Article Text

Abstract
Introduction High-income country (HIC) authors are disproportionately represented in authorship bylines compared with those affiliated with low and middle-income countries (LMICs) in global health research. An assessment of authorship representation in the global emergency medicine (GEM) literature is lacking but may inform equitable academic collaborations in this relatively new field.
Methods We conducted a bibliometric analysis of original research articles reporting studies conducted in LMICs from the annual GEM Literature Review from 2016 to 2020. Data extracted included study topic, journal, study country(s) and region, country income classification, author order, country(s) of authors’ affiliations and funding sources. We compared the proportion of authors affiliated with each income bracket using Χ2 analysis. We conducted logistic regression to identify factors associated with first or last authorship affiliated with the study country.
Results There were 14 113 authors in 1751 articles. Nearly half (45.5%) of the articles reported work conducted in lower middle-income countries (MICs), 23.6% in upper MICs, 22.5% in low-income countries (LICs). Authors affiliated with HICs were most represented (40.7%); 26.4% were affiliated with lower MICs, 17.4% with upper MICs, 10.3% with LICs and 5.1% with mixed affiliations. Among single-country studies, those without any local authors (8.7%) were most common among those conducted in LICs (14.4%). Only 31.0% of first authors and 21.3% of last authors were affiliated with LIC study countries. Studies in upper MICs (adjusted OR (aOR) 3.6, 95% CI 2.46 to 5.26) and those funded by the study country (aOR 2.94, 95% CI 2.05 to 4.20) had greater odds of having a local first author.
Conclusions There were significant disparities in authorship representation. Authors affiliated with HICs more commonly occupied the most prominent authorship positions. Recognising and addressing power imbalances in international, collaborative emergency medicine (EM) research is warranted. Innovative methods are needed to increase funding opportunities and other support for EM researchers in LMICs, particularly in LICs.
- other study design
- health policies and all other topics
Data availability statement
Data are available upon reasonable request. Data are available for free on reasonable request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous studies in the global health literature have demonstrated inequities in authorship representation; however, none has examined this topic in the relatively new field of global emergency medicine (GEM). Promoting authorship equity in GEM at an early stage in its development may ensure more equitable practices as GEM develops.
WHAT THIS STUDY ADDS
There were significant disparities in representation of authors affiliated with low and middle-income countries (LMICs) compared with high-income countries (HICs).
Authors affiliated with HICs were most commonly listed in the first, second and last author positions while local (study country) author representation in these positions was lowest among authors affiliated with low-income countries.
Having a local funding source and smaller authorship groups were associated with greater odds of local first and last authorship.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Innovative methods are needed to increase funding opportunities and other support for EM researchers in LMICs to ensure more equitable authorship representation, particularly in low-income countries.
Introduction
Global health is a broad and interdisciplinary field focused on ‘improving health and achieving equity in health for all people worldwide’.1 Despite the field’s emphasis on equity, a growing body of literature has highlighted pervasive inequities in global health research that mirror existing power asymmetries between researchers based in low and middle-income countries (LMICs) versus high-income countries (HICs).2–6 One such inequity is seen in authorship representation in global health research conducted in LMICs.2 4 7 Previous evaluations of authorship equity within the general global health literature have shown under-representation of LMIC authors and a predominance of authors affiliated with HIC institutions.7 8 These discussions are not limited to academia, and calls for equitable representation and influence of patients, clinicians and policymakers from LMICs in decision-making processes are similarly ongoing.9–11
Global emergency medicine (GEM) is a relatively new, and rapidly growing, subspecialty bridging the fields of global health and emergency medicine (EM), which focuses on improving the science and practice of emergency care (EC) globally.12–14 It encompasses a wide breadth of topics including the development of the EM specialty and EC systems in areas where such systems do not exist as well as clinical care during humanitarian emergencies.12 14 Despite the burden of conditions that fall within the scope of EM disproportionately affecting LMIC populations (eg, traumatic injuries, acute presentations of communicable and non-communicable diseases as well as presentations of a variety of other illnesses), global EM development has until recently, largely been led by academics from HICs where EM was originally pioneered. Notably, nearly all postgraduate fellowships in global EM are based in North American institutions, while most GEM projects are conducted in LMICs.13
If, and how, LMIC researchers are recognised in scientific publications in comparison to their HIC counterparts may be both a cause and consequence of unequal power dynamics in global health collaborations. Inequitable authorship representation, therefore, may be considered a ‘symptom’ of a more widespread disease characterised by systemic injustices in international collaborative partnerships that urgently need to be recognised and undone. In particular, first and last authorship positions are considered positions of prestige that can impact career advancement and create opportunities for acquiring subsequent research funding.15 Prior evaluations of authorship equity in the global surgery, paediatrics and infectious disease fields have found that first and last author positions are disproportionately held by researchers affiliated with HIC academic institutions.2 4 5
To date, there has not yet been an evaluation of authorship representation within the GEM literature. As one of the newest specialties in medicine, with rapid uptake in many countries in the past decade, it is essential to critically examine the state of authorship representation in GEM research. Identifying these patterns in GEM can help to shape the future of this emerging field, as the specialty continues to develop globally. Therefore, our aim was to evaluate authorship representation and distribution of researchers from LMICs and HICs in recent global EM articles published from 2016 to 2020.
Methods
Study design
This was a cross-sectional study of articles reporting original EM research conducted in LMICs published between 2016 and 2020. As this study used only previously published articles and did not involve any human subjects, institutional review board approval was not necessary.
Data source and identification of GEM articles
Citations previously identified for full-text evaluation from the 2016 and 2020 annual Global Emergency Medicine Literature Review (GEMLR) were screened for inclusion in this study. Since 2005, the GEMLR group has conducted an annual review of the peer-reviewed and grey literature to screen, evaluate and review the most rigorously conducted and relevant research in GEM published each year.12 Each year the complete database of selected articles as well as full summaries and critical analyses of the top articles are published in Academic Emergency Medicine online and open access. The screening methods and inclusion criteria for the GEMLR review have been previously described and were consistently applied from 2016 to 2020.12 Articles from the 2016 to 2020 GEMLR data sets were obtained by downloading the data sets which are available to the public online at www.gemlr.org.16
Inclusion and exclusion criteria
Articles were included in this study if they were included in GEMLR, reported original research conducted in an LMIC and were published in a peer-reviewed journal. For multicountry studies, articles were included if they included at least one LMIC as a study site. Systematic reviews, editorials, case reports, review articles, grey literature, conference abstracts and studies that exclusively used publicly available data sets were excluded. Studies which listed only a single collaborative authorship group (eg, CRASH-3 Collaborators) were excluded because author affiliations were unavailable.
Data extraction and variables
Articles were previously assigned by the GEMLR review group into three categories: Emergency Care in Resource Limited Settings (ECRLS), Emergency Medicine Development (EMD) or Disaster and Humanitarian Relief (DHR). For each article, the following data were extracted: article title, journal name, publication year, GEMLR category (ie, ECRLS, EMD and DHR), main study topic (later divided into subfields based on frequency), study design as reported in the article, publication language(s) (of either the abstract or full manuscript), study country(s) (ie, country where data were collected or from which data were obtained), number of authors, each authors’ order in the authorship list, each authors’ number of affiliations, the country of each author’s listed affiliation(s), if a funding source was listed, funding source type (government, industry, private foundation, academic institution, healthcare facility, non-governmental organisation (NGO), other) and the country(s) of the funding support. Articles and author affiliations were categorised using countries’ 2021 World Bank income classifications.17 Each country was categorised by region using WHO’s assignment of regions: African region, Region of the Americas, South-East Asian Region, European Region, Eastern Mediterranean Region, and Western Pacific Region.18
Articles were categorised based on the classification of the study country(s) as low-income country(s) (LIC) only, lower middle-income country(s) (MIC) only, upper MICs only and mixed income categories. Authors were categorised by the country(s) of their listed affiliation(s) as LIC only, lower MIC only, upper MIC only, HIC only or mixed affiliations. Authors were also categorised as being affiliated with the study country only, HIC only or other (ie, non-study country LMIC or mixed affiliation). Funding support data were extracted from the articles’ funding declarations (if one was published with the article). Articles were categorised as having any funding support or not; for those with a listed funding source, the country(s) of funding support were extracted. Data were extracted using a custom REDCap form that was piloted by members of the study data extraction team. An iterative process was used to revise the tool until consensus was achieved. To ensure quality of data acquisition, 5% of the articles were randomly selected for cross-check. Less than 5% of these articles had discrepancies. These few discrepancies were addressed by repeated review among two members of the data extraction team until consensus was achieved.
Data analysis
Descriptive analyses (ie, frequencies with percentages or medians with IQRs) were used to characterise the included articles according to GEMLR category, study topic, year of publication, World Bank income classification, WHO region, study design and number of study countries (single country vs multicountry). Author data were described using total proportions of authors categorised by World Bank income classification. Author data were also stratified by first, second and last authorship positions, and by affiliation with study country only, HIC only or other. Comparisons were conducted using Χ2 test. For single-country studies, multivariable logistic regression was performed to assess the association between the independent variables of WHO region, study country income classification (LIC, LMIC and upper middle-income country (UMIC)), number of total authors and having any study funding and the dependent outcomes of (1) first author from the study country and (2) last author from the study country in single-country studies. Independent variables were selected based on prior literature review of factors that may influence authorship positions.2 4 19 The number of total authors was categorised using the <25th percentile (1-5 authors), 25th-75th percentile (6-10 authors), and >75th percentile (11 or more authors). As a sensitivity analysis, the variable of having any funding support from the study country was analysed in the regression model instead of the variable for any funding support. Magnitudes of effect were reported as adjusted ORs and their respective 95% CIs. Additionally, authorship positions by World Bank income classification of the study country, study design and GEMLR category were evaluated in subanalysis for single-country studies. STATA V.16 (Stata Corp; College Station) was used for all analyses.
Patient and public involvement
Neither patients nor the public were involved in the design, conduct or dissemination of this bibliometric analysis.
Results
Summary of included articles
Of the 2137 full-text articles in the 2016–2020 GEMLR data sets, 1751 (81.9%) original research articles met inclusion criteria. Using World Bank classifications of the study countries, 394 (22.5%) were conducted in LICs, 394 (45.5%) in lower MICs, 414 (23.6%) in upper MICs and 147 (8.4%) in multiple income categories. By WHO region, 857 (48.9%) studies were conducted in sub-Saharan Africa, 364 (20.8%) in South-East Asia and 291 (16.6%) in the Eastern Mediterranean as shown in table 1 (multiple WHO regions possible for multicountry studies; therefore, proportions do not sum to 100%). Most studies (n=1575, 90%) were single-country studies, while 140 (8%) had two to nine study countries, and 36 (2.1%) had 10 or more study countries.
Descriptive characteristics of included articles
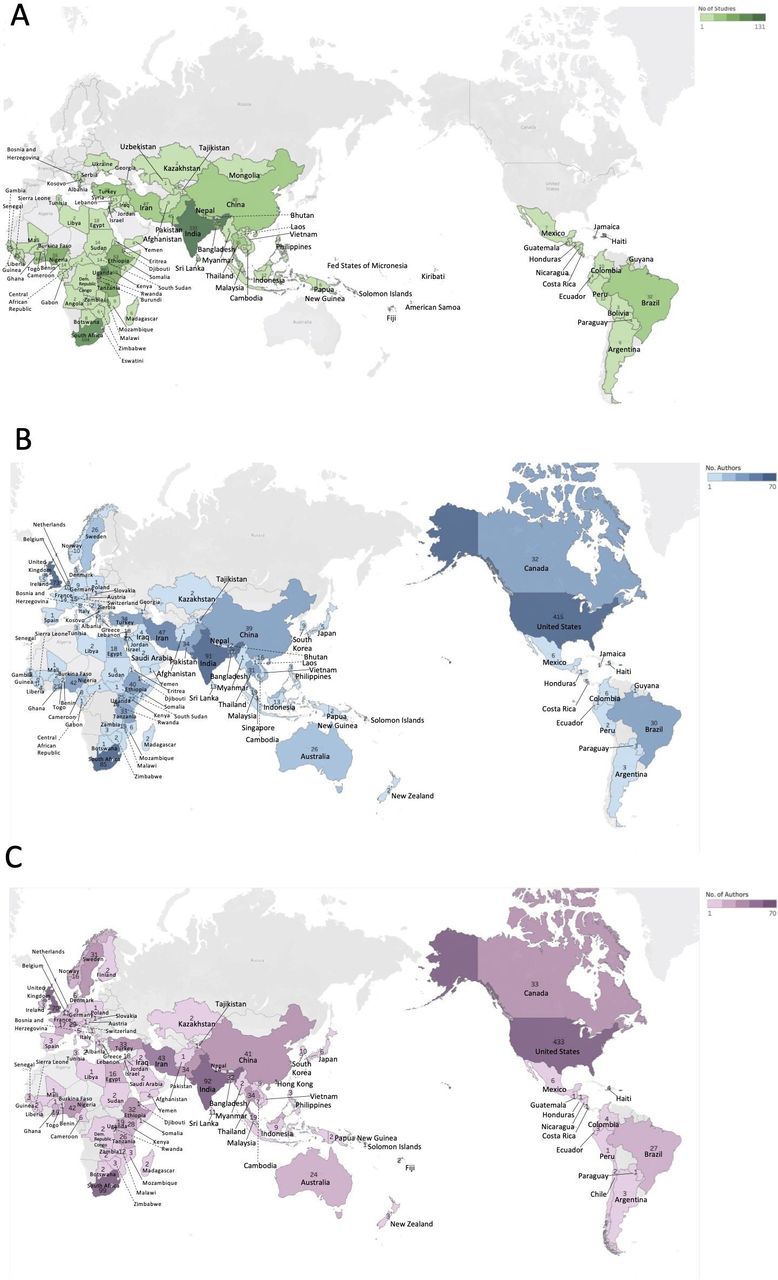
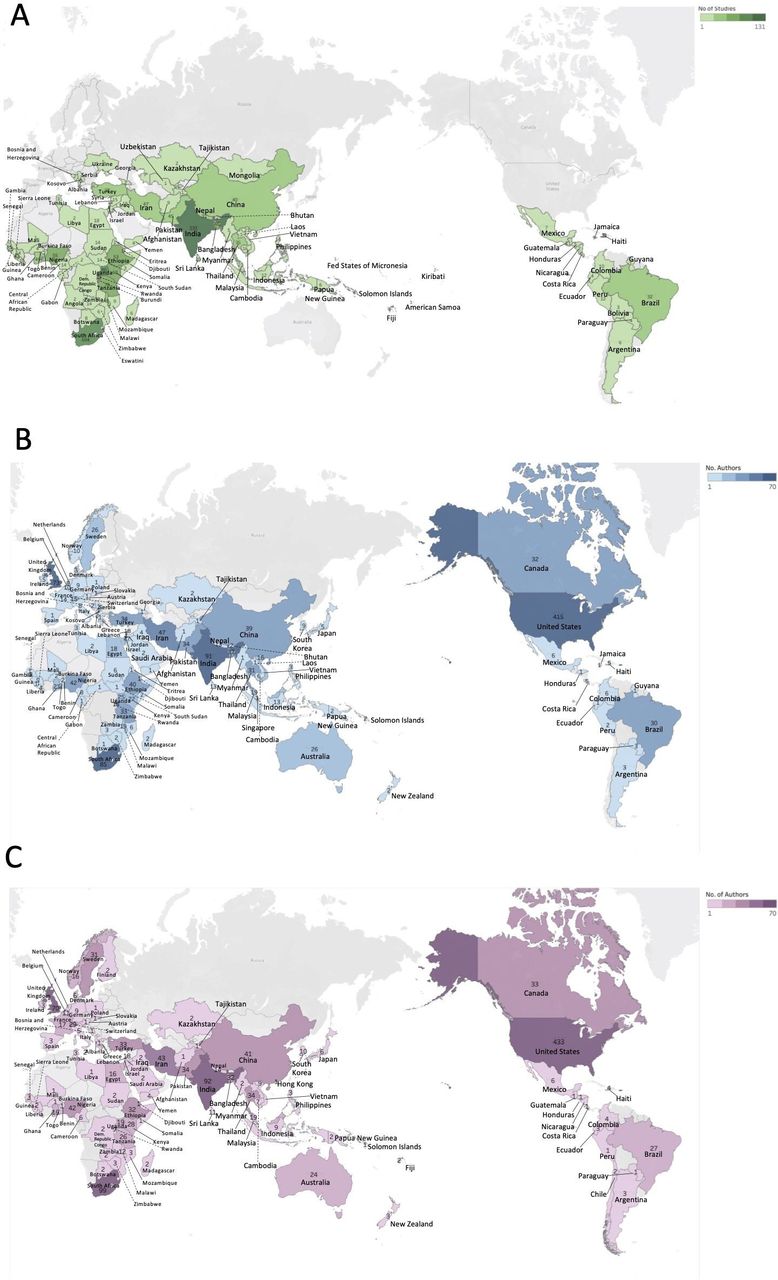
By GEMLR category, 1208 articles (69%) were ECRLS, 264 (15.9%) were DHR and 279 (15.1%) were EMD. The most common study topics were trauma (n=383, 21.9%), infectious diseases (n=477, 27.2%) and prehospital care/EMS (n=133, 7.6%). Regarding study designs, 419 (23.9%) were cross-sectional studies, 318 (18.2%) were prospective cohort studies, 301 (17.2%) were retrospective cohort studies and 86 (4.9%) were RCTs. Only 56 articles (3.2%) had an abstract or full text published in a language other than English. Approximately half (n=930, 53.1%) of all included articles reported funding support; of the 822 funded single-country studies, 28.5% (n=234) included funding from the study country. Further characteristics of the included articles are shown in table 1. Figure 1A shows a map of the distribution of study countries among single-country studies; study country frequencies are also listed in online supplemental table S6.
Supplemental material
{kind=link}
(A) Map showing distribution of study countries among single-country studies. (B) Map of the first-listed country of affiliation of all first authors. (C) Map of the first-listed country of affiliation of all last authors.
Summary of authors
A total of 14 111 authors were included in the articles included in our analysis. There was a median of 7 (IQR 5–10) authors per article. Of all authors, authors affiliated with HICs were the most common (n=5749, 40.7%), followed by authors affiliated with lower MICs (n=3731, 26.4%), upper MICs (n=2460, 17.4%) and LICs (n=1452, 10.3%); 721 authors (5.1%) had mixed affiliations (table 2). Among the authors with mixed affiliations, 691 (95.8%) had a HIC/LMIC affiliation, while 30 (4.2%) had mixed LMIC affiliations (ie, combination of LIC, lower MIC and/or upper MIC). First, second and last author positions were most commonly held by authors affiliated with HICs compared with those from LMICs (p<0.001). First, second and last authorship was lowest among authors affiliated with LICs (table 2). The most represented countries of affiliation were the USA and UK for authors with HIC affiliations, South Africa and China for authors with upper MIC affiliations, India and Bangladesh for authors with lower MIC affiliations and Uganda and Ethiopia for authors with LIC affiliation (online supplemental table S1). Figure 1B,C shows a map of the countries of affiliation of all first and last authors, respectively.
Country(s) of authors’ affiliation(s) using World Bank country income classifications for all authors, first, second and last authors
Single-country studies
Among the 1575 single-country studies, the proportion of local authors (ie, affiliated with the study country only) was greater with higher study country income categories (table 3). Of single-country studies conducted in LICs, out of 3325 authors, 1246 (37.5%) were affiliated with the study country, and 1737 (52.2%) were affiliated with HICs. However, among those conducted in lower MICs, out of 5740 authors listed, 3270 (57%) were affiliated with the study country, and 2050 (35.7%) were affiliated with HICs. Among studies conducted in upper MICs, of 2804 authors listed, 1954 (70%) were affiliated with the study country, and 681 (24.3%) were affiliated with HICs (table 3). The proportion of local authors in first and last author positions was lower than the overall proportion of local authors for all study country income categories (table 3). Local first and last authorship was lowest among studies in LICs, with only 118 (31%) first authors and 81 (21.3%) last authors affiliated with the study country, compared with 400 (50.8%) of first authors and 338 (43%) of last authors in studies in lower MICs and 276 (67.8%) of first authors and 260 (63.9%) of last authors in studies in upper MICs (table 3).
Authorship affiliation as from study country only, high-income country (HIC) or other, by study country World Bank income classification (single country studies only)
Articles having exclusively local authors comprised 29.3% (n=462) of the single-country studies. The proportion of studies with exclusively local authors increased with higher country income classes; only 34 (8.9%) studies conducted in LICs had exclusively local authorship bylines, compared with 227 (28.8%) studies conducted in lower MICs and 201 (49.4%) studies conducted in upper MICs.
Studies without local author representation
A total of 210 (12.2%) articles with less than 10 study countries did not include at least one local author from each study country. Among single-country studies, 8.7% did not include any local authors (online supplemental table S2). Studies which did not include local authors were most common among studies conducted in LICs (14.4%) and were less common with higher country income categories (8.3% in lower MIC studies and 4.2% in upper MIC studies) (online supplemental table S2). Among all multicountry studies, 103 (57.5%) did not include at least one local author from each study country. When specifically looking at the 38 multicountry studies with 10 or more study countries included, only four (10.5%) included at least one author from each study country.
Regression analyses
In multivariable regression analyses (table 4) evaluating the association of having a local first author with the independent variables, studies conducted in an LMIC or UMIC versus those in LIC had greater odds of having a local first author (aOR 3.81, 95% CI 2.61 to 5.58 UMIC vs LIC). Having any funding support (aOR 2.16, 95% CI 1.70 to 2.73) was also associated with greater odds of local first authorship. Studies with more authors (aOR 0.50, 95% CI 1.70 to 2.73 for 11 or more authors vs 1–5 authors) and those in the EMD and DHR versus ECRLS category (aOR 0.15, 95% CI 0.10 to 0.22 DHR vs ECRLS) had lower odds of having a local first author. Similar associations were found in multivariable regression for the outcome of having a local last author (table 4). Studies conducted in an LMIC or UMIC (vs LIC), as well as studies that had funding support (aOR 2.00, 95% CI 1.58 to 2.53), had greater odds of local last authorship (aOR 6.19, 95% CI 4.19 to 9.14 UMIC vs LIC). There was no significant association of world region with first or last authorship except for Americas region (vs EUR), which had lower odds of local first (aOR 0.30, 95% CI 0.13 to 0.71) or last authorship (aOR 0.43, 95% CI 0.21 to 0.92). In sensitivity analysis, substituting the variable of local funding (ie, funding from a source located in the study country) for the funding variable, the magnitude of association was greater, with articles reporting funding from the study country having greater odds of having a first (aOR 2.87, 95% CI 2.01 to 4.10) and last author (aOR 3.15, 95% CI 2.25 to 4.41) as shown in online supplemental table S3.
Multivariable regression for outcomes of local first and last authors (affiliated only with the study country) among single-country studies
Authorship by study design and GEMLR category
In subanalysis, when evaluating authorship by study design, among first authors, those affiliated with LICs were least common among RCTs (n=3, 3.5%), compared with prospective cohort studies (n=20, 6.3%) and other study designs (n=93, 6.9%). Similarly, last authors affiliated with LICs were less common among RCTs (n=1, 1.2%) than prospective cohort studies (n=13, 4.1%) and other study designs (n=69, 5.3%). First, second and last authors with mixed affiliations were more common in RCTs than in prospective cohorts or other study designs as shown in online supplemental table S4. When evaluating authorship by GEMLR category, first authors affiliated with HICs were more common in articles categorised as DHR (n=186, 66%) than articles categorised as EMD (n=146, 55.3%) and ECRLS (n=436, 36.1%), while first authors affiliated with LICs were least common in the DHR category (n=7, 2.5%) and most common the ECRLS category (n=98, 8.1%). Similar patterns were seen in second and last author positions as shown in online supplemental table S5.
Discussion
This bibliometric analysis is the first to assess authorship representation within the relatively new field of GEM. Our study highlights disparities in authorship representation between HIC and LMIC authors, similar to previous observations seen in bibliometric studies of other global health fields.2 3 5 Authors affiliated with HICs were the most represented, while those affiliated with LMICs, particularly LICs, were the least represented, despite all articles reporting work conducted in LMICs. Additionally, the proportion of studies with exclusively local authors (those affiliated with the study country only), which may be interpreted as an indirect measure of the amount of locally owned research, decreased with lower study country income levels. More troubling findings from this analysis were that more than 1 in 10 articles had no local author representation, and more than half of multicountry studies did not include at least one local author from each study country.
Our findings that HIC authors were the most represented in all key authorship positions (first, second and last authors) are consistent with recent publications examining authorship in other global health fields. In a 2019 study evaluating collaborative health research conducted in sub-Saharan African countries, inclusion of collaborators from the Global North (USA, Canada, Europe) was associated with a decreased percentage of first author positions belonging to Global South institutions.2 Similarly, a recent study in the global surgery field found that most authors were men, affiliated only with HICs, and held senior positions.5 In our analysis, LMIC-affiliated authors were most commonly in middle authorship positions; these positions have been considered less valuable or tokenistic as a means of improving the perceived diversity of the authorship group.2 Our findings contribute to the growing evidence base, which demonstrates pervasive inequity in research relationships and how authors affiliated with LMIC institutions are represented across subspecialties of global health, including newer fields such as GEM.
Notably, our analysis found evidence that the power dynamics that underlie authorship inequity may be most influenced by financial factors in several respects. First, we found that higher study country income levels were associated with greater odds of having local first or last authors, and that local first and last authors were least common in studies conducted in LICs. The differences in local authorship were also particularly striking between studies conducted in upper MICs versus in LICs, with only 8.9% of studies in LICs having exclusively local authors versus 49.4% of upper MIC studies. Additionally, studies that did not include any local authors were most common in studies conducted in LICs compared with those conducted in lower MICs and upper MICs. Studies of this nature have been referred to in the literature as ‘parasitic’ to reflect the major power imbalances and dispossession of data ownership from LMIC study participants and researchers by HIC researchers and are a highly concerning finding.4 In response, some journals have opted to not publish articles that do not include an author from the study country, although these requirements are not yet the norm.20 21 Second, in regression analysis, we found that having any funding from the study country was associated with greater odds of local first or last authorship. Prior research in the global maternal health literature has similarly shown that local lead authorship was more common among articles that reported funding from national NGOs or governments compared with those that reported funding from HIC–LMIC collaborative agencies (ie, bilateral and HIC research agencies), while HIC authors dominated articles with funding reported from the US Agency for International Development, the US National Institutes of Health, and the European Union.21 Local funders, such as national research agencies, NGOs and academic institutions, may also be more likely to invest in the career development and research capacity of domestic rather than foreign researchers, contributing to greater local research leadership and ownership, and concomitant lead authorship positions. These findings suggest that local control of financial resources for research are key drivers in authorship decision-making.
The fact that the global health field remains heavily dominated by HIC funders and much of global health funding is granted to researchers from HICs has recently been called to greater attention.22 23 This power imbalance is illustrated by HIC institutions and researchers often setting the agenda and making funding allocation decisions without consideration for LMIC partner priorities.8 24–26 This often perpetuates LMIC researcher dependence on HIC counterparts for research opportunities and funding.24 As GEM projects are often funded by HIC institutions, efforts to decolonise the GEM field and restore power to local researchers with respect to funding decisions and priority-setting are needed to increase equity. Increasing the funding opportunities specifically for LMICs researchers may play a large role in recognising the expertise of LMIC researchers and allowing professional growth beyond the role of data collector and collaborator into one of setting the agenda, designing the research and disseminating results.24 27–29 We also found that over-representation of HIC authors was more pronounced in multicounty studies, with less than half of the studies including at least one author from each study country. Potential explanations for this finding are the amount of funding needed for larger multicountry studies may be more likely to come from large HIC funding sources, the more complex and potentially hierarchical power dynamics involved in large international collaborations or that the resources needed for larger studies such as research administration and support tend to be in HICs.
Our regression analysis also sheds light on which factors have the greatest influence on authorship decisions. Our finding that larger authorship groups were associated with lower odds of local first and last authorship may indicate that equitable authorship discussions may be more challenging in larger collaborative groups, or simply that larger research groups require greater funding, which are often obtained from HIC sources. Additionally, prior research on authorship ‘parasitism’ in research conducted in sub-Saharan Africa has found that studies without any local authorship were less likely among articles with >10 authors.3 Together, these findings may be explained by larger authorship groups being more likely to include LMIC authors in token middle authorship positions to ensure formal or informal expectations for local author inclusion are met. Additionally, certain subfields within GEM, such as disaster and humanitarian response appear to have even greater inequities; further research is needed to understand how research within crisis settings may differ from general GEM research, and how long-standing colonial structures in the humanitarian sector may influence authorship decisions.30
Existing guidelines which aim to standardise criteria for academic authorship have been established by the International Committee of Medical Journal Editors (ICMJE) and reflect the degree of author contributions to research conceptualisation, analysis and study ownership.11 More recent efforts aim to repurpose ICMJE guidelines in a way that promotes equitable authorship, particularly within international collaborations.31 32 This includes placing a critical eye to where authorship guidelines have been unable to capture the value of a collaborators lived expert knowledge, which often plays a key role in the knowledge coproduction for publication, yet these voices are not often named as a coauthor.32 Additionally, calls for journal editors to require authorship reflexivity statements in international collaborative research are a step towards more equitable authorship practices.8 Such efforts highlight the need for technical sharing in areas that commonly exclude or minimise the contributions of LMIC authors per ICMJE guidelines—particularly in data analysis and manuscript preparation where local authors are often not writing in their native language for publication.31 However, the impact of these efforts has yet to be determined.
The causes behind the relative paucity of LMIC authorship representation seen in this study are likely multifactorial. First, EM as a formal medical specialty is one of the newest disciplines in medicine, being recognised as a specialty in the USA and Canada in 1979, the UK and Australia in 1993.33–35 LMICs have had shorter experience with the formalised specialty with the Philippines being one of the first to recognise the specialty in 1991, and South Africa the first in sub-Saharan Africa to have an EM specialty training programme since 2003.36 However, the specialty does not exist in many countries today, particularly in lower income countries. Given EM’s roots in HICs, this historical background of the specialty can explain some of the discrepancies in authorship in our analysis.33 37 Academics from HICs have often been supporters for the introduction of EM as a specialty in other countries, leading to previously established mentor/mentee relationships. Research relationships likely mirror the clinical teaching relationship (ie, senior authors on papers often may be the faculty that taught EM during early years of EM specialty development).38–40 However, this historical mentor/mentee relationship can hinder continued growth of LMIC colleagues if they are not allowed to move beyond the role of local partner into higher academic, research and leadership roles.41 Additionally, the resources available to conduct research, such as organised research governing bodies and ethical review boards, are often lacking, coupled with reduced or prohibitively expensive research training opportunities for LMIC scholars.42 ,43 44 This is further compounded by the shortage of human resource for health in LMICs, usually resulting in early career specialists in LMICs having a multitude of competing priorities such as heavy clinical workloads, internal quality improvement projects and the education of trainees.45 The movement of qualified medical personnel including researchers from LMICs to HICs or ‘brain drain’ exacerbates this situation.46 While reasons for this migration include better working conditions and increased income opportunities, studies have estimated that LMICs suffer an approximately US$16 billion loss each year as a result of physician brain drain.46
Building technical exchanges and development of research in LMICs have been made a priority by the Global Forum for Health Research to help correct the 10/90 gap in health research.47–49 To meet this need, research fellowship and scholarships for LMIC researchers have been developed in recent years, but lack of consistent funding from HIC partners can hinder these initiatives.50 51 Overcoming journal paywalls can also present an additional academic hurdle for LMIC researchers and the dominance of English-language publications, which is often not the mother tongue or primary language of LMIC researchers, creates major challenges together with lack of access to reliable, high-speed internet connections.44 This may result in researchers from LMIC needing to depend on HIC partners in order to increase the chance of publication.
As GEM and other newer subspecialties expand globally, it is critical that assessments of equity occur early and often as these fields develop and mature. Recognition of the extent of authorship inequities is only the first step in the process of creating an equitable field of GEM. However, further evaluation into the root causes of inequitable research partnerships between HIC and LMIC in GEM research is needed to begin to address systemic academic power structures at odds with equity, so that we can implement possible solutions. Increasing multidirectional research fellowship and mentorship programmes that cater to LMIC-based researchers and scholars and reimagining funding sources can reduce some of these disparities. Closing this gap also includes revisiting and further reducing open-access article-processing fees and paywalls for journals publishing studies from LMICs, and investing in research infrastructure such as the development of ethical review boards.52 53 Fianally, inequities in academic engagement and advancement opportunities are not limited to authorship representation alone. The global health research landscape is influenced by its colonial origins and with it has created power dynamics that support HIC researchers without advancing LMIC counterparts.8 25 28 As the specialty of EM spreads and GEM research partnerships continue to develop, the field must work towards equitable research collaborations and authorship parity.
Limitations
This study has several limitations. First, this analysis only evaluated original research articles from the annual GEMLR. Although GEMLR disseminates high-quality research from GEM, there may be some subjectivity to the article selection process that cannot be accounted for in this analysis. A majority of the articles in this analysis were also published in the English language, which may have excluded LMIC research published in local or national country journals in local languages. This was largely due to the primary languages of review for GEMLR being English, Spanish and additional languages depending on the language capacities in each year’s review group. Furthermore, in this analysis, authors’ country affiliation was determined based on their listed institutional location, which may not be a true reflection of the author’s actual country of origin. However, institutional affiliation is one of the few indicators that can be used to begin to investigate equity in academic partnerships, and prior studies suggest there is substantial correlation between listed affiliations and place of birth.8 26 54
The specialty of GEM does not carry the same historical or academic footprint as other specialties. The specialty is a multidisciplinary field where injury, prehospital care, communicable and non-communicable disease as well as humanitarian crises, global security and disaster medicine often meet. Despite this increased breadth, there are few journals dedicated to emergency medicine, and many international studies related to GEM may not have been captured in our study. Finally, our analysis does not allow us to explicitly extrapolate how authorship representation truly affects equity and vice versa. Additionally, an author’s institutional affiliation may not be able to fully capture other complex and intersectional dynamics such as positionality, gender, race, and identity.8 Furthermore, influences on achieving equity in global health are multifactorial in nature and many pieces of the academic process and structure remain biased to HIC researchers. There is significant work ahead that must be done to continue to identify and dismantle systems at odds with equity.
Conclusion
This analysis found significant disparities in authorship representation. Authors affiliated with HICs more commonly occupied the most prominent authorship positions. Recognising and addressing the underlying power dynamics and imbalances contributing to inequitable authorship in international, collaborative EM research is warranted. Innovative methods to increase funding and scholarship opportunities to support EM researchers in LMICs are greatly needed to address these disparities, particularly in LICs.
Data availability statement
Data are available upon reasonable request. Data are available for free on reasonable request from the corresponding author.
Ethics statements
Patient consent for publication
Acknowledgments
We thank the Global Emergency Medicine Literature Review (GEMLR) group and the Society of Academic Emergency Medicine Decolonizing Global Emergency Medicine Working Group for its support of this research.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
SCG and GH are joint first authors.
Handling editor Seye Abimbola
Twitter @sgarbern
Contributors Author contributions are detailed in the authors reflexivity statement in online supplemental file S9. SCG and CR are responsible for the overall content as guarantors. All authors approved the version of the manuscript to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.