Article Text

Abstract
Since the COVID-19 pandemic began, hospitals in the Eastern Mediterranean Region (EMR) have faced significant challenges in providing essential services, while simultaneously combatting this pandemic and responding to new and ongoing shocks and emergencies. Despite these challenges, policy-makers and hospital managers adapted their hospital responses to maintain operations and continue providing essential health services in resource-restraint and fragile and conflict affected, offering valuable insights to others in similar contexts. The aim of this paper is to share the lessons learnt from hospital responses to COVID-19 from the EMR. To do this, we triangulated findings from literature review, open-ended online surveys and 46 in-depth key informant interviews from 18 EMR countries. Qualitative findings from semistructured key informant interviews along with the open-ended survey responses resulted in nine major themes for lessons learnt in the EMR. These themes include Preparedness, Leadership and Coordination, Communication, Human Resources, Supplies and Logistics, Surge Capacity and Essential Services, Clinical Management (including Rapid Identification, Diagnosis and Isolation), Infection Prevention and Control, and Information and Research. Each of the nine themes (domains) included 4–6 major subthemes offering key insights into the regional hospital response to health emergencies. Resilient hospitals are those that can provide holistic, adaptable, primary-care-based health systems to deliver high-quality, effective and people-centred health services and respond to future outbreaks. Both bottom-up and top-down approaches are needed to strengthen collaboration between policy-makers, hospitals, front-line workers and communities to mitigate the continued spread of SARS CoV2, build resilient hospital systems and improve public health preparedness and emergency response.
- COVID-19
- Health policy
- Health services research
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Hospitals responding to COVID-19 in the Eastern Mediterranean Region (EMR), especially in the fragile and conflict affected settings (FCS), faced complex challenges of combatting the pandemic, maintaining critical and essential services while also responding to shocks and emergencies.
Systematic reviews conclude that lack of contingency planning and insufficient availability of resource threaten hospital disaster preparedness in the EMR.
EMR hospitals responding to COVID-19 offer 4–6 lessons for each of 9 areas including: Preparedness, Leadership and Coordination, Communication, Human Resources, Supplies and Logistics, Surge Capacity and Essential Services, Clinical Management (including Rapid Identification, Diagnosis and Isolation), Infection Prevention and Control, and Information and Research.
The most frequently repeated lessons included: ‘prevention’, ‘leadership’, ‘coordination’, ‘human resource management’ and ‘communication’, highlighting their central role in strengthening hospitals preparedness for crisis, outbreaks or pandemics.
These lessons learnt for each of the domains do not occur in isolation but rather through a holistic approach to enhance hospitals emergency readiness, response and resilience.
In FCS, EMR hospitals highlighted the need to increase capacities for critical care management, improving agility and adaptability for outbreak response and eliminating attacks on health facilities.
Strengthening hospitals preparedness entails strengthening each of the checklist domains within a proactive, multisectoral and system-wide approach; requiring both bottom-up and top-down strategies.
Strengthening hospitals’ capacities for preparedness, response and recovery is essential for health systems strengthening, emergency and outbreak response, and overall global health security.
Introduction
The dual aims of achieving universal health coverage (UHC) and protecting global health security (GHS) are central to realising the right to health for all, which requires significant health systems strengthening (HSS).1 The Eastern Mediterranean Region (EMR) comprises of 22 countries, ranging from Morocco to Pakistan, with varying diversity in wealth, political stability, health system resilience and emergency preparedness with two-thirds of health systems in the EMR are affected by humanitarian and graded emergencies.2 In the EMR, around 80% of hospital beds are in the public sector, ranging 3.9 hospital beds per 10 000 population in Afghanistan to 32 beds per 10 000 in Libya.3 Prior to the pandemic, health systems and hospital sectors across in the EMR were challenged by shortages of financial, material or human resources, inaccessible or ineffective services, or poor quality, especially in fragile conflict settings (FCS).2 3 By January 2021, 25% of essential health services (EHS) were disrupted in 21/22 EMR countries, mostly affecting routine immunisations, dental services, rehabilitation services and family planning, and further exposing the fragility of medical supply chains.4
As of August 2021, there were approximately 13 million cases with almost 240 395 deaths in the EMR.5 Early experiences in combatting COVID-19 highlighted the roles of hospitals in protecting GHS, achieving UHC, and ensuring patient’s rights to health.6 7 Strengthening hospitals’ capacities for preparedness, response and recovery is essential for mitigating the impacts of the pandemic on clinical management, EHS provision, health workforce, supply chain and risk communication, among others.8–11 A systematic review of hospital disaster preparedness in the EMR found that the current outbreak response was threatened by a lack of contingency planning and insufficient availability of resources.12
While responding to COVID-19 during the first year of the pandemic, hospitals faced an evolving set of challenges.13 14 A recent study found that in the first months of the pandemic, hospitals faced shortages of health workers (specifically critical care specialists), insufficient hospital beds, severe shortage of personal protective equipment (PPE) and insufficient/not enough/testing kits, which resulted in delays in confirming suspected cases, overcrowding of designated hospitals, inefficient use and wastages of resources, financial losses and in some cases preventable infections and deaths.15 In the face of second and third waves, additional factors challenged EMR hospitals including overwhelmed and exhausted staff, with high levels of burn-out, anxiety and absenteeism; excess numbers of severe cases requiring critical care; shortages of Intensive Care Unit (ICU) beds, ventilators and oxygen supply; and higher than usual lengths of stay.3 16 The COVID-19 pandemic has highlighted the importance of strengthening hospitals and health systems resilience to achieve UHC and protect GHS.3 14 17 18
Despite these challenges, policy-makers and hospital managers (HMs) adapted their hospital responses to maintain operations and continue providing EHS in resource-restraint and FCS, offering valuable insights to others in similar contexts .
This article aims to present the major lessons learnt from hospital responses to COVID-19 in the EMR.
Lessons learnt from the COVID-19 pandemic
Guided by WHO/EMRO’s COVID-19 readiness checklist, qualitative findings from semistructured key informant interviews (KIIs) along with the open-ended survey responses resulted in nine major themes for lessons learnt from hospitals experiences responding to COVID-19 in the EMR.19 These themes included: Preparedness, Leadership and Coordination, Communication, Human Resources, Supplies and Logistics, Surge Capacity and Essential Services, Clinical Management (including Rapid Identification, Diagnosis and Isolation), Infection Prevention and Control (IPC), and Information and Research. Each of the nine major themes (domains) included 4–6 subthemes offering key lessons for hospitals’ responses to infectious disease outbreaks (see figure 1). Further details regarding the methodology can be found in online supplemental annex 1.
Supplemental material
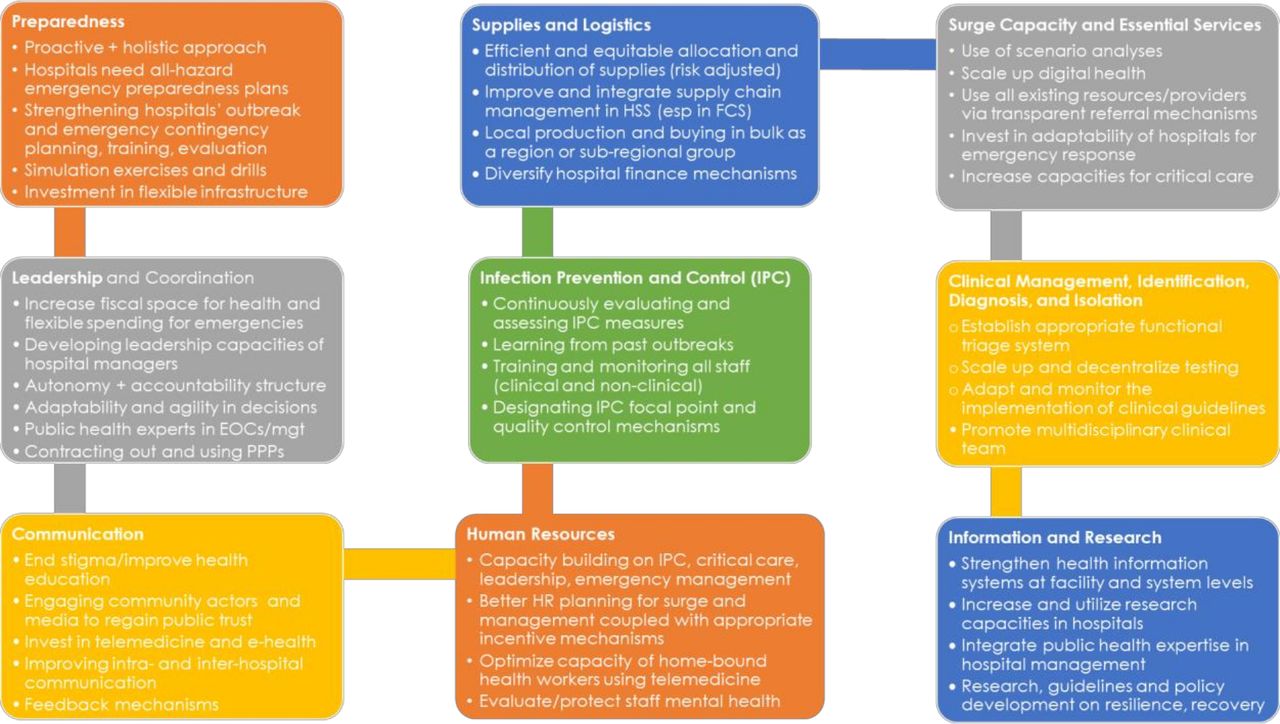
Nine major lessons learnt from hospitals responses to COVID-19. EOCs, Emergency Operating Centres; FCS, fragile and conflict setting; PPs, public private partnerships.
Hospitals’ preparedness
The most frequently cited theme across the qualitative findings was ‘preparedness’. Moreover, across survey responses, ‘prevention’ emerged as the most mentioned lesson learnt from hospitals responding to COVID-19 (see figure 2). KIs stated that early preparedness interventions were the biggest learning from responding to COVID-19, highlighting the need for a paradigm-shift from reactive and responsive to preventive and proactive contingency planning: ‘preparedness does not start at the time of the crisis’ (KI-1).

{kind=link}
{kind=link}
Most frequent responses from qualitative findings on lessons from hospitals’ responses to COVID-19.
Across our interviews, KIs from high-income, middle-income and low-income countries reflected on the need to evaluate hospital responses to previous infectious diseases outbreaks (eg, MERS and SARS) or nosocomial multidrug-resistant infections in order to inform facility-level contingency plans for various hazards. Furthermore, hospitals in FCS expressed the need to expand and adapt their readiness plans to all-hazards approach, beyond managing mass causalities and surges for traumas to include protocols for infectious diseases: ‘Every hospital should have preparedness plans for emergency, trauma, explosion, outbreak’ (KI-2). Furthermore, in responding to COVID-19 among other infectious diseases, HMs in several low-income countries in the EMR raised the importance of designating a section in hospitals for the management of infectious diseases, with appropriate structural and technical specifications: ‘At least one unit has to be dedicated for infectious diseases with proper air handling systems, all precautions and guidelines followed so we are not caught off guard’ (KI-3).
KIs further contrasted the lack of preparedness across the Region, as some hospitals followed national preparedness plans with limited adaptation at facility level, while others had plans but lacked implementation. Beyond creating facility-level guidelines and standard operating procedures, HMs stressed the need for all-staff trainings, continuous communications, drills and simulation exercises to strengthen readiness and response, along with monitoring, evaluation and learning from the experiences of other countries and hospitals.
In strengthening hospitals’ preparedness, KIs further emphasised the importance of adaptability and agility in leadership and decision making. Other KIs highlighted that all staff, especially nurses, paramedical and non-clinical hospital workers needed further training on preparedness, critical care management and IPC. HMs suggested using simulation exercises, hands-on trainings and sensitisation of health workers on proper use of PPE. HMs reported learning to use online platforms and e-learning to enhance risk communication and capacity building for outbreaks and emergency response.
Leadership and coordination
The theme of leadership and coordination was among the most frequently cited, and often in association or intersection with other domains such as communication, human resources, financial and supplies management, and effective clinical management (including IPC). KIs further concluded that strong leadership with clear vision to push through crisis to recovery, adequate coordination of all actors, clear communication and ability to motivate overworked and burnt-out staff are necessary attributes in outbreak response.
At the policy level, this pandemic revealed the importance of raising health as an urgent priority for state policy-makers, with effective collaborations across ministries and relevant actors. KIs associated the weak and delayed response of governments to this chronic under-prioritisation of health at the national level and highlighted the overall need to increase fiscal space for health and flexible funding for emergency preparedness in the hospital sector. This theme was especially prevalent among KIIs from the Region’s LMICs and FCS.
The interlinkages between the hospital and policy-levels was highlighted throughout KIIs. Some HMs were appointed to national COVID-response committees, where their technical expertise contributed to policy development, national security measures and decisions, and evaluation of clinical guidelines. Across the EMR, HMs also noted that decentralisation, transparency and increased autonomy for decision making coupled with robust accountability mechanisms improved operations, procurement and logistics. Donor dependency and restrictive budgeting were reported as limitations in hospitals’ emergency response; hospitals in the EMR’s FCS highlighted the need for increased fiscal autonomy to facilitate effective and efficient management. Across LMICs, KIs also suggested using Public Private Partnerships to surge the capacity of the hospital sector and to enhance hospitals performance and resilience in outbreaks (especially in FCS).
At facility level, hospital managers reported establishing Emergency Operating Centres and multidisciplinary COVID-19 management teams to ensure smoother coordination, communications, resource management, teamwork and compliance to clinical and managerial guidelines. Some KIs further noted that capacity building on leadership was necessary for hospital managers, to increase their competences in disaster and emergency management. Furthermore, qualitative findings also mentioned investment in young leaders and middle management to improve hospital outbreak response: ‘The real work is done by the middle management, we must equip them for assessing the situation and reacting right away as opposed to waiting for something to come from the top’ (KI-4). This lesson was especially critical for hospitals in FCS where political turbulences and instability threaten sustainability and retention of expertise.
Communication
Improving communication with staff (to improve operations and morale), other service delivery actors (to facilitate coordination and referrals), and the community (to revitalise services utilisation and rebuild trust in the health system) is necessary to ameliorate outbreak responses. KI further confirmed that: ‘If you want to implement [the response plan] right, you need to involve and effectively communicate with other sectors, private, NGO, and most importantly, the community’ (KI-1).
Between the community and facility levels, hospitals mobilised community volunteers and peer-educators to raise public awareness about the virus, its transmission, and preventive measures while others engaged community and religious leaders, collaborated with the media and established in-house public relations departments: ‘There was a media department in most hospitals to provide information about this virus and how to deal with this pandemic. Our role is not only to treat patients, but also educate the public‘(KI-5).
To enhance interhospitals and intrahospitals communications, HMs reported using social media platforms, such as WhatsApp groups and Hospital Information Systems. This enabled timely communication between senior management and clinical staff, and empowered front-liners with feedback, access to updated clinical information and guidelines, and training.
At the policy level, HMs noted that the establishment of national feedback mechanisms enhanced communication, coordination, evaluation and supportive supervision for hospitals, ministries of health (MOH) and other actors in service delivery.
Human resources
Our study revealed that biggest challenges hospitals faced during this pandemic was the shortages of ICU, infectious diseases and pulmonary specialists and nurses resulting in many clinicians working outside their disciplines, specialisations and environments. To fill this gap, KIs reported using e-learning in teaching temporary or new health workers critical care competencies which cannot be learnt overnight and require retraining and reaccessing training materials. HMs emphasised the need for hands-on training to improve practical skills in critical care management.
To overcome these challenges, HMs recounted recruiting surge staff through volunteering, task-shifting, international recruitment or special contracts. KIs, especially in FCS, reflected that more effective and sustainable HR planning was needed along with further research on recruitment and retention strategies for pandemic front liners: ‘Thousands spent on [ICU] training and the result was nothing because we lost all those we trained. We need sustainability and continuity’ (KI-6).
Moreover, strategic HR planning along with appropriate staff financing for different surge and outbreak scenarios, providing holistic incentive packages (including health insurance), developing better working environments, expanding scopes of work, exploring task-shifting especially in health promotion and risk communication were all suggested solutions to reduce brain wastage and optimise human resource management for outbreaks.2 20–23 Our study also revealed the need to prioritise hospital staff mental health, emergency and stress management, and equip hospital managers on motivating burn-out staff.
Supplies and logistics
To improve supply chain management and maintain EHS, many EMR hospitals applied scenario analysis to estimate consumption of supplies and pharmaceuticals and used needs-based inventory management. To overcome national and global shortages, restrictions on travel and trade, and challenges of procurement, some HMs invested in local capacities and relied on self-production of PPEs and supplies. KIIs reported utilising the collective strength of subregional and geopolitical partnerships for buying-in-bulk.
Furthermore, KIs highlighted the importance of investing in adaptable hospital infrastructure as a major lesson in pandemic preparedness: ‘When we build hospitals, flexibility in design is extremely important. The general wards could be converted into ICU beds with dialysis units’ (KI-7). Agile infrastructural redesign of wards and adapting hospital service areas for infectious disease outbreaks were central to strengthening hospital’s COVID-19 response.
Surge capacity for EHSs
To expand staffing for surges, hospitals used telemedicine to engage health workers currently outside the national labour market, including the diaspora, to address shortages, maintain EHS, increase accessibility of patients, and provide flexible working conditions for providers. The use of telemedicine and e-health was unanimously mentioned in the qualitative findings. KIs discussed the use of remote consultations with specialists in tertiary teaching hospitals and global experts from multinational organisations, academic institutions and the diaspora, particularly for critical care services.
Moreover, integrating hospitals into a strong primary-care network is essential to improving response, resilience and service delivery and was highlighted as an opportunity for growth among various KIs in EMR. This intervention was reported to improve efficiency in the response by reported reducing pressure, allocating resources more efficiently, referring patients on a needs and risk basis and empowering communities with information and preventative practices: ‘We need to integrate the whole system, we have very good primary health care and that why hospitals like us were able to focus and concentrate on [COVID-19]’ (KI-7).
Clinical management
With evolving clinical guidelines, HMs reported updating their protocols in line with the latest evidence-based recommendations. To improve rapid identification and diagnosis, KIs underscored the necessity of early investment, sufficient procurement, equitable distribution and decentralisation in testing, collaboration with private sector to increase lab capacity, and establishment of in-house laboratories. In resource-limited FCS, hospitals adapted and used innovative solutions to improve clinical management including: establishing fever clinics outside hospitals to screen suspected cases, using 24/7 hotlines for clinical guidance for critical care, adapting different mechanisms to increase sufficient oxygen supply, diversifying diagnostic tools, increasing the availability and distribution of ICU beds and critical care, using multidisciplinary clinical teams and altering hospital infrastructure for better triage, case management and IPC.
Infection prevention and control
Compliance with IPC emerged as one of the most important lessons in maintaining hospitals operations and ensuring quality, safety, efficiency, accessibility in service delivery.2 20–22 Qualitative findings highlight the themes of ‘prevention’, ‘control’, ‘PPE’, ‘protective’, ‘training’, among others (figure 2), reflecting the significance of IPC among the lessons learnt. KIs emphasised the need for staff training in IPC, social distancing, isolation of COVID-19 patients, handwashing and improving staff and public awareness: ‘I stress again the need to emphasize strict adherence to all IPC protocols to minimize the unnecessary losses of [patients and health workers]’ (KI-8). Mortuary management was seldom mentioned in the literature or by KIs, potentially due to stigmatisation and misinformation about IPC measures while burying COVID-19 patients. This area requires training and sensitisation for both health workers and the general public.
Information and research
Cited as essential factors in building hospitals for post-COVID recovery as a ‘New Normal’, KIs highlighted the need for guidance on optimising the use of digital health in order to design more adaptable and agile hospitals, allaying distrust of health workers and underutilisation of health systems, reducing mental health burdens on frontline workers, and evolving responses to adapting variants and vaccinations. Notably, KIs, especially in FCS, expressed the need to integrate electronic supply chain management and information systems into HSS efforts and strengthen local and facility research capacities. Furthermore, hospitals found that scaling up facility-based reporting mechanisms and adequate IT infrastructure supports the use of telemedicine, the collection of epidemiological and quality of care indicators, and the evaluation of the impact and effectiveness of preparedness interventions.
In addition to this, KIs described the integration of public health professionals and related expertise in hospitals and emergency management as necessary preparedness and leadership interventions at both the facility and national levels. Finally, HMs stated their expectations of both Ministries of Health and WHO in continuous updating of interim guidelines, resource mobilisation, virtual capacity building and technical support to maintain and monitor EHS while transitioning health systems back to normalcy and through recovery.
Implications for policy and practice
This article presents lessons learnt from hospital’s experiences combatting COVID-19 in the EMR across nine domains. Guided by the WHO/EMRO hospital’s readiness checklist for COVID-19, the qualitative findings of this study highlight key lessons (subthemes) across these various domains (as seen in figure 1).
The theme and lesson of preparedness (described by qualitative findings as ‘prevention’) was the biggest key takeaway from this analysis (see figure 2). Although preparedness was not mentioned as a component of the framework, but rather the overarching aim of the readiness checklist, this regional study revealed that strengthening hospitals preparedness entails strengthening each of the checklist domains within a proactive, multisectoral and system-wide approach.
With more than half of EMR countries facing emergencies, this regional study is unique in that in provides insights from many hospitals responding to the pandemic in FCS. Diversifying hospitals financing mechanisms, decentralising fiscal decision making, and increasing autonomy at facility level are consistent with the literature on strengthening preparedness especially in FCS.18 24–27 Due to the prolonged response to COVID-19, further research on improving health workforce resilience.14 20 28 29 Griffin et al highlight the need for the need for self-care, psychosocial support and timely access to mental healthcare for front responders.29 One of the main lessons learnt from this study, confirmed extensively across global literature, is the central role on in improving community ownership towards effective outbreak response; this was especially highlighted in FCS where hospitals are a trusted and reliable source for emergency care services, health education and risk communication.30–34 Further to this, in these humanitarian settings, EMR hospitals highlighted the need to increase capacities for critical care management, improving agility and adaptability for outbreak response and eliminating attacks on health facilities.24 25 34–36 Generally, these findings were comparable with the literature, particularly from other resource-limited and FCS.30 37 Ratner et al confirmed the importance of flexibility, task-sharing, monitoring, evaluating and daily learning (as a multidisciplinary team), and advocacy to improve hospitals’ preparedness, emergency response and subsequent resilience to shocks.30
Furthermore, this study revealed opportunities to explore numerous aspects of hospitals preparedness and response including the cost-effectiveness of building resilient hospitals, innovative evidence-based interventions to overcome complex challenges, and interlinkages between the various framework domains. Evidence generation is especially needed regarding the adaptation and contextualisation of these lessons in FCS.
Moreover, this regional study, with a large focus on FCS, confirms global systematic reviews which underscore the link between strengthening preparedness and improved resilience.1 14 17 18 This study highlights the crucial role that hospitals’ preparedness plays in health systems resilience, risk reduction and disaster response, and more universally GHS.8 8 17 38 While this framework-led analysis identified major themes for each of the checklist domains, cross-cutting sub-themes emerged including ‘preparation’, ‘prevention’, ‘higher-level coordination’, ‘prioritisation’, ‘adaptation’, ‘learning and evaluation’, ‘continuous training’, ‘stakeholder involvement’ and ‘compliance’. These lessons learnt and improvements for each of the domains do not occur in isolation but rather through a holistic approach to enhance hospitals emergency readiness, response and resilience.
Conclusion
The lessons learnt from this study confirm that building resilient hospitals requires strengthening preparedness capacities for contingency planning, surge capacity, communication, training and education, critical care and emergency management, surveillance, standard operating processes, protection from nosocomial transmission and promotion of mental well-being within a resilient health system which can adapt, absorb and recover from various shocks.7 8 13 17 Even in the highest-performing health systems in the EMR and worldwide, hospitals require capacity building, coordination, leadership to improve equity, quality and effectiveness in the whole of government COVID-19 response and health systems recovery.10 14 39 40 Bottom-up and top-down approaches are needed to strengthen collaboration between policy-makers, hospitals, frontline workers and communities to mitigate the continued spread of the virus, improve emergency and outbreak preparedness, and inform policy development.12 17 30
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by WHO EMRO Regional Ethics Review Committee. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Contributors HR: conceptualisation, data collection, data analysis and interpretation, critical revision, finalisation, and acts as the guarantor. MK: conceptualisation, data collection, data analysis and interpretation, drafting of manuscript, revision and finalisation. AM: conceptualisation, planning and study design and critical revision of manuscript. All authors have read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.