Article Text

Abstract
Objective To assess the health cost (or benefit) of crisis-driven migration by focusing on the infant mortality rate (IMR) of the Colombian diaspora in Venezuela and the Venezuelan diaspora in Colombia.
Methods We compare national to diaspora IMRs over the period 1980-2018. National IMRs are death-to-birth ratios reported by the official vital statistics, whereas diaspora IMRs are calculated by using a semiparametric regression model on the summary birth histories collected in the population censuses. We analyse the diaspora IMRs according to whether their arrival corresponds to precrisis or crisis-driven migration.
Results During crises, diaspora IMRs show better health outcomes than those of non-migrants. The Colombian diaspora had an average annual IMR of −1.8 (95% CI −3.3 to 0.28) per year and the Venezuelan diaspora had −4.5 (95% CI −5.8 to −3.3). However, the protective role of migration is neither guaranteed nor consistent, as a crisis in the country of destination exposes immigrants to worse health outcomes than the non-migrant population.
Conclusion Migration is a survival strategy that allows people to reduce the negative effects they face during a crisis in their country of origin. The distinction between crisis-driven and precrisis migration provides a framework for assessing the cross-border effects on health outcomes due to diaspora composition, particularly when populations face adverse conditions.
- Public Health
- Child health
- Medical demography
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous studies have documented higher infant mortality among children of immigrants compared with native-born in South-to-North migration. Newborns’ health outcomes in South-to-South migration contexts have been relatively neglected.
Mortality differences across migration status groups depend on immigrants’ socioeconomic status and the context of reception.
WHAT THIS STUDY ADDS
Comparing crisis-driven diaspora infant mortality rates with those of their non-migrant counterparts at the moment that migration occurred is key in the understanding of the effect of migration in health outcomes.
The protective role played by the stability of the long-term diaspora in crisis-driven migration health outcomes may be underestimated in academic studies due to the lack of data.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Given that migrants’ survival (dis)advantages relative to the native-born are concentrated in the neonatal period, reliable access to prenatal and postpartum care in the destination country is the key to reducing a crises’ harmful effects on newborns and their mothers.
Introduction
Colombia and Venezuela share a 1378-mile border along seven Colombian Departamentos and five Venezuelan Estados (states herein). These two countries have historically maintained active cross-border populations and economic exchanges1 2 nurtured by large numbers of binational families in circular mobility.3 4 Mass migration from Colombia to Venezuela occurred from the 1970s until the early 2010s, with around one million Colombians going to Venezuela throughout the 70-year undeclared civil war known as the Colombian armed conflict. This migratory flow has become reversed since 2014, when Venezuela began to undergo a profound social and economic crisis that drove Venezuelan families to pursue emigration as a crucial survival strategy. From 2014 to 2021, the main destination for Venezuelans was Colombia, which received approximately 1.8 million Venezuelans in that period.5 According to the figures cited here, the Venezuelan population fled their country at a much faster rate than Colombians migrating to Venezuela, and the process is still ongoing.
We measure the health cost (or benefit) of migration by examining the infant mortality rate (IMR) of the Colombian diaspora in Venezuela (the Colombian diaspora herein) and the Venezuelan diaspora in Colombia (the Venezuelan diaspora herein), particularly during crises. We focus on IMR because, in addition to being part of international developmental agendas such as the Developmental Millennium Goals, IMR is a very sensitive measure of population health. Social, economic and violence-related crises can negatively affect healthcare systems by reducing coverage and diminishing the availability of resources and personnel while simultaneously raising barriers for vulnerable groups (eg, forcibly displaced populations). All of these are likely to translate into lower quality care and attention, particularly for even more vulnerable populations (eg, pregnant women and newborns). By measuring the IMR among diasporas (at destination), we are capturing the potential role played by migration in one important aspect of population health.
From a theoretical perspective, migration can improve or worsen infant mortality. On the one hand, migration can reduce infant mortality because it allows families to escape violence, hunger and extreme deprivation, all of which negatively affect infant health.6 7 On the other hand, migration may be associated with worse health outcomes for infants because migrant women may face barriers to accessing healthcare services and prenatal care at the destination, which could in turn translate into higher mortality risk for newborns. Likewise, migration-related and violence-related stress as well as other adverse conditions during migration may affect foetal health, which could worsen birth outcomes.8 9
Using census data and civil registration vital statistics (CRVS), we reconstruct the IMR time series for non-migrant populations and diasporas from 1980 to 2018. We define the diaspora population as those residing in a country that is different from their country of birth. Next, we analyse IMR trends during crises by zooming into two critical periods: the bloodiest years of the Colombian armed conflict (1998–2003) and the most severe years of Venezuela’s socioeconomic crisis (2013–2018). Our main hypothesis is that IMR differences between diasporas and non-migrants are influenced by the socioeconomic background of those in the diaspora, their composition in terms of time since arrival (eg, recent, crisis-driven vs long-term or precrisis migration) and the host country’s capacity to respond to the specific health needs of recent arrivals. Hence, higher socioeconomic background and long-term migration correlate with better mortality conditions, whereas recent migration and low socioeconomic status are associated with higher IMR, although all these associations are contingent on pre-existing conditions at destination.
Data
We combine CRVS and census data to estimate infant mortality rates (IMR) for diasporas and non-migrant populations in each country. Specifically, CRVS provides us with the annual birth and death counts for the periods 1980–2019 for Colombia and 1980–2014 for Venezuela. The census data give us the summary birth histories (SBH), which include information on: (1) the number of children ever born; (2) the number of children still alive; (3) children born and still alive during the year previous to the census and (4) the date of birth for the last child ever born to all woman aged 15–49. We use the 1981, 1990, 2001 and 2011 Venezuelan censuses and, for Colombia, the 1993, 2005 and 2018 censuses (online supplemental appendix 1).
Supplemental material
Methods
National infant mortality
We calculate national IMR as the death-to-birth ratios using the official CRVS data for both countries. We assess CRVS data quality and completeness for the entire period of analysis (online supplemental appendix 2), and we adjust the undercounts of births and deaths by inter/extrapolating their differences to the IMRs provided by the LAMBdA inter-census life tables10 (online supplemental appendix 3.1).
Diaspora infant mortality
We apply the Trussell variant of the Brass method to the SBHs to estimate diaspora IMRs.11 This method allows us to overcome challenges in estimating diaspora IMRs due to data availability (online supplemental appendix 3.3). The Brass method produces estimates for up to 15 years prior to each census round. Infant mortality estimates are modelled into annual figures via independent p-spline models11 in order to obtain a yearly diaspora proportional factor for each country, that is, a diaspora-to-national ratio for infant mortality. These ratios capture whether and how much infant mortality is higher or lower among the diaspora population with respect to non-migrants in the country of destination. We apply these ratios to the adjusted estimates using CRVS data (online supplemental appendix 3.4).
Our analytical sample comprises women who migrated before age 20, a selection criterion that allows us to include only women whose entire reproductive years were likely spent in the destination country. Additionally, we consider women with up to one child whose date of birth was posterior to the mother’s declared year of arrival. We address women with one child because censuses only include the date of birth for the last child born. These sample selection strategies let us focus on births and child deaths occurring at destination (ie, the IMR of diasporas).
Since migration influxes are considerably high, especially during crises, we have reasonable sample sizes (online supplemental appendix 3.5) for reconstructing the time series of the diasporas’ infant mortality. However, the selectivity of our analytical sample (first and unique births and women who migrated before age 20) may imply some biases in our estimates. Due to the positive correlation between higher risk of dying through life and birth order,12 13 we expect our IMR estimates to underestimate the actual IMR. Moreover, since our selection concerns only the diasporas, the diaspora/non-migrant IMR ratios are likely to be underestimated, thus making our results conservative.
Crisis-driven and pre-crisis diaspora infant mortality
Analogously, we analyse the diaspora infant mortality differential according to their arrival at the destination, that is, whether they represent precrises (long-term migration) or crisis-driven (recent) migration. We create annual ratios of precrises and crisis-driven migrations to the whole diaspora, which are also applied to the adjusted IMR calculated from CRVS data (online supplemental appendix 3.5). In addition, we use linear regression models to contrast the conditional means of the subpopulations’ IMRs during crises and according to the time since arrival. We consider the non-migrant population’s IMR as reference. The statistical analysis allows us to determine differences in the rate of change of the conditional means among the subpopulations, which we measure as changes in IMR per 1000 live births during the period (online supplemental appendix 3.5). We assess and interpret the magnitude and statistical significance of the regression coefficient as a way to summarise our findings. Admittedly, these associations do not measure causal effects.
Patient and public involvement statement
Neither the study participants nor the public were involved in designing, planning, conducting, reporting or disseminating our research.
Results
National and diaspora infant mortality trends
Figure 1 captures the broad historical patterns (1980–2019) and mortality shocks during the two periods of crisis-driven migrations in each country. Whereas overarching historical patterns are consistent with those reported in the cited literature, short-term changes (eg, peaks, declines and crossovers within a 5-year period) need to be considered cautiously, as some of them may be affected by random fluctuations. However, considering the strong consistency with country-specific events such as peaks of violence and the onset of crises, this indicates that our correction approaches work as expected and short-term patterns are unlikely to be spurious or simply driven by random variations.

IMR in Colombia and Venezuela, 1980–2018. Source: Author’s own estimates based on civil registrations; vital statistics; Venezuelan population and household censuses from 1981, 1990, 2001 and 2011; Colombian population censuses from 1993, 2005 and 2018 and the LAMBdA. IMR, infant mortality rate; LAMBdA, Latin American Mortality Database.
Hence, though the initial levels and relative paces differ, the IMR has been decreasing in both countries since the 1980s, with Venezuela beginning at a much lower level and Colombia catching up to them in the 1990s. Figure 1 shows that, around 1993, the national IMRs converged to 23 deaths per thousand live births.
In Colombia, this convergence point was followed by 6 years of improving IMR up to 1998, which is the starting point of when the armed conflict intensified. The IMR trends after 1998 suggest that the conflict contributed to wiping out the 6 years of progress and restored the country’s IMR to levels observed at the beginning of the decade. Consistent with previous research, the increased IMR overlapped the bloodiest years of the Colombian armed conflict.14 15 With the 2010 peace agreement, conflict-related violence declined along with the IMR, which returned to its preconflict trend.
Overall, the national IMR for Venezuela has decreased continuously since the seventies—with a few brief exceptions. Sudden increases in the IMR potentially reflect the upsurges in economic shocks that hit the country, including the popular uprising against price increases known as El Caracazo (1989); the political and economic instability incurred by two attempted coups (1992 and 1993);16 the 1994 banking crisis; another failed coup d'état (2002) and the 2002–2003 national oil strike that led to food and fuel shortages, impacted most of the population and fuelled an increase in violence. The overall declining trend stalled around 2009, potentially due to the ongoing economic and social crises. In 2018, the official figures set IMR at 21 per thousand live births, setting the country back to levels observed at the end of the 1990s.17
The diaspora IMRs also show declining trends, although they responded differently to the crises compared with their countries of origin and the local populations. In Venezuelan territory, the Colombian diaspora’s IMR showed a slow decrease up to the mid-1990s, then culminated in its steepest decrease during the most acute years of Colombia’s crisis (1998–2003) and up until 2007, when it became more similar to Venezuela’s national IMR levels and finished, from the perspective of a point estimate, better off than any other subpopulation’s IMR. When the Venezuelan crisis started hitting the country, the Colombian diaspora’s IMR continued to maintain lower levels than that of Venezuelans, but was not better than the non-migrant Colombians back home.
In sharp contrast, among Venezuelans on the other side of the border (ie, in Colombian territory), this diaspora’s IMR saw a constant and accelerated decrease from the 1980s up to 1997, when the armed conflict intensified. This intensification negatively influenced the IMRs of both the Colombian and Venezuelan diasporas, as evidenced by the post-1998 patterns. These descriptive patterns could be related to the fact that some of the highest rates of armed conflict and highest numbers of armed actors are found in Colombian border states, which also have the highest concentrations of Venezuelan-born migrants. For more than a 10-year period (2003–2014), the trend continued to decrease for the Venezuelan diaspora’s IMR until a positive trend is again observed after 2015. The reappearance of an increasing trend coincides with the period of massive migration flows, which makes the trend more like that of the non-migrant Venezuelans.
Infant mortality during crisis-driven migration periods
To better understand the potential mechanisms behind the heterogeneous influence of crises on diaspora IMRs, we zoom into the two periods of crises and divide the diasporas into crisis-driven migration and precrisis migration. During the period of intensified conflict in Colombia (left panel in figure 2), the IMR increased and stalled at high levels among Colombian non-migrants while the IMRs of all Colombian diasporas declined and show lower levels. These declines and overall lower diaspora IMRs may be due to the positive selection of Colombian migrants, who have the lowest IMRs, particularly among precrisis migrants. The precrisis migrants show even lower levels than Venezuelans who did not migrate after the year 2002. For the crisis-driven migrants, the results suggest that migration also acts as a protective factor. However, these groups of migrants may be facing depressing health outcomes due to the intensification of the conflict, which precrisis migrants have avoided; thus, they display higher IMRs during the entire period.
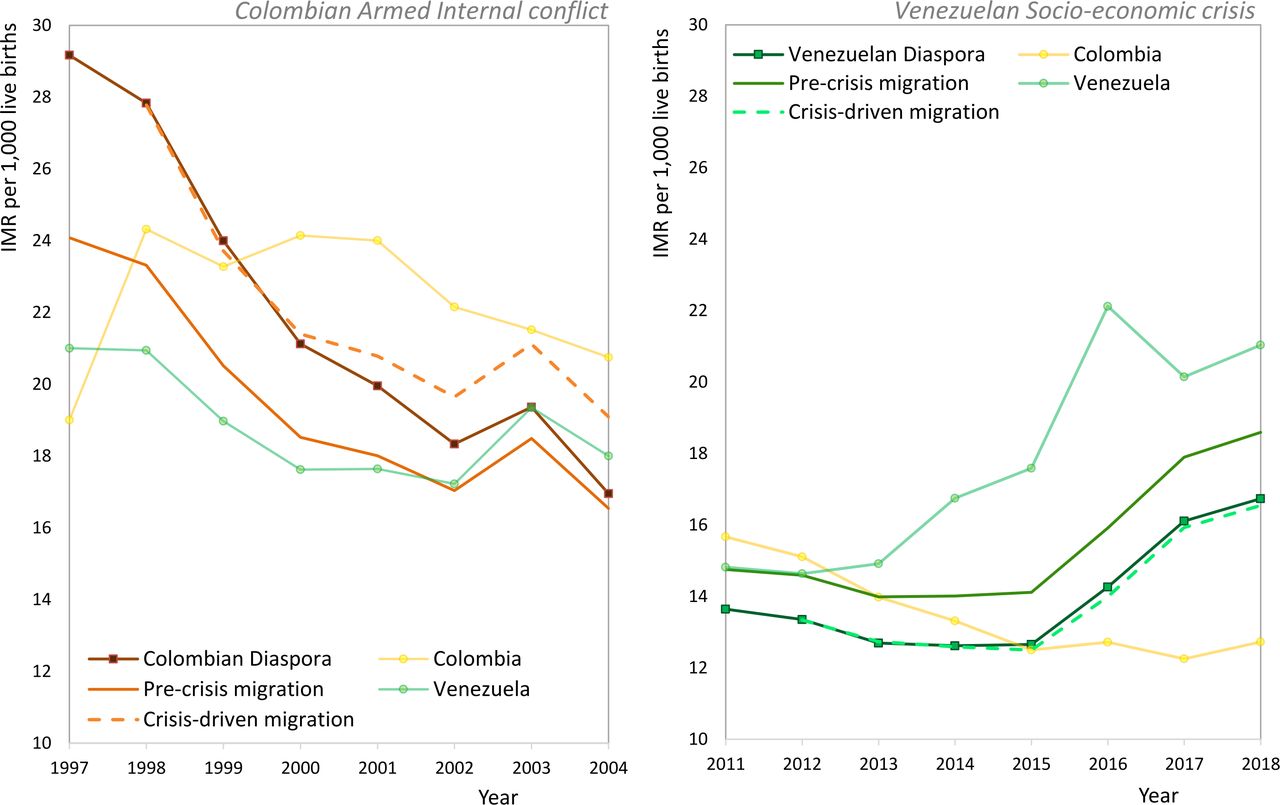
Diaspora IMRs, 1997–2004 and 2012–2018. Source: Author’s own estimates based on population census, civil registrations, vital statistics and the LAMBdA. IMR, infant mortality rate; LAMBdA, Latin American Mortality Database.
On the Venezuelan side (right panel in figure 2) until 2012, the IMRs of non-migrant Venezuelans were lower than those of their Colombian counterparts, an advantage that the precrisis Venezuelan diaspora potentially benefited from until 2013, when the Venezuelan-born flows began arriving in the Colombian border states. Throughout the most acute period of the Venezuelan socioeconomic crisis (2017–2018), the Venezuelan diaspora’s IMR rose and remained above that of Colombians who did not migrate, regardless of the time of migration. In contrast to the Colombian diaspora in Venezuela, the IMRs of the precrisis Venezuelan diaspora are higher than those for the crisis-driven diaspora during the entire period under analysis.
Despite the higher IMRs of Venezuelan diasporas relative to non-migrant Colombians, a positive association still exists between migration and newborn health when considering the IMRs of non-migrant Venezuelans during their national crisis. Two important roles in modelling the rise of the Venezuelan diaspora’s IMR may be played by, on the one hand, the socioeconomic characteristics of the migrants (who are probably more negatively selected during this time of crisis and travelling under precarious conditions) and, on the other hand, the limited access to health services at destination. Compared with other countries in the region, Colombian health systems rank poorly in terms of per capita investments, availability and access to health services.18
Figure 3 summarises the annual average rate of changes in all subpopulations’ IMRs during the crisis periods: 1998–2003 for Colombia (top panel) and 2013–2018 for Venezuela (bottom panel). The black vertical line indicates the reference category (IMR among non-migrants in the country of origin). All coefficients of diaspora subgroups are negative, meaning that the average diaspora IMRs are lower compared with those of non-migrants during the crises in the country of origin. The Colombian diaspora IMR was, on average, 1.8 (95% CI −3.3 to 0.28) units lower than the annual average rate of changes in the IMR of Colombian non-migrants. Likewise, the Venezuelan diaspora’s IMR was 4.5 (95% CI −5.8 to −3.3) units lower than that of its non-migrant counterpart.

{kind=link}
{kind=link}
{kind=link}
Diasporas IMR conditional means to non-migrants IMR (reference) during crises. Source: Author’s own estimates based on a regression model on IMR during the period of crisis in each country. Colombia 1998−2003 and Venezuela 2013−2018. The annual average rate of changes comes from the regression ß1 coefficients. IMR, infant mortality rate.
Figure 3 also shows evidence of the difference between the average rate of change in the IMRs of immigrants and the non-migrant populations. We use the term ‘immigrants’ to refer to Venezuelan-born migrants living in Colombia between 1998 and 2003 as well as to Colombian-born migrants living in Venezuela from 2013 to 2018. According to these results, the immigrant populations on both sides of the border are those who benefited the least from migration when crises occurred in their countries of destination. Despite the advantageous position that all diaspora IMRs have relative to their non-migrant counterparts, their levels are higher than the non-migrants in the country of destination.
Discussion
In the contexts of the violence and socioeconomic crises in Colombia and Venezuela, the interdependence of societal and demographic processes yielded a heterogeneous spectrum of relationships between migration and newborn survival opportunities. By reconstructing the long-term time series of the diaspora IMRs in Colombia and Venezuela, this study sheds light on two important aspects: first, how populations react to the societal pressures stemming from violent conflicts and acute economic crises; and, second, how infants’ health outcomes evolve during periods of stability. The historical migration flows between Colombia and Venezuela are particularly interesting due to the changing conditions at origin and destination.
Our analysis reveals that migration served as a protective factor for the diasporas, which had lower IMRs than their respective national counterparts during their native countries’ periods of intense crises. At the same time, it also suggests that the protective role of migration is neither guaranteed nor constant. The Venezuelan diaspora had worse health outcomes than non-migrant Venezuelans until their country’s current socioeconomic crisis began. In contrast, the Colombian diaspora did better than its non-migrant counterparts from the late nineties onward. Focusing on the destination reveals that the increasing flow of Venezuelans worsens the conditions of that country’s long-term diaspora, whose IMR had successfully coped with the non-migrant Colombian population’s increased IMR resulting from the Colombian-armed conflict.
The changing cause of binational migration flows and the consequent heterogeneity in the socioeconomic composition of the migrant populations could be the underlying reason why infant mortality is influenced by the interaction of: time since migration; the socioeconomic backgrounds of diaspora members and the social and economic crises occurring at origin and destination. As we hypothesise, the direction of IMR differences between diasporas and non-migrants depends on the diaspora’s composition in terms of socioeconomic background and time since arrival. Positive selection in terms of socioeconomic status was a feature of the Colombian diaspora during the 1970s and 1980s, when migration was driven by the economic boom in Venezuela.19 Middle-class Colombian families were more likely than their lower-class counterparts to have enough resources to benefit from economic conditions in their neighbouring country. They were also more likely to relocate beyond the bordering cities and settle in the interior, where living conditions and access to services are generally better in comparison to the border.20 By the time, the Colombian-armed conflict intensified, these middle-class families represented 77% of the Colombian diaspora. In contrast, lower-class families and rural populations were greatly affected by the armed conflict and pushed out of the country mostly towards bordering cities in Venezuela, thereby increasing the share of recent Colombian diaspora migrants. This different socioeconomic composition and spatial scope of the migrations also appears in the Venezuelan exodus to Colombia. Whereas it is mostly middle-class families that comprise flows to cities such as Bogota or Medellin, the crisis-driven migration flow that rapidly spread across the border involved mostly poor families.21 In the case of the Venezuelan diaspora, the precrisis migration represented only 7% of the total diaspora.
Beyond the composition effect, another factor is the protective role played by the stability of the long-term diaspora in crisis-driven migration health outcomes. When large numbers of binational families in circular mobility are able to nurture stable networks and mobility patterns, they can expand their survival strategies beyond national borders. Although the lack of data in Venezuela renders these mobility patterns invisible in the context of the Colombian armed conflict, the official Colombian figures provide us with some information on the increasing number of non-migrant Venezuelans seeking medical assistance and prenatal care.22
When comparing diaspora IMRs with those of their non-migrant counterparts, migrations correlate to better health outcomes during times of crisis, as migration results in a successful survival strategy. However, these gains do not necessarily persist in the context of a crisis at the destination because immigrant IMR can be highly sensitive to a local crisis, as seen for both diasporas under study in this analysis.
The patterns and trends documented here speak to the complexity of interrelated social and demographic processes such as armed conflicts, social unrest/upheavals, migration and mortality. Contrary to the classic assimilation model of immigrant adjustment, which suggests that the health outcomes of immigrant groups improve the longer they reside in the country of destination,23 24 our results show that migration’s positive effect on reducing diaspora IMR relative to the native-born and their countries of origin is not straightforward. The contradiction may arise from the fact that assimilation models are used to explain south-to-north migration flows. Our results are similar to those of other studies reporting excess mortality among diaspora IMRs relative to the native-born, which highlight that two of the leading non-demographic predictors of the differential are failure to detect complications and poor prenatal care.25
Limitations
We have focused on IMR and strategically combined a meticulously selected sample from the SBH (women who migrated before age 20 and women with up to one child born after their year of arrival), from census data and from the CRVS services in both countries. The migrant and non-migrant populations in these two countries can plausibly be compared due to their similar fertility trends. The main limitation of our study is the existence of birth order differentials in infant mortality, which makes our diaspora IMR estimates conservative. However, more detailed studies point to a neonatal mortality disadvantage for firstborns compared with later-born siblings, which later reverses during the postnatal period and throughout the life course.26 Because our data correspond to a retrospective collection, we believe our estimations somewhat smooth the differentials.
Although the IMR is internationally recognised as a fundamental measure of a population’s health, it does not cover all dimensions of this concept. In a context such as binational migration between Colombia and Venezuela, other equally important and relevant aspects are reproductive health, overall mortality and violence-related mortality, just to mention a few. We acknowledge the importance of these other measures and hope to see more research on these outcomes in the future.
Policy implications
The different diaspora IMR outcomes found in our study may be strongly related to healthcare access. Given that migrants’ survival (dis)advantages relative to the native-born are concentrated in the neonatal period,27 access to prenatal and postpartum care in the destination country is the key to reducing a crisis’ negative effects on newborns and their mothers. If health systems are overwhelmed and institutional barriers prevent migrants from accessing them, migration can be associated with worse mortality outcomes.
Health outcomes are better among the Colombian diaspora than for non-migrant Colombians, and even better than those of non-migrant Venezuelans during the crises. Since 1961, Venezuela has maintained a parallel contributory and unremarkable welfare system for assisting and protecting all persons in the national territory, regardless of whether or not they are native-born Venezuelans or otherwise citizens of the Venezuelan state.28 Likewise, the Colombian diaspora might benefit from having access to the health systems in both countries. In contrast, access to healthcare in Colombia is determined by the migrant’s legal immigration status. According to the Constitutional Court of Colombia’s 15 November 2017 unanimous sentence on SU677/17, access to the health system is limited to emergency services if a migrant has irregular residence status, which is the case for 56.4% of the Venezuelan diaspora in 2020.29
The Colombian government has undertaken many initiatives for regularising Venezuelan-born residency, from the Special Permanence Permit in 2017 to the implementation of a Temporary Protection Statute for Venezuelan Migrants in 2021. All these initiatives demand national ID documents, which represent a challenge for the Venezuelan diaspora. Therefore, their success in enlarging access to healthcare is limited. The most impactful initiative undertaken by the Colombian government may be the naturalisation of about 45 000 Venezuelan-born children in 2020.30 This measure avoided the risk of statelessness faced by the children and allowed better healthcare for these newborns. Further initiatives must be undertaken to provide prenatal care for the Venezuelan and other diasporas living in Colombia.
Supplemental material
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seema Biswas
Twitter @jennylind2000
Contributors All authors contributed equally. JA acts as guarantor author.
Funding JA received funding from the European Union's Horizon 2020 Excellent Science, Marie Skłodowska–Curie, Individual fellowship program 2019 (Grant agreement No: 892134). AF aknowledges funding from the Spanish MInistry of Science and Innovation through the Juan de la Cierva fellowship (FJC2020-042965-I).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The reflexivity statement for this paper is linked as an online supplemental file 1.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.