Article Text

Abstract
Introduction Several efforts have been made globally to strengthen the health workforce (HWF); however, significant challenges still persist especially in the African Region. This study was conducted by the WHO Regional Office for Africa to present the status of the HWF in 47 countries as a baseline in measuring countries’ progress in implementing the Global Strategy for HWF by 2030.
Methods This was a cross-sectional survey of 47 countries in the African Region using a semistructured questionnaire. Data were collected from January 2018 to April 2019. Before data collection, a tool was developed and piloted in four countries. The completed tools were validated in the countries by relevant stakeholders in the 47 countries. Data were collated and analysed in Epi Info and Microsoft Excel.
Results The total stock of health workers was approximately 3.6 million across 47 countries. Among these, 37% of the health workers were nurses and midwives, 9% were medical doctors, 10% were laboratory personnel, 14% were community health workers, 14% were other health workers, and 12% were administrative and support staff. Results show uneven distribution of health workers within the African Region. Most health workers (85%) are in the public sector. Regional density of physicians, nurses and midwives per 1000 population was 1.55, only 4 countries had densities of more than 4.45 physicians, nurses and midwives per 1000 population.
Conclusion This survey has demonstrated that the shortage and maldistribution of health workers in the WHO African Region remain a big challenge towards the attainment of universal access to health services. This calls for the need to substantially increase investment in the HWF based on contextual evidence in line with the current and future health needs.
- Health policy
- Health systems
- Public Health
Data availability statement
All data relevant to the study are included in the article .
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Ensuring universal access to health services requires adequate, qualified, fairly distributed and motivated health workers.
Despite numerous regional and country efforts, there remains key challenges to address the adequacy of the skilled health workers to respond to the health service needs for universal health coverage (UHC).
Due to low capacity of the human resources for health information systems and health workforce (HWF) registries in the African countries, HWF data are fragmented and are often not accurate.
WHAT THIS STUDY ADDS
A status of the health workers of all categories in all countries in the African Region in 2018.
The density of doctors, nurses and midwives per 1000 population in the WHO African Region in 2018 was 1.55. Only four countries—Seychelles, Namibia, Mauritius and South Africa—have densities above of 4.45 doctors, nurses and midwives needed to make advancements towards UHC.
Health workers in the public sector compared with the private sector in countries within the WHO African Region because there is limited information about the HWF in the private sector.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
In practice, the findings of the survey provides evidence on the state of the HWF in the African Region needed to build stronger health systems and ensure universal access to healthcare services.
Countries need more contextual evidence on the HWF to align their investment with the current and future health needs.
Introduction
Adequate, well-trained, fairly distributed and motivated health workers are critical to improving the health of a population, as well as ensuring the achievement of universal health coverage (UHC) and Sustainable Development Goals (SDGs).1–3 The Global Strategy on Human Resources for Health (GSHRH): Workforce 2030 emphasises that health systems can only function well when they have sufficient, well-trained and equitably distributed health workers; who are competent, responsive, motivated and productive.2 Health workers are recognised as an important component of all the health systems inputs and a top priority of the global agenda with the extent of the shortage of health workers in various countries highlighted in several publications.4 5 Although some global efforts have been made to improve the health workforce (HWF), nearly all countries are challenged by large deficits and inequitable distribution of health workers.5 This is compounded by the lack of accurate data on the HWF that is required to optimally use existing health workers and advocate for investment in the HWF.3 Countries worldwide are facing challenges in the education and development of their HWF.5 Africa on the other hand faces long-standing HRH crisis.6 7
In 2014, the Global Health Workforce Alliance and WHO reported on the status of the global HWF status based on the data of 186 countries. The report noted that only a few countries had comprehensive and accurate data on the existing health workers (only 53% of them had reported annual HWF data).8 This shortage was most severe in low-resource settings, including the African Region where 36 Member States were classified to have HWF crisis.6 It was found that there was a deficit of 7.2 million health workers worldwide, and it is predicted that by 2030 the shortage will grow to 18 million. It also indicated that 83 countries were below the WHO minimum threshold density of 22.8 health professionals (physicians, nurses and midwives) per 10 000 population, in relation to the objective of delivering essential health services of relevance to the Millennium Development Goals (MDG)—primarily MDG 4 and 5.
By 2015, only 11 countries in the WHO African Region had met the above-mentioned WHO minimum threshold density.5 However, there has been an overall increase in the stock of these categories of health workers in more than half (54%) of the countries, but in terms of density, about 23% only have reached or exceeded this minimum threshold. The projected shortage of health workers in Africa by 2030 is expected to be 6.1 million.5 This gap has not only hampered the provision of essential healthcare services to meet health-related development goals but has also constrained accelerated progress towards universal healthcare coverage.7 9–11 The African Region not only has the lowest number of health workers but also the lowest density of HWF12 and the highest disease burden.13 This high disease burden and the increase in health emergencies have exacerbated the need for qualified health workers in the region.
The GSHRH: Workforce 20302, within the framework of UHC, aims to support countries to scale up interventions aimed at strengthening health systems to ensure equitable and universal access to health workers. The African Region endorsed the Global Strategy in 2017 in adopting the African Regional Implementation Framework of the GSHRH6 to provide contextual guidance to the Member States in the Region. The main objective of this framework is to support countries' efforts to make adequate HWF strategies and investment plans to ensure availability and universal access of everyone to qualified health workers. This aligns with the approach for achieving UHC through health system strengthening, and concerted efforts to build a functional HWF.14 Health systems strengthening is considered a key to driving progress towards equity and UHC.14–16 This implies that strengthening universal healthcare systems, capable of addressing the needs of the population, requires, among other things, ensuring universal access to a well-trained, motivated and adequately supported HWF.2 17
The African Regional Implementation Framework of the GSHRH6 highlights that there is low production of health workers in the region, due to inadequate HRH education and training capacity. Additionally, the Framework also highlights the continued weakness of HRH management and steering as a key drawback to building a strong and effective HWF and achieving UHC in the African Region. In this regard, the Framework recommends that there is a need for high-level commitment and strong leadership to guide and coordinate stakeholders and to strengthen the capacity of HRH Departments in Ministries of Health (MOH) to improve the implementation of the HRH strategic plans. The Framework also highlights the need for reliable HRH data in the region to inform evidence-based planning of the HWF.
Towards achieving this, Regional Office for Africa conducted a HWF survey in the African Region covering all its Member States. Thus, this paper aims to present the status of the HWF in the WHO Member States in the African Region 2018 and discuss its implications in the context of the African Regional Implementation Framework of the GSHRH.
Methods
Study design and setting
This study used a cross-sectional survey design with all 47 countries in the WHO African Region invited to complete a semistructured questionnaire.
Data collection
We collected data from January 2018 to April 2019 to update information on the stock and distribution of health personnel in the region. Before data collection, a tool was developed and piloted in four countries. The semistructured questionnaire (online supplemental file 1) was designed to obtain country information on the active health workers based on the International Standard Classification of Occupations nomenclature,3 sector (public, private for-not-profit and private for-profit) and the sources of the secondary information.
Supplemental material
Following the pilot and review, the tool was used to brief the heads of human resource departments in the MOH and focal points for HWF information in the MOH and health system focal points of the WHO country offices through virtual meetings. The virtual meeting focused on the objectives of the survey and use of findings, details of the tool and the methodology for administration. Subsequently, the tool and administration protocol was emailed to each country office focal point who worked closely with the relevant MOH stakeholders in completing the tool based on available secondary information. This secondary information was obtained from institutional registries, published HRH profiles and reports, and registration and licensing tables and reports from the MOH, Labour and Education, Public Service Commissions, national professional councils, and the private sector. The completed tools were validated in the countries by relevant stakeholders, approved and submitted to WHO by the heads of human resource departments in all 47 countries.
Data analysis
Completed questionnaires were collated in Epi Info V.7. After checking the quality of the data collected, including the cleaning of data and data entry errors, data were processed in Microsoft Excel, and descriptive and comparative analyses were done to present information on stock and densities of health workers by country and sector.
Analysis of missing data was done through triangulation of data from external data sources such as the WHO National Health Workforce Accounts platform of the WHO Global Health Observatory and the Africa Health Workforce Observatory of the WHO, Regional Office of Africa.
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Findings
Health worker stock
Table 1 presents the stock (an estimate of the total absolute number) of health workers categorised by physicians (generalists and specialists), nurses/midwives, dentists, pharmacists, laboratory personnel, community health workers, health managers and support staff, and other health workers. The physician specialists included surgeons, anaesthetists, cardiologists, emergency medicine specialists, ophthalmologists, obstetricians, gynaecologists, paediatricians, pathologists, preventive medicine specialists, psychiatrists, radiologists, resident medical officers in specialist training. Categorised under other health workers were medical records and health information technicians, medical technicians and equipment operators, optometrists and opticians, health management and support workers, paramedical practitioner, pharmaceutical technicians and assistants, physiotherapists and physiotherapy assistants, social workers, speech therapists, traditional and complementary medicine practitioners, etc.
Health workers by country and selected cadres in the African Region, 2018
Findings indicate that the total stock of health workers was approximately 3.6 million with 0.24 million physician generalists, 0.09 million physician specialists, 1.31 million nurses/midwives, 0.06 dentists, 0.09 million pharmacists, 0.37 laboratory technicians, 0.49 million community health workers, 0.42 million health managers and support staff, and 0.5 million other health workers. Thirty-seven per cent of the health workers in the 47 countries were nurses and midwives and they are followed by community health workers and other health workers at 14% each, health managers and support staff, and laboratory personnel (10%). Disaggregation by country showed that of the 3.6 million health workers in Africa, Nigeria had 26% at 0.94 million, South Africa had 13% at 0.45 million, and Algeria had 9% at 0.32 million. Ethiopia, Democratic Republic of the Congo and Kenya had 7%, 6% and 5% at 0.25 million, 0.22 million and 0.16 million, respectively.
Density of health workers
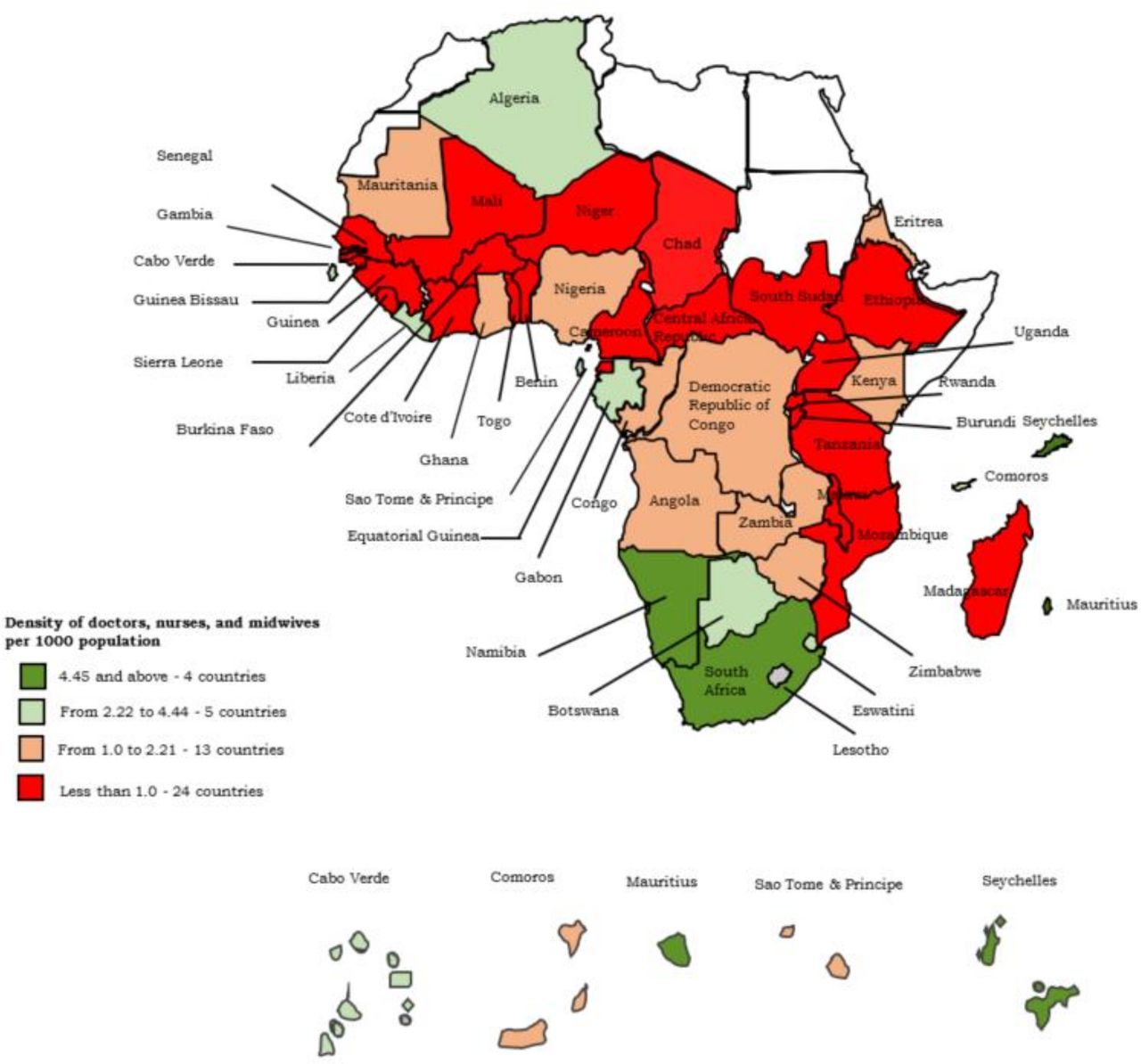
The densities in figure 1 were calculated based on the absolute number of doctors, nurses and midwives existing in a country calculated as a ratio to the total population (per 1000 population). The population estimates for each country were taken from the United Nation’s World Population Prospects 2019.18 The regional density of physicians, nurses and midwives were 1.55 per 1000 population, with Seychelles, Namibia, Mauritius and South Africa having thresholds above 4.45 physicians, nurses and midwives per 1000 population. Seven countries (Algeria, Botswana, Gabon, Cape Verde, Eswatini, Lesotho and Liberia) had thresholds between 2.0 and 4.0 doctors, nurses and midwives per 1000 population. Eight countries (Madagascar, Malawi, Togo, Benin, South Sudan, Chad, Central African Republic and Niger) had physicians, nurses and midwives per 1000 population thresholds of less than 0.5.
{kind=link}
Densities of physicians, nurses and midwives per 1000 population in the African Region.
Health workers by occupation and sector
The distribution of the health workers by occupation and sector are presented in tables 2 and 3. The categories of health workers with the high proportions in the public sector are the nurses and associates at 28%, community health workers at 15.3% and administrative and support staff at 12.9% (table 2). In the private for-profit sector, 26.9% were traditional and complementary medicine practitioners, 21.6% nurses and associates and 15.5% were community health workers. Nurses and associates, community health workers, administrative and support staff and laboratory workers comprised 30.6%, 13.6%, 12% and 10.4% of health workers in the private for non-profit sector, respectively.
Distribution of health workers by occupation in 47 countries in the African Region, 2018
Distribution of health workers by sector in 47 countries in the African Region, 2018
Sector-disaggregated data in table 3 show that 85% of all categories in countries were in the public sector, 11% in the private for non-profit and 4% in the private for-profit sector. The public sector had the highest proportion for all the categories except the traditional and complementary medicine practitioners where 79% of this staff category were in the private for-profit sector.
Discussion
In general, results for this survey show that there is still a shortage of health workers in the WHO African Region, as reported previously.2 4 8 There are low densities of doctors, nurses and midwives in most of the African countries and there are shortages across all HWF cadres, including doctors, nurses and midwives, dentists, pharmacists and laboratory technicians.7 The average density of 1.55 physicians, nurses and midwives per 1000 population in the African Region estimated in this survey is below the WHO SDG threshold of 4.45 health workers per 1000 population needed to achieve UHC.2 Evidence shows that the low HWF density positively correlates with poor health outcomes (including maternal and infant mortality) and high disease burden.2 4 19 Although several countries have made efforts to remedy this deficit of health workers, mainly through the implementation of HRH policies and plans in using global and regional frameworks, the complexity and scope of the issue make it difficult to resolve, and the number of countries under HRH crisis has not changed substantially.
Several factors have contributed to the HRH crisis in the WHO African Member States. Such factors include the inadequate training capacity resulting in low production of health workers, demographic conditions (rapid population growth), international migration, weak leadership and governance of HWF, career changes, poor retention of health workers, morbidity and premature mortality, lack of use of evidence for HRH planning and the limited capacity of the government to employ health workers in the public health sector among other factors.6 20
Results also show an uneven distribution of health workers within the WHO African Region with some of the countries having extremely low densities of health workers. This is compacted by the shortage of health workers and constrained resources in most of the countries within the region. The unequal distribution of health workers implies that many people in Africa, especially those most in need are having the least access to essential health services.21 22 Addressing the challenge of shortage and uneven distribution of health workers in the African Region is critical to building stronger health systems and ensuring universal access to healthcare services.6 23 It is important to conduct health labour market analysis periodically at national and subnational levels and use the findings to inform policies on the production, recruitment, retention and deployment of health workers.24 25 Distribution of health workers in service delivery can also be enhanced by applying the workload indicators of staffing needs tool26 that has been used in several countries in Africa to determine staffing needs based workload, rationalising the distribution of health workers and the recruitment of additional health workers to fill the gap.27–31
There were more health workers in the public sector compared with the private sector in countries within the WHO African Region. However, it should be noted that most of the countries that provided data in this survey had challenges to provide data for the private sector. This means that in some countries there was under-reporting of the data, while in other countries data was not provided at all—this was a limitation of this survey. The lack of reliable data from the private sector underlined a great need to get better data to enable clear situation analysis and projections of HWF needed in the future.4 Data from the private sector are frequently missing from the national HWF information systems and are urgently needed to complete a more realistic picture of the HWF at the national level.
Conclusion
In conclusion, this survey has demonstrated that the shortage and maldistribution of health workers in the WHO African Region remain a big challenge towards attainment of universal access to health services. Despite increased efforts to strengthen the HWF capacity in the WHO African Region, significant challenges persist in terms of adequate production in quantity and quality, employment capacity, deployment and retention of the existing health workers. This entails critical gaps in the delivery of essential health services to achieve health-related goals such as the UHC and SDGs. This calls for the need to increase substantially investment in HRH with contextual evidence in line with the current and future health needs. Member states should also implement interventions to increase preservice production and recruitment of health workers, as well as to improve their deployment and retention.
Data availability statement
All data relevant to the study are included in the article .
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors acknowledged the Human Resource Departments/Units in the Ministries of Health and all 47 country offices of the WHO African Region in facilitating the data collection and authorising the use. The authors also acknowledged Mr Jean Bernard Moussounda, Administrative Assistant at WHO African Regional office for assisting in the data capturing and data processing of the survey.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Press release
Footnotes
Handling editor Seye Abimbola
Twitter @adamahmat, @okoroaforsc
Contributors AA and SCO drafted the initial manuscript. AA, SCO, IK, JAA, JN, MMAI and JJSM conceptualised and conducted the analysis. All authors read and approved the final version of the manuscript. AA acts as the guarantor.
Funding This study was funded by WHO.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.