Article Text

Abstract
Background A few studies have assessed the epidemiological impact and the cost-effectiveness of COVID-19 vaccines in settings where most of the population had been exposed to SARS-CoV-2 infection.
Methods We conducted a cost-effectiveness analysis of COVID-19 vaccine in Kenya from a societal perspective over a 1.5-year time frame. An age-structured transmission model assumed at least 80% of the population to have prior natural immunity when an immune escape variant was introduced. We examine the effect of slow (18 months) or rapid (6 months) vaccine roll-out with vaccine coverage of 30%, 50% or 70% of the adult (>18 years) population prioritising roll-out in those over 50-years (80% uptake in all scenarios). Cost data were obtained from primary analyses. We assumed vaccine procurement at US$7 per dose and vaccine delivery costs of US$3.90–US$6.11 per dose. The cost-effectiveness threshold was US$919.11.
Findings Slow roll-out at 30% coverage largely targets those over 50 years and resulted in 54% fewer deaths (8132 (7914–8373)) than no vaccination and was cost saving (incremental cost-effectiveness ratio, ICER=US$−1343 (US$−1345 to US$−1341) per disability-adjusted life-year, DALY averted). Increasing coverage to 50% and 70%, further reduced deaths by 12% (810 (757–872) and 5% (282 (251–317) but was not cost-effective, using Kenya’s cost-effectiveness threshold (US$919.11). Rapid roll-out with 30% coverage averted 63% more deaths and was more cost-saving (ICER=US$−1607 (US$−1609 to US$−1604) per DALY averted) compared with slow roll-out at the same coverage level, but 50% and 70% coverage scenarios were not cost-effective.
Interpretation With prior exposure partially protecting much of the Kenyan population, vaccination of young adults may no longer be cost-effective.
- COVID-19
- Vaccines
- Health economics
- Epidemiology
Data availability statement
Data are available in a public, open access repository. All code and data for the transmission model and economic evaluation analysis underlying this study is accessible at the Github repository: https://github.com/SamuelBrand1/KenyaCoVaccines.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The COVID-19 pandemic has led to a substantial number of cases and deaths globally and COVID-19 vaccines are considered the main strategy of curtailing the pandemic. However, many African nations are still at the early phase of vaccination.
Evidence on the cost-effectiveness of COVID-19 vaccines is useful in estimating value for money and illustrate opportunity costs. Though, there is a need to balance these economic outcomes against the potential impact of vaccination.
WHAT THIS STUDY ADDS
In Kenya, a targeted vaccination strategy that prioritises those of an older age and is deployed at a rapid roll-out speed achieves greater marginal health impacts and is better value for money.
Given the existing high-level population protection to COVID-19 due to prior exposure, vaccination of younger adults is less cost-effective in Kenya.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Rapid deployment of vaccines during a pandemic averts more cases, hospitalisations and deaths and is more cost-effective.
Against a context of constrained fiscal space for health, it is likely more prudent for Kenya to target those at severe risk of disease and possibly other vulnerable populations rather than to the whole population.
Introduction
As of late May 2022, Kenya has experienced five distinct waves of the COVID-19 pandemic with more than 320 000 reported cases and 5600 deaths.1 While at the global level vaccines to prevent severe disease from SARS-CoV-2 are the main strategy for curtailing the pandemic burden on health,2 most African nations are still at a very early phase of vaccine roll-out, particularly in tropical sub-Saharan Africa, with most countries at less than 10% of the adult population fully vaccinated.1 However, in contrast to other part of the world where low vaccine coverage in high-risk groups has led to high mortality even from the omicron variant,3 in Kenya cross-sectional serological surveys of anti-SARS-CoV-2 spike protein antibodies together with transmission dynamic model forecasts indicate that about 80% of the population have been exposed to the virus at least once and thus generated considerable immunity4 with similar estimates in the region.5 This raises the question what additional benefit can vaccination still have in mitigating future disease burden from COVID-19?
The Kenyan government is pursuing a phased COVID-19 vaccination strategy that aims to follow a risk-prioritisation matrix leading sequentially to the vaccination of all adults by December 2022.6 The prioritised population are an estimated 30% of the adult population and include health and other essential workers, individuals at high risk of severe disease (those above 58 years, and those above 18 years with comorbidities), and individuals at high risk of infection (individuals in congregate settings, and those working in hospitality and transport sectors).6 Vaccine roll-out commenced in early March 2021. As of late May, 2022 more than 18.1 million doses had been administered with 31% of Kenya’s adult population above the age of 18 years being fully vaccinated.7 The initial procurement comprised of the Oxford/Astra Zeneca vaccine mainly sourced through the COVID-19 Vaccines Global Access Facility (COVAX) mechanism and bilateral negotiations, evolving more recently to a multivaccine type deployment through additional sources including the African Union’s African Vaccine Acquisition Task Team mechanism.6
Economic evaluations are useful in providing evidence of the value for money for different health interventions and illustrates the opportunity costs of the interventions in a setting with many competing priorities. However, there is a need to balance these economic outcomes against the potential impact of the interventions. Therefore, this study evaluates the potential epidemiological impact and cost-effectiveness of different vaccine roll-out scenarios in a Kenyan population that has already acquired a high-level immunity due to prior infections. The study employs a partially retrospective perspective with vaccination scenarios beginningon September 2021 and with an immune escape variant striking in November 2021.
Methods
Study setting
Kenya is a lower-middle income country with a gross domestic product (GDP) per capita of US$1838.21.8 The population as of 2019 was estimated at 47.56 million with a predominantly young population: 50% of the population are 19 years and below and only 11% of the population are 50 years and above.9 As of late May 2022, most COVID-19 cases were reported among those aged 20–49 years (n=2 04 756, 63%), followed by those above 50 years (n=86 275, 27%), and lastly among those 0–19 years (n=33 328, 10%).10 The reported case fatality rate as of late May 2022 was 1.7% with deaths increasing with age at 3% (163 deaths) among those 0–19 years, 23% (1,292 deaths) among those 20–49 years and 74% (4194 deaths) among those above 50 years of age.10
Study design
This study is an impact and cost-effectiveness analysis of COVID-19 vaccine roll-out strategies that uses cost estimates from primary costing studies and vaccine effectiveness measures from an age structured transmission model. The costs and effects are estimated from a societal perspective for a period of 1.5 years (1 September 2021 to 28 February 2023) starting at the peak of the Kenyan delta wave and simulating the emergence of a partial immune escape variant (omicron-like) from November 2021.
Intervention comparators
Primary analysis
We carry out an incremental analysis of four vaccination coverage scenarios deployed over an 18-month period (non-rapid deployment), starting at 0% coverage in September 2021 (table 1): No vaccination (0% coverage), or 30% 50% and 70% coverage of the population older than 18 years with prioritisation of those aged 50 years and above (until 80% of those >50 years old are fully vaccinated), then the remaining doses given to those 18–49 years).
Intervention comparators and number vaccinated within 1.5 years’ time horizon
Secondary analysis
We consider a secondary analysis that assesses the same scenarios under the primary analysis but with rapid vaccine deployment in which the targeted vaccine coverage is attained within 6 months of starting vaccination.
An assumption was made that all the vaccination coverage scenarios and deployment strategies were implemented alongside a low intensity mix of non-pharmaceutical interventions (NPIs). The low intensity NPI is matched with how government progressively lifted or modified the restrictions and refers to reopening of international borders, relaxed curfew, controlled public gatherings, controlled reopening of restaurants and bars, controlled reopening of schools, ban lift on mandatory use of masks and adherence to hand hygiene from November 2020 to the time of writing this manuscript. Further, we assume administration of the Oxford-AstraZeneca vaccine across all vaccination strategies, as it was the predominant vaccine in the country, at the time of analysis.
Transmission modelling and parameter inference
We extended a dynamic SARS-CoV-2 transmission model previously designed to estimate population level immunity from natural infection in Kenya by fitting to case notification and serological data4 to include additional age structure and vaccination status. In common with other approaches to modelling SARS-CoV-2 transmission,11 12 we assume that the rate of new infections depends on: (1) age and setting-specific contact rates within the population, (2) frequency of Alpha, Beta and Delta variants of SARS-CoV-2 among the infected subpopulation, (3) the first and second dose vaccine protection against infection in each age group which were assumed to wane over time and (4) prior primary infections. The probability of being infected with SARS-CoV-2 per infectious contact, and the chance of developing symptoms on infection, increased substantially with age (see online supplemental information and online supplemental figure 1) for details of the transmission model).
Supplemental material
Supplemental material
The goal of the transmission model is to project the health gains of the vaccine deployment strategies described above in comparison with the no vaccine scenario. This requires estimation of parameters pertaining to the risk of transmission, and, of risk factors associated with infection given age, and the infecting variant of SARS-CoV-2 in the Kenyan setting. These parameters were inferred by fitting the model to the following Kenyan epidemiological data (see online supplemental file 2 for inference methods).
Daily reported numbers of positive and negative PCR tests from the Kenyan Ministry of Health COVID-19 linelist (between 1 January 2021 and 1 November 2021).
Cross-sectional serological surveys of (1) donor samples from the Kenyan National Blood and Transfusion Service13 and (2) demographic surveillance systems (between 1 January 2021 and 27 May 2021).14
We used a Bayesian hierarchical inference approach aimed at allowing inference on reporting fraction in counties with higher numbers of serological tests to influence inference of reporting fraction in counties with lower numbers of serological tests (see online supplemental information) for details on underlying data for age-specific effects and details on inference methodology).
Infection outcome modelling and risk factor inference
Bayesian inference of transmission model parameters generated a posterior predictive distribution for the number of SARS-CoV-2 infections in Kenya broken down by day, county, age of infected, infecting variant of SARS-CoV-2, and, whether it was a primary infection event or a reinfection event. We categorised the outcome of each infection as being either deadly, critical (requiring treatment in an intensive care unit (ICU)), severe (requiring in-patient hospitalisation in a general ward), mild or asymptomatic. Severe and critical infections were assumed to cause admission to a health facility’s general ward or ICU for an average of 12 days postinfection. Severe infection was assumed to lead to an average 7-day stay in a general COVID-19 ward before discharge. Critical infection leads to an average 7-day stay in ICU,15 before transfer to a general COVID-19 ward for a further average 7-day stay before discharge (see online supplemental information) for details on hospital durations of stay).
Risk factors for infection outcome were inferred using reported Kenya outcome data:
Daily reported numbers occupying general health facilities with COVID-19 as the diagnosed cause (1 March 2021–1 November 2021).
Daily reported numbers occupying ICUs with COVID-19 as the diagnosed cause (1 March 2021–1 November 2021).
Daily reported incidence of death with COVID-19 as the diagnosed cause (1 January 2021–1 November 2021).
Vaccination roll-out modelling
We used the fitted model to predict the course of the pandemic from 1 September 2021 (historically this was past the peak of the fourth wave of cases in Kenya) to 30 June 2023 and the impact of vaccination on, severe and critical disease, and deaths. We distribute the total number of doses planned under each vaccination scenario to the 47 counties proportionally according to population size above the age of 18 years.9 We assume that the number of doses given per day will be the same during the study period. Doses will be offered to adults older than 50 years first, until take up of available vaccines dropped off, which we assumed would occur once 80% of over 50s had taken up both doses. The remaining doses will subsequently be randomly allocated to all 18–50 years. Within the model, individuals are either unvaccinated, partially vaccinated (14 days after receipt of the first dose), fully vaccinated (14 days after receipt of the second dose) or have waned vaccine effectiveness. We assumed vaccine effectiveness against death (delta variant) to range from 90% to 95% after the first dose and 95% to 99% after the second dose.16 Vaccine effectiveness against severe or critical disease (delta variant) of 80%–90% and 95%–99% after the first and second dose, respectively.16 The vaccine effectiveness against acquisition of infection per infectious contact (delta variant) was 55%–65% and 65%–80% after the first and second dose, respectively.16 We assumed an effectiveness of 0%–35% and 0%–69% against onward transmission, per infection (delta variant), after either the first or second dose.17 We assume that immunity due to either past infection of vaccination eventually wanes to 70% protection against disease and 0% protection against infection, with a mean time to complete waning of 460 days after the second dose of vaccine and 5 years following natural infection.18 19 Furthermore, we assume that protection due to prior infection combined constructively with vaccination; that is that people who had previously had a natural infection episode of SARS-CoV-2 were further protected from reinfection by vaccination (see online supplemental information and online supplemental figures 2–4).
Supplemental material
Supplemental material
Supplemental material
Immune escape variant
The scenarios investigated in this paper involve the rapid spread of a new variant of SARS-CoV-2 that, due to evolutionary adaptation, partially avoids protection from infection due to prior naturally acquired immunity and/or vaccination. Concretely, we assume that the immune escape variant enters Kenya in early November 2021 and rapidly dominates transmission by 15 November 2021. Compared with homologous protection against reinfection with the Delta variant, the protection afforded by prior infection and/or vaccination against acquiring the novel immune escape variant is assumed to be decreased by 50%, with all epidemiological rates increased such that the mean generation time of transmission is reduced by 30% compared with the transmission of the Delta variant. However, we also assume that the fundamental reproductive number and risk factors for severe, critical and deadly outcomes are unchanged compared with Delta (see online supplemental information for the details of how a 50% decrease in protection from infection was implemented).
Cost estimates
The cost estimates used in this study were derived using a hybrid method that involved both an ingredients approach (bottom-up) and a top-down approach.20 21 The analysis used economic costs, which reflect the opportunity cost and incorporated both recurrent and capital costs. Capital costs were annuitised using a discount rate of 3% over their useful life. Costs incurred in other years were adjusted for inflation using the GDP deflator and reported in 2021 United States Dollars. Key model cost input parameters are shown in table 2 and the three main cost components are described below. The costs of NPIs were excluded as all vaccination strategies employed the same NPI regimen (low NPI intensity) and would therefore not change the reported incremental cost-effectiveness ratios (ICERs).
Key analysis parameters
Supplemental material
Vaccination costs
We included vaccine and related supplies costs, as well as vaccine delivery costs. Vaccine and related supply costs were the economic costs to purchase the vaccine and related supplies such as syringes and safety boxes through the COVAX facility. A base cost of US$7 was used for vaccine procurement, which is the country’s procurement cost from the COVAX facility. Additionally, the freight costs, insurance costs, import declaration fees, clearance fees and the railway development levy associated with the vaccines and its supplies were included. Vaccine and syringe wastage rates of 10% were assumed.22 Vaccine delivery costs referred to costs associated with delivering COVID-19 immunisations to the adult population and were estimated across six components (1) vaccine supply chain (2) vaccine safety monitoring and adverse events following immunisation management (3) training (4) advocacy, communication and social mobilisation (5) data management, monitoring and supervision (6) vaccine administration. The resource used and costs were estimated through the analysis of programmatic budgets, and through key informant interviews. Details of the vaccine procurement and delivery cost analysis and results are reported elsewhere.22 This analysis assumed equivalent vaccine delivery costs for both the rapid and non-rapid vaccination strategies.
Treatment costs
The direct medical costs of COVID-19 treatment were sourced from a recently conducted study that examined the unit costs for COVID-19 case management in Kenya.23 This costing analysis employed an ingredients-based approach to estimate healthcare costs across the disease severity categories; with the exclusion of adverse events costs.23
Productivity losses
Productivity losses due to illness and mortality were estimated using a human capital approach.24 The impact of COVID-19 on lost time through illness or morbidity was estimated by accounting for the average Kenyan’s productivity measure (GDP per capita) and duration of disease/duration of quarantine; the latter was used where duration of illness was less than the 14-day quarantine period in Kenya. For asymptomatic and mild disease, the testing rate was accounted for and an assumption was made that only those in the informal sector are likely not to be productive as they isolate. Further, the economic impact of COVID-19-related mortality was estimated by considering the years of life lost (YLL) because of premature mortality and the average productivity measure. We did not account for productivity losses from long COVID-19, as the burden is poorly defined in our setting (see equation (a) in the online supplemental information).
Disability-adjusted life-years
The outcome of the cost-effectiveness analysis was reported in terms of disability-adjusted life-years (DALYs); the sum of YLL and years lost due to disability25 (see equations b, c and d in online supplemental information).
DALYs were calculated considering a discount rate of 3%, the Kenyan 2019 standardised life expectancies,26 assumed duration of illness of 7 days for asymptomatic and mild disease and 12 and 20 days for severe and critical disease, respectively,27 as well as disability weights. COVID-19 is a novel disease, and its disability weights are currently not available. Therefore, for asymptomatic COVID-19 disease we assumed a disability weight of 0. For mild-to-moderate COVID-19 symptoms and severe disease, we used disability weights from the 2013 Global Burden of disease of 0.051 (0.032–0.074) and 0.133 (0.088–0.190) assigned to infectious disease with moderate acute episodes and severe episodes, respectively.28 For critical disease, we assume disability weights of 0.655 (0.579–0.727) assigned to ICU admissions.29 This analysis did not incorporate age-weighting in the DALYs. These input parameters are reported in table 2.
The ICER was the measure of cost-effectiveness calculated as the net change in total costs and DALYs averted between comparators. The ICER was compared with the opportunity cost-based on Kenya’s cost-effectiveness threshold (US$919.11).30 31

Where
Costindex=cost of strategy of interest.
Costbaseline=cost of the next less effective strategy.
DALYindex=total DALYs under the strategy of interest.
DALYbaseline=total DALYs under the next less effective strategy.
ICERs are estimated within each of the two roll-out scenarios slow and rapid and are not comparable between the two vaccine-deployment cases except when the baseline is no vaccination.
Sensitivity analysis for the model
Vaccine effectiveness against different epidemiological outcomes such as the acquisition of disease, onward transmission, severe disease and death does vary with age, duration between vaccination and testing of efficacy, variant of infection and type of vaccine being used among other factors.32–35 Therefore, to determine the robustness of the epidemiological model predictions to the vaccine effectiveness parameter values, we performed a sensitivity analysis across a range of values using a vaccine waning effectiveness model fitted to the UK Health Security Agency COVID-19 data.16 17
A univariate sensitivity analysis was done on the economic model to determine the robustness of the unit cost estimates with variations in vaccine procurement costs (base cost of US$3 and US$10 used) and discounting rates of DALYs (rate of 0% used). Further, given the current evidence gap to confidently determine the magnitude of underreporting of COVID-19 deaths,36 the baseline cost-effectiveness analysis assumed an under-reporting of hospitalisation and deaths by a factor of 5 and a one-way sensitivity analysis was done by varying the under-reporting factor (1–4).
A probabilistic sensitivity analysis to explore the influence of some economic parameters on the ICERs was done using Sobol sampling and was based on the statistical distributions in online supplemental table S2. Sobol sequences belong to the family of quasi-random sequences which are designed to generate samples of multiple parameters as uniformly as possible over the multidimensional parameter space.37 For the parameters used in the probabilistic sensitivity analysis, the statistical distributions were chosen to model the available prior knowledge represented by existing data, as reported in table 2. For the cost estimates range, a 20% increase or decrease was assumed for the parameters.
Supplemental material
All code and data for the transmission model and economic evaluation analysis underlying this study is accessible at the Github open code repository.38
Patient and stakeholder involvement
No patients were involved in this study. The results of the study will be disseminated to key policy-makers and relevant stakeholders involved in COVID-19 vaccine deployment in Kenya. See online supplemental file 1 for author reflexivity.
Supplemental material
Results
Clinical impacts of vaccination strategies and scenarios
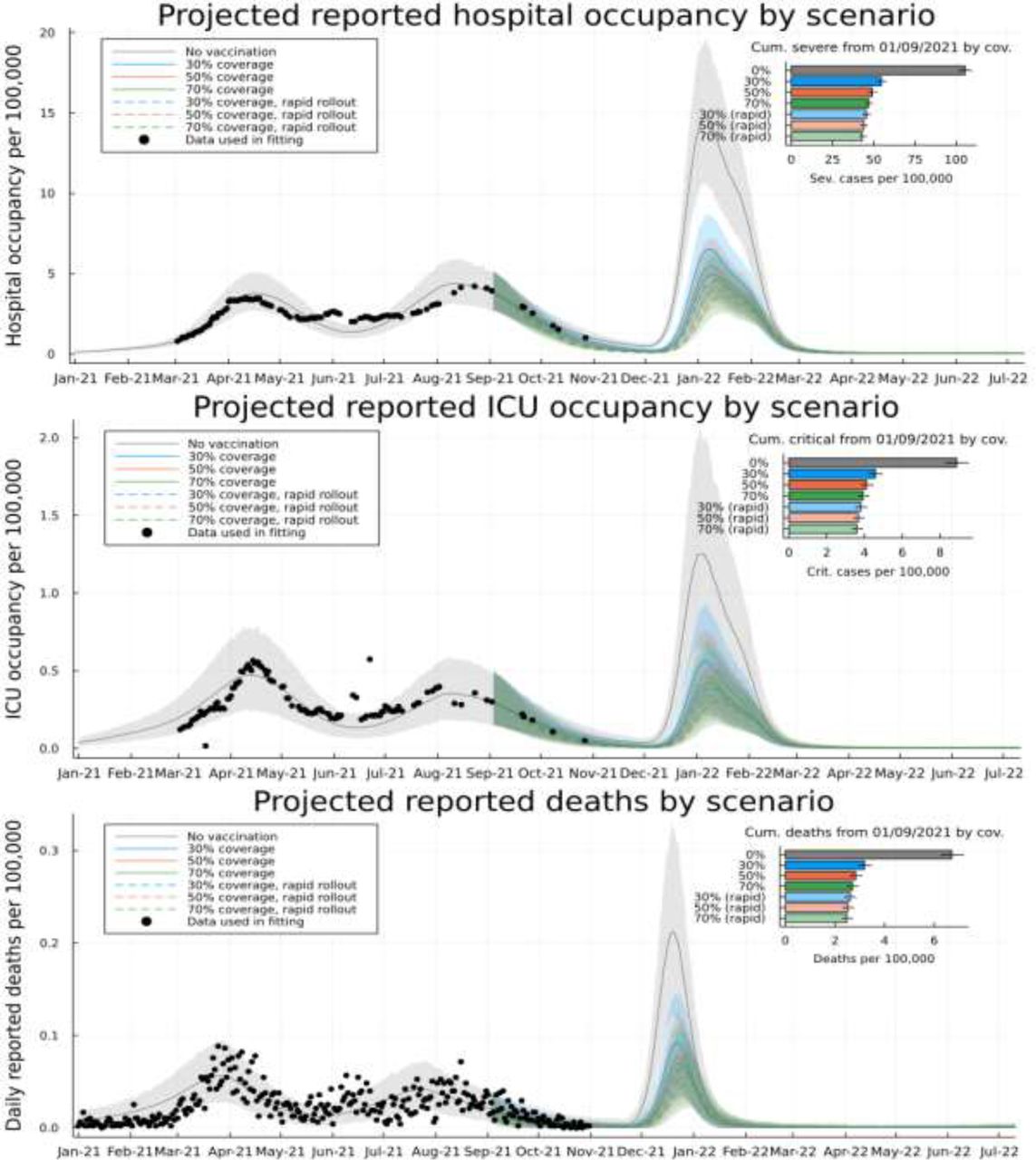
The non-rapid deployment of vaccinating 30% of the adult population results in 10% (32 (24–38) per 100 000) fewer infections, 54% (8132 (7914–8373) fewer deaths compared with no vaccination, and 978 (949–1005) people would need to be vaccinated to prevent 1 death. An increase of vaccine coverage of the adult population to 50% results in a further 1% (4 (3–5) per 100 000) reduction in infections, a further 12% (810 (757–872) reduction in deaths, and 5617 (5218–6011) more people would need to be vaccinated to prevent an additional death. Similarly, an increase of vaccine coverage to 70% leads to a 1% reduction in cases, a 5% reduction in deaths, and 17 730 (15 773–19 920) more people would need to be vaccinated to prevent an additional death compared with the 50% vaccination coverage.
In the rapid vaccine roll-out strategy, the 30% vaccine coverage averts 12% of cases preventing an average of 39 (29–48) per 100 000 infections and 63% of deaths saving an average of 9433 (9197–9711) lives compared with no vaccination. Therefore, 843 (819 to 864) people would need to be vaccinated to prevent a death. The 30% coverage under a rapid deployment averts more cases and saves more lives compared with a non-rapid roll-out with the same level of coverage (see table 3 and figure 1.)

Model-based projections and vaccine scenarios: model-based prediction intervals for daily occupancy of general wards in health facilities in Kenya (top), daily occupancy of intensive care units in Kenya (middle) and daily reported incidence of death with COVID-19 in Kenya (bottom). All scatter points represented data used in inference of the infection outcome model. Grey curves are the posterior mean model prediction (background shading 95% CIs) with no vaccinations. Coloured curves represent a target of 30% (blue), 50% (red) and 70% (green) of over 18-year-old population in Kenya over 18 months (solid) or 6 months (dashed). Insets: projections of cumulative number of severe (top), critical (middle) and deadly (bottom) cases after 1 September 2021 under each vaccine target scenario. ICU, intensive care unit.
Projected clinical outcomes, costs and the cost-effectiveness of different vaccination strategies in Kenya from a societal perspective
Cost-effectiveness of vaccination strategies
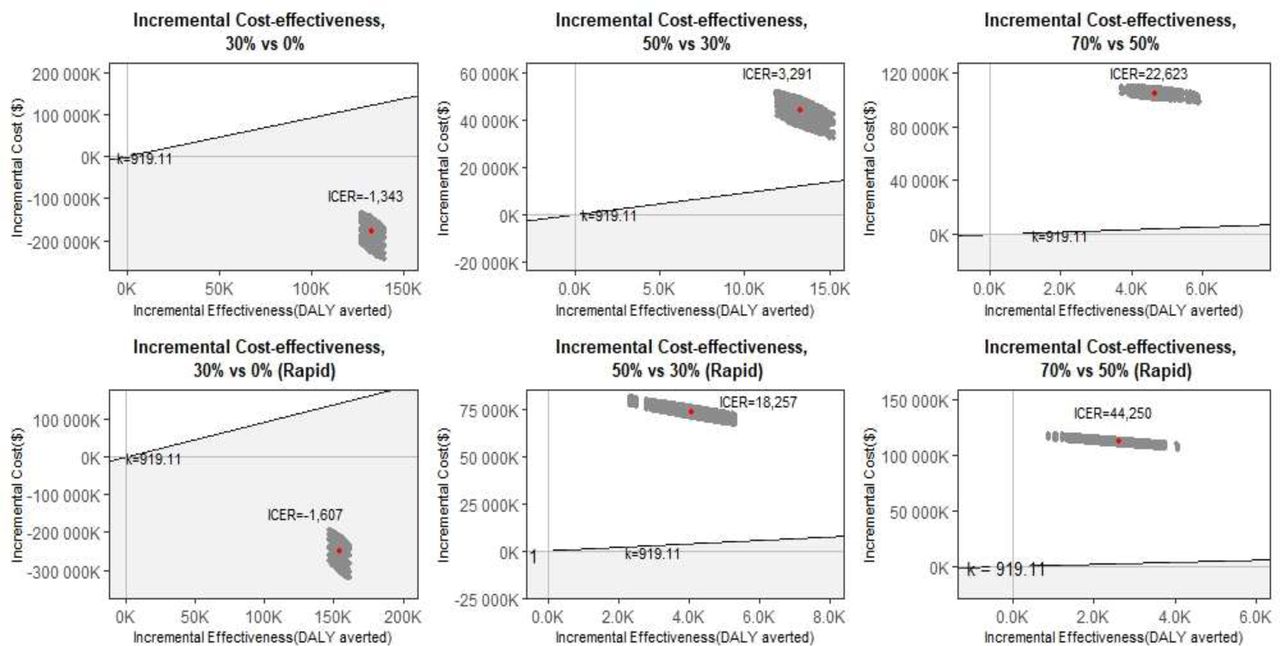
Table 3 shows the total costs, DALYs and ICERs of the vaccination scenarios considered in the analysis from a societal perspective. Under the non-rapid vaccination scenario, vaccinating 30% of the adult population is cost-saving (ICER=US$−1343 (US$−1345 to US$−1341) per DALY averted) and hence highly cost-effective. Increasing vaccine coverage to 50% of the adult population was not cost-effective (ICER=US$3291 (US$3287 to US$3295) per DALY averted) compared with 30% coverage. Similarly, increasing vaccine coverage to 70% was deemed not cost-effective (ICER=US$22 623 (US$22 602 to US$22 645) per DALY averted) compared with 50% coverage at a cost-effectiveness threshold of US$919.11.
Under the rapid vaccination scenario, a 30% vaccine coverage strategy was even more cost-effective ICER=US$−1607 (US$−1609 to US$−1604) per DALY averted compared with no vaccination. The ICERs of 50% and 70% coverage strategies under the rapid scenario are US$18 257 (US$18 226 to US$18 287) and US$44 250 (US$44 126 to US$44 374) per DALY averted compared with 30% and 50% coverage strategies, respectively, and hence are not cost-effective.
Sensitivity analysis
Table 3 presents the univariate sensitivity analysis of under-reporting of hospitalisations and deaths, from a societal perspective. Assuming no under-reporting or adjusting the under-reporting factor to 2, results in all the scenarios having ICERs above the cost-effectiveness threshold, except the 30% coverage with a rapid deployment. On the other hand, with an under-reporting factor of 3 or 4, 30% coverage with a rapid and non-rapid vaccination scenario remained cost saving.
Online supplemental figure S5 summarises the effects of vaccine prices and discounting rates of DALYs on the ICER. Vaccine prices, of the two parameters had the largest effect on the ICERs: leading to a 32%–103% decrease and a 36%–77% increase in ICERs across the different vaccination scenarios.
Supplemental material
The one-way sensitivity analysis focusing solely on a health system’s perspective is presented in online supplemental table S3. When considering this perspective, the total costs across the vaccination strategies increase as coverage increases, as reported from a societal perspective. However, the no vaccination scenario affords the least costs (US$313 million). The reported ICERs increase with increased coverage and the 30% coverage with a non-rapid and rapid vaccination pace are below the threshold: ICER=US$555 (US$553 to US$557) and US$291 (US$290 to US$295) per DALY averted, respectively, and considered cost-effective from a health system’s perspective.
Supplemental material
Figure 2 represents the findings of the probabilistic sensitivity analysis from a societal perspective. The region below the cost-effectiveness threshold line and within the grey region, shows all the points that are cost-effective at a cost-effectiveness threshold of US$919.11. For instance, the dominance of the 30% coverage scenarios (ie, more effectiveness at a lower cost) compared with no vaccination, was shown in 100% of the replications (ie, 100% of the cost-effect pairs were in the southeast quadrant). Further, 100% of the replications for 50% coverage and 70% coverage strategies (both rapid and non-rapid roll-out) were in the northeast quadrant (implying that these strategies were more costly but also more effective compared with the 30% and 50% coverage strategies, respectively).
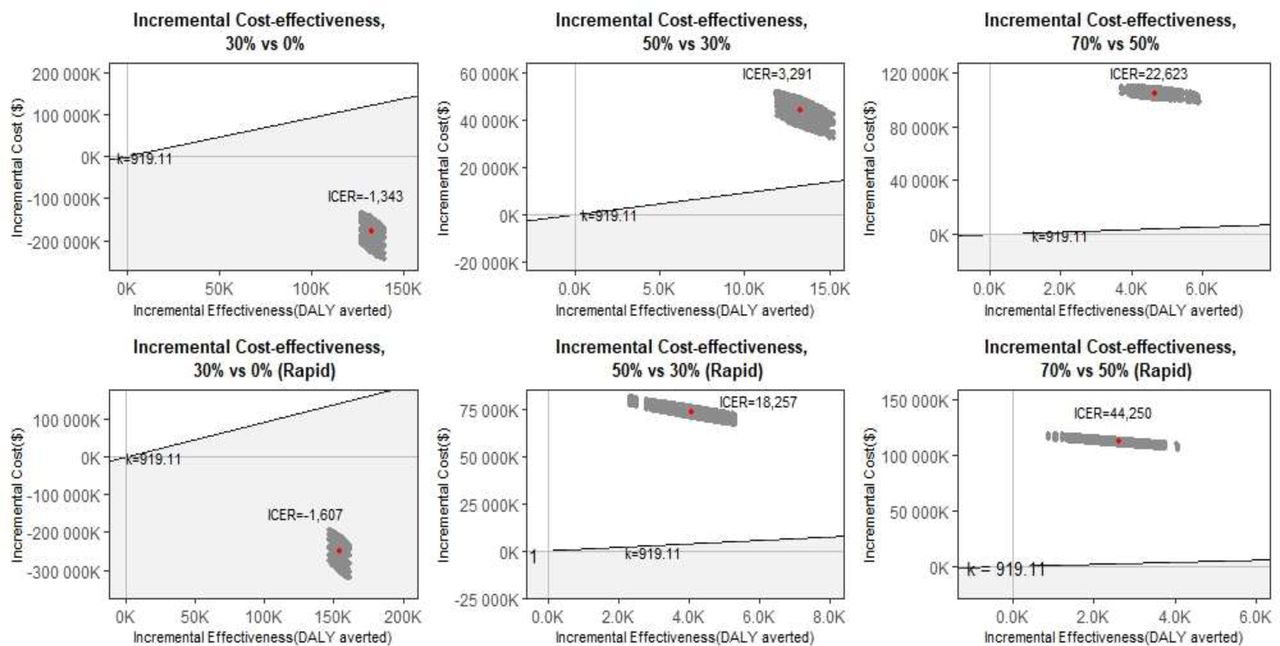
Probabilistic sensitivity analysis of different vaccination strategies from a societal perspective. The first row shows the vaccine scenarios comparisons under a non-rapid roll-out pace while the second row shows the rapid roll-out results. Each grey dot represents a pair of values of incremental cost and incremental effectiveness and the red point is the mean ICER points for each vaccine comparison. The grey shaded area below the diagonal cost-effectiveness threshold line (k=US$919.11) shows the cost-effective region. DALY, disability-adjusted life-year; ICER, incremental cost-effectiveness ratio.
Figure 3 presents the cost-effectiveness acceptability curves of the analysis from a societal perspective based on a range of cost-effectiveness thresholds. Under the non-rapid vaccination roll-out and given a US$3300 willingness to pay threshold, the probability of the 50% coverage strategy being cost-effective compared with 30% coverage would be 0.5. Further, there was 0.5 probability that the 70% coverage in comparison to 50% coverage would be cost-effective at a threshold of US$22 600 in the non-rapid deployment.

{kind=link}
{kind=link}
{kind=link}
Cost-effectiveness acceptability curves (CEAC) showing the probability that each index scenario is cost-effective compared with the comparator over a range of cost-effectiveness thresholds (k=cost-effectiveness thresholds, pr=probability of cost-effectiveness).
Discussion
We assessed the epidemiological impact and cost-effectiveness of a range of COVID-19 vaccine deployment strategies and scenarios in Kenya. Our findings show that if Kenya had started with a full-scale vaccination programme in September 2021 and with an omicron-like variant introduced in November 2021, the deployment of COVID-19 vaccines in the Kenya population would likely avert a substantial number of cases, hospitalisations and deaths from COVID-19. We find that a strategy to vaccinate mostly older adults (80% of those over 50 years) who are at high risk of severe disease but which achieves low (30%) overall population coverage, yields the greatest reductions in severe infections and deaths per fully vaccinated adult. The marginal health benefits decrease with higher vaccine coverage levels (50% and 70%) as an increasing proportion of low risk younger adults, most with some immunity from previous infection, are vaccinated. These diminishing returns of increased coverage result in only the programme for older adults (ie, the 30% coverage scenario) being cost-effective while the expansion to younger age groups (ie, 50% and 70%) was found not cost-effective. Further, where an upsurge of SARS-CoV-2 occurs shortly after scale-up of vaccination (as modelled in this study) then deployment strategies that achieve rapid coverage of the target groups are more effective compared with slow vaccine deployment strategies.
Our findings are similar to evidence from South Africa, Madagascar, Pakistan, UK and USA that found vaccinating their population would decrease COVID-19 infections and deaths compared with a no vaccination scenario11 39–42 and increasing vaccination coverage would increase the clinical benefits.39 41 The South African study also found that a rapid vaccination roll-out pace resulted in ‘better’ clinical outcomes (infections and deaths averted) and economic effectiveness compared with a non-rapid roll-out pace.39 The studies done in Madagascar, UK and USA reported a greater impact when distribution of vaccines was prioritised according to the number of people of an older age in the region or among the elderly, reflecting similar findings to our study.11 40 42 However, in contrast to the South African and Pakistan studies39 41 who found that higher coverage scenarios had higher marginal impacts, we found that a minimal vaccine coverage of 30% of the adult Kenyan population targeting older age groups had the highest marginal impact. These differences could be explained by differences in the demographic profiles of the different populations of study. Higher population coverage with the COVID-19 vaccines have greater health impacts in countries that have higher proportions of the elderly and/or low previous exposure to COVID-19.
Using a societal perspective (that incorporates health system costs and productivity losses), we find that COVID-19 vaccination in Kenya is most cost-effective when targeted at older age groups in the population. This is because all our scenarios have the elderly covered first, and the incremental impact of increasing vaccination coverage among younger populations was less value for money. Given that the proportion of the elderly population in Kenya is low (11% of total population are aged 50 years and above),9 targeting the COVID-19 vaccine to this vulnerable population achieves high cost-effectiveness at relatively low population-level vaccine coverage; 30% coverage of the population ensures that the maximal 80% of the older age group is vaccinated and a very low coverage of the younger age group (19%). Accounting for productivity losses improves the cost-effectiveness profile of COVID-19 vaccines, compared with when only direct health system costs are considered. For instance, for the 30% coverage scenarios with both a non-rapid and rapid deployment pace, the ICERs decreased on average by 342% and 652%, when the societal perspective was considered as opposed to the health system perspective, and as a result improving the cost-effectiveness profile. This underlines the limitations of using a narrow health system perspective that ignores broader societal costs of health system interventions. This is even more so for a vaccine deployed in a pandemic that has substantial socioeconomic impacts, in addition to health impacts. These findings mirror cost-effectiveness studies of COVID-19 vaccination done in Turkey and Pakistan that found that although COVID-19 vaccination strategies were cost-effective from a health system’s perspective, they were cost saving from a societal perspective.41 43 This is in line with arguments from studies that estimate the public health value and impact of vaccination, which argue the need to broaden the perspectives for cost-effectiveness analysis of vaccines, as their impact is far-reaching, especially in the context of a pandemic.44–46
These findings have implications for COVID-19 vaccination policy in Kenya and other low-income and middle-income countries settings with comparable demographic and COVID-19 epidemiological profiles. First, not unexpectedly, where an outbreak is imminent efforts to rapidly deploy the vaccine not only avert more cases, hospitalisation, and deaths, but are also more cost-effective. By extension, had Kenya been able to deploy vaccines more rapidly, benefits would have been greater. Second, COVID-19 vaccination is likely to offer the best value for money when targeted to older age groups and possibly other vulnerable groups (such as those with risk increasing comorbidities) with high risk of severe disease and death, rather than to the whole population, in settings with overall low risk of severe disease and deaths, and high natural immunity due to previous exposure. This has several further implications. Kenya and other similar settings will achieve better health impacts and value for money with relatively small numbers of vaccines targeting the high-risk sections of the population. Against a context of constrained fiscal space for health, it is likely more prudent for Kenya and other African countries to target the vulnerable rather than whole populations. This consideration is likely to be even more relevant as African countries consider two shifts; the eligibility of children (below the age of 18 years) to COVID-19 vaccination and the transition to endemicity. If an endemic scenario will require annual vaccinations, Kenya and other African countries are unlikely to afford yearly vaccinations of their entire population. It is also apparent that such a strategy (vaccinating the entire population) is unlikely to be cost-effective, necessitating the need for Kenya and other African countries with comparable demographic and epidemic profiles to be both pragmatic and evidence-based in setting COVID-19 vaccine coverage policies and targets that are both feasible, effective and cost-effective in their contexts (rather than replicating high income country strategies).
These results should be interpreted within the context of several limitations. First, our results are dependent on model assumptions and input parameters, as is the case with all modelling studies. We selected transmission model parameters based on published literature and available observation data. However, some data were limited, lacking or uncertain and therefore we assumed our ‘best’ estimate for Kenya. For example, we used estimates of vaccine effectiveness based on UK data and assume a duration of 14 days between vaccination and peak efficacy within our model structure. We noted from literature,32–35 vaccine effectiveness varies with age, duration between vaccination and testing of efficacy, variant of infection and the type of vaccine among other factors. The model does not consider the different professions of the population such as essential workers (healthcare workers, teachers, among others) as it focusses on age as the key risk group. However, front-line workers may be important to target since preventing infection among them lessens the potential impact on health and learning capacity. The latter might become more influential in the future with new vaccines if they are more effective in preventing re-infection and mild symptoms than current generation of vaccines. Second, sub-Saharan African countries like Kenya have notably reported lower cases and deaths compared with other countries across the globe, this could be attributed to their lower testing capacity. Hence, we assumed an under-reporting factor of 1:5 in hospitalised cases and deaths. Third, we instituted vaccination roll-out near in time to the introduction of a new variant, which enhances the benefit of rapid over slow roll-out. Distance between vaccine introduction and the emergence of an immune escape variant is likely to favour slower vaccine roll-out. Fourth, assumptions about wanning immunity (natural and vaccine) and varying protection depending on variants affect the results. We; therefore, acknowledge the need to further investigate duration of protection accorded by both vaccines and natural immunity. Fifth, at the time of writing this (May 2022—over 1 year after the start of the vaccination campaign in Kenya), only 1% of the adult population had received booster doses.47 As a result, we did not include booster doses in this analysis but recognise that their inclusion may change the findings by improving the epidemiological impact of the vaccines as well as increase the costs of the vaccination programme. Sixth, in relation to the economic evaluation, although the cost-effectiveness analysis was conducted from a societal perspective, some costs have not been fully captured due to unavailability of data. These costs include household indirect costs incurred due to COVID-19 illness (eg, transport costs), costs as a result of long-COVID, and reduced productivity for those in the formal sector with asymptomatic/mild disease. In the latter, although we assume that they can resume work from home/places of quarantine they may have reduced productivity which is not captured in this analysis. These costs not captured in the analysis are however expected to be minimal. Seventh, the analysis assumed similar vaccine delivery costs for both rapid and non-rapid vaccination across similar coverage levels. However, it is likely that the rapid vaccination scenario may need more resources, especially cold chain equipment to hold larger batches of vaccines at a time. Eighth, the reported uncertainty of the ICER likely does not capture the full extent of the uncertainty, given the uncertainty of the costs of a yet to be established adult vaccination programme in Kenya. Lastly, the economic evaluation considers a 1.5-year time frame, potentially excluding costs and benefits of COVID-19 that may accrue over a longer period of time.
Conclusion
This study contributes to the growing body of literature on the health impact and cost-effectiveness of COVID-19 vaccines. Kenya will achieve both greater marginal health impacts and better value for money if it prioritises a targeted vaccination strategy among those at increased risk of severe disease and at a rapid roll-out speed. The cost-effectiveness of the COVID-19 vaccine should be considered alongside other priority setting considerations in the Kenyan context.
Data availability statement
Data are available in a public, open access repository. All code and data for the transmission model and economic evaluation analysis underlying this study is accessible at the Github repository: https://github.com/SamuelBrand1/KenyaCoVaccines.
Ethics statements
Patient consent for publication
Ethics approval
The KEMRI Scientific and Ethics Review Unit approved this study under KEMRI/SERU/CGMR-C/4244
Acknowledgments
We would like to acknowledge the Health Intervention and Technology Assessment Program (HITAP) and the Africa CDC Health Economic Program for their advice on the analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Lei Si
Twitter @AmbroseAgweyu, @edwinebarasa
DJN and EB contributed equally.
SO and JO contributed equally.
Contributors EB, DJN and PB conceptualised the study. SO, JO, CO, AK, RA, MO, AA, GMW, SU, EO, LIO-O, CNA, KK, PA, MM, RAA, WN, IMOA, JAGS, PB and EB acquired the data. SPCB, JO, SO and CO analysed the data. SO, JO, SPCB, CO, PB, DJN and EB were involved in the interpretation of the data and work. SO and JO wrote the first draft of the manuscript which was subsequently revised for important intellectual content by all authors. All authors read and approved the final manuscript. EB and DJN are responsible for the overall content as guarantors.
Funding This work was supported by funding from the Bill and Melinda Gates Foundation funded International Decision Support Initiative (IDSI), and funding from the National Institute for Health Research (NIHR) Global Health Research Unit on the Application of Genomics and Modelling to the Control of Virus Pathogens (17/63/82), on Mucosal Pathogens (16/136/46), and on Tackling Infections to Benefit Africa (16/136/33),using UK aid from the UK Government to support global health research, The UK Foreign, Commonwealth and Development Office and Wellcome Trust (grant# 220985/Z/20/Z).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.