-19 specimens on a regular basis from the different Lebanese regions and contribute to the genomic surveillance by sending random specimens regularly to reference laboratories for genotyping to monitor the circulating COVID-19 variants
Timely sharing of results
Timely sharing of results helped in reducing the transmission of the virus from new cases to contacts. Results of the field-testing activities were timely shared to avoid any delay in sharing the positive results that may increase the risk of virus transmission to the close contacts. Positive cases were informed about their results as soon as laboratory results were shared and guided on proper isolation and preventive measures.
Proportion in the public sector
From March to August 2021, the field testing represented 16% of all tests conducted in the public sector, including hospitals and universities, and excluding the tests done at points of entry. During January to April 2021 wave, the proportion had an average of 21% and reached 26% at week 15. As for the second wave, the proportion had a weekly average of 11%.
Conclusion
Timely development and implementation of a testing strategy is crucial during epidemics. The success of Lebanon’s field experience is mainly due to the timely adapted approach that covers all national territories targeting all nationalities without leaving anyone behind, the efforts of the dedicated teams at the Ministry of Health and the different collaborating stakeholders and partners.
As the pandemic has been evolving so are the WHO recommendations for testing strategies at country level, where there has been always the call for prioritisation of testing in community transmission levels in countries with limited resources. Exhaustion of the human capacity at laboratories and the shortage of reagents and consumables are key factors dictating any testing strategy in countries. Testing is considered inefficient if there is no implementation of isolation for cases and quarantine measures for contacts. Risk communication and community engagement represent key factors for effective implementation of public health, social and individual measures in an attempt to decrease virus transmission.
Data availability statement
All the data relevant to this study are included in this article.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Laboratory of Molecular Biology and Cancer Immunology at the Faculty of Sciences at the Lebanese University at Hadath, Health and Environment Microbiology laboratory at the Faculty of Public Health/ Doctoral School of Science and Technology at the Lebanese University at Tripoli, National Influenza Center at Rafic Hariri University Hospital, Baalbeck Governmental Hospital, United Nations High Commissioner for Refugees (UNHCR), Amel Association, International Orthodox Christian Charities (IOCC), Medecins Sans Frontieres (MSF), Armenian Cross, Islamic Health Society, Lebanese Red Cross.
Footnotes
Handling editor Seye Abimbola
Contributors HAN, NG and HH initiated the field-testing activities in 2020. HAN, TT and ZF coordinated the activities in late 2020 and 2021. All authors contributed to the compilation of the data. ZF, NG and HS did the analysis. ZF and NG drafted the manuscript. All authors revised for critical content and approved the version for submission. ZF is the guarantor of this work. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.