Article Text

Abstract
Introduction Although hospitalisation remains the preferred management for neonatal sepsis, it is often not possible in resource-limited settings. The Home-Based Newborn Care (HBNC) study in Gadchiroli, India (1995–1998) was the first trial to demonstrate that neonatal sepsis can be managed in the community. HBNC continues to operate in Gadchiroli. In 2015, WHO recommended community-based management of neonatal sepsis when hospitalisation is not feasible but called for implementation research. We studied the implementation and effectiveness of home-based management of neonatal sepsis over 23 years in Gadchiroli.
Methods In this cohort study (1996–2019), community health workers (CHWs) visited neonates at home in 39 villages in Gadchiroli, India. CHWs screened, diagnosed sepsis and offered home-based antibiotic treatment if hospitalisation was refused. We evaluated the implementation outcomes of coverage, diagnostic fidelity and adoption. We assessed the association between treatment type and odds of neonatal death using mixed effects logistic regression. Time trends were analysed using the Mann-Kendall test.
Results CHWs screened 93.8% (17 700/18 874) of neonates (coverage) and correctly diagnosed 89% (1051/1177) of sepsis episodes (diagnostic fidelity). Home-based management was preferred by 88.4% (929/1051) of parents (adoption), with 5.6 percent of total neonates receiving antibioties at home. Compared with neonates treated at home, the adjusted odds of death was 5.27 (95% CI 1.91 to 14.58) times higher when parents refused all treatment, 2.17 (95% CI 1.07 to 4.41) times higher when CHWs missed the diagnosis and 5.45 (95% CI 2.74 to 10.87) times higher when parents accepted hospital referral. Implementation outcomes remained consistent over 23 years (coverage p=0.57; fidelity p=0.57; adoption p=0.26; mortality p=0.71). The rate of facility births increased (p<0.01) and the sepsis incidence decreased (p<0.05) over 23 years.
Conclusion Implementation of home-based management of neonatal sepsis was sustainable and effective over 23 years. During this period, the need for home-based management in Gadchiroli is declining. Home-based management is advised where sepsis remains a major cause of neonatal mortality and hospital access is limited.
- other study design
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The Gadchiroli field trial (1995-1998) showed that neonates with suspected sepsis could be effectively managed by trained Community Health Worker.
In 2015, WHO recommended community-based management of neonatal sepsis when referral to a health facility is not possible but acknowledged the need for implementation studies to ensure long-term feasibility in real-world settings.
WHAT THIS STUDY ADDS
Home-based management of neonatal sepsis has been successfully sustained for 23 years in Gadchiroli, India using targeted implementation strategies, and the mortality rate of neonates treated at home has remained low.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Home-based management of neonatal sepsis should be implemented in areas where sepsis remains a major cause of neonatal mortality and hospital access is limited.
Implementation strategies that focus on task-shifting, education, financing and quality management are needed to sustain home-based management of neonatal sepsis.
Introduction
Every year, >500 000 neonates die from pneumonia, sepsis and meningitis.1 Hospitalisation with inpatient antibiotic therapy remains the preferred treatment option for neonates with a possible serious bacterial infection (collectively referred to as ‘sepsis’).2 However, hospitalisation is often not accessible, acceptable or affordable for families living in resource-limited settings.3 Without hospitalisation, neonates in resource-limited settings may not receive treatment, resulting in potentially preventable morbidity and mortality.
In 1999, the Home-Based Newborn Care (HBNC) field trial in Gadchiroli district of Maharashtra, India was the first to report that community-based management of neonates with sepsis reduced neonatal mortality.4 As part of a broader home-visitation programme for mothers and their newborns, trained female community health workers (CHWs), working under medical supervision in 39 villages, used a clinical algorithm to screen neonates for sepsis.5 If a CHW diagnosed sepsis, she advised hospital referral. However, if parents refused referral, she offered home-based management to eligible neonates, including 7–10 days of injectable gentamicin and oral co-trimoxazole. From 1996 to 2003, >90% of eligible families accepted home-based treatment, and the mortality in the 39 villages decreased by 56%.6
Since the HBNC field trial, there have been additional clinical trials in South Asia and sub-Saharan Africa demonstrating that outpatient therapy with simplified antibiotic regimens is efficacious for neonates with sepsis.7–10 As a result, in 2015, WHO endorsed community-based management of young infants with sepsis when hospital referral is not feasible.11 However, WHO recommended ongoing implementation research to ensure effective local adaption and sustainability.11
The non-government organisation Society for Education, Action and Research in Community Health (SEARCH), which conducted the HBNC field trial, has continued to provide HBNC in the same 39 villages in Gadchiroli, India since the trial ended. During this time period, there have been changes to Gadchiroli’s sociodemographics and governmental health services, which have the potential to impact the implementation of home-based management of neonatal sepsis. Therefore, the aim of the current study is to assess the long-term implementation and effectiveness of home-based management of neonatal sepsis in Gadchiroli, India over a period of 23 years (1996–2019).
Methods
The study design and methods of the original HBNC field trial have previously been published.4 12 13 The study setting of Gadchiroli is an economically poor, predominantly rural district, in the state of Maharashtra, India. Health services are few and ill developed. SEARCH conducted the original field trial of HBNC and has continued to deliver home-based interventions and monitoring in the Gadchiroli field area since the end of the trial. For the current implementation study, all neonates who spent all or part of the neonatal period in 39 villages in Gadchiroli, hence, were eligible to receive HBNC, from September 1996 to March 2019 were included.
Implementation strategies
The implementation of home-based management of neonatal sepsis involved multiple strategies recognised in implementation science.14
As the first strategy, the tasks of diagnosing and treating sepsis were shifted to CHWs from the usual method of physician-based diagnosis and treatment. Trained CHWs were advised to make 8–14 home visits during the neonatal period, depending on the neonate’s health status, birth weight and gestational age at birth. Additional visits were made if a family had a concern. CHWs assessed prespecified signs of neonatal sepsis at each home visit (online supplemental appendix A).6 Sepsis was defined as the simultaneous presence of two or more clinical criteria. The criteria were modified in 1998 to improve the sensitivity and specificity.5 All neonates who were diagnosed with sepsis by the CHW were advised to be referred to a hospital. If families refused the referral, home-based management of sepsis was offered after obtaining written informed consent. Home-based management included keeping the baby warm, ongoing breast feeding and a regimen of syrup co-trimoxazole and intramuscular gentamicin. Specifically, all neonates with sepsis received syrup co-trimoxazole (sulfamethoxazole 200 mg+trimethoprim 40 mg/5 mL) 1.25 mL two times per day for 7 days. Preterm neonates with a birth weight <2500 g received intramuscular gentamicin 10 mg/day for 10 days while full-term neonates or those with a birth weight ≥2500 g received intramuscular gentamicin 15 mg/day for 7 days. Gentamicin was divided in two daily doses, except from June 1998 to January 2001 when it was administered once daily. CHWs administered gentamicin in the anterolateral thigh with a single-usage 1 mL syringe and needle.4 6
Supplemental material
For neonates receiving home-based management of sepsis, CHWs made twice-daily visits (except from June 1998 to January 2001 when they made once-daily home visits) to support the mother, encourage breast feeding, administer the antibiotic and record the neonate’s health status. If the neonate did not improve within 24 hours of initiating treatment, was unable to tolerate the oral co-trimoxazole or was not breast feeding well, the CHW again advised the parents to take their child to a health facility. CHWs also monitored for the following potential complications of the intramuscular injections: (1) cellulitis or abscess at the site of injection, (2) haemorrhage at the site of injection, (3) decreased tone and movement in the injected limb and (4) skin rash.
The second implementation strategy we employed was an educational strategy.14 CHWs received an initial training of 36 days during 1995–1996. Subsequently, we conducted ongoing training of the CHWs, every 3–4 months in a 2-day training workshop. The workshop included knowledge-based and skills-based sessions. In addition, field supervisors conducted educational outreach visits twice per month and corrected gaps in knowledge and practice as needed.
We also used financial strategies to implement our home-based management of neonatal sepsis. CHWs received monthly fixed remuneration and a performance-based remuneration based on the number of neonates to whom HBNC was provided, and also the treated cases of sepsis. CHWs were penalised for errors through deductions in their payment. We also incentivised CHWs by offering a reward if there were no neonatal deaths in a cohort of 30 successive live births, which was increased to 40 births starting in 2010.
Finally, we focused on quality management strategies to implement our intervention. We developed and organised a quality monitoring system by ensuring that CHWs filled out a printed Sepsis Diagnosis Form at every home visit as a screening tool.6 If the CHW made a diagnosis of sepsis, she completed the Sepsis Management Form to guide her management and record the neonate’s progress. Three senior and high performing CHWs were promoted and trained as field supervisors (1 CHW per 13 villages) in addition to a medical supervisor. Field supervisors audited all cases of neonatal sepsis diagnosed by CHWs, including an audit of the supplies and medication used for treatment. The written data collected by the CHWs was entered electronically within 30 days. A computer algorithm written based on the clinical definition of sepsis (online supplemental appendix A) identified the ‘true’ cases of sepsis using the data collected by the CHWs. The algorithm’s diagnostic determination of sepsis was not available to the CHWs at the time of their home visits.
Implementation outcomes
(a) We evaluated our strategy of task shifting sepsis management to CHWs through the implementation outcomes of coverage, adoption and acceptability.15Coverage was calculated as the percentage of total live-born neonates in the area (as documented by the vital statistics surveillance system of SEARCH),12 who received home visits and sepsis-screening from a CHW. To measure the adoption of the intervention, we evaluated the rates of parental agreement to receive home-based sepsis management, hospital referral or refusal of both treatment options. Additionally, from 2015 to 2019, maternal acceptability of HBNC was assessed by a questionnaire administered by field supervisors. CHWs’ continuation of providing HBNC was determined by assessing the percentage of CHWs who were recruited in 1995 and continued to work in 2019. (b) Our implementation strategies of education, financial incentives and quality management aimed to promote the accurate diagnosis of neonates with sepsis. Therefore, these strategies were evaluated using the implementation outcome of fidelity, defined as the degree to which an intervention was implemented as designed.15 We assessed fidelity by comparing the CHWs’ diagnoses with the sepsis diagnoses generated by the computer algorithm. Using the computer algorithm’s diagnostic determination as the reference, we categorised each CHW diagnosis as a ‘true positive’, ‘false positive’, ‘true negative’ or ‘false negative’.
Clinical effectiveness outcomes
All neonates screened by CHWs were followed until the 28th day of life or until death, and the outcome (survival or death) was recorded and verified by the field supervisor. Clinical effectiveness of the intervention was evaluated by an examination of mortality rates associated with the four types of treatment received. Since the neonates to these treatments were not allocated randomly, the logistic regression analyses were performed to evaluate the odds of neonatal death for the different treatment types while adjusting for relevant confounders. Treatment was categorised as home-based treatment, hospital referral, refusal of all treatment and no treatment offered due to a missed diagnosis by the CHW (false negative). Confounders included variables that were significant (p<0.05) in bivariate analyses as well as the time period. Variables were checked for significant (p<0.05) interactions using the Stata command ‘lrtest’ and for multicollinearity using the VIF command. A mixed-effect model was used to account for clustering at the village level. Adjusted ORs with 95% CIs were calculated.
The trend of the four outcomes (coverage, fidelity, adoption and mortality) was assessed over the 23 years using the Mann-Kendall test. The 23-year study period was divided into six discrete time epochs, and each time epoch was compared against the preceding time epoch. All tests were two-tailed with p<0.05 considered significant. STATA V.15.1 (College Station, Texas, USA) was used for all analyses.
Of note, India’s National Rural Health Mission launched a cash incentive scheme to promote births at health facilities in 2006. In addition, in 2011, government-funded CHWs, known as Accredited Social Health Activists (ASHAs), were introduced to provide home-based neonatal care. Although all births and deaths in the study villages were captured in the current analysis, our analysis did not include data regarding any cases of sepsis that were diagnosed and/or treated by ASHAs. Similarly, cases of neonatal sepsis that were exclusively diagnosed at a health facility were not included.
Patient and public involvement
HBNC has broad community support expressed by way of resolutions passed by the 39 villages. The CHWs are part of the local population. Community engagement has informed the design and implementation of HBNC. No members of the public were directly involved in the design, conduct or reporting of this study.
Results
Study population and coverage
From September 1996 to March 2019, 18 751 live births were documented in the 39 villages. An additional 123 neonates from other areas came to these villages during the neonatal period. Over the 23-year period, the proportion of neonates born in health facilities increased from 6.1% (1996–2000) to 94.6% (2016–2019) (p<0.01) (figure 1). The proportion of mothers with no schooling decreased during this period, from 50.4% in 1996–2000 to 1.1% in 2016–2019, and mothers with >10 years of schooling increased from 6.0% in 1996–2000 to 47.6% in 2016–2019.
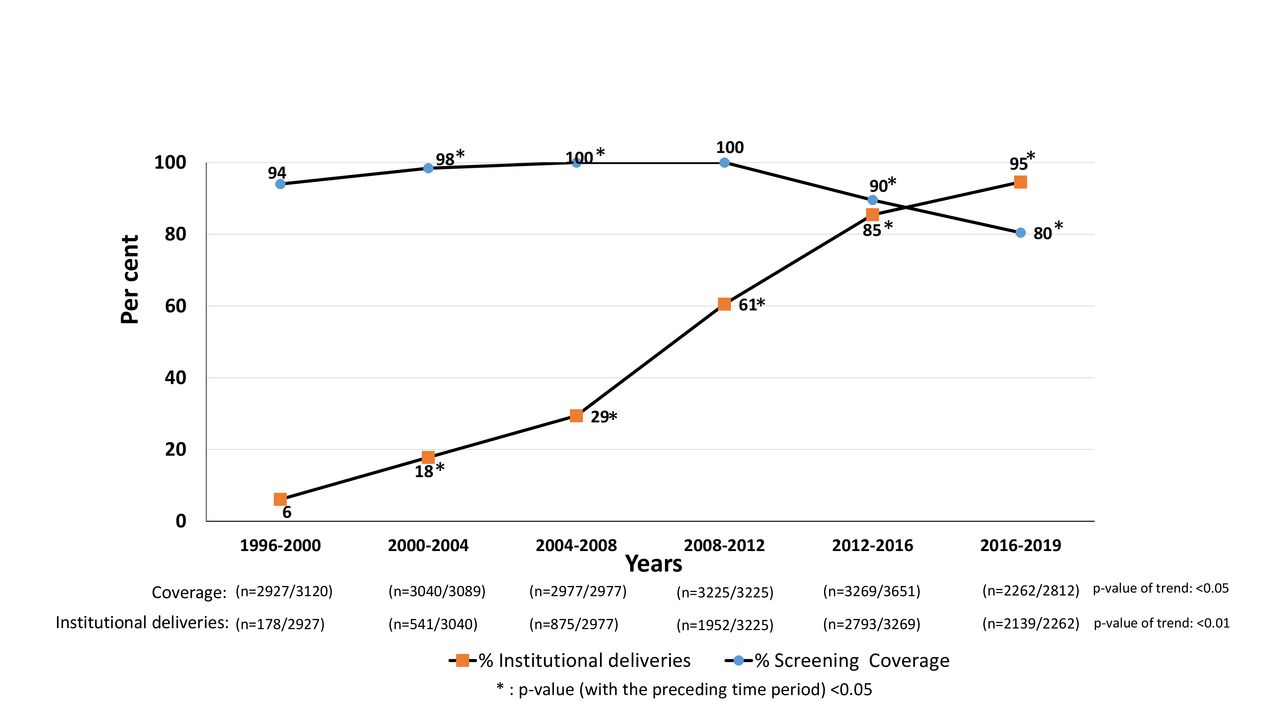
Per cent institutional deliveries and % coverage of neonates screened for sepsis in 39 villages in Gadchiroli, India (1996–2019).
CHWs made home visits and screened 17 700 (93.8%) neonates for sepsis. Over the 23-year period, the coverage remained consistent (p=0.57) (figure 1). However, there was reduced coverage in the time epochs of 2012–2016 and 2016–2019 that corresponded with a rise in health facility births (figure 1).
Sepsis cases and diagnostic fidelity
Based on the data recorded by the CHWs, the computer algorithm identified 1177 cases of sepsis (sepsis incidence 6.6%). However, the incidence of neonatal sepsis decreased over the 23-year time period (p<0.05) with a peak of 10.7% in 2000–2004 and a nadir of 1.9% in 2016–2019 (table 1). Of the mothers whose neonates were diagnosed with sepsis, 270 (23.7%) had no education, the median parity was 1 and 902 (76.6%) had received antenatal care. Premature births accounted for 197 (16.8%) sepsis cases and 601 (51.4%) neonates were low birth weight (<2500 g) (online supplemental appendix B).
Neonates screened, diagnosed and treated at home for sepsis, 1996–2019
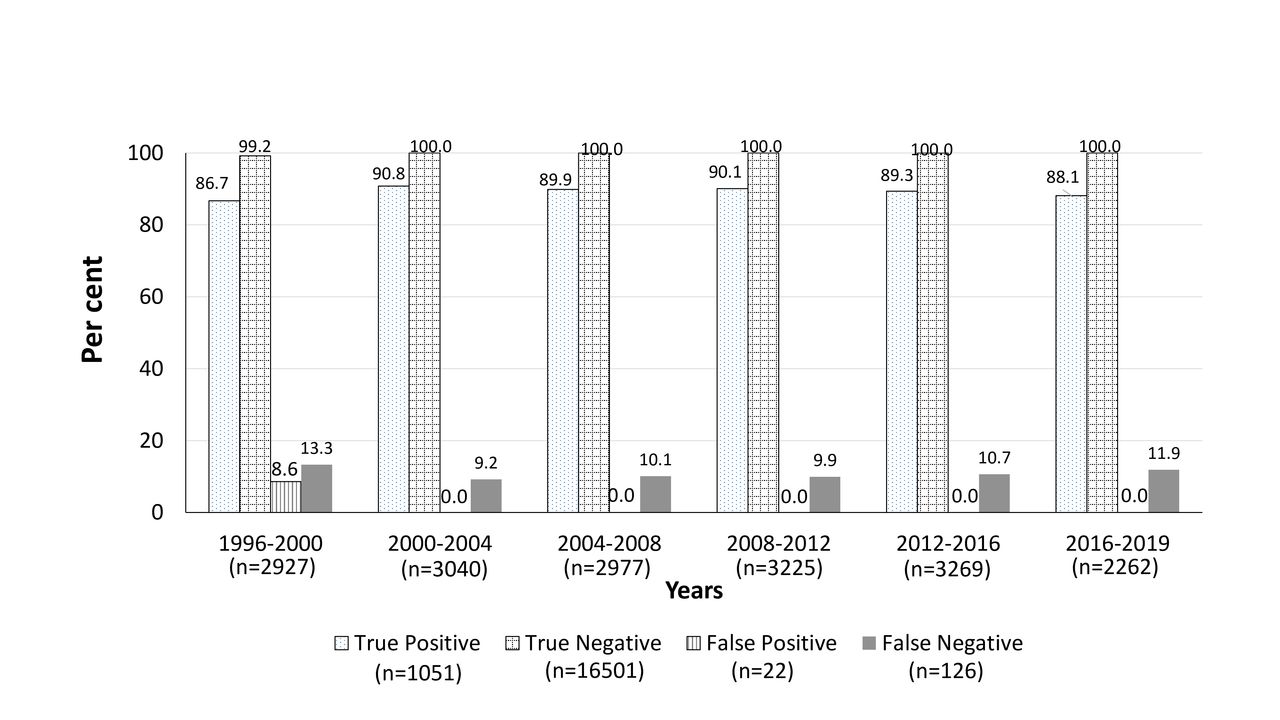
Of the 1177 cases of sepsis identified by the computer algorithm, CHWs correctly diagnosed 1051 (89.3%) cases of sepsis (true positives). The ability of CHWs to identify true positives did not significantly change during the study period (p=0.57) (figure 2). However, CHWs missed the diagnosis in 126 (10.7%) cases (false negatives) and incorrectly diagnosed 22 cases as ‘sepsis’ for a false positive rate of 0.1%. Importantly, all 22 false positives were diagnosed before April 2000, and there were no false positives after that time.

Clinical diagnosis of neonatal sepsis by community health workers compared with computer algorithm, Gadchiroli, India (1996–2019).
Intervention adoption
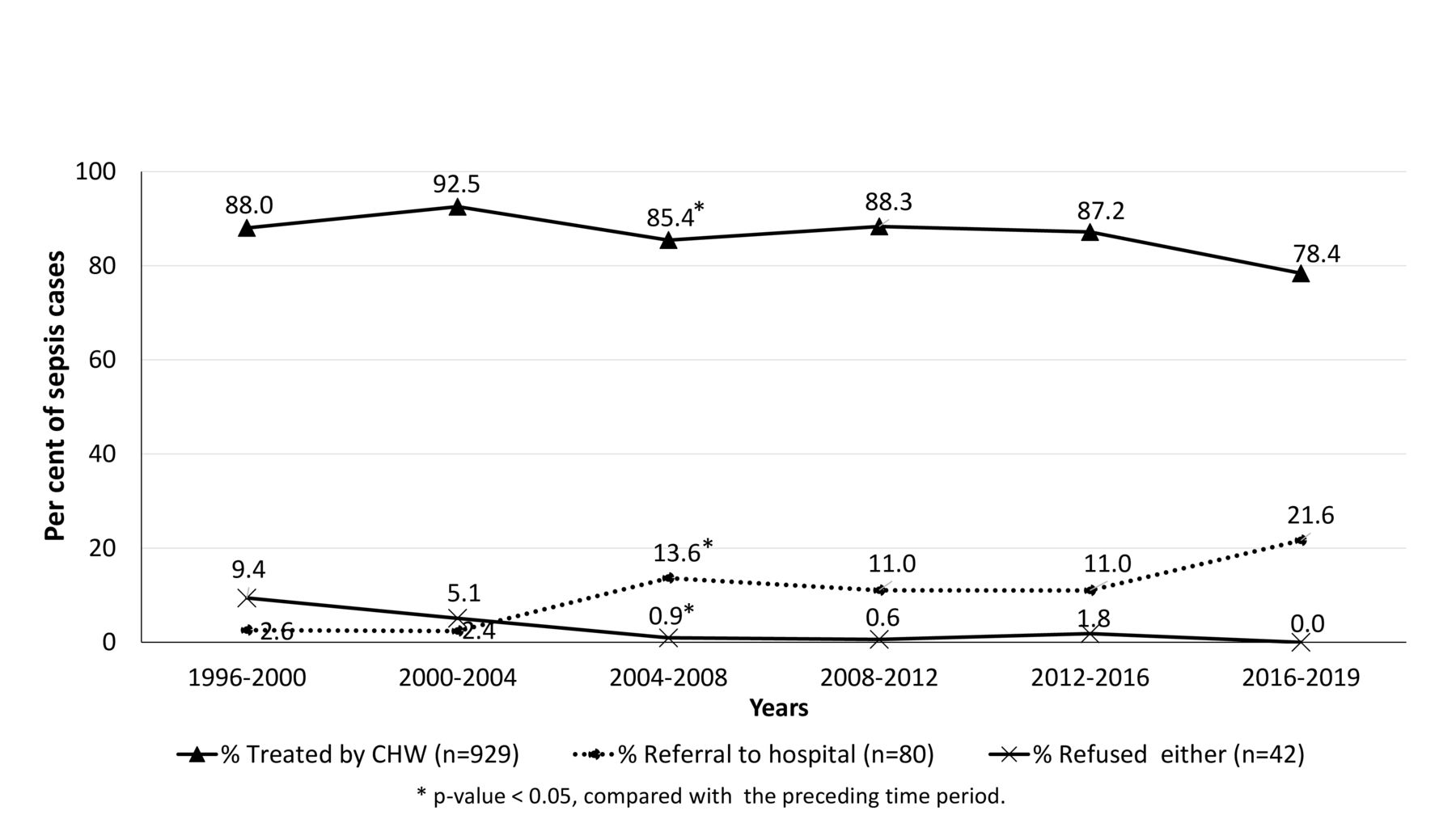
Of the 1051 cases of neonatal sepsis that CHWs correctly diagnosed, the families of 80 (7.6%) neonates agreed to a hospital referral. Home-based sepsis management was provided to 929 (88.4%) neonates, and the remaining 42 (4.0%) families declined both hospital referral and home-based management. From September 1996 to March 2019, the rate of parental adoption of home-based treatment remained unchanged (p=0.26). However, there was a significant decrease in adoption of home-based treatment in 2004–2008 and a non-statistically significant decrease in 2016–2019, both of which correlated with an increase in hospital referrals (figure 3).
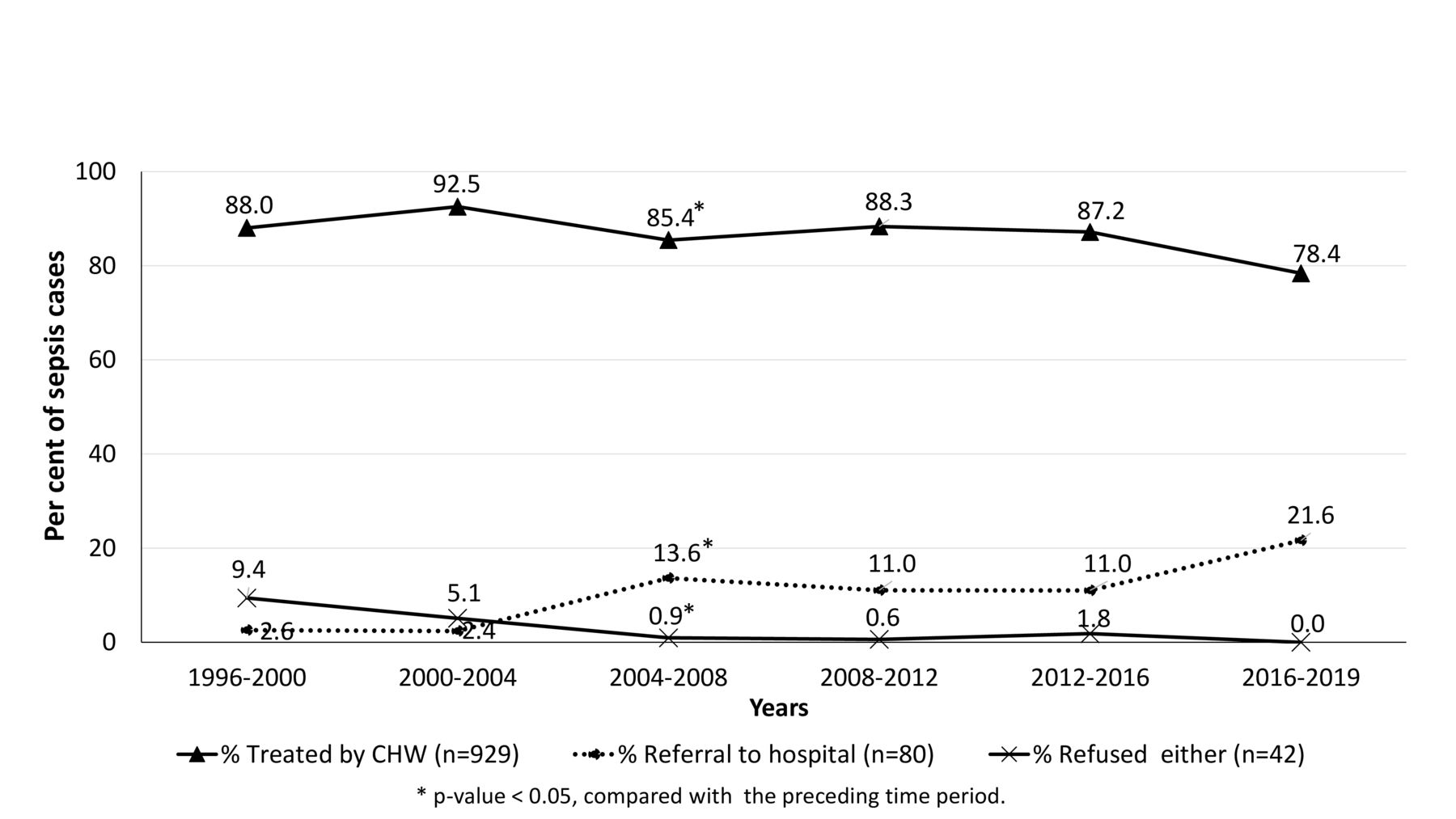
Parental adoption of the place of treatment of sepsis, 1996–2019. CHW, community health worker.
Between 2015 and 2019, 3052 (98.4%) mothers whose neonates received HBNC from CHWs were interviewed by field supervisors, and 99.6% were satisfied with the care provided by CHWs. In terms of the CHW retention rate, 69% (27/39) of CHWs who were recruited in 1995 continued to provide HBNC in 2019.
Clinical effectiveness
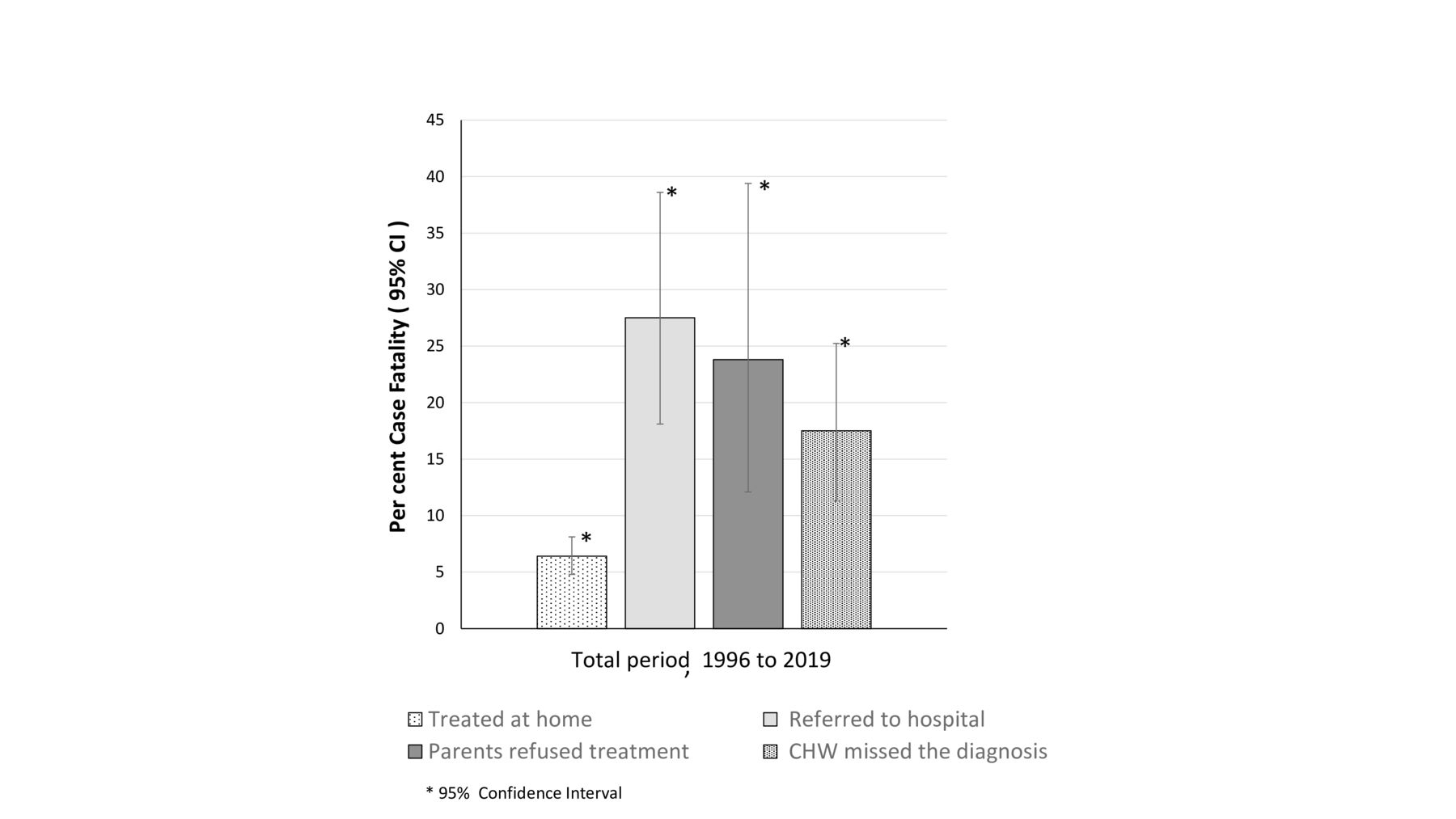
Among all neonates with sepsis (1996–2019), the mortality rate was 6.4% (59/929) for neonates who received home-based treatment, 27.5% (22/80) for neonates whose families accepted hospital referral, 23.8% (10/42) for neonates whose families refused all treatment and 17.5% (22/126) for neonates whose diagnosis was missed by the CHW (‘false negatives’) (figure 4 and online supplemental appendix C). In bivariate analyses, maternal education, place of delivery, gestational age, birth weight and age at diagnosis were identified as significant confounders (online supplemental appendix D) and were adjusted for, along with time period. No significant interaction was found between the variables. The VIF values were <5.0, indicating no multicollinearity in the selected variables. When compared with neonates who received home-based treatment, the adjusted odds of death was 5.45 (95% CI 2.74 to 10.87; p<0.001) times higher for neonates whose parents accepted hospital referral and 5.27 (95% CI 1.91 to 14.58; p=0.001) times higher for neonates whose parents refused all treatment. In addition, the adjusted odds of death was 2.17 (95% CI 1.07 to 4.41; p=0.032) times higher for neonates whose diagnosis was missed by the CHW compared with neonates who were treated by the CHW.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mortality in neonates with sepsis exposed to four types of treatment, 1996–2019 (treated at home (929), hospital referral (80), refused all treatment (42) and CHW missed the diagnosis (126)).
The mortality rate for neonates treated at home remained consistent over the 23-year study period (p=0.71). Notably, from 2016 to 2019, all of the 29 neonates who received home-based sepsis management survived. Moreover, CHWs administered a total 11 439 injections of gentamicin to the 929 treated neonates during the 23-year study period, and there were no antibiotic-related or injection-related adverse events.
Discussion
This study demonstrates the sustained implementation and clinical effectiveness of home-based management of neonatal sepsis over a 23-year period in rural Gadchiroli, India. Specially, CHWs correctly diagnosed 89.3% of sepsis cases (figure 2) and there was persistent parental adoption (>78%) of home-based antibiotic therapy (figure 3). Moreover, neonates treated at home had a significantly lower adjusted odds of death compared with all other treatment types (figure 4 and online supplemental appendix D) with no reported injection complications. However, the reduced coverage in the last two time epochs and the declining incidence of sepsis highlight the decreasing need for home-based management of sepsis as the rate of health facility births and access to hospitalisation have increased over time (figure 1).
At its foundation, sustainability is the ongoing implementation of an intervention beyond its trial period with continuation of the desired outcomes while allowing for some degree of adaptation.16 Multiple elements of SEARCH’s home-based management of neonatal sepsis might have contributed to its sustainability. First, SEARCH has maintained local acceptance since its inception through ongoing efforts to secure community involvement and buy-in. Second, the choice of using women who reside within the community and are available everyday as CHWs was a crucial factor in achieving the high coverage rate. The overall high coverage rate and quality of care provided by the CHW were maintained through a motivated and skilled human resource with refresher training, regular field supervision and performance-based remuneration. Finally, SEARCH’s HBNC programme has benefited from long-term funding granted by national and international philanthropic sources, including the MacArthur Foundation, the Bill and Melinda Gates Foundation and the Tata Trusts.
As the pioneer of home-based management of neonatal sepsis,4 SEARCH has the unique advantage of the longest continuous experience and data on procedures and outcomes. To our knowledge, this is the first report of long-term sustainability of home-based management of neonatal sepsis. Since the 2015 release of WHO’s guidelines for community-based management of sepsis in young infants,11 there has been preliminary implementation research in sub-Saharan and South Asian countries to assess local feasibility and adoption.17–26 Similar to our findings, most sites found that the vast majority of families refused referral to a health facility but agreed to outpatient antibiotic therapy.17 20 21 26 The ability of primary healthcare workers to correctly identify sepsis and adhere to management protocols varied greatly by site,17–26 opening the opportunity for collaboration and education between sites as well as the need for ongoing local adaptation. Of note, families at the majority of sites in other studies needed to bring their child to a primary health centre daily to be assessed and receive injections as opposed to SEARCH’s programme in Gadchiroli in which all management was provided at home. In addition, the WHO diagnostic criteria and antibiotic regimen differ slightly from those used by SEARCH, which were developed based on analysis of local efficacy prior to publication of the WHO guidelines.5 11
Interestingly, compared with neonates who received home-based treatment, the adjusted odds of mortality was more than 5 times higher for neonates whose parents accepted hospital referral (online supplemental appendix D). We believe that hospital referral was associated with higher risk of death for two reasons. First, neonates who were referred to a hospital had a more severe illness presentation, placing them at higher risk for mortality. Second, home-based treatment has the crucial advantage of ensuring prompt treatment with antibiotics after a diagnosis of sepsis is made. When neonates are referred to hospital, there is often a delay in accessing treatment and some may never receive antibiotics.
A concern that has been raised about community-based management of neonatal sepsis is the potential for indiscriminate usage of antibiotics leading to antimicrobial resistance.27 However, in the current study only 5.2% (929/17 700) of all births seen by CHWs received home-based antibiotics. This rate is not very dissimilar to the 3.1% of all infants <3 months of age in the USA who were hospitalised for sepsis treatment from 1988 to 2006.28 In the current study, only 22 neonates were incorrectly diagnosed and treated for sepsis (false positives), and all of these episodes occurred prior to the year 2000. In addition, there were no injection-related complication in the >10 000 injections that were administered. Finally, the fact that the mortality in treated neonates did not rise over the 23-year study period indirectly suggests that antimicrobial resistance is not an emerging problem in our population. Together, these results confirm that rational usage of oral and injectable antibiotics by CHWs is possible with a strict diagnostic definition and high-quality training and supervision.
Following the local sustainability of a health intervention, the next question is whether the intervention can be scaled-up. Through several partnerships, SEARCH has replicated the comprehensive HBNC to other parts of India with successful reduction in neonatal mortality when the package was delivered by a dedicated health worker in the community.29 However, these health workers in the field trial only administered home-based antibiotic therapy to 40% of the infants with suspected sepsis compared with 88.4% in Gadchiroli, suggesting that additional effort is needed to improve compliance.29
The majority of India’s rural poor receive health services from the Government of India’s National Rural Health Mission (NRHM). The NRHM engages ASHAs who are female CHWs focused primarily on reproductive and child health. In 2011, the NRHM decided to incorporate HBNC and deliver it through ASHAs in rural India.30 Since then, SEARCH, the National Health Systems Resource Centre and state governments have trained nearly 900 000 ASHAs to provide HBNC, including screening, diagnosing and either referring neonates with sepsis or treating with oral co-trimoxazole or amoxicillin when referral is not possible.31 The ASHAs have been deployed in SEARCH’s 39 study villages as well, creating some overlap which may explain the reduction in the screening coverage by SEARCH’s CHWs in the later years (figure 1). The reduced coverage may also be explained by the discontinuity in care caused by the increase in health facility births during the later years.
During the 23-year study period, several other changes occurred in rural India. Since 2006, the national policy increasingly favoured facility-based deliveries. A national scheme called Janani Suraksha Yojana was launched by government which offered cash incentive to mothers as well as ASHAs for facility-based delivery. This resulted in a rapid shift towards institutional delivery as seen in our data as well (figure 1). Moreover, the socioeconomic standard and women’s education improved, maternal and neonatal care practices changed to align with best practices. Most probably due to these changes, coupled with the continued HBNC by SEARCH’s CHWs and ASHAs, the incidence of neonatal sepsis in these 39 villages progressively declined. We have previously reported that the incidence of sepsis declined from 111 per 1000 live births (1998–2001) to 19 per 1000 live births (2016–2019).32 Presummably, facility-based delivery also led to increased identification and treatment of early onset sepsis in the facility. This also might have contributed to the decreasing number of cases of sepsis treated during the study period (table 1).
It is a welcome trend that over the past two decades the need for home-based management of sepsis has substantially reduced, and hopefully, at some time in the future, home-based management of sepsis will no longer be required. Until such time, home-based management should continue to fill the gap for families for whom facility-based care is inaccessible, unaffordable or unacceptable, including those who give birth at a health facility but require community-based follow-up.
A few limitations of our study should be explored. First, the diagnosis of sepsis was based solely on clinical signs without microbiological confirmation. Because clinical signs of neonatal sepsis are non-specific, we might have overestimated the true incidence of bacterial infections. This is an unavoidable limitation in resource-limited settings. In addition, the reduced mortality in treated versus untreated neonates suggests that the benefits of not missing a case of sepsis outweigh the risk of overtreatment. Moreover, even in resource-rich hospitals, the current standard of practice dictates the initiation of antibiotics when there is any clinical suspicion of neonatal sepsis. Second, the diagnosis of sepsis in this study relied on the recording of clinical criteria by CHWs who have significantly less training than physicians or nurses. Nevertheless, a previous study in Gadchiroli demonstrated a 92% concordance between data on neonates recorded by CHWs compared with a visiting physician.33 Finally, our cohort of untreated neonates with sepsis was a non-random, heterogeneous compilation (ie, neonates whose families refused all treatment and neonates whose sepsis diagnoses were missed by the CHW but determined by the computer algorithm), which may have introduced selection bias. The direction of bias is unknown as parents who refused treatment could have assessed their child’s illness as either mild with no need for treatment or hopeless with no expected benefit from treatment. This limitation was not preventable given that it would have been unethical to randomise neonates with sepsis not to receive any treatment. While our comparison between treated and untreated is opportunistic, the protective effect of treatment was apparent even after adjusting for confounders.
Conclusion
In summary, home-based management of neonatal sepsis is an effective option when referral to a health facility is not feasible in resource-limited settings. The current study demonstrates that its implementation was sustained over 23 years in Gadchiroli through appropriate task shifting, educating, financing and quality management strategies.14 The mortality in treated cases of neonatal sepsis in Gadchiroli remained low for more than two decades compared with all other treatment options. With the improved socioeconomic status and healthcare access, especially the shift towards facility-based delivery in Gadchiroli, the need for home-based management of neonatal sepsis has declined and will likely continue to decline. Scale-up of this intervention is advised in areas in India and internationally where sepsis remains a major cause of neonatal mortality until hospital care becomes accessible and acceptable to all.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Contributors AB: leader of Home-Based Newborn Care, conceptualised the current study, interpreted the results, edited and finalised the manuscript revisions. MD: data verification, data management and data analysis. SB: field programme supervision and monitoring. Anand Bang: field programme management, interpretation of results. JD: data interpretation, wrote the first draft and manuscript revisions. AB is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.