Article Text

Abstract
Introduction Incentives conditional on school attendance or on remaining free of sexually transmitted infections have produced mixed results in reducing HIV incidence.
Methods HIV-negative adolescent girls and young women aged 15–22%–50% of whom were out of school—were recruited from 293 clusters in Eswatini from urban (30%) and rural areas (70%).
Financial incentives conditional on education attendance were randomly allocated at the cluster level. All participants were further individually randomised into eligibility for a raffle incentive conditional on random selection into the raffle, on negative tests for syphilis and Trichomonas vaginalis and on being a raffle winner, creating four subarms in a 2×2 factorial design: no-intervention, raffle incentive, education incentive and raffle & education incentive. Randomisation was unblinded to participants.
Logistic regressions were used in intention-to-treat analysis of HIV incidence over 3 years to estimate the impact of incentives conditional on school attendance and raffle incentives conditional on remaining sexually transmitted infection free.
Results The study recruited 4389 HIV-negative participants, who were distributed into four subarms: no intervention (n=1068), raffle incentive (n=1162), education incentive (n=1088) and raffle and education incentive (n=1071).
At endline, 272 participants from 3772 for whom endline data were collected, tested positive for HIV. HIV incidence among participants in education treatment arm was significantly lower than in the education control arm, 6.34% (119/1878) versus 8.08% (153/1894) (p=0.041); OR: 0.766 (0.598 to 0.981); adjusted OR (aOR): 0.754 (0.585 to 0.972). Compared with the no intervention subarm, HIV incidence in the raffle and education incentive subarm was significantly lower, 5.79% (54/878) versus 8.84% (80/905); OR: 0.634 (0.443 to 0.907); aOR: 0.622 (0.433 to 0.893), while it was not significantly lower in the raffle incentive subarm.
Conclusion Financial incentives conditional on education participation significantly reduced HIV infection among adolescent girls and young women in Eswatini and appear to be a promising tool for prevention in high HIV prevalence settings.
Trial registration number Western Institutional Review Board—protocol number 20 141 630.
Eswatini National Health Research Review Board—FWA00026661.
Pan African Clinical Trials Registry—PACTR201811609257043.
- HIV
- cluster randomized trial
- health economics
- public health
Data availability statement
Data are available upon reasonable request. Relevant anonymised individual level data available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Studies focusing on the impact of incentives conditional on participation in education on HIV prevention have had mixed results, and studies with financial incentives contingent on negative sexually transmitted infection (STI) results showed success in reducing STI prevalence in Tanzania and reducing HIV incidence in Lesotho.
Given these mixed results and, therefore, uncertain policy outlook, this study was designed to test the impact of both types of conditional financial incentives, and their combination, on HIV incidence among adolescent girls and young women (AGYW), a population at high risk for HIV infection in Eswatini.
WHAT THIS STUDY ADDS
The financial incentives conditional on education participation significantly reduced the odds of HIV infection among AGYW in Eswatini.
Raffle incentives amplified the effect since the strongest reduction in HIV incidence was found for participants eligible for both types of incentives.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
With this study showing that HIV incidence reductions could be on par with biomedical interventions like HIV treatment as prevention, the use of financial incentives can be a useful tool for HIV prevention among AGYW in other high HIV prevalence settings.
INTRODUCTION
In 2020, Eswatini had the highest HIV prevalence among the general population (15–49 old) in the world (25.4%),1 with women and adolescent girls and young women (AGYW) disproportionally infected (12.2% HIV prevalence among women 15–24). There are 120 000 women living with HIV, which is 63% of the total people living with HIV in Eswatini. AGYW aged 15–24 are particularly at higher risk: in 2014, at study design, there were approximately 2400 new infections among young women, compared with just under 500 among young men.1
Income inequality in Eswatini is high, despite the country being classified as a lower middle-income country: in 2016, the Gini coefficient showed that Eswatini was the seventh most inequal country in the world.2 Just under 40% of Swazis were considered poor by global standards.3 In 2017, only 41% of women and 66% of men participated in the labour force, while unemployment overall was 24%, unemployment among the youth aged 19–24 was a staggering 50%.4 The poor economic prospects, low levels of education and employment among AGYW result in increasing prevalence of age-disparate and transactional sex.5 Population-based surveys showed that these rates among AGYW increased from 7% in 2007 to 14% in 2010, 15% in 2014 and 16% in 2016.6–8
During the last decade, several studies tested the impact of conditional financial incentives as a strategy to prevent new HIV infections.9–16 A first set focused on incentives conditioned on school participation and found mixed evidence: some showed that financial incentives may reduce HIV and Herpes Simplex Virus (HSV)-2 prevalence,9 but others using either financial incentives conditional on education10 11 or multisectoral combination interventions including cash transfers and education subsidies12 13 have not demonstrated significant reductions in HV incidence. A Cochrane review in 2017 recommended that more studies of education incentives were needed.14 Another set of studies evaluated the impact of financial incentives conditioned on remaining negative for curable STIs.15 16 In Tanzania, such incentives were found to significantly reduce STI prevalence,15 while in Lesotho lottery-based financial incentives significantly reduced HIV incidence.16 Given the mixed results suggesting equipoise, more evidence is needed on the efficiency of financial incentives for HIV prevention. With a 2×2 factorial design, the Sitakhela Likusasa Impact Evaluation was designed to test the hypothesis that incentives conditional on school attendance, raffle incentives conditional on remaining STI free, and their combination, would reduce HIV incidence measured at the individual level in a sample of AGYW who were in and out-of-school in both rural and urban settings in Eswatini. The cluster randomisation was used for education incentives to avoid contamination across participants attending the same school. Sitakhela Likusasa is a Siswati phrase meaning ‘we build the future.’
Methods
Trial design
The study, a cluster randomised trial, comprised 293 clusters—30% urban clusters and 70% rural clusters—in Eswatini.17 A cluster was defined as a census enumeration area (EA) in Eswatini. There were 2076 EAs defined in the last census in 2007, and the average number of households per area was 103 (274 for rural EAs and 34 for urban EAs). To guarantee that AGYW living in the same area and, in particular, around the same school had access to the same education incentives and to, therefore, avoid contamination, participants’ access to financial incentives conditional on education attendance were randomly allocated, using stratified random sampling, at the cluster level.
After enrolment into the study, participants were further individually randomised to have access to a raffle incentive or not. Those eligible for the raffle incentive would receive a prize if they satisfied all of the three following conditions: random selection into the raffle for that round, testing negative on negative tests for syphilis and Trichomonas vaginalis (TV) and on being a raffle winner, creating four subarms in a 2×2 factorial design: no intervention subarm, raffle incentive subarm, education incentive subarm and raffle and education incentive subarm, as per study protocol.18 Treatment and control groups for the raffle incentive and education incentive were created, as follows: education treatment arm was the education incentive subarm and education and raffle subarm; education control arm was the raffle subarm and no intervention subarm; raffle treatment arm was the education and raffle subarm and the raffle subarm and raffle control arm was the education incentive subarm and no intervention subarm.
Participants
Enrolling participants into the study and allocating them to one of the four study subarms was a five-step process, detailed in the randomisation section of this paper. Participants were randomly selected from a filtered set of EAs in Eswatini that met these criteria: (1) EAs that were not part of, or adjacent to, another impact evaluation focusing on unconditional incentives for orphans and vulnerable children that was taking place at the time in four local government areas in Eswatini and (2) EAs that had a population of 200 or higher (based on the 2007 census data, the latest available at the time).
Participants were offered enrolment into the study if they met these criteria: HIV-negative AGYW aged 15–22 at the time of enrolment were enrolled as study participants if they further met three eligibility criteria: willingness to go back to some form of education, not planning to leave Eswatini for the duration of the study and being a Swati resident. A list of eligible girls and young women was drawn from census data and confirmed with community leaders, creating two lists: one of in-school and another of out-of-school AGYW.
Interventions
Financial incentives conditional on education attendance
In the education treatment arm, participants were eligible for financial incentives when enrolling in school (at the beginning of each school year) or starting the tertiary education (university) year, starting a short course, starting a course at a technical college or vocational training, or taking up upgrading classes. Participants were also eligible for an additional incentive if they had at least 80% attendance during the school term. Participants in university, college, upgrading classes or in a short course received an additional incentive if they completed the course or a particular year. The exact conditionalities for the education incentive payments, the commensurate incentive amounts and the 2×2 factorial design are further detailed in tables 1 and 2. School enrolment and attendance were verified using Ministry of Education enrolment and attendance register data from the schools (registers were requested from entire grades, so as to avoid individual study participants being identified). The study team extracted school enrolment and school attendance data from these registers and made payments using MTN (Mobile Telecommunication Network) Mobile Money system once a term, within 3 months of the school-term ending. Enrolment in upgrading classes, vocational training, university or a short course—as well as completion of these types of education—was verified through letters from the respective institutions. Payment was made to study participants directly using MTN Mobile Money within 3 months of the proof being sent from the school directly to the study team. Participants who did not have access to (or were too young for) the MTN Mobile Money electronic payment system were paid using the local post office’s fund transfer process.
Randomisation and incentive eligibility
Description of study sub arms, with eligibility, amounts and other intervention details assigned to each group
Due to initial challenges in verifying school attendance, the payment of education incentives started slowly in the first year. This issue led to extending study implementation period by 1 year and to reinforcing the education incentives during the last year as detailed in table 2. The reinforcement of the education incentives entailed paying, in the latter half of the study, an additional incentive to participants who were in the education treatment arm and who were out of school at midline data collection.
Raffle incentives conditional on testing negative for syphilis and TV
In the raffle incentive treatment arm, the intervention took place as follows (for details, see tables 1 and 2): some participants (randomly selected at each raffle round) were enrolled in a raffle conditional on testing negative for syphilis and TV. Those two curable STIs were selected based on their known prevalence in Eswatini and neighbouring KwaZulu Natal at the time of study design.19 20 Seven rounds of raffle took place over the course of the study. At each raffle draw, participants in the raffle incentive treatment arm were randomly selected (n=200 at each round) for STI screening. Those who tested negative for TV and Syphilis were then entered in a raffle draw through which n=80 winners per round were randomly selected to receive a prize of E1 000 (~ US$72). Free medical treatment was offered to those who tested positive for either STI; post-treatment, those who tested negative were eligible for future raffle incentives.
To minimise attrition in all study groups, a study helpdesk was established and tasked with regularly updating contact details of all participants. The study’s helpline was able to maintain up-to-date contact information by using WhatsApp and phone call back feature, which helped with participants’ ability to get in contact with the study team.
Outcomes
This study was designed to evaluate the impact of incentives conditional on school attendance, raffle incentives conditional on remaining STI free and their combination, on HIV incidence measured at the individual level over 3 years (November 2015–March 2016 until November 2018–April 2019).
Sample size
Sample size for the treatment arm was calculated with the Hayes and Bennet approach,21 using equations derived from cluster-randomised trials and confirmed using the cluster sampsi programme in Stata V.12.0. Assuming a lower HIV incidence rate due to the younger age of participants than observed in the 2011 Swaziland HIV Incidence Measurement Survey (SHIMS), the study protocol, assuming the coefficient of variation k=0.25, estimated 5% HIV incidence rate after 2 years, with a 30% reduction in the treatment arm, requiring at least 83 clusters of 20 participants in each arm followed for 2 years, or 1660 per arm, for a total of 3320 participants. The sample size was increased by 10% per year or 19% over 2 years to account for attrition. Thus, the study aimed to recruit a minimum of 3950 participants from 250 clusters (80% of these clusters were rural and 20% were urban, with 50% of participants being in-school at the time of enrolment, and 50% out of school at the time of enrolment into the study).
In the interest of efficiency, the sample size calculation assumed that there was no interaction between the interventions. Few studies have examined this question, and, therefore, there is little certainty for this assumption. Without a considerable increase in sample size, the test of interaction is likely to be underpowered; however, as our primary interest was the main effects of each intervention, the study aimed to provide adequate power for the primary evaluations.22
Randomisation
Randomisation entailed the following steps:
a) For the incentives conditional on education attendance
First, at the cluster level, 50% of EAs were randomly allocated in Stata to the education incentive control arm and 50% to the education incentive treatment arm, stratified by rural and urban (70% and 30%, respectively).
Second, after selection of EAs into the study and to the education incentive treatment or control arms, EA selection validation was done to minimise the risk of contamination. In particular, geospatial analytics was used to determine which control and treatment EAs were adjacent to each other, creating an ‘adjacent EA pair’. For each of these ‘adjacent EA pairs’, simple random selection determined which of the EAs in the ‘adjacent EA pair’ should be replaced. The EA in the adjacent pair selected for replacement was replaced with another EA (randomly selected) from the sample frame (ensuring that a rural EA replaces a rural EA and an urban EA replaces an urban EA). After this was done, adjacency had to be checked again as the newly selected EA could cause adjacency issues with other EAs. The selection validation process was repeated four times until no education treatment EA or education control EAs were adjacent to each other.
Third, during enrolment into the study, the study team aimed to enrol at least 12 participants per EA, of which six had to be in school at the time of enrolment in the study, and six were out of school at the time of study enrolment. In some of the original 250 randomised EAs, it was not possible to enrol 12 participants per cluster. In 132 EAs, no AGYW could be found who were eligible and agreed to be enrolled in the study. These 132 EAs were dropped and 132 new EAs were selected from the sample population of eligible EAs, following the same adjacency checking process as described in step 2.
Fourth, after participant enrolment in the 132 new EAs was completed, the minimum sample size still had not yet been reached. To accommodate the dropped 132 EAs and the additional EAs needed to ensure that the participant enrolment targets were met, in total, 177 additional EAs were selected, following the process described in step 3—totaling 295 EAs. After enrolment into baseline data collection, two EAs were dropped because baseline data were not collected from any participants in those EAs. Eventually, after baseline data collection was completed, participants from 293 EAs (148 education treatment EAs and 145 education control EAs) were enrolled in the study. Endline data were collected from 292 EAs (one EA was not part of endline data collection because all participants in that EA either dropped out of the study or were loss to follow-up during endline data collection). See figure 1 describing the cluster level filtering and randomisation process.
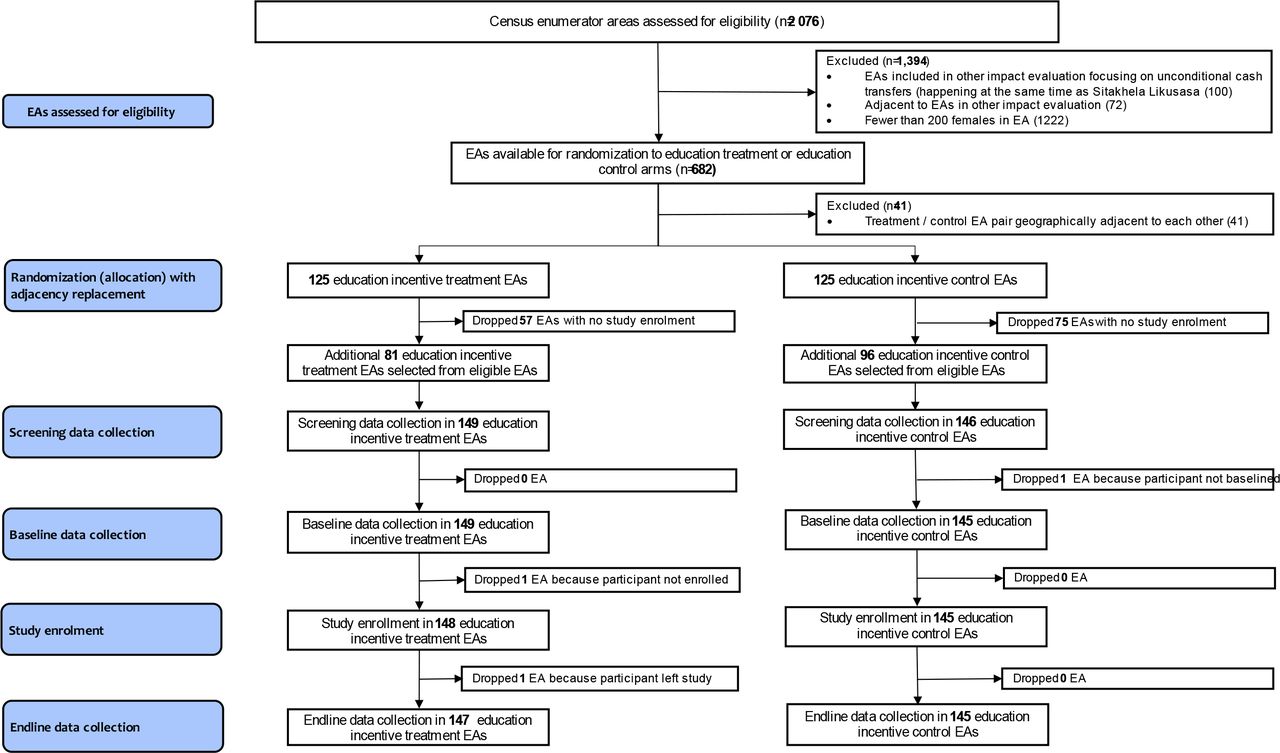
Flowchart: EA filtering and randomisation. EA, enumeration area.
At the individual level, a random sample of girls and young women from the lists of in-school and out-of-school AGYW was selected and invited to participate in the study. In EAs where it was not possible to enrol 12 participants per cluster, additional EAs were selected from either the treatment or control list of oversampled EAs. The same ‘EA adjacent criterion’ described in step 4 above was followed to ensure that no control or treatment EAs were adjacent to each other. Eventually, participants from 293 EAs were enrolled in the study. Average cluster size was 20 participants (maximum 42).
All randomisation procedures for the education incentives were computer implemented by the study statistician in Stata.
b) For the raffle incentives conditional on testing negative for syphilis and TV
This individual randomisation was facilitated by the study staff at the time of study enrolment: participants were asked to draw a ball from a closed bag with four blue and four red balls in it—blue signalled raffle enrolment and red signalled no raffle enrolment.
Allocation concealment mechanism and blinding
Due to the nature of the interventions relying on incentives, there was no masking of intervention status to the recipients either at the cluster or the individual level. Data capturers determining a participant’s school attendance every quarter, data collectors administering the education status and behavioural questionnaire and counsellors providing HIV testing at study data collection points at baseline, midline and endline, were blinded to a participant’s assignment to a study subarm.
Statistical methods
Recruitment and data collection
The study took place from November 2015 until April 2019. Participants were enrolled into the study between November 2015 and March 2016. Due to delayed implementation in the first year, the impact evaluation was extended for a third year after obtaining IRB clearance to do so. Therefore, participants who consented to being part of the third year of implementation were followed up over 3 years. All study participants were tested for HIV prior to enrolment and at different timepoints in the study. More specifically, testing, screening and surveys were conducted at baseline (November 2015 to March 2016), midline (November 2017 to March 2018) and endline (November 2018 to April 2019) to determine HIV, syphilis and TV status and elicit information on education status, household characteristics, sexual and dating behaviour, employment status, levels of knowledge, risk-taking behaviour, access to other programmes, gender-based violence incidence and related information. Raffle participation and education participation data were also collected from intervention data and school registers, respectively.
Data analysis
Stata V.15.1 (StataCorp, College Station, Texas) was used to analyse the data on an intention-to-treat (ITT) basis. Loss to follow-up included participants who refused, withdrew, were reported to be deceased or out of Eswatini or could not be contacted/traced. Absolute measures of HIV incidence, defined as seroconversion between baseline and endline, were calculated for each study group and categorical variables. Random effects logistic regression models with EA as a cluster were used to estimate unadjusted and adjusted ORs. In online supplemental table S1, we also fit generalised linear models to express the main intervention effects as risk ratios and incidence rate ratios. Adjusted regression models controlled for the following baseline variables: schooling status at baseline; rural/urban locality; region of residence; highest schooling level attained; participant age; asset-based social economic status23 and risk behaviour preference16 24 as measured at endline were also estimated. Cluster robust SEs were computed.
Supplemental material
Sensitivity analysis
Sensitivity analysis to assess the robustness of the missing at random (MAR) assumption using pattern-mixture multiple imputation model approach was conducted,25 see online supplemental figure S1 and table S2. The analysis showed nearly identical results with no change in interpretation of the MAR analytical results, and, thus, only the MAR results from complete case analyses are reported.
Ethics
All potential participants and their legal guardians (for minor adolescent girls) were informed of the purpose of the study, the outcomes and process, and the confidentiality of their responses. They received an information sheet detailing the risks and benefits of enrolment and were then invited to participate in the study, and their informed consent was sought. All participants could refuse to participate or leave the study at any time. Communities were sensitised to the study via public and radio announcements. Guardians were not informed of HIV testing for minors as the age of consent for testing in Eswatini is 12 years. This was implemented to minimise the chance that guardians would be able to deduce that the minor was excluded due to their HIV status for those minors who do not wish to disclose their status to their guardians.
HIV-positive participants were referred for HIV care at baseline and during the study, and follow-up was done with all positive participants to assess levels of uptake of linkage to care. STI treatment was offered for the participant and her sexual partner. In the raffle incentive treatment group, every STI-positive participant was also retested 2 weeks after treatment and if STI negative, she was eligible for the next raffle round.
Patient and public involvement
This study was launched after extensive discussions with HIV stakeholders in the country including the Ministry of Health, Ministry of Education and Training, the Office of the Deputy Prime Minister that coordinates programmes for and help with orphans and vulnerable children and the Department of social welfare, the Ministry of Tinkhundla Administration and Development, NERCHA, Central Statistics Office and civil society organisations supporting and representing youth groups, UN agencies, other researchers working on HIV in the country, and other development partners—to determine the most pertinent research questions, implementation modalities and focus of the study. The study further involved traditional leaders and local leaders in all four regions of Eswatini to ensure that the study was well understood and that their concerns were taken into account. Moreover, the study team obtained feedback from and held conversations with parents, teachers and school administration staff and the regional education officers to both understand the challenges in school access, what can be done to address it and how to best implement the study in ways that would be perceived as fair by the parents and teachers. The survey questionnaires were piloted with typical study participants to improve the wording of the questions in the local language. Prior to designing the research, the study team also conducted qualitative research using ethnography methods to understand the range and type of sexual relationships and behaviours in the country and how people in local vernacular refer to them. During the study, a helpdesk was established to ensure that study participants had access to the study team for any questions or concerns. During the time of recruitment of study participants, posters about the study were put up in public places in the community and information shared with local leaders, including about the study sites and their purpose. Study progress and results were also shared with these stakeholders.
Results
Participant flow
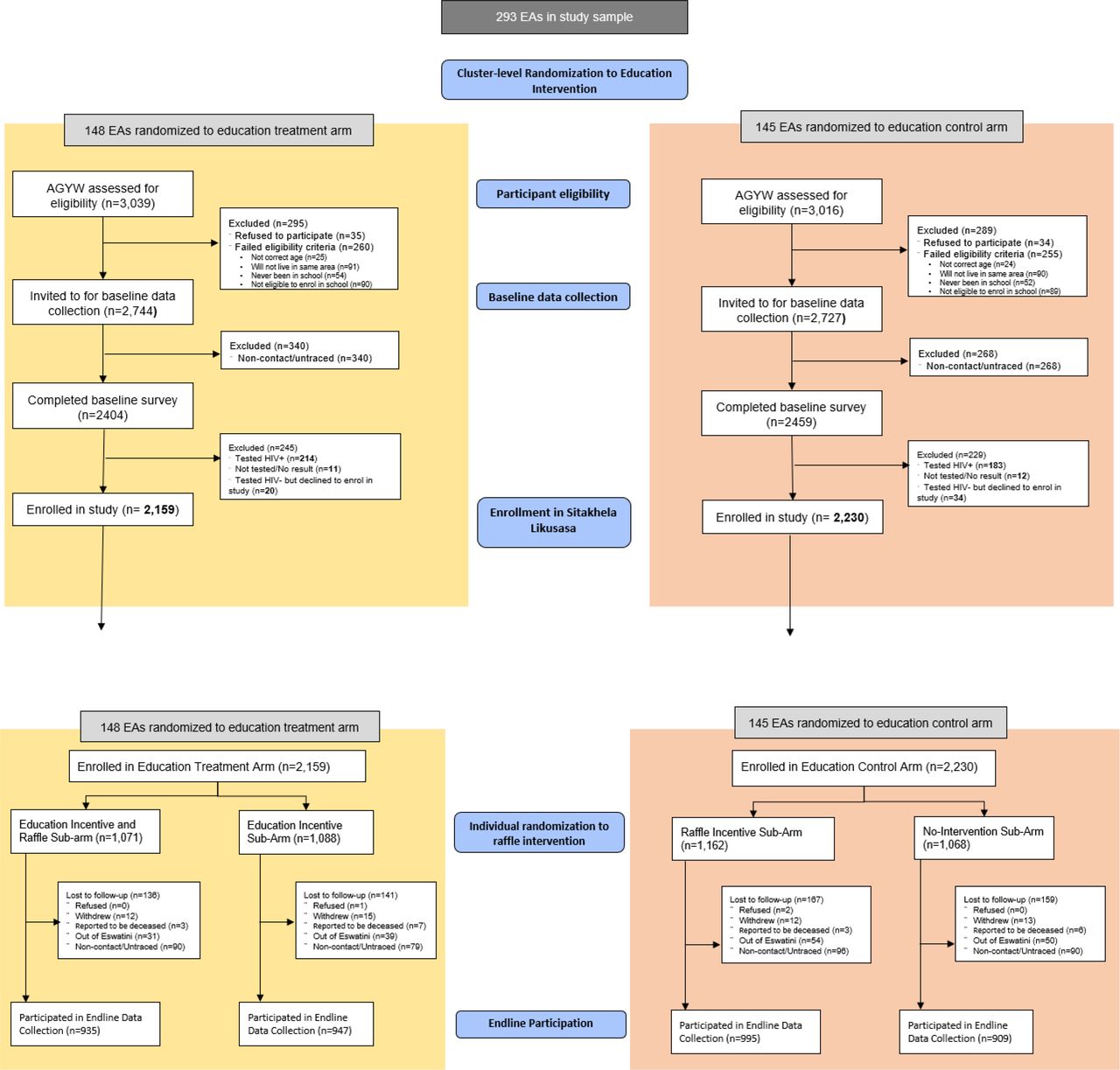
Due to a lower number of participants enrolling in the study per cluster than assumed during the study design, a total of 293 clusters were eventually included in the study: 148 education incentive treatment clusters and 145 education incentive control clusters, enrolling 4389 participants. From 4389 recruited participants, 2159 were in 148 randomly selected clusters eligible for the education incentive. Individual randomisation for the raffle incentive distributed participants into four subarms: no intervention (n=1068), raffle incentive (n=1162), education incentive (n=1088) and raffle and education incentive (n=1071). There was no opportunity to enrol after baseline. Midline participation rates were 84.2% overall (3695/4389), 81.1% in the no-intervention group, 86.1% in the raffle incentive group, 85.6% in the education incentive group and 83.8% in the raffle and education incentive group. Endline participation rates were 86.3% overall (3786/4389), 85.1% in the no-intervention group, 85.6% in the raffle incentive group, 87% in the education incentive group and 87.3% in the raffle and education incentive group (see participant flow in figure 2). Fourteen endline participants did not have HIV test results that is, 14/3786=0.37%.
{kind=link}
{kind=link}
Participant enrolment and participation. AGYW, adolescent girls and young women; EA, enumeration area.
The differential loss-to-follow-up was not statistically significant, p=0.085. Sensitivity analysis assessing the MAR assumption in the ITT complete case analysis at endline showed that estimates were almost identical and, thus, there were little to no effect of attrition on estimates, see online supplemental table S2.
Baseline data
Table 3 shows that there were no statistically significant differences between the education treatment and education control arms at baseline and endline on the following variables: schooling status at baseline, urban/rural locality, baseline highest education level and age at enrolment and attitudes towards risk, while differences were observed by region and for baseline wealth quintiles using an asset-based measure.17 The proportion of enrolled participants from each region was retained at endline.
Participant characteristics at baseline and endline
Intervention exposure
Fifty nine per cent (1274/2159) of all participants in the education treatment arm received at least one incentive payment during the implementation period. Across all rounds, education incentive payment varied between 88% and 100% of all participants whose school participants had been verified. The proportion of participants verified and paid was higher in calendar year 2018 (98%–100%) compared with calendar years 2016 and 2017 (88%–99%). The primary reason for non-payment of verified participants was due to non-contact, see Table S3.
Raffle payments for participants who were randomly sampled, tested negative for TV and syphilis, and selected for a raffle prize, was between 95.0% and 98.7%. Non-payment to the raffle ‘winners’ was due to non-contact of raffle ‘winners’ after a negative STI test, see Table S4.
Outcomes and estimation: HIV incidence
At endline, 272 participants from 3772 analysed had seroconverted to HIV.
HIV incidence in education incentive control arm: HIV incidence among participants in the education incentive control arm over 3 years averages to about 2.7% per year, or 8.1% over the study period (see table 4).
HIV incidence and bivariate and multivariable association with baseline characteristics
HIV incidence by education incentive treatment arm: across the study period, HIV incidence among participants in the education incentive treatment arm was 6.3%, statistically significantly lower than among those in the education incentive control arm (8.1%), p=0.039. Participants in the education incentive treatment arm had 23.4% lower odds of acquiring HIV over the study period compared with those in the education incentive control arm (OR: 0.766 (0.598 to 0.981), p=0.035). After adjusting for other key variables, participants in the education incentive treatment arm had a 24.6% lower odds of HIV infection (aOR: 0.754 (0.585 to 0.972), p=0.029) (see table 4).
HIV incidence by raffle treatment arm: although not significant at the 5% level, HIV incidence was lower in the raffle incentive arm compared with those in the raffle control arm, 6.61% versus 7.83%, p=0.086. Participants in the raffle incentive arm had 17.3% lower odds of acquiring HIV compared with those in the raffle control arm (OR: 0.827 (95% CI 0.645 to 1.060), p=0.133).
The unadjusted and adjusted odds of acquiring HIV was lower for participants in any of the three subarms compared with those in the no intervention subarm. Those in the education incentive and raffle subarm had 36.6% lower chance of acquiring HIV over the implementation period compared with those in the no-intervention subarm (OR: 0.634 (0.443 to 0.907), p=0.013), and it was 37.8% (aOR: 0.622 (0.433 to 0.893), p=0.010) after adjusting for other key variables as shown in table 4.
Discussion
The Sitakhela Likusasa study is a rigorous cluster randomised control trial to evaluate financial incentives conditional on education attendance and raffle incentives conditional on remaining STI negative. The findings indicate that financial incentives conditional on education participation significantly reduced the odds of acquiring HIV infection among AGYW in Eswatini by 24.6%. While raffle incentives on their own did not lead to a statistically significant reduction in HIV incidence, the combination of raffle and education incentives statistically significantly reduced the odds of acquiring HIV infection by 37.8%.
Not only these are significant reductions in the odds of acquiring HIV, but the study was implemented (a) in a public sector education system and (b) managed to enrol and incentivise even study participants who were out of school at baseline with less motivation to return to school to engage in other alternative forms of learning.
The results among the study population are representative of the AGYW population in Eswatini, writ large, because of three reasons. (a) the HIV incidence in the education incentive control group was comparable to the HIV incidence among women 15–24 in Eswatini measured through a population-based biobehavioural survey in 2015/2016 (at the same time as enrolment into Sitakhela Likusasa study), namely, the second SHIMS; (b) the HIV incidence of 2.7% in the education incentive control arm is within the 95% CI limits of the SHIMS2 estimate,26 suggesting that the study population is comparable to the Eswatini population; (c) with 30% of participants from urban areas and 70% from rural areas, the study sample reflected the distribution of the population of Eswatini.
The Sitakhela Likusasa results are consistent with a study conducted in Malawi9 that showed that cash transfers conditional on education participation reduced HIV prevalence, but they stand in contrast with the results of the CAPRISA10 and HPTN06811 studies, both of which also tested financial incentives conditional on schooling but reported a lack of statistically significant impact among their study populations. A key difference between these two studies and Sitakhela Likusasa is that in these two studies, most study participants were AGYW already in school and living in urban areas while the Sitakhela Likusasa study enrolled 50% of AGYW who were out-of-school at baseline, following the hypothesis that they would be more at risk and also potentially more likely to change their behaviour in response to incentives.
These results are an important contribution to the ongoing debate about the relevance of structural and social programmes for HIV prevention. To date, the impact of structural interventions (ie, interventions that address social determinants of HIV infection, or what is termed ‘social vaccine’-type initiatives including financial incentives for HIV prevention) has yielded mixed results in terms of its impact on HIV infection prevention.27 According to Baum et al, a term ‘social vaccine’ in the context of public health efforts was coined to ‘encourage the biomedically orientated health sector to recognise the legitimacy of action on the distal social and economic determinants of health’.28 The potential of structural HIV prevention programmes (like secondary education programmes) as a ‘social vaccine’ has been postulated numerous times29 30 and shown in natural experiments to be effective (such as an estimated 8.1 percentage point decrease in HIV prevalence for every added year of schooling in Botswana).31 But, experimental evidence has been scarce, sometimes because of limitations in study design: interventions were tested using self-reported behavioural outcomes and not HIV incidence, and some were small-scale evaluations without sufficient power to detect a statistically significant result.
In this regard, Sitakhela Likusasa aimed to provide rigorous evidence about the potential of a structural intervention to be a ‘social vaccine’ for HIV prevention. For a structural intervention to be deemed as a ‘social vaccine’, it would require that such an intervention has experimental results with a similar effect size to that of a biomedical intervention. Contrasting the effect sizes in the Sitakhela Likusasa results with studies evaluating universal (HIV) test-and-treat strategies (UTT)—which put persons on HIV treatment immediately on an HIV-positive diagnosis—provides such a comparison. Out of five UTT trials, two studies32 33 showed a reduction in HIV incidence,34 with effect sizes around 30%, comparable to Sitakhela Likusasa. This shows that ‘social vaccine’-type HIV prevention programmes (such as the interventions evaluated in Sitakhela Likusasa) that also address other, wider human capital challenges (education drop out and incompletion), can have an effect of similar magnitude to that of biomedical/drug-based HIV prevention strategies like test-and-treat.
The following study limitations should be considered in interpreting the results: attrition, especially for the no-intervention group, and difficulties in verifying school attendance on a regular basis were identified at the outset as potential study limitations. The attrition challenge was satisfactorily addressed by the establishment of a study helpdesk tasked with regularly updating contact details of all participants. Due to challenges in verifying school attendance, the payment of education incentives started slowly in the first year. For that reason, the study implementation period was extended by 1 year. The education incentives were reinforced during the last year. A further limitation of the study is the lack of power to detect differences in effects between study subarms. While this study was conducted at a relatively large scale for Eswatini and with direct involvement of the Government of Eswatini, some of the interventions were supported outside the national administrative system and externally funded, raising issues about scalability and sustainability. In particular, the programmatic implementation of regular raffle incentives might be challenging to scale-up, even though our design which randomly selected the participants taking part in each raffle round minimised the testing costs. The findings reported in this paper focused solely on the impact of the intervention on HIV incidence and did not account for potential health and education benefits of the intervention (which might have been sufficient to justify the implementation of such a safety net supporting human capital challenges among AGYW in Eswatini, regardless of the HIV outcome).
Conclusions
The study results have shown that financially empowering AGYW likely gave them more opportunities to decline risky sexual encounters and incentivising them to attend school offered them productive occupations and long-term aspirations. Keeping AGYW in education significantly reduces HIV incidence and is essential for the HIV response in contexts like Eswatini with high HIV prevalence and elevated risk among AGYW; the added benefit of this intervention is not just that it is a social and behavioural intervention requiring no medication to be successful but also that it has benefits far beyond the health benefit alone. Promoting access to and completion of more years of schooling is a critical component to forming human capital in Eswatini and more generally in all low and middle-income countries.35 While financial incentives and other behavioural interventions have shown mixed results in HIV prevention, the use of financial incentives for education appears to be promising tool to reduce HIV incidence and achieve better education, health and opportunities for AGYW in Eswatini and other high HIV prevalence settings.
The absence of statistically significant effect of the raffle incentives on their own could potentially be explained by the fact that their salience might have been eclipsed by the education incentives. However, raffle incentives amplified the education incentives’ effect since the strongest reduction in HIV incidence was found for participants eligible for both types of incentives. While the study was not powered to detect differences across subarms, together with previous results from Lesotho,16 this suggests that raffle or lottery-based incentives conditional on being STI negative should be further explored as a prevention tool for HIV in combination with education incentives.
The study results have shown that an incentivised behavioural intervention can work at scale in a context such as Eswatini where HIV incidence among AGYW and the high school dropout rate are both very high. In contexts with hyperendemic HIV epidemics and high HIV incidence among AGYW, this study has shown that behavioural interventions remain an important tool for HIV prevention strategies for the AGYW population.
Supplemental material
Data availability statement
Data are available upon reasonable request. Relevant anonymised individual level data available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. Participants gave informed consent to participate in the study before taking part. The study was registered with and the protocol was approved by the Western Institutional Review Board (WIRB), IRB Tracking Number: 20141630, effective 18 December 18, 2014. In Eswatini, the study was also registered with and approved by the Eswatini National Health Research Review Board (NHRRB), Bboard registration number: FWA00026661/IRB00011253, effective 15 August 15, 2015. To accommodate extension to the study period, expansions of the education incentives, and amendments to the questionnaires, and protocol amendment approval were granted by both review boards a number of times over the implementation period, with the latest approval by NHRRB effective 12 August 2019, and WIRB effective 26 September 2019.
Acknowledgments
The authors wish to thank the Eswatini National Health Research Council and the Western Institutional Review Board that served as the institutional review boards and the data safety monitoring board for the Sitakhela Likusasa Impact Evaluation. The authors would like to thank the members of the Sitakhela Likusasa’s technical advisory committee and the Eswatini Ministry of Health for their inputs and suggestions during the study design and implementation phases. Eswatini education sector stakeholders played a significant role during the study. The authors therefore wish to thank the Eswatini Ministry of Education and Training, in particular (a) Lindiwe Dlamini, the Director of Educational Testing, Guidance and Psychological Services and (b) the Ministry’s team of Regional Guidance Officers (RGOs) amongst them Dumisile Masuku, Mlimi Mamba, Nokuthula Dlamini, Caiphus Nyaweni, Siphiwe Nkosi, Sthembile Mbingo, Sibusiso Ndlangamandla, Lindiwe Dube, Zodwa Mamba, Pinkie Masuku, Thompson Bhembe, Nature Shabangu, Zwakele Motsa and Simon Mazibuko. The RGOs provided invaluable help in ensuring the study team’s access to schools to collect the necessary class attendance records. Thanks are also due to Edwin Simelane from UNESCO who provided ongoing support and assisted the Ministry of Education and Training team involved in the study. The authors would like to thank the head teachers (principals) of schools that study participants were enrolled at. The authors wish to thank the team at SWAGAA (Swaziland Action Group Against Abuse), in particular Cebile Manzini-Henwood and Gcinaphi Ndlovu, who provided inputs to the gender-based violence aspects of the study questionnaires, and who provided counselling to any study participants who sought their assistance. The authors would like to thank the team at the National Research Laboratory (Swaziland Health Laboratory Services, as part of the Ministry of Health) that provided technical advice to ensure adherence to the country’s sexually transmitted infection guidelines and HIV testing protocols, conducted quality assurance in relation to the HIV and STI testing aspects of the study, and that performed confirmatory Trichomonas vaginalis testing (using the Cepheid Xpert TV test) during endline data collection. The authors wish to acknowledge the support of Cepheid for providing the Trichomonas vaginalis confirmatory test kits (Xpert TV) and trained the Swaziland Health Laboratory Services staff in how to use these tests on the GeneXpert platform. The authors acknowledge the support of the Lancet Laboratories in Eswatini that conducted the Trichomonas vaginalis confirmatory testing during the raffle rounds and midline data collection. The authors would also like to thank the institutions and individuals involved in managing the payments to study participants, in particular the team at the Institute for Health Measurement Southern Africa (IHM), supported by Nontobeko Fakudze, Melusi Sacolo, Mbongeni Dube, and members of the Sitakhela Likusasa Study Implementation Help Desk (Thobile Ndzabandzaba and Lindelwa Hlophe), all under the leadership of the CEO, Kelvin Sikwibele. The authors also thank the teams of field workers and the team of nurses who undertook the biomedical testing, the counsellors who provided HIV testing and counselling support, the research assistants who interviewed the study participants in the field, and the drivers who transported them. Acknowledgement is due to the team from Enhancing Care Foundation (ECF) led by Dr Sandy Pillay, and to Janan Dietrich, Gugulethu Tshabalala and Mamakiri Mulaudzi at the Bio-Behavioural Research Division of the Perinatal HIV Research Unit (PHRU), a division of the Wits Health Consortium, who were both contracted by the World Bank to code and analyze the qualitative data collected for the Sitakhela Likusasa Impact Evaluation’s Qualitative Research component. The authors would like to thank the wider team at the National Emergency Response Council on HIV/AIDS in Eswatini (NERCHA), namely Futhi Dennis (who led from NERHCA’s side the study design and implementation before leaving for postgraduate studies), as well as Bheka Mziyako, Nsindiso Dlamini and Bongani Dube. The authors want to thank the World Bank team initially involved in different stages of the study: (a) the study’s first co-Principal Investigator who was involved in the study conceptualisation and design and who left for an academic position before the study started to enrol participants, Dr Andrea Low, (b) World Bank staff involved in study design, Pandu Harimurti and Emiko Masaki, (c) World Bank staff providing support to the study’s implementation and analyses (Susan Sebastian, Silu Feng, Nigel Herath, Jasmine Vicencio, Laura Ruiz, and Tommy Wilkinson), and (d) consultant to the World Bank, Dr Audrey Pettifor, who consulted on the design and analysis of the qualitative research component of the study. Finally, and most importantly, the authors thank all the study participants who consented and their parents who assented to their involvement in the Sitakhela Likusasa Impact Evaluation, for their willingness to participate in the Sitakhela Likusasa Impact Evaluation. All the study partners appreciate the willingness of every individual participant who contributed to this important research and greatly value their participation and readiness to share personal experiences and information. The authors have written a reflexivity statement which is published as a Supplementary Appendix. The findings, interpretations, and conclusions expressed in this paper are entirely those of the authors. They do not necessarily represent the views of the World Bank and its affiliated organisations, or those of the Executive Directors of the World Bank or the governments they represent.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
DdW and KM are joint senior authors.
Handling editor Seye Abimbola
Contributors MG, KM and DdW conceived of the study idea, led and directed the study. SK was the lead statistician and guided statistical analysis throughout. AFL and VT undertook statistical analyses throughout the study under SK’s supervision. WH and MM coordinated all aspects of study implementation and supported the Sitakhela Likusasa study implementation team with challenges and bottlenecks. MM facilitated community and stakeholder engagement throughout the study, as well as managed the involvement of SWAGAA. VT, SK, TC, MLN, WH, GM, MN, and LD contributed to the design and implementation of the study, to the analysis of the results and to the writing of the manuscript. DW helped to conceptualise the study and advised on implementation challenges during the study period. KS and VT oversaw the work of the Sitakhela Likusasa implementation team. TC, VT and MLN supervised fieldwork implementation. MG, SK, VT and DdW wrote the paper, with inputs from WH, MM, AFL, LD, MLN, TC, MN, GM, KM, DW and TD. All authors discussed the results and commented on the manuscript. MG is the guarantor of the study. Other contributors are: Study participants (and their caregivers, if younger than 18) gave consent and assent to participate in the study, respectively, study participants participated in the study, and made it possible to conduct this research. Regional Guidance Officers at the Ministry of Education and Training supported study implementation through liaison with school principals on attendance register submission. School principals and heads of short course training institutions supported access to attendance registers to verify school enrolment and attendance. The Eswatini Ministry of Health’s National Health Laboratory Service staff provided support with HIV testing training and conducting confirmatory HIV testing. The Sitakhela Likusasa implementation team at the Institute for Health Measurement Southern Africa collected baseline, midline and endline data, and manned the study helpdesk. Lancet Laboratories, Ampath Laboratories and Cepheid undertook trichomonas confirmatory testing and provided trichomonas confirmatory test kits, respectively. Members of the Sitakhela Likusasa study advisory group served as scientific advisors. The Western Institutional Review Board and Eswatini National Health Research Committee provided institutional review board and research ethics oversight. Staff of MTN Eswatini supported the voucher payments to study participants. Andrea Low (of the World Bank) contributed to the study design, study parameters and study implementation initialization preparations. Futhi Dennis (of NERCHA at the time) contributed to the study conceptualization, initialization and the initial stages of study implementation in Eswatini, as well as liaison with all relevant government departments. Thembi Gama (of NERCHA) supported legal and implementation arrangements for the study’s partnership between the three institutions involved in co leading it. Pandu Harimurti (of the World Bank) supported study conceptualization and initiation. Theo Hawkins (of the World Bank) designed the visual images used in the study paper. Nontobeko Fakudze (of the Institute for Health Measurement Southern Africa) provided administrative and program support. Tommy Wilkinson (of the World Bank) supported discussions and conceptualization of the economic evaluation aspect of the study. Yai Ellen Gaye (of the World Bank) provided editorial support for the manuscript review and editing.
Funding The Department for International Development, United Kingdom; The Global Fund to Fight AIDS, TB and Malaria; the Joint United Nations Programme on AIDS and the Ministry of Finance of the Government of the Kingdom of Eswatini provided funding for this study. The funding sources did not participate in the design or conduct of the study; collection, management, analysis or interpretation of the data; or preparation, review, or approval of the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The reflexivity statement for this paper is linked as an online supplemental file 2.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.