Article Text

Abstract
Background Low birth weight (LBW), including preterm birth (PTB) and small for gestational age (SGA), contributes a significant global health burden. We aimed to summarise current evidence on the effect of preconception and periconception interventions on LBW, SGA and PTB.
Methods In this systematic review and meta-analysis, we searched PubMed, Embase, Cochrane Library and WHO Global Index Medicus for randomised controlled trials and quasi-experimental studies published by 28 November 2020, which assessed interventions delivered in preconception and periconception or preconception and pregnancy. Primary outcomes were LBW, SGA and PTB. Studies were categorised by intervention type and delivery during preconception and periconception or during preconception and pregnancy. Estimates were pooled using fixed-effects or random-effects restricted maximum likelihood method meta-analyses. Quality of evidence for primary outcomes was assessed using the Grades of Recommendations, Assessment, Development and Evaluation approach.
Results We included 58 studies. Twenty-eight studies examined nutrition interventions (primarily micronutrient or food supplementation). Thirty studies (including one reporting a nutrition intervention) provided health interventions (general preconception health, early adverse pregnancy outcome prevention, non-communicable disease and infectious disease prevention and management). One study assessed a social intervention (reproductive planning). Studies varied in terms of specific interventions, including delivery across preconception or pregnancy, resulting in few studies for any single comparison. Overall, the evidence was generally very uncertain regarding the impact of any intervention on LBW, SGA and PTB. Additionally, preconception and periconception nutritional supplementation containing folic acid was associated with reduced risk of birth defects (10 studies, N=3 13 312, risk ratio: 0.37 (95% CI: 0.24 to 0.55), I2: 74.33%).
Conclusion We found a paucity of evidence regarding the impact of preconception and periconception interventions on LBW, SGA and PTB. Further research on a wider range of interventions is required to clearly ascertain their potential effectiveness.
Trial registration number This review was prospectively registered with PROSPERO (CRD42020220915).
- Maternal health
- Child health
- Public Health
- Systematic review
Data availability statement
Data are available on reasonable request. Data and other materials are available from the authors on reasonable request (contact corresponding author at: upartap@hsph.harvard.edu).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous reviews on the effect of maternal preconception status on low birth weight (LBW), small for gestational age (SGA) and preterm birth (PTB) and other adverse birth and pregnancy outcomes have identified potential preconception risk factors from observational evidence; assessed selected preconception interventions; and mainly studied outcomes such as micronutrient or disease status in the preconception period.
To our knowledge, no review has comprehensively and systematically examined the evidence directly linking interventions in the preconception period to the risk of adverse pregnancy outcomes such as LBW, SGA and PTB.
WHAT THIS STUDY ADDS
In this systematic review and meta-analysis, we identified 58 eligible studies on the impact of preconception and periconception interventions on LBW, PTB, SGA and other birth and maternal outcomes—however, there were few studies for any single comparison, for example, food supplementation in preconception and pregnancy versus pregnancy only to prevent PTB.
Studies reported mainly on health and nutrition interventions, with little research on other relevant areas such as environmental health, and the available evidence was generally very uncertain regarding the impact of these interventions on LBW, PTB and SGA.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
This work highlights that there is currently not enough high-quality evidence to clearly understand the effect of a range of possible preconception and periconception interventions on LBW, PTB and SGA; further, well-designed research is required in this area.
Introduction
Low birth weight (LBW), including preterm and small for gestational age babies (preterm birth, PTB and SGA), presents a significant global health burden. Approximately 20.5 million (14.6%) live births globally were estimated to be LBW in 2015, with 91% of these occurring in low-income and middle-income countries (LMICs).1 It is estimated that 14.84 million (10.6%) live births in 2014 were preterm, while approximately 23.3 million (19.3%) neonates were born SGA in LMICs in 2012.2 3 LBW is associated with increased risk of mortality especially in the neonatal period and infancy,4 5 and increased morbidity across the lifespan, including developmental and behavioural problems,6 7 undernutrition in childhood8 and cardiometabolic disease development in adulthood.9 Much research and programmatic attention has focused on interventions during pregnancy to prevent LBW.10 However, there is growing recognition of the need to identify additional windows for interventions prior to pregnancy for its prevention.11 12
Preconception is broadly understood as the period up to a few months before conception among women of reproductive age, although definitions encompassing a wider interval have also been proposed.12 13 Recent research indicates that maternal morbidity and nutritional status in the preconception period have important influences on pregnancy outcomes and the health of offspring,11 14 15 highlighting its value as a potentially critical window for preventative interventions. Although specific pathways have not been fully delineated, health and nutritional status up to conception are thought to inform physiological and epigenetic mechanisms during embryonic and fetal development, thereby influencing pregnancy and later life outcomes.13 16
While much research has been primarily from observational studies, evidence regarding potential preconception interventions to prevent adverse pregnancy outcomes has been growing.11 17–19 This includes studies assessing interventions in the periconception period (until pregnancy is detected), and those examining interventions delivered from preconception throughout pregnancy. However, there is currently no comprehensive picture of the impact of such interventions. Previously published reviews on the preconception period have included observational studies of potential contributing risk factors,11 14 15 17 20 examined endpoints other than pregnancy outcomes,21 and restricted searches to specific interventions.12 13 22 A better understanding of current data on the effect of interventions in the preconception period on pregnancy outcomes is key to identifying knowledge gaps and informing relevant and appropriate prevention strategies.
Objectives
We undertook a systematic review and meta-analysis aiming to summarise the current evidence regarding the impact of interventions delivered in the preconception and periconception period on the risks of LBW, SGA and PTB.
Methods
Eligibility criteria
Eligibility criteria for this systematic review are outlined below:
Population: Target participants were women in the preconception period, defined as any period in the life cycle prior to conception. This was guided by our conceptual framework (figure 1).
Intervention: Interventions had to be delivered prior to conception, or prior to the detection of pregnancy (periconception).
Comparator: Interventions were compared against no intervention, standard of care or routine care or placebo.
Outcome: The primary outcomes were LBW, PTB and SGA. Where possible, we also aimed to examine these outcomes reported in combination, as outlined by Lee et al.3 Secondary outcomes included other birth outcomes (birth weight, gestational age and birth weight for gestational age, stillbirth, birth defects, perinatal mortality, and large for gestational age) and maternal outcomes during pregnancy: (malnutrition (underweight, overweight and obesity), anaemia, haemoglobin concentrations, pre-eclampsia, gestational hypertension and gestational diabetes mellitus).
Study design: We included randomised controlled trials (RCTs), cluster RCTs and quasi-experimental designs in this review. Quasi-experimental designs were included only if concurrent comparator groups were used.

Conceptual framework outlining domains (morbidity, nutrition, social, WASH and related—at both individual and household level) for potential interventions to improve preconception health. While underlying, contextual risk factors are outlined in this framework, interventions are expected to have more direct effects on potential risk factors relevant to preconception health at the individual or household level. WASH: water, sanitation and hygiene; RTI: reproductive tract infection; STI: sexually transmitted infection.
Information sources and search strategy
We performed searches in PubMed, Cochrane Library (Cochrane Database of Systematic Reviews and Cochrane Central Register of Controlled Trials), the WHO Global Index Medicus and EMBASE. Searches were performed on 28 November 2020. A comprehensive search strategy was developed and agreed on by the authors, with key terms including variants of “preconception” and “periconception” and words related to outcomes of interest, but no terms relating to specific interventions to ensure the broadest search possible (see online supplemental appendix 1). This was informed by our conceptual framework (figure 1), which indicated a broad range of possible domains for interventions in the preconception and periconception period. Reference lists of records included in the full text assessment stage were examined for additional relevant studies. Searches were performed without restrictions on language or publication date.
Supplemental material
Selection process, data collection process and data items
We used Covidence review management software (Veritas Innovation, Melbourne, Australia) to manage study selection. Two authors (RC and UP) independently assessed potential studies for inclusion through title and abstract screening, followed by full-text review. Studies with unclear eligibility during title and abstract screening were included for full-text review; where possible, further doubts regarding eligibility were clarified through corresponding with study authors during full-text review. Reports based on the same study were linked. Disagreements regarding eligibility of studies were resolved through discussion. Two authors (RC and UP) independently extracted data using a prespecified form. Broadly, data extracted included study population and setting, sample size (including initial number of participants recruited and analytical size), study design, participant characteristics, interventions and comparators and preconception phase in which these were delivered, outcomes and analytical strategy. We extracted both crude and adjusted effect estimates where possible. Relevant group level data were extracted for all reported study arms to facilitate comprehensive comparisons. For all outcomes, we noted and used definitions as described by the authors. Data were checked for accuracy, and we contacted study authors for further information if any relevant information was missing or unclear. Disagreements during data extraction were resolved by discussion or consultation with a third author.
Study risk of bias assessment
Risk of bias was assessed for studies examining primary outcomes of interest, and their corresponding continuous measures. Two authors (RC and UP) independently assessed risk of bias using the revised Cochrane Risk Of Bias tool (ROB 2 tool) for randomised trials,23 the Risk Of Bias In Non-randomised Studies - of Interventions (ROBINS-I) tool for non-randomised trials,24 and the ROB 2 for Cluster Randomized Trials (ROB 2 CRT) tool for clustered studies.25 Risk of bias was visualised using robvis.26
Effect measures
For binary outcomes, we used risk ratios (RR) or odds ratios (OR) where risk could not be calculated. For continuous outcomes, we used mean differences (see online supplemental appendix 1 for details on use of study estimates). Results adjusted for potential confounders were used in preference to unadjusted results; when these were not available, unadjusted results were used. For clustered studies, cluster-adjusted effect estimates as reported by the study or calculated independently (see online supplemental appendix 1) were used. Risk estimates were not included in meta-analyses if the outcome was a composite measure, or if no outcome cases were observed in both intervention and comparator groups. We used estimates based on intention-to-treat analyses where possible.
Synthesis methods
For each outcome, included studies were categorised by intervention into three domains based on a predefined framework (see online supplemental appendix 1), and then into further subdomains. The domains were nutrition (subdomains: multiple micronutrient, iron and folic acid, folic acid or food supplementation and other); health (subdomains: general preconception health interventions, interventions to prevent early adverse pregnancy outcomes among women with a history of miscarriage, interventions to prevent or manage non-communicable diseases and interventions to prevent or manage infectious diseases); and social (subdomain: reproductive planning). Within subdomains, studies were additionally categorised by any other relevant study-specific characteristics (eg, high-dose vs low-dose supplementation, or potentially adverse effect hypothesised).
For our main analyses, we further divided studies according to two comparisons: (1) preconception and periconception intervention versus preconception and periconception no intervention, standard of care or routine care, or placebo, (2) or intervention in preconception and pregnancy versus same intervention in pregnancy only. Studies describing interventions delivered in preconception and pregnancy versus any other comparator in preconception and pregnancy were not included in main analyses, as these did not allow for examination of the effect of interventions in the preconception period alone. Where there were two or more studies for a specific comparison (eg, preconception and periconception folic acid supplementation to prevent LBW), data were pooled in a meta-analysis. Data were analysed using Stata V.16 (StataCorp). For health interventions, meta-analyses were only undertaken where study interventions were deemed to be sufficiently similar (eg, clinical interventions or lifestyle interventions); otherwise, studies were summarised individually.
Statistical heterogeneity among studies was examined through visual inspection of forest plots, assessment of the χ2 test for homogeneity, and the I2 value; notable heterogeneity was assessed as I2 ≥50%.27 Where no notable heterogeneity was observed, we pooled results using fixed-effects models using the inverse variance method. In situations of notable heterogeneity, we used random-effects restricted maximum likelihood models, and conducted subgroup analyses where meta-analyses included four or more studies.
Clinical heterogeneity was systematically explored in relation to three key variables, in prespecified subgroup analyses. In these analyses, we aimed to group and examine studies by (1) the number of months preconception in which interventions were delivered (<3 and 3+ months prior to conception), (2) the age of participants (<30 and 30+, or <24, 25–29 and 30+, years) and (3) study setting (LMIC vs high-income country as defined by the World Bank). Additionally, in sensitivity analyses, we restricted meta-analyses to only studies assessed as low risk of bias by the ROB-2,23 ROBINS-I24 or ROB 2 CRT tool.25 These indicated the potential impact of risk of bias as a source of methodological heterogeneity on effect estimates. Although in the protocol we planned to undertake these assessments for all meta-analyses, as the number of studies for any single meta-analysis was generally low and studies assessing health and social interventions were highly variable with regards to setting and intervention type, we examined subgroup effects and conducted sensitivity analyses only for studies examining nutritional interventions and primary outcomes where four or more studies were included in meta-analyses.
Reporting bias assessment
Funnel plots and Egger’s test were used to assess the presence of publication bias in cases where four or more studies were included in meta-analyses, or in cases where meta-analyses included less than four studies but interventions were being assessed for primary outcomes. This was different to our original aim of conducting such assessments for all analyses as noted in the protocol, and was done due to the small number of studies for any single meta-analysis. These methods of assessment are recognised to have low power when based on a small number (<10) of studies, as in our case28; and we took this into consideration when interpreting the results. Additionally, although in the protocol we planned to stratify analyses by study size to assess the impact of publication bias on the pooled estimate, we did not do this as in most cases there were too few studies to obtain meaningful conclusions.
Certainty of evidence
Quality assessment of the pooled estimates for the primary outcomes was conducted through the Grades of Recommendations, Assessment, Development and Evaluation (GRADE) approach, consisting of a systematic assessment of risk of bias, consistency of effect, imprecision, indirectness and publication bias, as outlined in the Cochrane Handbook.28 Quality assessments were undertaken using the GRADEPro GDT tool.29
Patient and public involvement
As this study was a systematic review with a broad remit, and given that no de novo data and sample and collection was involved, patients and the public were not involved in this research.
Results
Study selection and characteristics
Summary of screened and included studies
We retrieved a total of 6268 records; following removal of duplicates, 5107 records were screened. Of these, full texts of 182 records were assessed, and 66 records based on 58 studies were included for this analysis (figure 2). Unique studies included 37 RCTs, 3 cluster RCTs and 18 quasi-experimental studies (table 1).18 19 30–93

Study screening process.
Summary of included studies
Overall, studies varied widely in terms of interventions and comparators, and their delivery across the preconception and pregnancy phases. Generally, few and often diverse interventions were identified for any single comparison, especially for studies examining health interventions (table 1, online supplemental appendix 1).
Interventions
Twenty-eight studies examined nutritional interventions. Of these, 10 studies examined multiple micronutrient supplementation.18 35 41 45 50 53 56 63 64 66 76 85 87 89 Five studies, including one study which also had a multiple micronutrient supplementation arm, examined iron and folic acid supplementation.18 39 46 47 56 58 65 Six studies assessed folic acid supplementation,32 42 48 52 83 84 86 and four studies assessed food supplementation.19 30 38 43 57 Four studies reported on other nutrition interventions (calcium supplementation, iodine supplementation, vitamin A or beta carotene supplementation or inclusion of mushrooms in diet) (table 1).31 61 80 82
Thirty studies, including one also contributing information on a nutrition intervention,70 76 89 assessed health interventions. Of these, five studies assessed general preconception health interventions.34 37 44 51 55 Eight studies examined interventions to prevent early adverse pregnancy outcomes among women with a history of miscarriage.36 49 60 67 69 73 75 88 Five studies assessed interventions to prevent or manage non-communicable diseases,40 78 81 92 93 and 12 studies reported on interventions to prevent or manage infectious diseases (table 1).33 59 62 68 70–72 74 77 79 90 91
One study examined a social intervention (reproductive planning) (table 1).54
Outcomes
Forty studies reported on at least one primary outcome.18 19 30 31 34 36–41 43 46 47 49 51 53–64 66–80 87–89 93 Eighteen studies assessed one or more secondary outcomes of interest.32 33 35 42 44 45 48 50 52 65 81–86 90–92 We found no studies examining combinations of LBW, PTB and SGA (eg, SGA and preterm), and only one study that differentiated between spontaneous and iatrogenic PTB.59 We found one or more studies on all secondary outcomes, except for maternal malnutrition measures (underweight, overweight, obesity) and perinatal mortality (no studies).
Results of syntheses
A summary of estimates is provided in table 2, and outlined in greater detail below.
Summary of evidence regarding the effect of preconception and periconception interventions to prevent LBW, SGA and PTB

Summary of evidence regarding the effect of interventions delivered in the preconception and periconception period or preconception and pregnancy (vs pregnancy) period on low birth weight. The upper plot summarises the effect of interventions delivered in the preconception and periconception period compared with folic acid supplementation, other micronutrients (not folic acid), standard or routine care, placebo or no intervention (apart from food supplementation, see i below). The lower plot summarises the effect of interventions delivered in the preconception and pregnancy period compared with the same intervention delivered during pregnancy only. NCD interventions: NCD prevention and management. Infectious disease interventions: infectious disease prevention and management. Numbers in brackets denote the study reference. RR (95% CI): RR (95% CI). Grade: certainty of evidence assessment using the grading of recommendations assessment, development and evaluation tool. Preconception and periconception multiple micronutrient supplementation: one study was based among women with a previous birth with neural tube defect. Preconception and periconception calcium supplementation: the identified study was based among women with previous pre-eclampsia. Preconception and periconception early adverse pregnancy outcome prevention: the identified study was based among women with previous miscarriage. Preconception and pregnancy NCD interventions: the identified study was based among women with type one diabetes. Preconception and pregnancy infectious disease interventions: the identified study was based among women with HIV. iThe identified study compared the effect of a longer duration of food supplementation with a shorter duration; the OR is reported for this study as risk ratio could not be computed. iiThe aim of interventions was not to prevent low birth weight, and the anticipated effect of interventions was not necessarily protective. GRADE, Grades of Recommendations, Assessment, Development and Evaluation; NCD, non-communicable disease; RR, risk ratio.

Summary of evidence regarding the effect of interventions delivered in the preconception and periconception period or preconception and pregnancy (vs pregnancy) period on small for gestational age. The upper plot summarises the effect of interventions delivered in the preconception and periconception period compared with folic acid supplementation, standard or routine care or placebo. The lower plot summarises the effect of interventions delivered in the preconception and pregnancy period compared with the same intervention delivered during pregnancy only. Infectious disease interventions: infectious disease prevention and management. Numbers in brackets denote the study reference. RR (95% CI): RR (95% CI). Grade: certainty of evidence assessment using the grading of recommendations assessment, development and evaluation tool. Preconception and periconception early adverse pregnancy outcome prevention: both studies were based among women with previous miscarriage; in one study, participants also had antiphospholipid syndrome. iThe aim of interventions was not to prevent low birth weight, and the anticipated effect of interventions was not necessarily protective. GRADE, Grades of Recommendations, Assessment, Development and Evaluation; RR, risk ratio.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
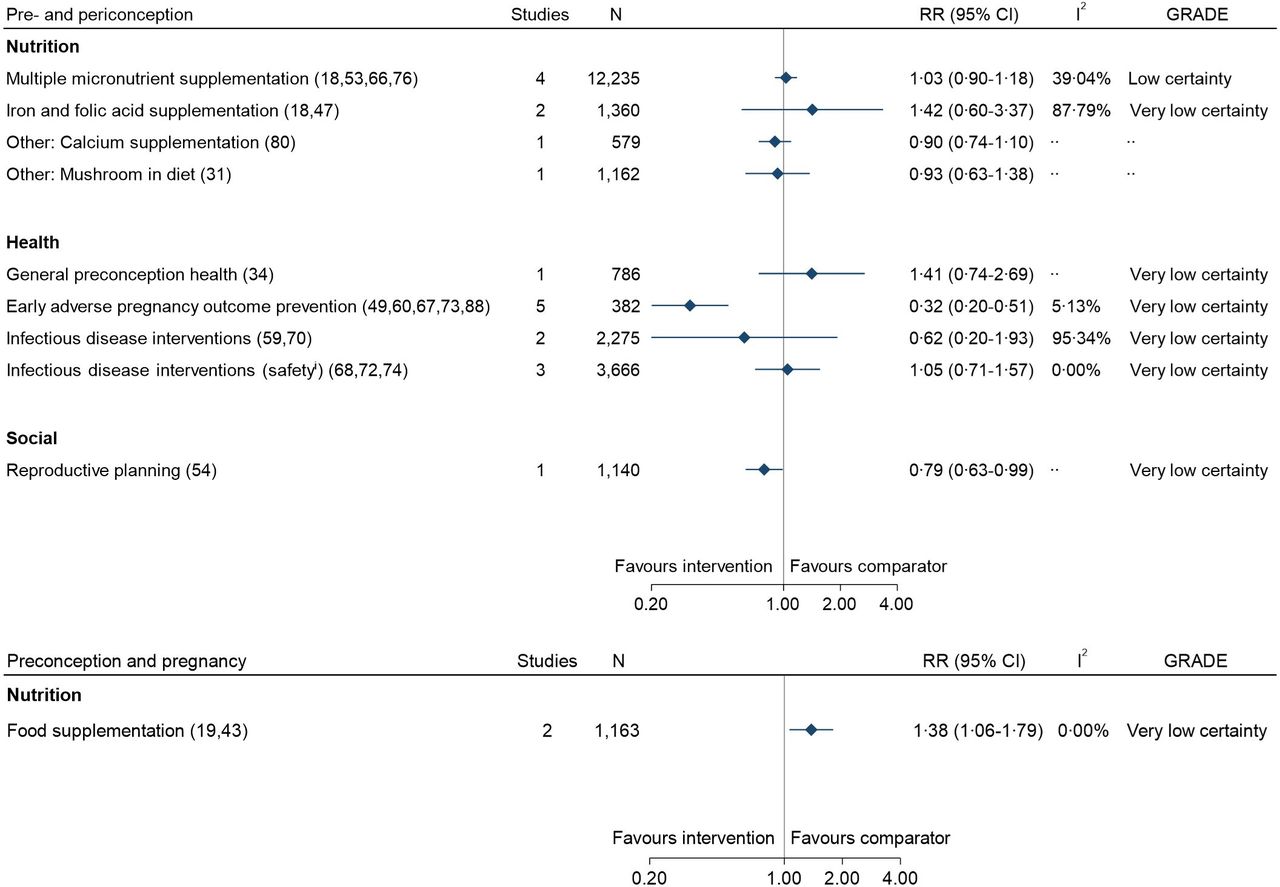
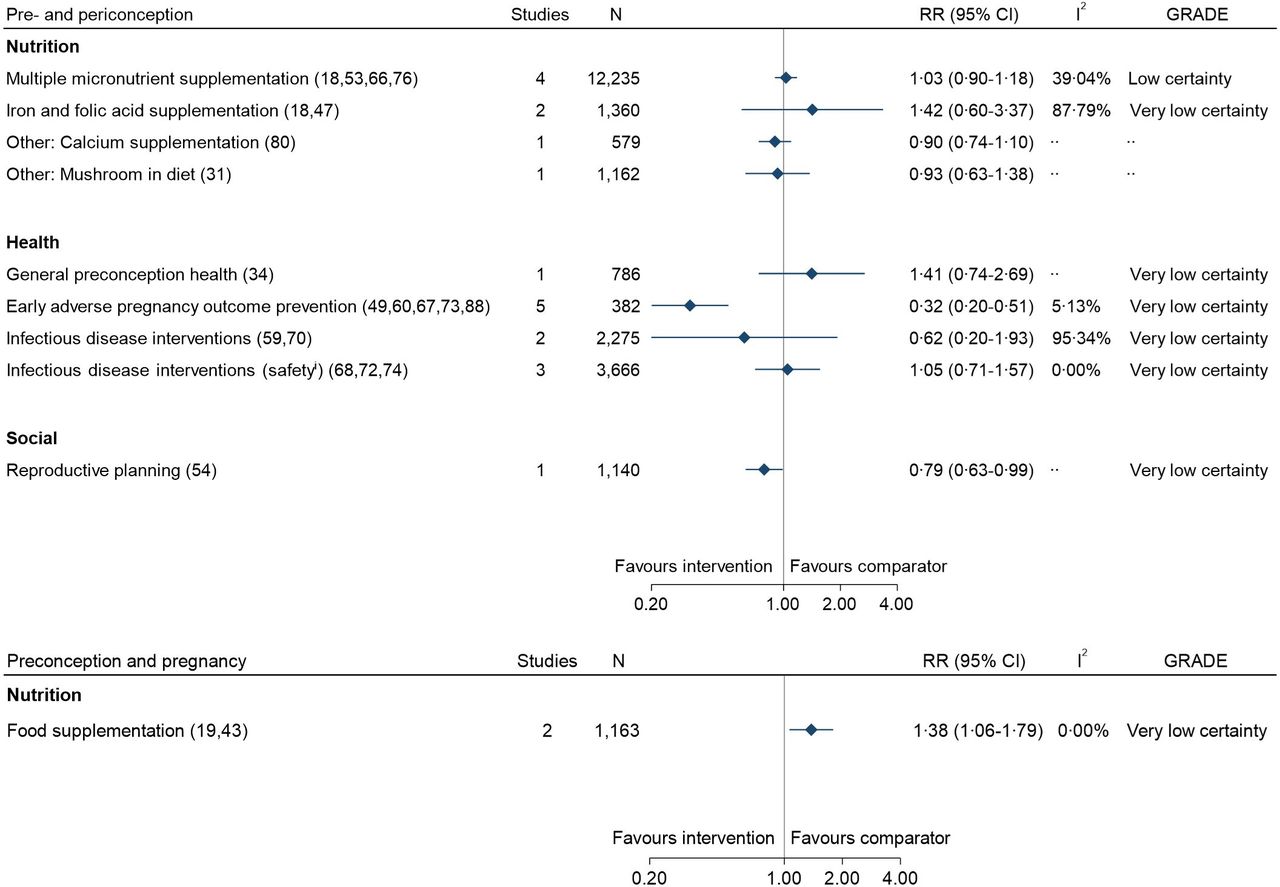
Summary of evidence regarding the effect of interventions delivered in the preconception and periconception period or preconception and pregnancy (vs pregnancy) period on preterm birth. The upper plot summarises the effect of interventions delivered in the preconception and periconception period compared with folic acid supplementation, other micronutrients (not folic acid), standard or routine care, placebo or no intervention. The lower plot summarises the effect of interventions delivered in the preconception and pregnancy period compared with the same intervention delivered during pregnancy only. Infectious disease interventions: infectious disease prevention and management. numbers in brackets denote the study reference. RR (95% CI). Grade: certainty of evidence assessment using the grading of recommendations assessment, development and evaluation tool. Preconception and periconception calcium supplementation: the identified study was based among women with previous pre-eclampsia. Preconception and periconception early adverse pregnancy outcome prevention: the identified study was based among women with previous miscarriage; in one study, participants also had antiphospholipid syndrome. iThe aim of interventions was not to prevent low birth weight, and the anticipated effect of interventions was not necessarily protective. GRADE, Grades of Recommendations, Assessment, Development and Evaluation; RR, risk ratio.
Effect of interventions on LBW
Identified studies
We identified 18 studies reporting effects of 19 interventions on LBW where the preconception or periconception effect of interventions could be ascertained (table 2, figure 3, online supplemental appendix 1).18 19 31 34 38 39 43 47 49 53 55 58 62 64 76 78–80 This included 14 interventions (10 nutrition18 31 38 47 53 58 64 76 80 and 4 health34 49 55 62) delivered in preconception and periconception, and 5 (3 nutrition19 39 43 and 2 health78 79) delivered in preconception and pregnancy (vs pregnancy-only intervention).
Interventions in preconception and periconception
We found two or more studies for two nutrition interventions delivered in preconception and periconception. These were preconception and periconception multiple micronutrient supplementation and preconception and periconception iron and folic acid supplementation. The evidence suggested that preconception and periconception multiple micronutrient supplementation results in little to no difference in LBW (four studies, N=12 054, RR: 1.06 (95% CI: 0.90 to 1.25), I2: 0.00%, GRADE: low certainty).18 53 64 76 Overall, the evidence was very uncertain about the effect of preconception and periconception iron and folic acid supplementation on LBW (three studies, N=1831, RR: 0.74 (95% CI: 0.34 to 1.61), I2: 83.10%, GRADE: very low certainty).18 47 58 Similarly, the evidence was very uncertain regarding the effect of preconception and periconception food supplementation on LBW (one study, N=529, OR: 0.40 (95% CI: 0.14 to 1.12), GRADE: very low certainty) (table 2, figure 3, online supplemental appendix 1).38 We found only two single, non-comparable studies for other nutrition interventions, both of which reported no clear effect on LBW (table 2, figure 3, online supplemental appendix 1).31 80
Among health interventions, we found two studies for preconception and periconception general health interventions. The available evidence from these studies suggested that such interventions may increase LBW; however, the evidence was very uncertain (two studies, N=1188, RR: 1.27 (95% CI: 0.83 to 1.94), I2: 39.11%, GRADE: very low certainty).34 55 We found no studies examining effects on LBW of preconception and periconception interventions to prevent or manage non-communicable diseases, and only one small study (N<100 each) for each of the other health interventions (early adverse pregnancy outcome prevention among women with previous miscarriage: clomiphene citrate vs placebo,49 and infectious disease interventions: H1N1 vaccine vs placebo62). The overall evidence was very uncertain regarding the effect of either of these interventions in the preconception and periconception period on LBW (early adverse pregnancy outcome prevention: one study, N=82, RR: 0.23 (95% CI: 0.11 to 0.51), GRADE: very low certainty; infectious disease interventions: one study: N=39, RR: 4.96 (95% CI: 0.27 to 89.87), GRADE: very low certainty) (table 2, figure 3, online supplemental appendix 1).
Interventions in preconception and pregnancy versus intervention in pregnancy only
We found two or more studies for only one nutrition intervention delivered in preconception and pregnancy vs pregnancy only: food supplementation.19 43 Evidence from these studies suggested that preconception and pregnancy food supplementation may have little to no impact on LBW compared with pregnancy-only supplementation, but was very uncertain (two studies, N=1134, RR: 1.00 (95% CI: 0.79 to 1.26), I2: 0.00%, GRADE: very low certainty).19 43 We found one other small study (N=200) examining the effect of preconception and pregnancy iron supplementation (vs pregnancy-only supplementation) on LBW; overall, the evidence was very uncertain about its effect on LBW (one study, N=200, RR: 0.28 (95% CI: 0.08 to 1.03), GRADE: very low certainty).39 We found no studies examining any other nutrition interventions (table 2, figure 3, online supplemental appendix 1).
For health interventions, we found only one small (N<200) study each reporting effects of a preconception and pregnancy versus pregnancy-only non-communicable disease intervention (intensive therapy for type 1 diabetes)78 or infectious disease intervention (antiretroviral therapy)79 (table 2, figure 3, online supplemental appendix 1).79 Overall, the evidence was very uncertain about the effect of either of these interventions on LBW (non-communicable disease interventions: one study, N=149, RR: 4.34 (95% CI: 0.55 to 34.34), GRADE: very low certainty; infectious disease interventions: 1 study: N=186, RR: 2.65 (95% CI: 1.20 to 5.81), GRADE: very low certainty).
Effect of interventions on SGA
Identified studies
Eight studies reported the effect of nine interventions where the preconception or periconception impact of interventions on SGA could be examined.18 19 34 43 47 49 72 88 Of these, seven interventions (three nutrition18 47 and four health34 49 72 88) were delivered in preconception and periconception, while two (both nutrition19 43) were delivered in preconception and pregnancy versus pregnancy only (table 2, figure 4, online supplemental appendix 1).
Interventions in preconception and periconception
Among nutrition interventions, we found two studies assessing preconception and periconception iron and folic acid supplementation. The evidence suggested that preconception and periconception iron and folic acid supplementation reduces SGA (two studies, N=1351, RR: 0.83 (95% CI: 0.66 to 1.05), I2: 0.00%, GRADE: low certainty).18 47 Additionally, the evidence was very uncertain about the effect of preconception and periconception multiple micronutrient supplementation on SGA (one study, N=1084, RR: 1.02 (95% CI: 0.74 to 1.40), GRADE: very low certainty).20 We found no studies for any other nutrition intervention (table 2, figure 4, online supplemental appendix 1).
Among health interventions, we found two studies examining heterogeneous preconception and periconception interventions to prevent early adverse pregnancy outcomes (clomiphene citrate49 or aspirin and heparin vs placebo88) among women with previous miscarriage. The evidence suggested that such interventions result in a large reduction in SGA (two studies, N=208, RR: 0.35 (95% CI: 0.18 to 0.68), I2: 0.00%, GRADE: low certainty).49 88 No studies examined non-communicable disease interventions. One study each examined the impact on SGA of a general preconception health intervention (home visit following first delivery offering comprehensive preconception care vs standard or routine care)34 or an infectious disease intervention (HPV vaccine vs placebo)72 (table 2, figure 4, online supplemental appendix 1). The evidence was very uncertain regarding the effect of each of these interventions on SGA (general preconception health interventions: 1 study, N=760, RR: 1.13 (95% CI: 0.57 to 2.14) GRADE: very low certainty; infectious disease interventions: 1 study, N=2871, RR: 1.23 (95% CI: 0.33 to 4.57), GRADE: very low certainty).
Interventions in preconception and pregnancy versus intervention in pregnancy only
We found studies for only food supplementation interventions delivered in preconception and pregnancy versus pregnancy. The evidence from these studies suggested that preconception and pregnancy versus pregnancy-only food supplementation reduces SGA slightly (two studies, N=1161, RR: 0.89 (95% CI: 0.78 to 1.02), I2: 0.00%, GRADE: low certainty).19 43 No studies were found for any other nutrition or health intervention delivered in preconception and pregnancy versus pregnancy only (table 2, figure 4, online supplemental appendix 1).
Effect of interventions on PTB
Identified studies
Twenty-three studies (24 interventions)18 19 31 34 43 47 49 51 53 54 59 60 66–68 70–74 76 80 88 examining PTB were identified which estimated preconception or periconception effects of interventions. Most interventions were delivered during the preconception and periconception period (8 nutrition,18 31 47 53 66 76 80 13 health,34 49 51 59 60 67 68 70–74 88 1 social54). Only two interventions (both nutrition)19 43 were delivered in preconception and pregnancy and compared with pregnancy-only intervention (table 2, figure 5, online supplemental appendix 1).
Interventions in preconception and periconception
We found two or more comparable studies for two nutrition interventions delivered in preconception and periconception that reported on PTB. These were preconception and periconception multiple micronutrient supplementation and preconception and periconception iron and folic acid supplementation. The evidence suggested that preconception and periconception micronutrient supplementation results in little to no difference in PTB (four studies, N=12 235, RR: 1.03 (95% CI: 0.90 to 1.18), I2: 39.04%, GRADE: low certainty).18 53 66 76 Furthermore, the evidence was very uncertain about the impact of preconception and periconception iron and folic acid supplementation on PTB (two studies, N=1360, RR: 1.42 (95% CI: 0.60 to 3.37), I2: 87.79%, GRADE: very low certainty).18 47 We found no studies examining preconception and periconception food supplementation, and two studies indicating no clear effect of other preconception and periconception nutrition interventions (calcium supplementation,80 inclusion of mushrooms in diet31) on PTB (table 2, figure 5, online supplemental appendix 1).
We found two or more studies for two preconception and periconception health interventions. These were interventions to prevent early adverse pregnancy outcomes among women with previous miscarriage (five studies, N=382)49 60 67 73 88 and infectious disease interventions. We subdivided infectious disease interventions into those that specifically aimed to reduce PTB risk (two studies, N=2275, GRADE: very low certainty),59 70 and those with unclear or adverse hypothesised effect (three studies, N=3666, GRADE: very low certainty).68 72 74 The available evidence suggested that preconception and periconception interventions to prevent early adverse pregnancy outcomes among women with previous miscarriage may reduce PTB; however, the evidence was very uncertain (five studies, N=382, RR: 0.32 (95% CI: 0.20 to 0.51), I2: 5.13%, GRADE: very low certainty).49 60 67 73 88 Importantly, these interventions were widely varying, and included clomiphene citrate,49 aspirin and heparin,88 intravenous immunoglobulin60 or third party leucocyte transfusion vs placebo,67 and intrauterine hyaluronic acid gel vs no intervention following dilation and curettage.73 Furthermore, the evidence was very uncertain regarding the effect of preconception and periconception infectious disease interventions or general health interventions on PTB (general preconception health interventions: one study, N=786, RR: 1.41 (95% CI: 0.74 to 2.69), GRADE: very low certainty; infectious disease interventions to reduce PTB risk: two studies, N=2275, RR: 0.62 (95% CI: 0.20 to 1.93), I2: 95.34%, GRADE: very low certainty; infectious disease interventions with potential unclear or adverse effects: three studies, N=3666, RR: 1.05 (95% CI: 0.71 to 1.57), I2: 0.00%, GRADE: very low certainty).34 We found no studies examining preconception and periconception non-communicable disease interventions (table 2, figure 5, online supplemental appendix 1).
Two studies examining health interventions were not presented in figure 5: one examined a preconception counselling intervention on a composite outcome including PTB (online supplemental appendix 1),51 and one assessed effects of the dapivirine vaginal ring compared with a placebo ring, with no PTB cases in the intervention group and a resulting estimate that could not be pooled but which suggested no clear effect (one study, N=181, RR: 0.06 (95% CI: 0.00 to 0.96), GRADE: very low certainty) (table 2, online supplemental appendix 1).71
We found a single study on a preconception and periconception social intervention. This study examined the impact a reproductive planning intervention to increase interpregnancy interval on PTB risk. The available evidence suggested that such an intervention may reduce PTB, but the evidence was very uncertain (one study, N=1140, RR: 0.79 (95% CI: 0.63 to 0.99), GRADE: very low certainty) (table 2, figure 5, online supplemental appendix 1).54
Interventions in preconception and pregnancy versus intervention in pregnancy only
We identified studies for only food supplementation interventions delivered in preconception and pregnancy versus pregnancy. The evidence was very uncertain regarding the impact of preconception and pregnancy food supplementation compared with pregnancy-only supplementation on PTB (GRADE: very low certainty).19 43 No other preconception and pregnancy versus pregnancy-only interventions were identified.
Subgroup and sensitivity analyses and reporting biases
Subgroup and sensitivity analyses indicated no clear trends or differences in findings, although these were limited by the small number of studies for any main meta-analysis (online supplemental appendix 1). We found no clear evidence of publication bias for studies assessing primary outcomes. In most cases, these analyses were based on ≤4 studies overall or within subgroups, insufficient to draw firm conclusions.
Risk of bias in studies and certainty of evidence
Only a small proportion of studies assessing the primary outcomes or their continuous measures were assessed as low risk of bias (LBW or birth weight: 6/35 studies, SGA or birth weight for gestational age: 4/12 studies, PTB or gestational age: 6/37 studies) (see online supplemental appendix 1). GRADE assessment suggested low or very low quality evidence overall (table 2, figures 3–5 and online supplemental appendix 1).
Effect of interventions on other birth and maternal outcomes
We observed some effect of interventions on some birth and maternal outcomes as well, although certainty of evidence was not examined for these secondary outcomes. Among other birth outcomes, preconception and periconception nutritional supplementation containing folic acid was associated with 63% reduced risk of birth defects, which were mainly neural tube defects (NTDs) (10 studies, N=3 13 312, RR: 0.37 (95% CI: 0.24 to 0.55), I2: 74.33%) (online supplemental appendix 1).32 35 42 48 50 53 64 83–85 89
Limited evidence suggested 33%–39% reduced risk of maternal anaemia during pregnancy associated with preconception and pregnancy nutritional supplementation (iron and folic acid or food supplementation) compared with pregnancy-only supplementation (second trimester—two studies with N=307, RR: 0.61 (95% CI: 0.47 to 0.80), I2: 0.00%, third trimester—two studies with N=289, RR: 0.67 (95% CI: 0.47 to 0.96), I2: 0.00%).39 43 A 61% reduced risk of maternal pre-eclampsia was associated with preconception and periconception early adverse pregnancy outcome prevention interventions (two studies, clomiphene citrate49 or aspirin and heparin88 vs placebo, N=208, RR: 0.39 (95% CI: 0.20 to 0.74), I2: 0.00%) (online supplemental appendix 1).
Discussion
This systematic review identified 58 studies examining the effect of interventions delivered during the preconception and periconception period or from preconception throughout pregnancy on LBW, SGA, PTB, and other birth and maternal outcomes. These studies mainly examined nutrition or health interventions, with only one study on a potential social intervention. Studies varied widely in terms of the nature of interventions and comparators and their delivery across preconception and pregnancy. This led to many comparisons, but few studies for any single comparison. Most studies examining LBW, SGA and PTB and their continuous measures were assessed as moderate or high risk of bias. In terms of effect sizes, our findings indicated no clear impact of preconception and periconception nutrition interventions on any primary outcome, although preconception and periconception interventions aiming to reduce early adverse pregnancy outcomes were associated with reduced risk of SGA and PTB among women with previous miscarriage. However, evidence regarding any specific intervention was sparse, limiting any conclusive interpretations. The overall quality of evidence regarding interventions in preconception and periconception or from preconception throughout pregnancy to prevent LBW, SGA and PTB was low or very low certainty. Thus, the evidence summarised here is very uncertain about the effect of most of the interventions examined on LBW, SGA and PTB, at best suggesting that some interventions may reduce these LBW, SGA and PTB. To our knowledge, this is the first comprehensive systematic review and meta-analysis examining the effect of preconception and periconception interventions on LBW, SGA, PTB and other birth and maternal outcomes.
Recognition has grown in recent years of the preconception period as a window of opportunity to improve pregnancy outcomes.13 16 94 Recent reports have noted the potential value of improving health, nutrition and psychosocial status during the preconception period, highlighting its importance given the global burden of malnutrition and morbidity among women of reproductive age and increasing observational evidence indicating associations between preconception health status and pregnancy outcomes.13 16 95 96 Recent research has also assessed the impact of interventions delivered preconceptionally on preconception health outcomes, key to ensuring that women enter pregnancy in a healthy state.11 17 21 97 However, previous evidence syntheses in this area have been limited, due to their assessment of specific interventions and non-pregnancy endpoints, or inclusion of observational studies.11 12 14 15 17 21 22 Importantly, the available data directly linking preconception interventions to LBW, SGA, PTB and other outcomes have not yet been systematically examined and summarised. This systematic review bridges this gap, collating current evidence on preconception interventions across all possible domains and outlining their impact on these outcomes. Importantly, it highlights a dearth of relevant high-quality evidence in this area, and a need for much further research to accurately and reliably ascertain any impact.
Overall, the evidence is generally very uncertain about the effect of nutrition interventions delivered in the preconception and periconception period, including multiple micronutrient supplementation, iron and folic acid supplementation, folic acid supplementation and food supplementation, on LBW, SGA and PTB. Our observations may be explained by multiple reasons. First, evidence regarding any single comparison generally came from few studies, limiting the ability to examine the question and yield meaningful effects. Second, most studies provided nutritional supplementation for approximately 3–6 months before conception,19 43 57 64 66 76 which may not be sufficient to achieve sustained improvement in preconception nutritional status to the extent that an effect could be observed on pregnancy outcomes. Third, while adherence was not systematically reported or assessed, certain studies noted poor adherence to interventions, which may have contributed to drawing true effects towards the null.43 57 Finally, the specific interventions themselves may not be adequate.43 57 Studies were conducted mainly in LMICs, where the burden of undernutrition remains high among women of reproductive age.18 19 43 47 66 In this context, interventions such as single or multiple micronutrient supplementation or food supplementation alone may not be sufficient to improve pregnancy outcomes when delivered in the preconception period.
Notably, we found reduced risk of maternal anaemia during the second and third trimesters associated with preconception nutritional supplementation, supporting the notion that such interventions may confer some beneficial effects at least into pregnancy. These findings extend previous research establishing reduced risk of maternal anaemia with prenatal iron supplementation.98 99 Given evidence that antenatal care is often started late in LMIC settings,12 100 they suggest potential opportunities to further improve anaemia status by focusing on the periconception period. Additionally, we observed reduced risk of birth defects (primarily NTDs) associated with preconception and periconception nutritional supplementation containing folic acid, consistent with previous reviews in this area.101 Multiple genetic and environmental factors are thought to contribute to the pathway between folate supplementation during preconception and periconception and reduced risk of NTDs.101 102
The totality of evidence identified regarding preconception and periconception health interventions was heterogeneous and inconsistent, preventing conclusive interpretations. Evidence from this review suggests that preconception and periconception interventions to prevent early adverse pregnancy outcomes on the may result in a large reduction in SGA. Although the evidence was very uncertain regarding the effect of such intervention on PTB and certainty of evidence was not ascertained for pre-eclampsia, effect estimates indicated that such interventions were associated with reduced risk of PTB and pre-eclampsia. However, these findings may have limited utility in terms of potential for wider application given the wide variability in the specific interventions, although the individual interventions may merit further investigation. Though the available studies contribute important data regarding preventative and adverse effects of specific strategies to address key diseases when delivered in preconception and periconception, there is scope for much future work addressing a wider range of conditions.
We found little to no literature regarding other important areas in which interventions delivered preconceptionally may have a positive impact on LBW, SGA and PTB. Although symptoms of most common mental disorders are noted to begin in adolescence and young adulthood,103 and evidence has linked prepregnancy and pregnancy mental health to adverse pregnancy outcomes,104 105 we found no studies assessing preconception mental health interventions. Additionally, no studies examined strategies to address environmental conditions contributing to poor preconception health, such as those improving water, sanitation and hygiene, which may increase the risk of chronic infectious conditions,106–108 and those reducing indoor air pollution, which has been linked to LBW.109 More research is also needed regarding interventions addressing sociocultural issues, including approaches to reduce smoking and substance abuse,15 or to empower women of reproductive age in ways that may benefit maternal and child health, such as through preventing adolescent pregnancy or increasing inter-pregnancy interval.110 We identified only a single study reporting reduced risk of PTB following integration of family planning services into late antenatal and postpartum care.54 This community-based study from Bangladesh highlighted notable decreases in the proportion of women with a short (<24 month) interpregnancy interval in areas where the intervention was delivered, indicating the potential value of applying such approaches to similar settings and other aspects of reproductive planning.
It will be particularly important for future research to assess integrated, multicomponent interventions addressing different determinants of preconception health. This is essential given previous evidence that women of reproductive age may have a combination of risk factors or conditions which may interact, and that standalone interventions in pregnancy have not shown large effects on LBW and related outcomes.13 94 More generally, evidence from countries such as Bangladesh, where rates of adverse maternal and neonatal outcomes have decreased in recent decades, suggests an important role of multisectoral advances, covering aspects from women’s education, empowerment and equity to infrastructure, water supply and sanitation.111 112 Additionally, further investigation is required of age and intervention timing and duration, or other underlying characteristics such as preconception nutritional status or geographic region, as factors affecting overall impact.57 More broadly, research may need to consider how the preconception period is defined, with a view to informing appropriate intervention and study design.22 For example, lifestyle and nutrition interventions requiring sustained delivery may be more effective when starting in adolescence, rather than a prespecified number of months before women intend to become pregnant. In this regard, approaches that integrate preconception and adolescent health research may be an efficient way to maximise insight. This may be particularly valuable given increasing recognition of the need for further research into adolescent health.113 Importantly, such approaches acknowledge the overlap in both periods, and recognise that potential benefits are twofold—to individuals regardless of whether they conceive, and to offspring once conception occurs.22 103 However, such approaches must also take into account a potential need for continuity of interventions after adolescence to have some impact on birth outcomes, especially given global increases in age at first pregnancy to well beyond this period.114
There are limitations to this systematic review. Some of these relate to the evidence base. Our primary outcomes were often reported as secondary outcomes or as part of post hoc analyses in most studies examining health interventions and some studies examining nutrition interventions. Therefore, studies may not have been powered to identify clinically significant effects, and ascertainment and follow-up for outcomes may not have been rigorous. As may be expected, most studies had notable lost to follow-up (over 20%) due to participants not conceiving, or other reasons which were not always reported, suggesting potential for selection bias. Studies also had distinct inclusion and exclusion criteria, which may have had some impact on effect estimates and conclusions. We included quasi-experimental designs in our systematic review, which often did not adequately account for confounding, potentially affecting reported estimates. Such aspects were considered when assessing risk of bias and the certainty of evidence.
One limitation specific to the systematic review was that we examined a small set of sources of clinical and methodological heterogeneity. We did not assess other potentially relevant ones; for example, we did not differentiate studies that may have used varying definitions of SGA, PTB and other outcomes. We also did not examine potentially different effects by region, which may be relevant given the distinct geographical distribution of LBW, PTB, SGA.1 2 115 As such, given the low number of studies for any single comparison, consideration of these would most likely not be particularly informative; due to the scarcity of studies for any single comparison, we were unable to parse potentially important effects of interventions by age, preconception period when interventions were conducted, and country income setting. Additionally, as we combined studies for distinct interventions within subgroups, particularly in the health domain, this review may offer only broad conclusions about their effect on the outcomes of interest. Finally, due to there being generally few studies per comparison, we did not conduct subgroup and sensitivity analyses or assess publication bias for all comparisons as we had originally planned in the protocol.
Importantly, many of these limitations may be viewed as important findings, justifying the call for further research in this area. Furthermore, this systematic review has several strengths. To our knowledge, this systematic review and meta-analysis is the first to comprehensively assess evidence on the effect of preconception interventions on the risk of LBW, SGA and PTB. We searched multiple databases for published evidence and did not place limits regarding specific intervention types or domains, language or publication date, allowing us to identify all possibly relevant interventions. We also considered evidence on other birth and maternal outcomes, and followed a systematic method to summarise, analyse and consider the quality of available evidence.
Conclusion
While interventions delivered during pregnancy have demonstrated the potential to reduce the risk of LBW and related outcomes, reported effects have generally been modest.13 94 Consequently, the preconception period is increasingly considered as an additional window of opportunity where interventions may have larger impact on such outcomes. In this systematic review, we aimed to summarise current evidence on the effect of preconception and periconception interventions on LBW, SGA and PTB. We noted that the available evidence is generally very uncertain regarding any impact of such interventions. Importantly, our findings indicate that there is not yet sufficient high-quality evidence to understand their effect. Further, well-designed studies are required on the effectiveness of preconception nutrition, health, social and environmental interventions delivered either singly or in combination, in preventing LBW, SGA, PTB and other birth and maternal outcomes.
Data availability statement
Data are available on reasonable request. Data and other materials are available from the authors on reasonable request (contact corresponding author at: upartap@hsph.harvard.edu).
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Soumyadeep Bhaumik
Twitter @ranapersplexing
Contributors RB, ADC, WF, NB, ST, RC and UP designed the study. RC and UP conducted the literature search, extracted data, and undertook risk of bias and quality assessments. UP conducted data analysis, and RC and UP interpreted the data along with RB, ADC, WF, NB and ST. UP drafted the manuscript with input from RC, and RB, ADC, WF, NB and ST reviewed and critically revised the manuscript. UP and RC accessed and verified all the data in the study, and all authors had full access to all the data in the study. All authors had final responsibility for the decision to submit for publication. UP is the guarantor of this work.
Funding This study was funded by the Children’s Investment Fund Foundation. The funding source had no role in the writing of the manuscript or the decision to submit for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.