Article Text

Abstract
Globally, non-communicable diseases (NCDs) or chronic conditions account for one-third of disability-adjusted life-years among children and adolescents under the age of 20. Health systems must adapt to respond to the growing burden of NCDs among children and adolescents who are more likely to be marginalised from healthcare access and are at higher risk for poor outcomes. We undertook a review of recent literature on existing models of chronic lifelong care for children and adolescents in low-income and middle-income countries with a variety of NCDs and chronic conditions to summarise common care components, service delivery approaches, resources invested and health outcomes.
- Health systems
- Paediatrics
- Review
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Chronic conditions account for one-third of disability-adjusted life-years for children and adolescents which impacts future healthcare needs, and long-term health outcomes and trajectories across the life course. A majority of research on the effectiveness of comprehensive models of chronic care have been drawn from research among adults, and primarily from research on models of HIV care.
What this study adds
We identified common components of care, service delivery approaches and resources invested to support models of chronic care for children and adolescents globally. Care components focused on patient and family education to support disease self-management, underscore mental health and psychosocial well-being, and integrate social and community services for sustainability of care; service delivery approaches focused on decentralised care and accessible and patient-centred care to increase uptake and sustain follow-up; and resources invested included health worker training in chronic care and paediatric and adolescent development, and adequate infrastructure.
How this study might affect research, practice or policy
Common elements of the models of care identified in this review can inform the development and implementation of comprehensive chronic care for children and adolescents. Despite a growing global burden of paediatric chronic diseases, this review found a limited body of evidence of comprehensive models of chronic care with a majority focused on HIV. More robust implementation research on a diverse set of chronic conditions will inform the development of effective programmes to mitigate poor health outcomes of a burgeoning paediatric chronic disease epidemic.
Introduction
Substantial global progress has been made in reducing childhood mortality since 1990. The total number of under-5 deaths worldwide has declined from 12·6 million in 1990 to 5·0 million in 2020.1 Nonetheless achievements in reducing the morbidity burden, as measured by year of life lost due to disability and disability-adjusted life-years (DALYs), do not match the progress shown in reducing mortality in young people.2 Non-fatal health loss makes a substantial contribution to the total disease burden among children and adolescents enabling young people to now live with and manage chronic conditions along their life course.3 4 Chronic conditions now account for one-third of DALYs for children and adolescents which can affect future healthcare needs, long-term health trajectories and productivity prospects dependent on physical and intellectual development.5 6
Health systems in low-income and middle-income countries (LMICs) have traditionally focused paediatric care around acute management of episodic communicable diseases. To respond to the increase of non-communicable diseases (NCDs) in children and adolescents, health systems must adapt to provide monitoring and treatment of chronic conditions including changes to service delivery and clinical information systems, and the development of new approaches to care including resources for self-management support.7 These changes must be designed and implemented with consideration of the unique needs of paediatric and adolescent populations, as they are more likely to be marginalised from healthcare access.8 Children and adolescents have limited agency to advocate for their needs, depend on caregivers for knowledge and access to care, and often are at disproportionally heightened risk for factors affecting their health including poverty, violence and limited education. Childhood and adolescence are also critical developmental periods during which young people establish lifestyle habits and make choices that can mitigate or accelerate disease progression.9 Positive experiences and interactions with the health system can establish the foundation for a future of positive health-seeking behaviours.10
Data on the effectiveness of various aspects of chronic care such as where care is delivered, how longitudinal follow-up is structured and what types of support are needed to longitudinally manage disease is primarily drawn from research among adults and our knowledge on this topic for children and adolescents in LMICs is primarily drawn from research on models of HIV care.11–14 Evidence on the effectiveness of chronic care models in this younger population is essential to achieve optimal health outcomes and launch a trajectory for sustained health along the life course.
In this scoping review, we evaluate the literature on models of care for children and adolescents with a diverse set of chronic conditions in LMICs and summarise common components of care, service delivery approaches and resources invested for model implementation. We then assess the existing evidence of effect on child and adolescent health outcomes. Our goal is to draw from existing, recent evidence to inform a contemporary model of chronic lifelong care for children and adolescents.
Methods
Search strategy and selection criteria
This is a scoping review, following the Arksey and O’Malley framework, on models of chronic lifelong care for children and adolescents in LMICs (figure 1).15 We defined ‘model of care’ as a system of health service delivery or multicomponent intervention aimed at improving health outcomes for children and/or adolescents. We searched Medline, PubMed, and the Cochrane library databases with search terms “model of care”, “chronic disease”, “chronic care”, and “pediatric OR child OR adolescent OR youth”, and terms for each specific condition (eg, “HIV”, “diabetes”) (figure 2). A diversity of chronic conditions was selected based on their contribution to the global burden of disease, and with the aim to include conditions that require levels of care that vary in intensity, frequency and resources. An external expert group, convened by UNICEF and composed of health professionals with extensive expertise in paediatric chronic diseases, provided guidance on the scope and direction of this review and recommendations based on the results. We searched the literature for models of care for these 11 selected conditions: asthma, cancer, cerebral palsy, cystic fibrosis, depression, diabetes, disabilities, hepatitis B, HIV, rheumatic heart disease and syphilis. We limited studies to manuscripts published after 1 January 2015 to build off a previous review of the same scope.14 We did not set language limits. One reviewer (LKR) conducted the primary search, the external expert group guided the selection of references that were comprehensive and relevant to the scope of this review and solved any disagreements by consensus, and all authors approved of the final selection of references.

Scoping review objective and methods.

Flow chart for articles which were reviewed and included.
Patient and public involvement
Patients nor the public were involved in the design, conduct or dissemination plans of this research.
Data extraction and synthesis
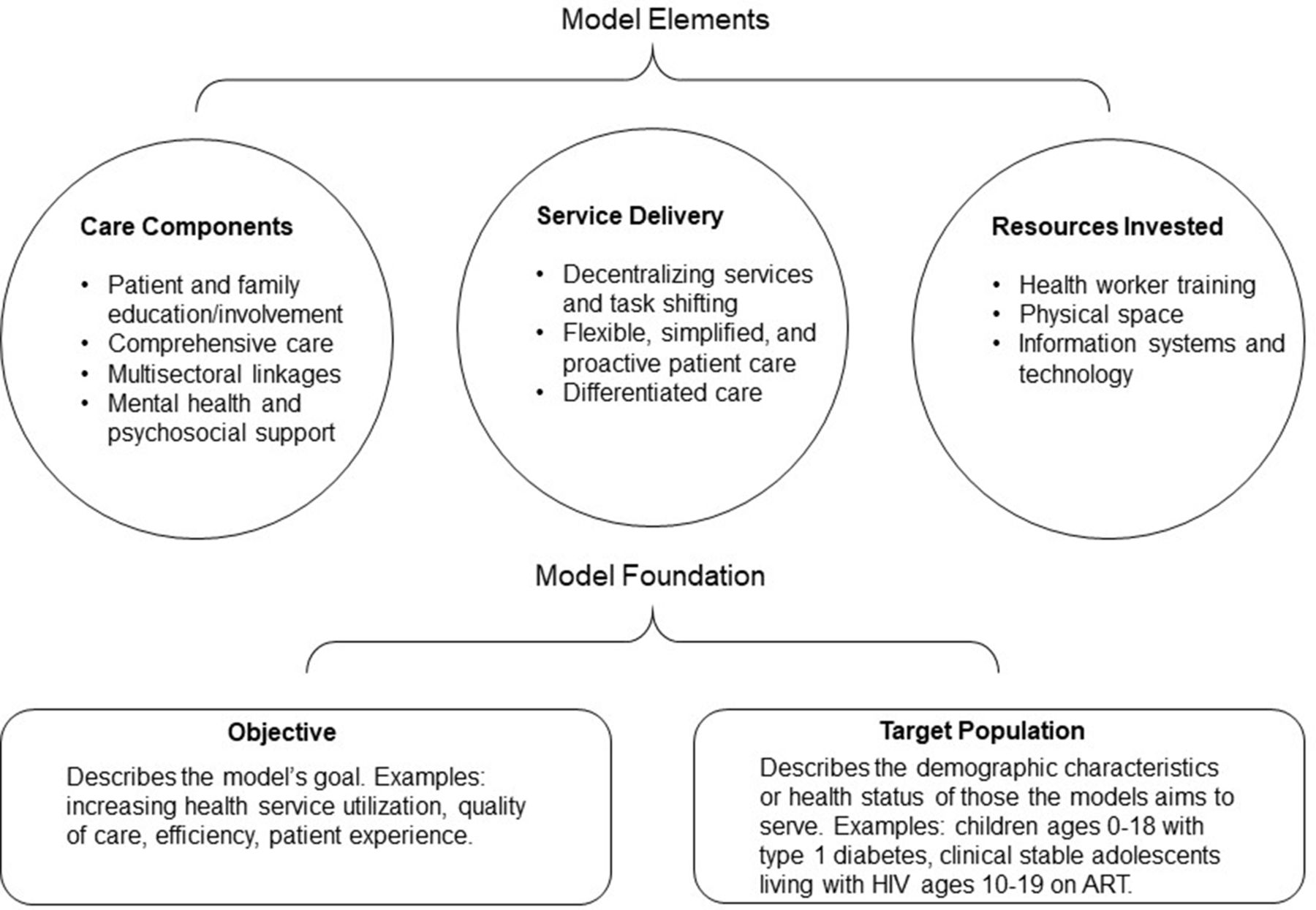
Data extraction from the manuscripts selected was guided by an adapted version of the foundations framework which describes the theoretical basis—the foundation—of a model of care, and the core components and principles—the elements—of a model of care (figure 3).16 The model’s foundation includes: (1) the objective and (2) the population targeted. The objective describes the model’s goal, for example, improving health service utilisation, quality of care, health service efficiency or patients’ experience, and the explicit objective the model aims to achieve. The population targeted describes the demographic characteristics or health status of those the model aims to serve. The model’s elements include: (1) care components; (2) service delivery and (3) resources invested. Care components are the mechanisms to support patients’ access or use of services. Service delivery is how care components are organised in the health system and offered/provided to a patient. Finally, resources invested describe the inputs required for the model’s implementation. Models were categorised based on the primary location of service delivery—facility based, community based or a hybrid—and the primary focus of the care provided—individuals, families or peer groups.

{kind=link}
{kind=link}
{kind=link}
Adaptation of the foundation framework to map components of chronic lifelong models of care for children and adolescents. Adapted from Stokes et al.16 ART: Antiretroviral Therapy.
We synthesised the evidence to identify major themes and commonalities across care components, service delivery approaches and resources invested. We aligned this thematic analysis according to the WHO guidance and standards for child and adolescent care.17 We also summarised the health outcomes reported across studies, by condition.
Results
Description of studies identified
We identified 16 publications which met our inclusion criteria. The studies assess models of care for five conditions: asthma (n=1), cerebral palsy (n=1), diabetes (n=2), HIV (n=11) and mental health (n=1). We summarise the content of each model’s foundation and elements according to the foundation framework and the health outcomes measured (table 1). Study target populations varied: two focused on children <12 years; six focused on adolescents ages 13–19 and eight studies included children and adolescents. The mean number of participants was 2097 (range 50–11 695). Study designs varied with four retrospective cohorts or chart reviews, four prospective observational cohorts or pilot studies, four randomised controlled trials and four programmatic descriptions. Studies were conducted across several regions: East Asia and Pacific (China), Europe and Central Asia (Turkey), Latin American and the Caribbean (Haiti), South Asia (India) and Sub-Saharan Africa (Ethiopia, Ghana, Kenya, Malawi, South Africa, Tanzania, Uganda, Zambia, Zimbabwe). We mapped care components, service delivery approaches and resources invested across studies to quantify and compare frequencies (table 2).
Summary of recent studies describing models of chronic lifelong care for children and adolescents in LMICs
Mapping of elements of each model of care across included studies
Types of models
Studies included three categories of model types—eight facility-based models, all focused on individual patients; six community-based models, one focused on individual patients, four focused on the family and one on peer groups; and six hybrid models which included facility and community-based activities, two focused on individual patients and four focused on the family.
Model elements
Care components
Patient and family education/Involvement
The most frequently incorporated care components were patient education and family involvement, each used in ten models (table 3). Patient education, often by a trained community health worker, focused on disease self-management and accessing supportive services. In Uganda, type 1 diabetes mellitus (T1DM) clinics provided patients with a curriculum, Diabetes Self-Management Education, starting at diagnosis. Patients ages ten and over participated in an additional 5-day structured training in self-management of diabetes. The training was facilitated by health workers with a major focus on identifying and independently accessing self-support resources outside of the clinical setting.18 In South Africa, community-based support workers provided education on disease management and treatment adherence for HIV and tuberculosis to patients and caregivers during regular home visits.19 In India, trained lay health workers visited patients and their families at home to provide psychoeducation, health promotion, psychosocial rehabilitation and relapse prevention services for mental health disorders.20
Summary of common model elements and approaches to inform models of lifelong care for chronic conditions for children and adolescents
Facilitating family education and involvement in care was often done by involving families in intake assessments and when establishing longitudinal care plans. In Turkey, a nurse conducted home visits for adolescents with diabetes and involved family in developing and monitoring care plans to support proper monitoring of blood glucose, insulin administration, nutrition and exercise.21 The primary activity of the ‘Getting to Know Cerebral Palsy’ intervention was caregiver education to equip caregivers with the knowledge of how to care for their child, how to structure their own peer support groups and access community resources.22
Comprehensive care
A comprehensive care approach to address a patients’ full range of physical, mental and social health service needs was included in the model for mental health, in both models for diabetes, and in 7 of the 11 models for HIV (table 2).18–21 23–28 Nine models used multidisciplinary care teams, for example, physicians and specialists to manage complex clinical care, nurses and trained community health workers to manage long-term follow-up and routine care, and social workers or case managers to address family, social and community support. Similarly, the use of a case manager to oversee and manage patients’ engagement with each aspect of care—physician visits, nurse follow-up visits and social worker support was used in eight studies.19–22 24 25 27 28
Multisectoral linkages
Linkage to services to support non-clinical needs, such as food insecurity, housing assistance, or school fees, often facilitated by a social worker or case manager was a component in six of the models (table 2). Three HIV models included a specific role for linking patients to non-clinical community resources. In South Africa, a community-based support worker did eligibility assessments for government social assistance grants and guided the application process.19 In Zimbabwe, the Zvandiri peer community adolescent treatment supporters (CATS) provided Department of Social Services referrals.27 Finally, in the Zambian ZAMFAM intervention primary caregivers of HIV patients were linked to village loan groups to help them meet financial and nutritional needs.28
Mental health and psychosocial support
Mental health or psychosocial services were provided in six models, five of which focused on adolescents with HIV (table 2). The FANMI (Haitian Creole for ‘My Family’) intervention in Haiti consisted of groups of 5–8 adolescents who met monthly, replacing the 1-on-1 clinician visit. The group setting provided a social support network for adolescents to share experiences and a curriculum on dealing with stigma, building self-confidence and developing coping skills to address psychosocial risk factors that could impact antiretroviral therapy (ART) adherence.24 In the Zvandiri intervention, peer CATS were trained to identify patients with mental health disorders and link them to mental health services.27 In Ghana, an education and support group for caregivers of children with cerebral palsy emphasised sharing experiences and building a peer support network to enhance their own quality of life.22
Service delivery
Decentralising services and task shifting
Decentralising services to make them accessible at local clinics or health centres as opposed to solely in regional or referral health facilities was the most common service delivery approach, used in all 11 HIV models and in 12 models total (table 2). In Uganda, T1DM specialised clinics were placed in primary care facilities nationwide.18 In India, rural HIV centres that lacked trained paediatric HIV specialists used videoconferencing for consultation with a paediatric HIV centre of excellence on HIV management, ART initiation and follow-up, management and/or prophylaxis of opportunistic infections, drug toxicities, nutrition and adherence counselling, and age-appropriate disclosure. Further, this telemedicine approach facilitated training, mentoring and capacity building of peripheral site staff.20 Reorganising the health workforce by task-shifting to make more efficient use of limited health human resources and enable a facility to treat a higher volume of patients was widely employed—nine HIV models included specific roles for nurses or trained lay health workers to conduct routine follow-up for stable patients.
Flexible, simplified and proactive patient care
Each model adapted care in some way to be more accessible for patients (table 2). Components that made care-seeking easier for patients included home visits for regular care, used in eight models, colocating services in a single clinic to be more convenient for patients, used in four models, 24/7 telephone access for patients’ questions, used in two models and extended clinic hours, used in one model. Mobile phone access to a provider or appointment reminders via text, used in six models, were also ‘proactive’ services to encourage and support retention in care and adherence to treatment.
Differentiated care
Six models classified as differentiated models of care in which patients are stratified based on level of care needed, aiming to better serve patients and reduce health system inefficiencies (table 2). Two models of care for HIV—Standardised Paediatric Expedited Encounters for ART Drugs Initiative and Multi-Month Prescriptions—were structured specifically around less frequent clinical visits, or nurse-only visits for clinically stable patients with adequate ART adherence or viral suppression.29 30 In FANMI, a monthly cohort meeting of 5–8 adolescents living with HIV replaced the individual physician–patient visit and participants were referred to a physician visit only if clinically indicated.24 This approach both transitioned participants to nurse-led care and increased the number of patient encounters a nurse could manage daily by providing care in a group setting.
Resources Invested
Five studies, nearly one third, did not include information on resources invested. Among those that did detail types of resources required for model implementation, training of health professionals or lay health workers was the most frequently cited with eight models specifically providing health professionals education in a chronic disease (table 2). Health worker training to implement T1DM clinics in Uganda included regular refreshers and attendance at international and regional conferences to remain current with treatment guidelines.18 The training of lay mental healthcare workers in India included a full week of didactic lectures followed by 3 months of field training including shadowing clinicians.20 Four models required designating clinical space for patient care, either by reallocating existing space or establishing new space. Lastly, information systems and technology were common resources invested. Mobile phones were used to support communication between patients and providers in five models. Telehealth was the primary intervention for two models of care. One in China used a smart phone application for patients and caregivers to enter routine health information, adherence tracking and communicate between visits.31 Another in India, used a video conference system to connect paediatric centres of excellence to rural sites for patient management and consultation.23
In table 3, we summarise common model elements and approaches with examples from the models described above that can inform the development and implementation of effective models of chronic care for children and adolescents.
Health outcomes
The nature of a scoping review includes broad inclusion criteria and evaluation of a diverse set of diseases and conditions which makes a direct comparison of each models’ impact on health outcomes inappropriate. Instead, effect on health outcomes, reported in each study are outlined in table 1, and we provide a summary of the most significant improvements to health outcomes, organised by chronic condition, below.
Asthma
The nurse-led, mobile application-assisted model of asthma care showed a decrease in the frequency of asthma exacerbations among intervention participants compared with control participants at 1 year (3 vs 4, p<0.001), showed slightly higher medication adherence among intervention participants compared with control participants (94.46% vs 92.67%, p<0.05), and showed lower respiratory tract infections among intervention participants compared with control participants (3 vs 4, p<0.05).31
Cerebral palsy
A community-based caregiver-focused model of cerebral palsy care showed mixed results with an improvement in caregiver mean quality of life score (12.5–51.4, p<0.001) and decrease in recent child illness episodes measured 2 weeks after intervention completion (64% to 50%, p<0.05), but persistently high rates of malnutrition (63% vs 65%, p=0.5) and high serious illness frequency over the twelve months of intervention implementation (67%).22
Diabetes
The implementation of T1DM clinics in primary care facilities in Uganda showed low mortality (3.8%) and loss from care (2.1%) over a ten year period, however, no improvement in glycaemic control measured by mean hemoglobin A1C (HbA1c) was observed between baseline and several follow-up time points.18 Authors hypothesise financial barriers (eg, cost of transport to health facility), no support for medicine for comorbidities and persistent lack of understanding of HbA1c as a target of glycaemic control leading to less rigorous self-monitoring contributed to a lack of improvement of this outcome.
HIV
A majority of HIV models showed improvement in participants’ retention in care and several showed an increase in the proportion of participants who achieved viral load suppression. For example, a streamlined HIV test-and-treat model of care which provided community-based testing and immediate clinic evaluation for ART initiation, and offered extended clinic hours, and flexible appointment dates and locations achieved high retention in HIV care (89% at 1 year) and high rates of viral suppression (<500 copies/mL) (92% of those in care with a viral load measurement).32 A community-based support worker model showed a high rate of retention (>85%), a low rate of mortality (<5%) and a high rate of viral load suppression (>80%) 5 years after model initiation.19
Mental health
A lay health worker model of mental healthcare showed a high number of cases identified by lay health workers over a 14-month period (n=279) and a high proportion of immediate linkage to psychiatric consultation (n=262, 94%). A high proportion of patients (78%) and family members (78%) were retained in care at twelve months. Patients showed significant improvements in clinical, functional and quality of life outcomes, all measured using validated scores.20
Discussion
In this scoping review, we identified 16 studies that evaluated models of chronic care for children and adolescents in LMICs. Across models, care components focused on patient and family education to facilitate appropriate disease self-management, emphasised mental health and psychosocial well-being, and included a comprehensive care approach that incorporated supportive social and community services which are integral to maintaining health over the long term. Service delivery approaches were responsive to the shifting burden of disease from a focus on acute illness to providing longitudinal care of chronic diseases. This included a focus on decentralising care from large referral centres to local clinics and health centres and designing patient-centred and accessible services to increase uptake and ensure follow-up, while maintaining health system efficiency. The resources needed to support these models focused on health worker training in both chronic disease specialties and in paediatric and adolescent development, and advancements in health infrastructure including adequate physical space, information systems and technology.
Decentralising services was the most common model element. As health systems align with the increasing burden of NCDs, with the most dramatic shifts occurring in LMICs, primary care centres must build capacity to provide integrated disease prevention, screening and treatment in a way that is patient-centred and easily accessible since care needs to be regular and sustained, using a longitudinal approach to care across the life course.33 Several different approaches to decentralisation were identified in the studies in this review. Placing a chronic disease-specific clinic within a primary care facility serves to co-locate specialised services which requires availability of high level healthcare specialists.18 Alternatively, training primary healthcare workers in the screening, diagnosis and treatment of chronic conditions builds provider capacity but requires resources including established training curricula and materials and expertise to train.24 25 34 This approach, often employed as ‘task-shifting’ to train less specialised health workers such as nurses and clinical officers in the prevention, screening and management of a specific disease has been used widely in HIV care.35–37 Applying these lessons to chronic disease management could improve the accessibility and quality of care for children and adolescents with chronic conditions.
Patient and family education and involvement was also heavily emphasised. Building patient capacity for self-management is central to chronic lifelong care.37 Patients and caregivers must manage medication regimens and schedules, coordinate consistent interactions with the health system, and make lifestyle decisions that accommodate their condition and promote health. Education was often the primary focus of a care plan to ensure patients and caregivers were equipped with the knowledge to manage their disease and the problem-solving, decision-making and resource-utilisation skills to enable the self-efficacy to manage complications over the long-term. Patient education can be administered by trained lay health workers—a task shifting approach to share the burden of continued education with highly skilled clinicians.38 39 Empowering patients with the knowledge to understand their chronic condition, recognise their needs and identify and access resources to support their own health enables effective disease self-management.40 In paediatric models of care, family-centred care is essential to support self-management, given the significant role of the caregiver in a child’s health.41 Involving families in the care plan strengthens the patient’s immediate support network and further, when caregivers and family members’ own health and well-being are addressed, they are better prepared to provide the necessary level of care and oversight of the child’s or adolescent’s health needs.42–46
Comprehensive care and linking patients to social and community services and resources to support overall well-being was an essential component of most models. The management of chronic conditions for children and adolescents requires access to a range of health services since health outcomes are closely linked to behaviour, social and physical environment and socioeconomic status.47 48 Chronic disease management may require the support of a broad and diverse team of providers including physicians, nurses, behavioural specialists, dieticians, psychologists and social workers.49 50 Further, a case manager or care coordinator role on a patient’s care team can serve to adequately incorporate and synchronise long-term clinical and social services.
Mental health and psychosocial support are particularly central to child and adolescent health outcomes. A range of psychosocial aspects—family and social support, peer influence, experienced or perceived stigma—all impact a child or adolescent’s psychosocial well-being and capacity for self-care of chronic conditions.51 52 Opportunities to engage with peer educators or ‘expert patients’, group-based care and activities, and facilitating family and community involvement can strengthen social support and prevent or address psychosocial and mental health challenges.37 53–55 The adolescent period is a particularly dynamic developmental period of biological, social and emotional growth during which peer relationships and social networks may carry enhanced impact on health behvaiors.56 57 Training providers on the vulnerability of adolescence can equip them with the ability to predict, understand and respond to patients’ needs and identify periods of change or instability that could impact self-management or care-seeking.58–60
Lastly, a common theme was the design and delivery of patient-centred services that are accessible and easily incorporated into patients’ lives to increase uptake and facilitate better retention and medication adherence. Healthcare focused on acute illness or episodic treatment are generally patient initiated and brief, with limited attention to care planning, patient education and care coordination. Part of chronic care requires proactive care planning, anticipating patients’ needs and planning for future visits. It also requires tailored and flexible care plans that match individuals’ needs, which shift according to both disease and developmental status. Proactive outreach to patients such as appointment reminders via text, home-based care, medication delivery, extended clinic hours, tracking patients lost from care or telephone management for routine check-ups and patient questions were used across models and have shown to be effective.61–64
The most common type of resource investment across models was health worker training in the screening, diagnosis and treatment of chronic conditions. This requires established training curricula and materials, guidelines on certification, and expertise to train. Lastly, repurposing or creating new physical space for chronic disease care services in primary care facilities and advancing healthcare infrastructure including wider internet access, access to point-of-care technologies, greater laboratory capacity and longitudinal patient information systems will bolster the quality of accessible chronic disease care.
A previous review by Graham et al which included studies published through 2015 on the same topic area—strategies for chronic care for children in LMICs found results similar to ours—strong evidence for patient, family, and community education and involvement; integration of community resources and psychosocial support; and emphasised the importance of health system inputs including health worker training, infrastructure and information systems.14 Further, they noted the dearth of evidence on comprehensive models of care and any in the literature were limited to HIV models of care. Our review shows limited progress in increasing the number of these evaluations and expanding the diversity of conditions addressed with just 16 studies of models of care identified, a large majority of which again focused on HIV. Reasons for this could be attributed to the challenges associated with rigorous evaluations of complex and multipronged interventions and models of care, feasibility of long-term longitudinal follow-up required for evaluating chronic disease outcomes and funding priorities which remain HIV-focused.
This review has several limitations to note, which also serve to highlight several gaps in the literature. First, the number of studies identified that have evaluated full models of chronic disease care were limited, heavily weighted by those focused on HIV and only included four randomised trials. A broader evaluation of targeted interventions could provide additional evidence for specific aspects of chronic disease services and a greater number of randomised trials, while feasibly challenging for evaluations of comprehensive models of care, could generate stronger evidence of impact. Second, several components common to paediatric and adolescent chronic care are not represented including school-based activities and transitions in care. Only two models of care included brief mention of school-based activities, neither of which were central components. The school environment can be particularly influential in child and adolescent health outcomes and more meaningful engagement of school-based activities and a stronger relationship between schools and care providers may provide an opportunity to strengthen models of chronic lifelong care.65 Importantly, for many childhood chronic conditions—HIV, diabetes, congenital heart disease, cystic fibrosis—healthcare transition from paediatric to adult services is associated with disruptions in retention in care, poor medication adherence and subsequent decline in health outcomes.66 Research has established many of the barriers adolescents face in transitioning to adult care67–70 and guidelines have been established including written protocols and timelines to advise transition.71 72 However, data on the impact of interventions to improve transition to adult care is limited and a focus on transition was not a key consideration in any model of care identified in this review. Third, the studies did not systematically include adequate information on implementation details such as cost, buy-in from local or national partners, and training materials which limits our ability to assess potential for scale-up and sustainability particularly in low-resources settings. Lastly, few models spoke to the role of tertiary care centres–which play an important role in the management of some chronic conditions–or provided minimal description of referral to higher level care for serious complications. For certain chronic conditions, highly skilled care will be required over the life course (eg, asthma exacerbations, diabetic ketoacidosis) or conditions may become more advanced or severe later in life (eg, congenital heart disease). Describing plans for coordinating referral and linkage to higher level care is a key consideration and should be included in lifelong care models.
Conclusion
This review identified a very limited body of evidence considering the growing global burden of chronic disease in this young population and a particularly dramatic relative increase of in LMICs. More robust implementation research led by local investigators, scale-up of promising interventions applicable in resource-limited settings and evaluation of models of chronic lifelong care are highly warranted. Research and reported evidence for effective models of chronic disease care that includes details on implementation, cost and linkage between primary and tertiary care to inform the development of comprehensive, effective and scalable programmes will contribute to mitigating the health consequences of the burgeoning chronic disease epidemic in children and adolescents globally.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
This study did not involve human subjects research and Ethics Committee review and approval was not required.
References
Footnotes
Handling editor Sanne Peters
Twitter @rachelnugent
Contributors LKR conducted the initial literature review and wrote the first draft of the manuscript and served as the guarantor. NP and RB developed the research topic concept, assembled an expert group and provided guidance on the scope of the research topic, study design, interpretation of results. JvO, SA, NP, RB, RN, EP, BD, CV and EJA were members of an expert group who provided guidance on scope of the research topic, study design and interpretation of results. MM and NS provided guidance on the scope of the research topic interpretation of the results. All authors contributed to the writing and editing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.