Article Text

Statistics from Altmetric.com
Summary box
The AIDS and COVID-19 pandemics are intersecting at multiple levels.
Both pandemics have previously been described as wicked problems and can be studied as complex adaptive systems.
We recently designed a qualitative model of all known factors influencing HIV drug resistance (HIVDR) in sub-Saharan Africa and analysed its complexity as a complex adaptive system. Our detailed systems map featured three main feedback loops driving HIVDR.
Visualising both pandemics in one systems map confirms the urgency to address both simultaneously in order to mitigate a prolongation of the current COVID-19 pandemic and a rise in drug-resistant HIV.
Also at local level, a visualisation of the effects of the COVID-19 pandemic and response measures on the HIVDR system is valuable in gaining an understanding of its system-wide impact when rapid public health action is needed.
Concern is justified observing the link between the AIDS and COVID-19 pandemics. COVID-19 outcomes are significantly worse in many people living with HIV (PLHIV), even when vaccinated, because of their impaired immune system. Moreover, CD4 T-cells are affected by both HIV and SARS-CoV-2.1–3 SARS-CoV-2 variants can evolve in immunosuppressed patients due to prolonged viral replication in the context of an inadequate immune response.4 Accelerated intrahost evolution of SARS-CoV-2 was reported in a South African HIV patient with antiretroviral therapy (ART) failure.5 6 With 25 million HIV patients in sub-Saharan Africa (SSA) of whom an estimated 8 million are not virologically suppressed, this potentially creates a reservoir for future variants. Such variants, arising in PLHIV anywhere in the world, can spread to other continents, as has been reported for variants of concern (VoCs) (Beta, Omicron) and variants of interest (B.1.6.20, B.1.640.2) that arose in Africa.7–9 Conversely, the COVID-19 pandemic impacts HIV treatment programmes, due to supply chain issues, overburdening of healthcare systems, limiting access to testing, treatment and prevention programmes and further increasing inequalities.10 Modelled COVID-19 disruptions of HIV programmes in SSA included decreased functionality of HIV prevention programmes, HIV testing and treatment, healthcare services such as viral load testing, adherence counselling, drug regimen switches and ART interruptions, which may lead to selection of drug-resistant HIV.11 A 6-month interruption affecting 50% of the population would lead to a median number of excess deaths of 296 000, during 1 year. Scientists advocate for the AIDS and COVID-19 pandemics in Africa to be addressed simultaneously, by increasing African access to COVID-19 vaccines, prioritising research on the interaction between HIV care and COVID-19, maintaining high-quality HIV services and integrating health services for both viruses.7 Both the COVID-19 and the AIDS pandemic, more specifically the issue of HIV drug resistance (HIVDR), have previously been described as wicked problems which are best studied as complex adaptive systems (CASs).12–15Wicked problems consist of diverse interconnected factors and require complexity-informed and locally adapted solutions rather than one solution that fits all. We recently designed a qualitative model of all known factors influencing HIVDR in SSA and analysed its complexity.13 Our detailed systems map featured three main feedback loops driving HIVDR, representing (1) the alternation between adherence and non-adherence, (2) the impact of an overburdened healthcare system and (3) the importance of sustaining global efforts of tackling HIVDR even when new antiretroviral drugs with high genetic barriers become available. These HIV-related feedback loops are interconnected with COVID-19 pandemic impact (in yellow, figure 1). The loop starts from PLHIV with an unsuppressed viral load, which weakens the immune system and may in turn slow down immune clearance of SARS-CoV-2, allowing prolonged replication and mutation of the virus in the context of an inadequate immune response. Prolonged viral clearance facilitates the selection of immune escape SARS-CoV-2 variants. Variants may emerge that have a selective advantage and therefore may spread through populations due to increased transmissibility (with possibly increased virulence), thereby creating an additional burden on the healthcare system, putting the overall healthcare system and the HIV care at risk. These stressors on the healthcare system lead to a higher risk of unsuppressed viral load in PLHIV, increasing the risk of HIVDR. Figure 1 shows the need to address both wicked problems simultaneously and to do so in a complexity-informed manner as they are inevitably linked and influence each other. Evidently, the exact interconnections between both pandemics need to be locally assessed. For instance, a study in South Africa showed that while lockdown severely impacted HIV testing and ART initiation, ART provision was largely maintained, indicating that the strength of the connection between the virological suppression-related loop and the pandemic, indicated in figure 1, are context-dependent.16

Interlinkage of the HIV and COVID-19 CAS at the international level, as supported by literature (see main text). The blue, pink and purple loops are feedback loops identified in the HIVDR CAS.13 The yellow elements are related to the COVID-19 pandemic and illustrate the interlinkage between both complex problems. Other links between the COVID-19 on the HIVDR CAS are to be expected, such as the likely increase in transmission of HIVDR due to increased sexual violence during lockdown.21 The 60% increase in teenage pregnancies in South Africa during the pandemic points in the same direction.22 ART, antiretroviral therapy; CAS, complex adaptive system; HIVDR, HIV drug resistance.
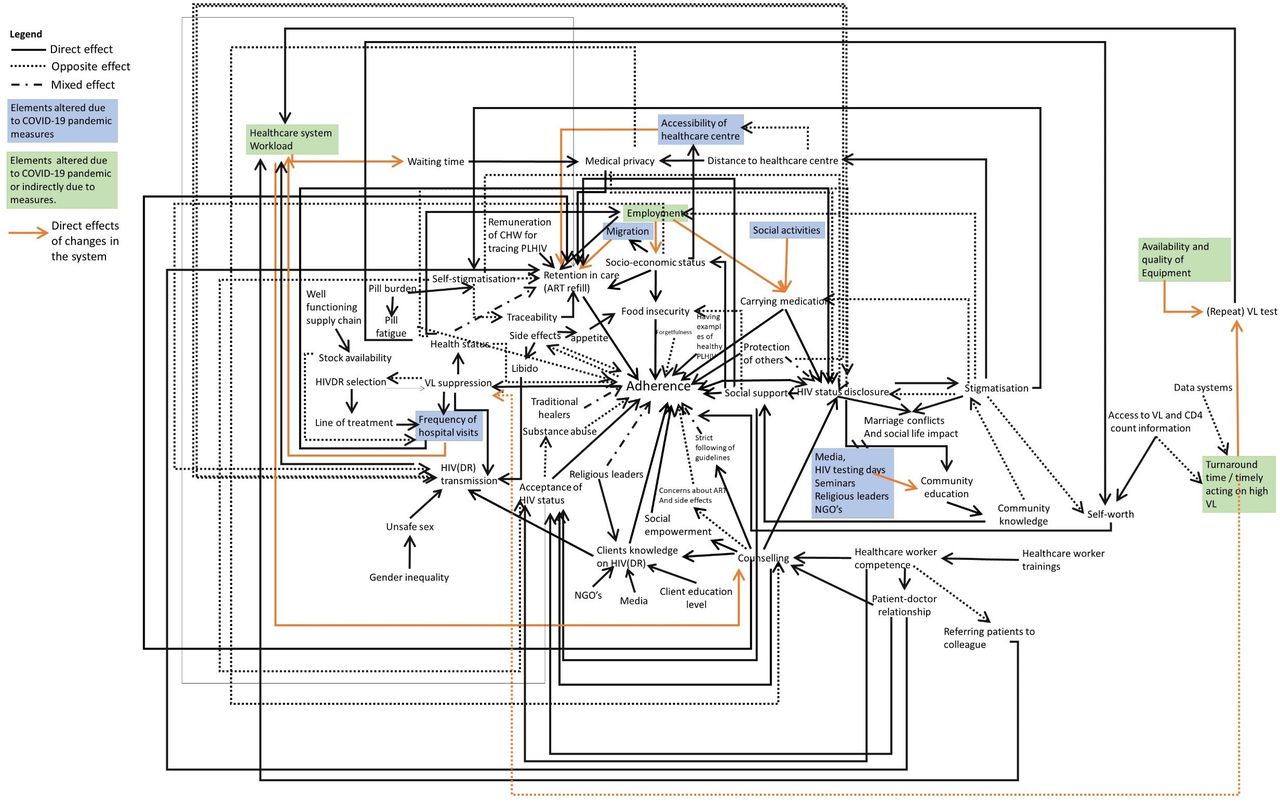
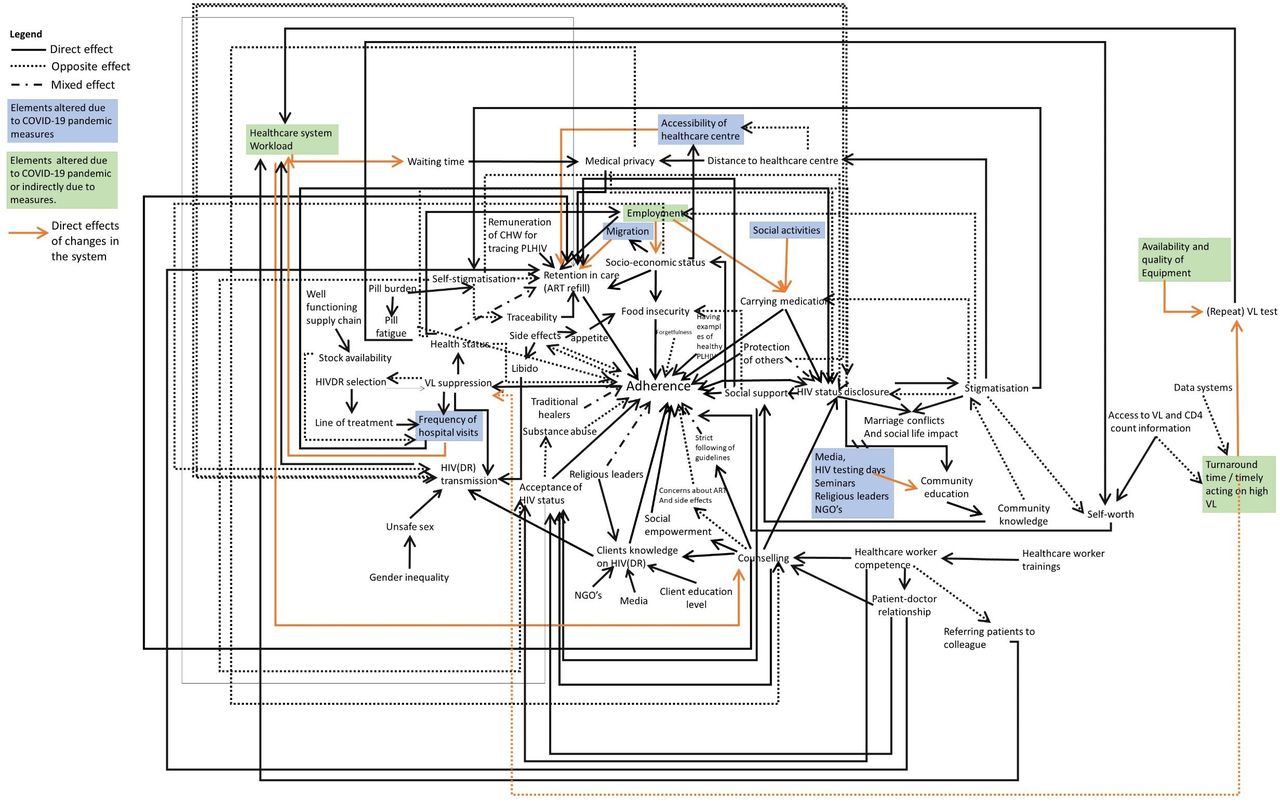
At a local level we can visualise the impact of the COVID-19 pandemic and measures impacting HIV care and the lives of PLHIV. We did so based on a systems map of factors influencing HIVDR in the Ukonga and Gongolamboto areas of Dar es Salaam region, Tanzania.14 In the period between March and June 2020 several COVID-19 related restrictions were implemented in Tanzania. These included banning social gatherings, avoiding non-essential travel, obligatory face masks at health facilities, and the provision of 6-month ART for all PLHIV, instead of the usual programmatic recommendation of 1-month and 3-month supplies for patients without and with recent viral suppression, respectively.17 18 In figure 2, we indicate the effects of both the measures and the pandemic in itself on the CAS of HIVDR which could be used to make complexity-informed decisions when rapid public health action is required. Systems maps help to make a first estimation of the impact of the COVID-19 pandemic and response measures on the HIVDR system. For example, due to restrictions in social activities, the feedback loop surrounding difficulties of carrying medication everywhere would have become obsolete for a certain period of time. On another note, many Tanzanians left the cities to go to the countryside at the start of the pandemic, due to the believe that SARS-CoV-2 circulated only in the cities. This migration, in combination with healthcare centres being overburdened by patients suffering from COVID-19, and with the implementation of other pandemic mitigation measures, would have made retention in care and continuous adherence to prescribed ART a challenge for PLHIV.
{kind=link}
{kind=link}
Effects of the COVID-19 pandemic and related measures on the HIVDR CAS in the study site. Between March and June 2020, social gatherings were restricted, the number of pill pick-ups was reduced, public transportation seats were limited to allow physical distancing, and patients were obliged to wear face masks at the healthcare centre, impairing access for people who were not able to afford masks. Moreover, some people were afraid of going to healthcare centres and instead bought their ART at pharmacies or chose to interrupt their treatment. Places in the system affected by government measures are indicated in blue. While the healthcare system’s HIV-related workload temporarily decreased, there was an increase in COVID-19-related workload, and due to worldwide stock-outs of reagents, laboratory capacity was reduced and delays in turnaround time of VL tests were noted. The pandemic also decreased employment opportunities. These indirect effects of the pandemic and/or pandemic measures are indicated in green. Effects on other elements are indicated with an orange arrow. ART, antiretroviral therapy; CAS, complex adaptive system; HIVDR, HIV drug resistance; NGO, Non-Governmental Organization; VL, viral load.
Our visualisations confirm the urgency to integrate care for PLHIV and the current and future pandemic response measures, in order to mitigate a prolongation of the current COVID-19 pandemic and a rise in drug-resistant HIV. Additionally, they also provide a tool for the assessment of evidence-based interventions, which could help to mitigate the pandemic’s impact, such as multimonth prescribing practices or differentiated service delivery.19 20
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Footnotes
Handling editor Seye Abimbola
Twitter @rsangeda
Contributors Conceptualisation, AK, A-MV, IHM, GMB, AM, CD, NV, OS, RZS, MRJ, TRdW and JK; writing—original draft preparation: AK; writing—review and editing, AK, IHM, GMB, AM, NV, CD, OS, RZS, JK, MRJ, TRdW and A-MV; visualisation, AK; Supervision, A-MV, NV, JK and RZS; Funding Acquisition, A-MV, AK, RZS and JK.
Funding This work was funded by VLIR-UOS, grant numbers TZ2019SIN263 and TZ2020JOI032A101.
Competing interests A-MV declares consultancy fees from Gilead.
Provenance and peer review Not commissioned; externally peer reviewed.