Article Text

Abstract
Based on real-time recording and reflection of responses to the COVID-19 pandemic, this article identifies the features of ‘community resilience’ across sites in rural Zimbabwe. The findings confirm the importance of local knowledge, social networks and communication, as highlighted in the literature. In addition, a number of other aspects are emphasised, including the importance of adaptable livelihoods, innovation and collective learning. Flexible adaptation was especially important for responding to lockdowns, as livelihoods had to be reconfigured in response to public health measures. Meanwhile, innovation and shared learning was vital for generating local treatment responses to the disease. In the Zimbabwe context, these adaptation and innovation capabilities emerge from a particular historical experience where resilience in the face of harsh economic conditions and in the absence of state support has been generated over years. This is often a more resigned coping than a positive, empowering, transformational form of resilience. While adaptation, innovation and shared learning capabilities proved useful during the pandemic, they are not evenly spread, and there is no singular ‘community’ around which resilience emerges. The article therefore argues against seeing ‘community resilience’ as the magic bullet for disaster preparedness and response in the context of pandemics. Instead, the highly differentiated local practices of adaptation, innovation and shared learning—across gender, age and wealth differences—should be seen as an important complement to public, state-led support in health emergencies and so are part of a wider, plural health system.
- COVID-19
- Health policy
- Health systems
- Descriptive study
- Qualitative study
Data availability statement
The real-time reflections on the pandemic over two years are available in a short, open access book (https://zimbabweland.files.wordpress.com/2022/06/learning-in-a-pandemic-book-hi-res.pdf).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Much discussion of ‘community resilience’ in the literature has failed to come up with a clear definition, partly because of a lack of empirical grounding of the concept.
WHAT THIS STUDY ADDS
Findings from rural Zimbabwe during the COVID-19 pandemic show that capabilities to adapt livelihoods in response to pandemic conditions were essential for survival, as was the ability to innovate and share learning on local treatments.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
‘Community resilience’ is not a magic bullet solution, as pandemic response capabilities are highly differentiated within ‘communities’ and ‘resilience’ may emerge simply from long-practised coping in harsh conditions. Instead, local capabilities for livelihood adaptation, innovation and collective learning/sharing need to be seen as complementary to other forms of health provision as part of a strengthened plural health system.
Introduction
‘Community resilience’ has emerged as a central feature of disaster and emergency planning and recovery.1–3 In the wake of the COVID-19 pandemic, building ‘community resilience’ has become a watchword for improving pandemic preparedness and boosting the capacity of health systems.4–7 But what does ‘community resilience’ mean and what might it look like on the ground?
This article draws on a 2-year process of engaged reflection in a number of sites across rural Zimbabwe during the COVID-19 pandemic. As the pandemic evolved, there were a series of phases associated with different variants. The first phase from the first identification of the SARS-CoV-2 virus in the country on 20 March 2020 lasted until early 2021, with an initial peak in early August and then again around Christmas/New Year. The second phase, largely associated with the Delta variant, was when severe illness and mortalities peaked in mid-July 2021. Finally, the third phase was associated with the Omicron variant and started in late 2021, continuing into 2022. Over this period, a series of strict lockdowns were imposed by the state through public health regulations issued as a series of amended statutory instruments.8 The first full lockdown started on 30 March 2020, with lockdowns of various levels of restrictiveness until February 2022.9 In each full lockdown period, movements were restricted, gatherings were banned, schools were closed and businesses were allowed to open only during restricted periods, as curfews were imposed. Lockdowns (at different levels) were justified in terms of public health measures and WHO guidelines were broadly followed. However, heavy-handed implementation was widely criticised, especially as it was linked to corrupt practices of officials as well as suspected political motivations linked to controlling opposition mobilisations.10
The pandemic is of course not yet over, but some estimate that around two-thirds of the population have been exposed,11 even though recorded COVID-19 cases to the end of May 2022 were only 252 398 and recorded deaths were 5503. A total of 41.4% of the country’s population had been vaccinated at least once by the end of May 2022.12 Recorded cases and deaths in Zimbabwe, as elsewhere in Africa, were lower than some expected, but there remain questions about the data. Unlike in some other parts of the continent, severe disease and mortality were faced in Zimbabwe in certain periods, although not as badly as in South Africa. In Zimbabwe’s case, the formal health system was unable to cope due to lack of staff and facilities, although measures were taken to streamline the pandemic response within districts and province, dedicating some hospitals as COVID-19 centres and additional funds were availed through the government as well as through donor support, both for healthcare and wider economic stimulus.13
Through our research, we were interested in finding out how rural people responded to the unfolding pandemic and what processes emerged over time. In this article, we track these responses across our rural sites and identify some of their core features. At the end of the article, we reflect on whether these responses together constitute ‘community resilience’. In the context of rural Zimbabwe during the pandemic, we conclude that ‘community resilience’ emerged through processes rooted in local relationships and collective agency, based on the building of knowledge, learning, sharing of ideas and innovating, both socially and technologically.
‘Community resilience’ has been defined in many different ways. Some take an instrumental view, identifying how ‘communities’ can assist the state in responding to emergencies.14 Others instead emphasise processes that result in ‘transformation’ or ‘empowerment’, building the capacities of communities to respond better in the future,15–17 including emphasising characteristics such as ‘courage’, ‘hope’ and ‘adaptability’.18–20 A systematic literature review concluded that there was no single definition of community resilience, as some studies focused on processes through which resilience is built, others emphasised outcomes or ways that negative consequences were avoided and still others identified attributes of those involved.21 Nevertheless, across the literature, a number of themes emerge, highlighting the importance of networks and relations, communication, the existing state of healthcare, the ‘mental state’ or embedded attitudes towards risk and uncertainty of the people involved, alongside wider governance and economic contexts for response.21
How ‘community resilience’ is defined depends on how the broader concept of ‘resilience’ is understood. This is much debated, with diverse framings offered. The classic notion of resilience from engineering science refers to the response of a system to a shock and its ability to return to its former state, both in terms of form and function.22 This engineering view is carried over into some of the more instrumental interpretations used in the global health and development literature, with the image of ‘bouncing back’ from disasters such as pandemics being central. Others see resilience in terms of adaption and transformation, changing the system in response to shocks and stresses.23 Here, the phrases ‘build back better’ or ‘leave no-one behind’ suggest that disasters and emergencies are not only moments to address vulnerabilities but also to engage with their causes and so addressing inequality and injustice.24 25
Many also argue that resilience does not exist simply as a system property, but that it has to be built through a process of assemblage of practices and relationships.26 Resilience is therefore emergent from social, political and, crucially, historical conditions and cannot simply be ‘designed’ by external programmes.27 This suggests looking at the ‘vernacular’ features of resilience, exploring how strategies of coping and response are constructed by different people, rooted in cultural practices.28
The political contexts of ‘community resilience’ are important too. Some argue that narratives of resilience—and perhaps especially those that emphasise reliance on ‘communities’—are reflections of a ‘neoliberal’ standpoint, where the state and other authorities wash their hands of responsibility for care and support, transferring responsibilities.29–31 While celebrating local knowledges and capabilities, those who in the past might have assisted at times of crisis now rely on other unpaid, voluntary associations to do this work, thus reducing costs and increasing efficiencies. Underfunded state services thus are supported in terms of core functions such as surveillance, communication, trust building and mobilising responses.
The idea of ‘community resilience’ also begs the question of what is the ‘community’.32 This is often left rather vague, conjuring up a uniform localism that erases power relations, social differentiation and conflicts within ‘communities’. It is no surprise therefore that such interventions are often blind to questions of difference—of class, gender, ethnicity, age and so on—and sometimes get captured by powerful figures within ‘communities’, such as chiefs or other local leaders, upsetting the idea of a standardised ‘community’ resilience.
All these themes emerged within our work in rural Zimbabwe and are highlighted in other research on the COVID-19 pandemic in Zimbabwe and Africa more broadly.33–35 This means that defining what community resilience is highly challenging, as we discuss at the end of the article. The next section outlines our methodology.
Methods
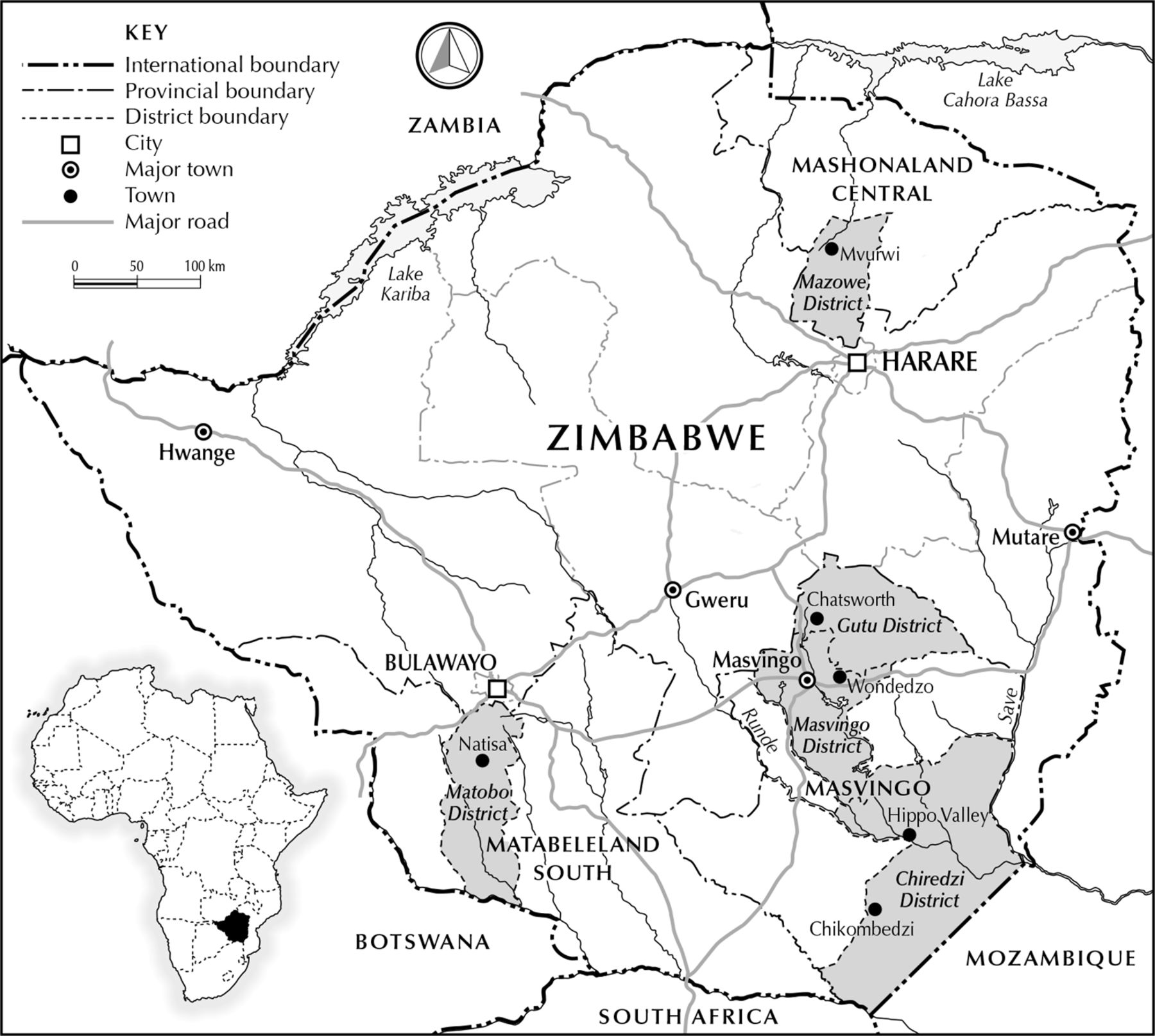
This study explores the response to the COVID-19 pandemic in rural Zimbabwe across six sites (figure 1) between March 2020 and April 2022. Each month the field-based team reported on observations, informal interviews and discussions. These reports were collated and a summary was posted on a blog site (zimbabweland.wordpress.com/tag/COVID-19/). In total, 20 blogs on COVID-19 responses were produced, which are now available as a short, open access book (https://zimbabweland.files.wordpress.com/2022/06/learning-in-a-pandemic-book-hi-res.pdf). All blogs were shared widely, including via local newspaper articles. In sum, the analysis process was iterative and inductive, emergent from engaging with the qualitative material and reflecting on field experiences. In our reflection discussions, each month we would identify emerging themes; these included the role of lockdowns, the importance of indigenous medicines and women’s and young people’s experiences, for example. Combined with a detailed analysis of all the blog material (34 455 words in total) for key terms and concepts, these provided the basis for our collective qualitative analysis of ‘community resilience’ at the end of the process, allowing us to cluster findings around the overarching categories of ‘adaptable livelihoods’ and ‘innovation and learning’ (see below).
{kind=link}
Map of study areas.
Our rural study sites stretch from the very dry south of the country (Chikombedzi and Matobo) to the sugar estates (Hippo Valley), to medium-potential agricultural areas in Masvingo province (Wondedzo, Chatsworth) and to the tobacco growing areas to the north of the capital Harare (Mvurwi) (figure 1). In all settings, agriculture is the primary source of livelihood, whether in the smallholder communal areas and A1 resettlement sites or the larger-scale farms.36 In all sites, government health facilities existed, ranging from rural clinics to district hospitals. In addition to regular discussions with farmers, traders, small-scale miners and others on livelihood responses to both the disease and the public health measures imposed, we also interacted with nurses, health technicians and village health workers over the 2 years, exploring how the health system operated and how links with ‘community’ efforts were forged during the pandemic.
We did not start with prior views, nor hypotheses to test, nor did we introduce particular categories or terms, such as ‘community resilience’. Instead, we aimed to have an open-ended conversation within and between sites to learn in as unconstrained manner as possible. In this way, we pursued a tradition of located ethnography and inductive research central to social anthropological research, although in this case involving ‘insiders’ to the society as the main field researchers. As in all research, we of course came with our own biases and interests, for example, we were interested in outcomes for livelihoods and the intersections with agriculture in particular. We aimed to counter any biases through our collective discussions, with all of us probing and challenging findings before compiling the results in a blog summary. During these discussions, comparative insights arose with insights from different sites across the country being set against each, again highlighting the diversity of experiences both over time and across space in ways that a more restrictive study would not allow.
The authors include five extension workers who are also farmers, two full-time farmers and one university professor; all but one author lives in the study areas, but some of us have worked together over several decades in these sites, making the research process rooted in long-term engagement and trust relationships, with no challenges faced in any of the field settings. This collaboration offered the opportunity for a very different type of insight to standard, ‘tried-and-tested’ conventional methods, shifting the gaze from the standard, hypothesis-driven external survey approach to understanding health responses from a more embedded perspective, based on local understandings and commitments. The result is, we hope, a more nuanced account of what happened during the pandemic, identifying themes iteratively over time in ways that would not have emerged if a predefined frame was imposed. We offer our perspectives in the spirit of an approach that, as a result, shifts the epistemological and ontological frame and also the pattern of authorship, in ways that challenge the conventional style of global public health research (see online supplemental author reflexivity statement).37
Supplemental material
Patient and public involvement
As discussed above, the study involved real-time reflection on the pandemic, with an author group who were resident in the study areas. Being members of ‘the public’ and in some cases ‘patients’, the research was led by and involved local people in all sites. Through the research community members with whom the field team engaged helped frame the research, providing input to the sequential process of deciding on research foci over the 2 years. The results were shared as they emerged through the published blogposts, providing the basis for reflection on and adaptation of the study. The overall findings are being shared through a compilation of the blogposts in a book shared with both local community members and health professionals in all sites.
Results
In the following sections, we share the results around two themes that emerged from our collective analysis of the qualitative data: adaptable livelihoods and innovation and learning. These allow us to tell the story of the pandemic from the perspective of rural people. Through this discussion, we draw out the key elements of what might be termed ‘community resilience’.
Adaptable livelihoods
COVID-19 is a disease of crowds and congregation.38 This makes quite a lot of necessary daily activities risky, and rural people became well aware of this. Following the first recorded case in Zimbabwe in March 2020, knowledge about the disease spread quickly and most started early on a routine of personal hygiene, wearing masks and distancing. There was of course plenty of misinformation too pushed via foreign websites often with a religious orientation. Before the virus arrived in the country, the minister of defence even fell prey to such arguments, claiming that the disease was a divine curse on the West for its continued sanctions on Zimbabwe.39 Few repeated such claims, but other sources of misinformation around the risks of vaccines, for example, were vigorously pushed across Facebook, WhatsApp groups and in general conversation. As a nurse commented, “When vaccines were introduced, we were also scared of them. Some messages on WhatsApp were really negative”.40 In fast-moving, uncertain situations like in the midst of a pandemic, people must process diverse sources of information and make choices. At the beginning, with fear and anxiety in the air, people were less confident about managing the disease, but this changed over time: “At first, we feared the disease. Then it was just in Harare, but cases were rising. People ran away from visitors from South Africa. Later, yes, people got sick, but after steaming for a few days it was over”.41
As the pandemic progressed, people had to make judgements between risks of the disease and the imperatives of survival. This became especially acute in mid-2020 with the repeated lockdowns striking hard.42 43 Lockdowns caused great hardship. Farmers could not get their farm produce to market, traders could not restock their supplies, children were not going to school and took to multiple vices, attendance at funerals and weddings was restricted and churches were often closed. This caused stress and unhappiness, as well as economic challenges. As Mr M argued, “If we continue with lockdowns there will be serious hunger”.44 In negotiating this period, complex trade-offs were involved. Should a crop be abandoned? Could a roadblock be circumvented or a bribe paid? Could kids be supported to do something other than hang around, drinking and taking drugs? Throughout the pandemic multiple precarities intersected, balancing protecting health in conditions where the risks were not known with the immediate requirements to farm, market produce and supply food for the family.42 43 45 As Mrs M explained, “We are worried about lockdowns, as they affect everyone. We cannot afford blanket lockdowns anymore. We cannot live like that”.46
Over time and particularly towards the end of 2020 and into 2021, an improved understanding of COVID-19 disease risks emerged. When local outbreaks occurred in any of our sites, people could quickly point to a particular funeral, a market gathering or the potential for a certain type of transportation that spread the disease.47 People’s knowledge of epidemiology was impressive and they knew how the virus transmitted and could adapt behaviour accordingly.48 49 However, heavy-handed lockdowns persisted, often with a political motivation, and harsh sentences for infringements were handed out.50 People had to learn ways to circumvent such measures—and officials were often complicit, even if still accepting bribes, as they too were suffering the harsh consequences of lockdowns. As MM explained, “You needed letters to move to Harare to sell. But you end up going late, as you have to run around finding the travel permits. Our crop was badly affected. It was difficult to bribe the police, as there were soldiers there. And we didn’t have money. We could only bribe with tomatoes! We got arrested for not masking and paid 1000 Zimbabwe dollars each time”.51
This was not a rejection of public health, but a realisation that the measures were, in their words, ‘killing us’. As people explained, “we are good at surviving, but things are really tough”.42 52 Since the mid-1990s, the economic conditions in Zimbabwe have been disastrous, and this accelerated in the 2000s with hyperinflation and economic chaos, resulting in major impacts on the public health system and the morale of public health professionals. When the pandemic struck the national economy was in deep trouble, with parallel exchange rates, rising inflation and limited finance in rural areas.53 People were—and had been for some time—largely on their own, as state support for rural development had declined dramatically. This survival mentality—some might say ‘resilience’—had become embedded for many years before the pandemic.
A sense of resilience was most pronounced in our resettlement area sites, where people had been allocated land following the 2000 land reform. However, the follow-up support from the state to regenerate the agrarian economy had been minimal and people had largely built up their farms, created markets, repaired roads, improved services and enhanced their livelihoods through their own labour and investment.54 A sense of stolid independence and autonomy prevailed, with local systems of support and redistribution providing some form of safety net for those who were doing less well.
The pandemic therefore struck an economic setting that was often self-reliant, even if market oriented and dynamic. Links to small towns, contracting firms and market networks were all vibrant. Many in the nearby communal areas were reliant on the land reform farmers, both for labour hiring and for food provisioning. Networks of support stretched further too as resettlement farmers provided support for their relatives in town, now out of employment due to the pandemic.43
These were not uniform settings as there was much differentiation between richer and poorer farmers, men and women and young and old.55 Social relations that bound people together for farming were also important during the pandemic, so relations of kin in clusters of households were important for caring and support, just as they were for helping with draft power or farm labour. Church groups provided forms of solidarity especially for women, while savings clubs, marketing groups and other informal associations also were important for information sharing and support during the pandemic.56 While people identified with a particular location, these were not homogenous communities by any means.
By the end of 2020, there was an increasing flow of people to rural areas and especially to the resettlement areas where land availability was higher. Migrants included the unemployed from Zimbabwe’s urban areas and also those who had been retrenched due to the pandemic or had become sick in South Africa and returned home.42 Arable areas were subdivided and offered to sons and daughters, as well as other relatives. These patterns of migration reshaped land access, labour and demographic profiles in the rural areas and so the social relations of ‘communities’ during the pandemic, resulting at times in conflicts as new people were accommodated. Rural land, especially in the land reform areas, became an important livelihood safety net in the absence of other support. Gaining access to land was therefore crucial to survival and was central to the draw of migrants to rural areas, many of whom have stayed. Even as lockdowns eased, the possibilities of gainful employment in urban areas or in other countries remained limited.57
In a highly constrained economy, making a living from farming is nevertheless hard and in our different sites contrasting strategies were seen. 2019–2020 was a drought year, making it essential to market as much as possible. Irrigated horticulture is important across our sites and many return migrants, able to purchase irrigation equipment, could make a living on small plots if water access could be secured. They were joined by women, who have long led horticultural production and marketing in our sites. As people explained, “everyone is a gardener now”.47 In the high-potential area of Mvurwi, tobacco remained the dominant cash crop throughout the pandemic, supported for some by contracting arrangements with private companies. In all areas, rainfed maize is the major food crop and production varied widely across sites and between years through the pandemic. In 2020 harvests were low, but in 2021 with good rains granaries were full and much maize was sold for cash both to the state grain marketing board and private traders.
The differences in economic fortunes across the 2 years were stark. In 2020, diversification for survival was necessary due to the combination of a poor harvest and heavily enforced lockdowns. Livelihood diversification in 2020 included a focus on dry season horticultural sales, although lockdowns massively restricted market access and the growth of off-farm activities including small-scale mining for gold and amethyst.47 While livelihood diversification has long been a feature of rural responses to shocks, the pandemic—and especially the resulting lockdowns—made such strategies essential. However, later in 2020 and through 2021, with a much better harvest, people had found ways around many restrictions, and they adopted a range of marketing tactics, including selling produce from cars and open top trucks, which could be moved if the police came. Night markets flourished to coincide with the time when police were less present, and transportation happened along back routes, avoiding roadblocks, sometimes involving motorbikes going across country to connect with cars. As one informant explained, “It may be illegal, but it’s about survival”.58
In the face of uncertainty—perhaps less the disease itself for much of this time, but the uncertainties that surrounded state enforcement of lockdowns including the imposition of often punitive fines for breaches of regulations—people had to follow highly adaptable livelihoods, always creating new opportunities despite the risks.59 Over time, people largely took the management of the pandemic into their own hands finding new routes to assuring livelihoods. This meant that people had to innovate through continuous experimentation, learning and sharing, a central theme identified from our regular reflections that is discussed next.
Innovation and learning
While farmers were innovating around forms of transport and styles of marketing during the pandemic in order to get around lockdown restrictions, many rural dwellers were also experimenting with COVID-19 treatments. Although cases were low for most of the period, there were times when people needed treatment as infections spread.
The Delta wave in mid-2021 was the most acute, and some deaths were experienced in our sites for the first time. No longer was this the urban, rich person’s disease, but now people had to respond themselves, yet with very limited health facilities available.60 Going to a clinic would maybe get you some paracetamol, but it could also get you clamped into a quarantine facility without support from relatives and without local remedies that people had begun to rely on, so alternatives had to be sought.
Innovation around local treatments started early in the pandemic, with astute business people selling herbal concoctions for COVID-19 treatments in towns.57 Many in the rural areas saw these options and began to experiment themselves. A fairly standard mix of remedies emerged, centred on lemons, ginger and onions for teas and compresses to assist with breathing, which was the biggest problem with the early variants. These had long been used for respiratory problems in winter, but there was now a rush on these products and many began to produce these in their gardens for wider sale. WhatsApp messages were full of what the right mix or application was and how steaming should be conducted. Traditional remedies, including roots and leaves, were widely available. Zumbani/Umsuzwane (Lippia javanica), for example, was extensively used and became commercialised as a tea, soon available in shops. Imported remedies, notably from China, were sold as tinctures and drops to help with breathing, including the widely used brand, Tsunami.61
As the pandemic shifted, the remedies changed. The Omicron variant crossed the border from South Africa in November 2021, and people in our southern sites soon realised that this was a different disease; more like a influenza and less dangerous with less impact on the lungs, they explained. New concoctions were suggested—including a mix of chilli with Coca-Cola to clear the nose—and such remedies again were quickly shared through WhatsApp groups. Questions are of course raised about their therapeutic efficacy, but in the absence of biomedical alternatives such options were widely used. By the time the Omicron wave had hit villages further north, many already were equipped with knowledge about the symptoms and ideas about what remedies worked best. The speed of experimentation, learning and sharing had increased during the pandemic. In this case, it was only a matter of weeks before knowledge spread across the country.
As the pandemic progressed, people had also become more discerning about shared information. Trusted sources—a particular family member, a certain local leader or church person—were noted and others were rejected. Many of the more outrageous claims from US evangelists or Nigerian prophets were regarded with much more circumspection. Practical advice on treatments were largely shared on informal WhatsApp and Facebook groups and spread far and wide, including to relatives in the diaspora who had yet to meet Omicron.62 Dealing with plural information sources—what the WHO has called the ‘infodemic’63—has been an important part of daily life and people have become more practised at sifting, judging and assessing. As Mrs M observed, “The WhatsApp groups tell us everything, but you don’t know who to believe. We rely on each other to experiment with and test treatments”.64 Practical experimentation has been important, as people could demonstrate and share what actually worked. The array of treatments that accumulated over time certainly made people more confident in confronting and managing the virus and dealing with the uncertainties that it brought.65
A plural health system evolved, involving many different actors. The clinics and formal health provision were certainly part of this, but most people relied on informal networks among families and between local ‘experts’ in the villages. Some people became well known for advice on particular herbal treatments, while n’angas (traditional healers) and spirit mediums provided insights from their connections with the spirit world.66 In looking for help, people would often move between different sources of advice and support, depending on their condition and the severity. For those trained in formal medicine, this was sometimes seen as a rejection of ‘science’, but for others this was a sensible, diversified response to an unknown disease context. Nearly everyone today has a good stock of herbs and local medicines in their homes just in case, and countless lemon trees have been planted, along with ginger, onions and garlic.67
This local innovation emerged in a context where alternatives were few. The formal health services were limited, the consequences of years of neglect, and people had to make do and get by.68 Authorities were not trusted to provide support and many suspected political motives and opportunities for elite accumulation during the lockdowns. In the context of extreme uncertainty and lack of external support, a pattern of cultural-rooted resourcefulness was needed.56 While some local remedies may have had no effect and some other could have even caused harm, the psychological importance of such responses cannot be under-estimated, as they gave, as they gave a sense of agency in a time of extreme turbulence and threat when people felt very much on their own. Through the pandemic people therefore had to draw on their resources, skills and networks to experiment, learn and share. As Richards observes, “epidemics are group learning experiences”38 and the COVID-19 pandemic in Zimbabwe was no exception.
Discussion
Was this experience in rural Zimbabwe an example of ‘community resilience’? Certainly, adaptation and innovation, as described as the two central themes in the section above, are key to generating resilience and the ability to withstand, adapt to and transform through shocks and stresses. But we have to be more cautious in concluding that ‘community resilience’ is the solution to pandemic response.
First, we must appreciate that the adaptable livelihoods and innovation capabilities observed have emerged from a particular historical context—in this case, a long-term neglect by the state of rural areas, massively reduced capacity of state services, including health, and an over-riding sense that people must survive in the absence of a supportive, developmental state. Since the 1990s, and especially through the 2000s, this has been the case in Zimbabwe, with the sense of abandonment and ‘disposability’ evident, perhaps especially in times of disease and emergency.69 It is therefore a resigned resilience due to low expectations, not necessarily a positive vision as sometimes portrayed.
Second, we must ask whether this ‘resilience’ is a community-wide feature? A simplistic notion of ‘community’ is definitely challenged by our findings. Communities are highly differentiated across many axes. Networks, relationships and associations form around an array of activities—marketing produce, trading, attending churches, socialising at beer parties and so on—and those participating may be quite particular. These have long been features of rural settings, but the pandemic emphasised the importance of existing relationships and forms of solidarity. Also, communities are not just ‘local’ as they stretch beyond the boundaries of the immediate area, connected through WhatsApp groups to other relatives, including in the diaspora. Despite the costs of mobile phone data in Zimbabwe, these relationships are seen as essential, binding together a ‘virtual community’ central to the pandemic response. All these relationships and forms of solidarity and connection may generate resilience—and together this may be seen as ‘community resilience’, but it is however a highly differentiated ‘community’.
That said, in relation to the literature on ‘community resilience’, there are clear resonances with our findings.21 70–73 Local knowledge and social relations are central in relation to the development of COVID-19 treatments, for example, and so also is communication and information sharing. The rapid response to the Omicron variant in late 2021 is witness to the efficient way information spread; indeed, knowledge about the variant and the ways it presented, as well as options for its treatment, spread faster than in the published literature and so was ahead of ‘science-based’ policy advice. The regular sharing of treatments, the result of local experiments and general learning through WhatsApp groups were important throughout the pandemic response.
A key dimension of knowledge and communication is trust, and it is the exchanges among family and friendship groups that are trusted. Information was shared, discussed and digested in various fora. Women would discuss in church groups; others would assemble at markets or auction sites, while men would debate at beer parties. During lockdowns, of course all such gatherings were prohibited and people had to find other ways of interacting, very often informally in family groups. As we have discussed, through the pandemic people became very selective about information use. They listened to health messaging and took up hygiene practices, masking and so on, but in ways compatible with their lives. They listened to prophets, priests and traditional leaders and followed advice, much of it reflecting the official line, but again highly selectively. Advice had to be in their judgement sensible and proportionate.
While the advice on the first lockdown was accepted as people were scared and the pandemic was a complete unknown, later people rejected lockdown advice as it was seen to be inappropriate and politicised.74 Trust in different people varied. There were some living in our study sites who were always consulted and some members of WhatsApp groups were seen as reliable, but almost universally people reserved much scorn for politicians and party-connected elites as some were seen to be taking advantage of the pandemic to make money.
When conditions are so uncertain and people have to survive, this means that resilience in the face of the crisis had to be actively developed, assembled through different knowledges and practices as part of an evolving process. Unable to rely on service provision or safety nets from the state and largely distrusting state authority in any case, people had to improvise themselves. However, in the Zimbabwe context, this was not a postpolitical resilience of ‘coping’ or ‘bouncing back’, but ‘community resilience’ involved collective agency, building knowledge, sharing ideas, learning about how to respond and innovating, both socially and technologically, with all these resilience-building processes rooted in local relationships.
People were not operating completely independently, however. There were important relationships with the local health service, even in its much-deteriorated state. Village health workers and environmental health technicians are members of these communities, and the nurses based at clinics also live in the area, even if they do not come from it. These health workers follow the same practices, are part of the same discussion groups and hold the same fears, anxieties and suffered the same traumas during the pandemic. As a nurse from Chikombedzi hospital put it, “When I come home, I leave my uniform in the bathroom, and of course the whole family takes local remedies”.75 In the context of deep uncertainty about the disease, trained health workers will draw on a plural health system, just as everyone else, consulting herbalists, taking advice from evangelical preachers, as well as responding to formal health messages. All parts of this health system are important in supporting physical, spiritual and mental health and so are vital for ‘resilience’.
The important dimension of mental health came through strongly in our discussions. The pandemic caused much stress—people worried continuously about their ability to sell produce, trade goods and feed their families. Lockdowns came suddenly and were heavily enforced. Breaking the law in order to survive does not come easily; avoiding the police roadblocks in order take tomatoes to market meant long walks avoiding the road, often at night. With schools closed for long stretches, children became unruly and sometimes got involved in petty theft and other crimes. Young girls became pregnant and there was a rise in early marriages. All these challenges took a major toll on families and parents often did not know how to cope. In the absence of schools and other services, family and community networks of support therefore became important for psychological resilience.
People in rural Zimbabwe of course did not face a full health emergency. Disease came in waves and the effects were patchy. There was illness and death, but this was not significant in our study areas. Ironically, much of the ‘resilience’ capabilities were focused on coping with and getting around public health measures—notably lockdowns—that were supposed to provide protection against the disease. The resilience to cope with market closures, transport restrictions, incessant roadblocks, bribes and fines generated a feeling of resignation and despair. Across our discussions, there were common refrains: When would this be over? When could we live with the virus and use our treatments to get on with life? We eat healthily, live outdoors, do hard work in our fields, we live with diseases, we always have! We just have to get on with our lives and get rid of these lockdowns, otherwise we will starve.76
However, such a spirit of self-reliance, bolstered by local capabilities to adapt, innovate and treat illness, would surely be upset if the pandemic had caused more extensive, severe illness and mass death. Under such conditions, autonomy and independence would not be enough and people would have looked for more external, state support to assure resilience.
Conclusion
Pandemics are an opportunity to rethink the way health systems operate.77 However, the increasingly popular idea of ‘community resilience’ must not be seen as a magic-bullet solution to pandemic response. Instead, resilience building must always be developed in relation to local contexts and as part of a wider suite of responses. Our findings from Zimbabwe show how responses to COVID-19 occurred in the context of a weak health service, an economy in a dire state and at a time when trust in the state—or more precisely politicians—was extremely low.
Across our study sites, we observed a resigned resilience—or coping—centred on autonomous local capabilities. Such forms of resilience were however highly differentiated within a ‘community’, and community connections also stretched beyond a particular locality, as wider networks were drawn on. While the moniker ‘community’ is problematic and ‘resilience’ of course is an extremely difficult concept to pin down, we conclude that features of what is referred to as ‘community resilience’ in the wider literature were present in our study areas during the pandemic.21 These included the importance of local knowledge and innovation; the significance of networks and relations within and beyond the community; attitudes of local people towards risk and uncertainty; levels of trust in authority and the state; and the wider economic and political context affecting health provision. Our findings highlighted in particular two central elements that contributed to resilience during the COVID-19 pandemic in rural Zimbabwe: adaptable livelihoods and innovation and learning under uncertain conditions, both emerging from a spirit of independence, autonomy and self-reliance.
In generating such resilience, we saw the importance of a plural health system, involving many actors—formal and informal. This was not just ‘the community’, but a wider mix of players, including traditional healers, herbalists as well doctors, nurses and other health professionals. All were connected around a complex, adaptive pandemic response. While such a plural system had long existed, it came into its own during the pandemic, as uncertain conditions had to be confronted at a local level.
Based on our real-time reflections across multiple sites over 2 years, we conclude that there are no simple solutions to improving ‘community resilience’. With a different type of shock, disaster or emergency, the options may look very different. We conclude that ‘community’ responses must build from a solid foundation of primary public healthcare at the local level, yet in Zimbabwe, capacity has declined since the heyday of public health provision in the 1980s.78 79 As Farmer noted, nothing can be done without the ‘staff, stuff, space and systems’ that make health systems function.80 ‘Community resilience’, centred on local adaptation, innovation and learning, must be seen as part of a plural health system. Being prepared for the next health emergency—which may take a very different and more severe form—requires building all the elements together.
Data availability statement
The real-time reflections on the pandemic over two years are available in a short, open access book (https://zimbabweland.files.wordpress.com/2022/06/learning-in-a-pandemic-book-hi-res.pdf).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. This study was conducted under the auspices of the Agricultural Policy Research in Africa project (https://www.future-agricultures.org/apra/) and was approved through the Institute of Development Studies ethics approval process. The study involved interviews and informal interactions. Participants gave informed consent to participate in the study before taking part. Confidentiality and anonymity were assured and all interviews were undertaken with prior consent according to ethics guidelines. However, since ‘researchers’ were also being ‘community’ members, the relationships between research participants contrasted with conventional, externally driven, extractive research.
Acknowledgments
The research is part of a long-term study of land, agriculture and livelihoods in Zimbabwe (www.zimbabweland.wordpress.com). All perspectives presented are personal views based on research evidence and do not reflect the views of employers. The authors would like to thank all those in the field study site for their ongoing engagement with the work, as well as Professor Hayley MacGregor and two anonymous reviewers for comments on earlier versions of this paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Stephanie M Topp
Twitter @IanScoones
Contributors All authors contributed to the paper and have approved its content. The fieldwork was carried out by all authors, with field team coordination led by FM. IS drafted the paper and led the process of writing and revision. This paper is a collective output, with all authors contributing to data collection and analysis. This article emerges from a long-term collaborative effort. As explained in the main text, different authors took on different roles, but all are recognised equally with an alphabetical listing of authors. There are no lead authors. In terms of roles, IJB, JM, MMa, BM, MMu and VS were based in the study sites and collected data on a monthly basis. This was relayed to FM via WhatsApp messages/conversations and the findings were compiled together with IS, who wrote a blogpost for each reflection period. Based on these inputs, IS drafted the paper, which was reviewed and checked by all team members. A period of fieldwork in February 2022 complemented this process, with interviews undertaken by FM, JM, MMa, MMu, VS and IS. The core team that contributed to this paper (JM, FM and IS) has been working together since the early 1990s and has been publishing together since then. IS acts as the guarantor and is responsble for the overall content.
Funding This work took place under the auspices of the FCDO-funded APRA programme, with linked permissions/ethical clearance. Research and writing were also supported by the ESRC STEPS Centre and the ERC-supported PASTRES research programme (Grant: 74032).
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.