Article Text

Abstract
Introduction Despite growing scholarship on the social determinants of health (SDoH), wider action remains in its early stages. Broad public understanding of SDoH can help catalyse such action. This paper aimed to document public perception of what matters for health from countries with broad geographic, cultural, linguistic, population composition, language and income level variation.
Methods We conducted an online survey in Brazil, China, Germany, Egypt, India, Indonesia, Nigeria and the USA to assess rankings of what respondents thought matters for health and what they perceived decision makers think matters for health. We analysed the percentages of each determinant rated as the most important for good health using two metrics: the top selection and a composite of the top three selections. We used two-tailed χ2 test for significance testing between groups.
Results Of 8753 respondents, 56.2% (95% CI 55.1% to 57.2%) ranked healthcare as the most important determinant of good health using the composite metric. This ranking was consistent across countries except in China where it appeared second. While genetics was cited as the most important determinant by 22.3% (95% CI 21.5% to 23.2%) of the overall sample with comparable rates in most countries, the percentage increased to 33.3% (95% CI 30.5% to 36.3%) in Germany and 35.9% (95% CI 33.0% to 38.8%) in the USA. Politics was the determinant with the greatest absolute difference (18.5%, 95% CI 17.3% to 19.6%) between what respondents considered matters for health versus what they perceived decision makers think matters for health.
Conclusion The majority of people consider healthcare the most important determinant of health, well above other social determinants. This highlights the need for more investment in communication efforts around the importance of SDoH.
- health policy
- public health
- health policies and all other topics
Data availability statement
Data are available on reasonable request. Data are available on reasonable request
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Health is largely determined by social and economic forces beyond the healthcare system, often referred to as the social determinants of health (SDoH). There is now growing scholarship on—and recognition by governments of—the foundational role SDoH play in shaping individual and population health. However, wider action on SDoH remains in its early stages.
Implementing successful policies around SDoH relies on many levers, including broad public knowledge and support. Yet, research assessing public knowledge of SDoH is scarce.
WHAT THIS STUDY ADDS
The majority of respondents in Brazil, Germany, Egypt, India, Indonesia, Nigeria and the USA considered healthcare the most important determinant of health. Healthcare was ranked a close second, after education, in China.
Respondents in Germany and USA ranked genetics as a determinant of health in higher frequency than respondents in Brazil, China, Egypt, India, Indonesia and Nigeria.
Respondents rarely selected politics as a determinant that matters for their health, but they viewed it as a determinant that decision makers considered matters for health. This lack of linkage of politics and health outcomes showcases that people’s views of what determines health are often skewed towards downstream rather than upstream forces.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
There is need for more investment in communication efforts to the public around the importance of SDoH in our efforts to improve the health of populations.
More research is needed to better understand how public perceptions are associated with policy implementation, how perceptions change over time and how they are linked to changes in health indicators.
Introduction
In the last quarter of the 20th century, a persuasive body of scholarship began to shift the conversation about determinants of health, highlighting the importance of forces beyond individual attributes and healthcare as foundational causes of health. Earlier efforts included the introduction of multiple frameworks that highlighted the connections between the individual, the various external layers of influences around them and health.1–3 There is now a growing understanding of, and scholarship on, the role that social and economic factors play in shaping both individual and population heath.4–9 These factors are often collectively termed the social determinants of health (SDoH). The academic embrace of SDoH has been accompanied by increasing recognition by governments and commercial entities of the drivers of people’s health beyond medical care.10–13 A number of initiatives, such as Health in All Policies, have been proposed as potential pathways to translate scholarship to action on SDoH. Yet, wider policy and political action on SDoH remains in its early stages.14–19
Designing and implementing successful policies and programmes on any issue relies on the alignment of multiple levers. One of these levers is political will and broad public support. Public support to enact interventions to improve population health beyond the healthcare sector is contingent on understanding SDoH as foundational causes of health, which can help catalyse action on SDoH. It can also help establish a culture of accountability for political decisions that concern the allocation of resources that affect health .20 However, efforts expended to ensure that the general public understands the role of social and economic factors in shaping health are scarce. This is exemplified in a review of the literature on SDoH, which found that the majority of SDoH scholarship targets policymakers and academics as recipients of research findings.21
Building broad public understanding and support around SDoH can be achieved through educational and advocacy efforts. For such efforts to succeed, there is a need to first measure the level of public views about what shapes health. Yet, research assessing public knowledge of SDoH is scarce, and existing data are largely from high-income countries (HICs).
This paper aimed to help tackle this gap in the literature and document public perception of what matters for health in eight countries, including low-income and middle-income countries (LMICs) that are often excluded from discussions of how SDoH shape population health. Furthermore, we assessed what the public thinks matters for decision makers to better understand the gap, if any, between what the public thinks matters to them compared with what they perceive matters to those with the ability to act, including decision makers at all levels.
Methods
This analysis used data collected through a multicountry, anonymous, opt-in, cross-sectional online survey in eight countries between 16 September and 1 November 2020. Data were collected through RIWI, a professional global survey platform that uses a patented Random Domain Intercept Technology (RDIT).22 RDIT platform has been used extensively by many international agencies including the United Nations World Food Program and World Bank to conduct global surveys.23 The tool is compatible with many web-enabled devices including computers, mobiles and tablets and has captured more than 1.6 billion survey responses since its launch in 2009, covering more than 100 million people in every country and territory. A survey administered through RDIT cannot be blocked by state surveillance or internet control, nor is it susceptible to ad-block technologies as it leverages real registered domains (not pop-ups or ad interstitials).24
Study population and sample size
The target population for this analysis was all web users who directly typed into the URL bar to browse the internet in Brazil, China, Germany, Egypt, India, Indonesia, Nigeria and the USA. These countries were selected to provide a wide range of geographic, cultural, linguistic, population composition and gross domestic product categories variation. The target sample size was a minimum of 1000 responses from each of the eight countries. Users who made errors while typing in addresses of websites or those who inadvertently navigated to a domain or subdomain while typing websites addresses landed in one of the thousands of URLs owned or controlled by RIWI. Using a series of algorithms, a random sample of these users then received an invitation to participate in this survey. Each respondent who opted-in received the survey in the language used by the majority of people in their country (eg, Portuguese in Brazil and Arabic in Egypt) and was allowed to respond to the survey only once based on their IP address. The technology then adopted various filters to prevent non-human respondents or ‘bots’ from responding. None of the respondents were paid or provided with any incentive. The platform also applied an algorithm to exclude paid panel respondents.
We did not collect any identifiable information other than age and gender of respondents. The respondents had the option to opt out of answering one or more questions or quit the survey at any time. The data were saved in a server maintained by RIWI.
Demographic variables
The sociodemographic characteristics collected from respondents included country, gender, age, area of residence, education level and income. Educational level was categorised into no formal schooling, some primary school, completed primary school, some secondary or high school, completed secondary or high school, completed college or university, and completed a graduate school degree. Area of residence was categorised as living in a large city, suburb, small town or village and rural area farm.
Income was categorised into five groups: poor, low income, middle income, high income and rich based on the income levels of each country and the self-reported monthly household incomes in respective local currencies (online supplemental appendix table 1).
Supplemental material
Determinants of health variables
Respondents were asked to select what they thought were important determinants of good health from the following list: culture, employment and work conditions, early life or childhood conditions, income and family wealth, genetics, built environment (eg, housing or neighbourhood conditions), education, social support, healthcare and politics. The list of SDoH included in the survey is mainly derived from existing literature and frameworks that highlight important determinants of health.25–28 The question was then repeated twice with the remaining items on the list to yield a participant’s top three choices for important determinants of good health.
Respondents were also asked about their perceptions of what decision makers—whose work affects their daily lives—think is most important for good health using the same list of determinants. Examples of relevant decision makers provided in the survey included mayors, council members, representatives, governors, ministers and presidents. The question was then repeated twice with the remaining items on the list to yield respondents’ perceived second and third choices of important determinant of good health for decision makers.
Statistical analysis
First, we summarised the frequencies and unweighted percentages of the demographic characteristics of the overall study sample and by country. Second, we calculated two metrics that indicated the percentage of the sample for which a determinant was: (1) what respondents considered as important determinants of health and (2) what respondents considered decision makers think of as important determinants of good health. We conducted a descriptive analysis calculating the percentages and 95% CIs of respondents who cited each determinant either as their first choice or a composite of the first, second or third choice for important health determinant. We repeated the analysis with respondents’ perception of what decision makers think about determinants of health. Third, we calculated the absolute and relative differences between what respondents considered important compared with their perceptions of what decision makers considered important. We used a two-tailed χ2 test for significance testing between groups, and a p value <0.05 was considered statistically significant throughout the analysis.
The data were cleaned and analysed using R software (V.4.1.2). We used R packages ‘tidyverse’, ‘data.table’, ‘epiR’ and ‘gtsummary’ for analysis. We followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guideline for cross-sectional studies when designing and reporting on this analysis.
Patient and public involvement
Patients and the public were not involved in developing the research question, design or implementation of this analysis. This is primarily because we did not have funding to support such involvement, and our analysis was on a global level.
Results
Sample characteristics
Table 1 presents the demographic characteristics of the study sample. A total of 37 566 people saw the survey and 8753 unique users answered the full survey, giving a full response rate of 23.3%. The remainder of the respondents either chose to hit ‘skip’ or closed their web browsers before completing and submitting the survey. The number of completed responses was comparable among countries. Nigeria (n=1014, 17.1% response rate) and China (n=1282, 30.3% response rate) had the fewest and most absolute number of completed responses, respectively. More men (68.2%) answered than women (31.8%). The narrowest gap in response by gender was in the USA (54.6% vs 45.4%), and the widest gap was in China (81.4% vs 18.6%). Younger age groups constituted higher percentages of respondents, with those between the ages of 18 and 24 years constituting the highest percentage (35%) in the overall sample. The age distributions of respondents varied by country. The USA and Germany had the lowest percentage of 18–24 years respondents (19.2% each) and Nigeria (46.9%) had the highest. The USA had the highest percentage of respondents 65 years and older (17.0%) and Nigeria had the lowest (1.3%).
Demographic characteristics of the study sample*
A substantial percentage (42.1%) of respondents lived in large cities, while only 13.0% lived in rural areas in the overall sample. The proportion of those living in large cities ranged from 53.5% in Brazil to 29.2% in Germany. Income level was more evenly distributed in the sample than other demographic factors. The country with the widest gap between the poorest (32.5%) and richest (9.6%) groups was Nigeria, and the country with the narrowest gap (25.1% vs 28.3%) was the USA. More respondents with at least a college degree completed the survey (42.2%) with the highest percentage in China (59.7%) and lowest in Brazil (24.3%).
Perceptions about important determinants of good health
Overall, respondents selected healthcare as the most important determinant of good health when using the composite metric (56.2%, 95% CI 55.1% to 57.2%). This remained consistent among respondents in each country, except for China, where healthcare appeared second (39.2%, 95% CI 36.6% to 42.0%). Brazil (69.4%, 95% CI 66.5% to 72.1%) and Nigeria (69.7%, 95% CI 66.8% to 72.5%) had the highest percentage of respondents citing healthcare among the top three important determinants.
Education ranked second in the overall sample (47.9%, 95% CI 46.9% to 49.0%) and in all countries, except in China where it ranked first (41.7%, 95% CI 39.0% to 44.4%). Education tied with healthcare for first place in India (56.2%, 95% CI 53.3% to 59.0%). Built environment (32.7%, 95% CI 31.7% to 33.7%) ranked third in the overall sample. Conversely, politics was the determinant selected least often, both in the overall sample (10.9%, 95% CI 10.2% to 11.6%) and across countries. The remainder of determinants were selected among the top three important determinants by 20%–30% of the overall sample (figure 1).

Rankings of what respondents think matters for good health stratified by country.* *A composite of the first, second or third choice for important health determinants for good health.
Some countries’ ranking of specific determinants differed substantially from both the overall sample and other countries. Germany and China were the only countries in which fewer than half of the respondents chose healthcare as the most important determinant of good health using the composite metric with 48.3% (95% CI 45.2% to 51.4%) and 39.2% (95% CI 36.6% to 42.0%), respectively. While genetics was selected by 22.3% (95% CI 21.5% to 23.2%) of the overall sample with comparable rating in most countries, the percentage rose to 33.3% (95% CI 30.5% to 36.3%) in Germany and 35.9% (95% CI 33.0% to 38.8%) in the USA. Indonesia was the only country where more than half of the respondents selected built environment (53.1%, 95% CI 50.0% to 56.2%) using the composite metric. Respondents in China (42.8%, 95% CI 40.1% to 45.6%), Nigeria (37.8%, 95% CI 34.8% to 40.9%) and India (34.9%, 95% CI 32.2% to 37.7%) selected income and wealth in the top three determinants more frequently than other countries (figure 1). Egypt was an outlier with about a third of respondents selecting culture (36.7%, 95% CI 33.8% to 39.7%) in the top three important determinants of good health compared with lower percentages in other countries (figure 1). Differences between countries were statistically significant.
The rankings of determinants did not change when we examined a single top determinant of good health. One notable change was the heightened contrast between Indonesia and other countries in the percentage of respondents selecting built environment as the most important determinant (online supplemental appendix figure 1).
Perceptions about what decision makers consider as important determinants for good health
Overall, respondents selected healthcare (41.9%, 95% CI 40.9% to 42.9%) as the most important health determinant for decision makers when using the composite metric with education (40.8%, 95% CI 39.8% to 41.9%) as a close second. Among countries, healthcare was selected as the top determinant using the composite metric in Indonesia (48.3%, 95% CI 45.2% to 51.4%), Germany (44.6%, 95% CI 41.6% to 47.7%) and the USA (45.5%, 95% CI 42.4% to 48.5%). Education was most selected as the top determinant using the composite metric in Egypt (46.5%, 95% CI 43.5% to 49.5%), Nigeria (45.0%, 95% CI 41.9% to 48.1%), India (44.9%, 95% CI 42.1% to 47.8%), Brazil (41.3%, 95% CI 38.4% to 44.3%), and China (37.6%, 95% CI 35.0% to 40.3%) . Childhood conditions (19.8%, 95% CI 19.0% to 20.7%) and genetics (18.7%, 95% CI 17.9% to 19.5%) were the least cited in the top three determinants. This applied to all countries, except for Germany and the USA (figure 2).

Rankings of respondents’ perceptions of what decision makers think matters for good health stratified by country*. *A composite of the first, second or third choice for important health determinants for good health.
Some countries’ ranking of specific determinants differed substantively from both the overall sample and other countries. Respondents in Indonesia selected built environment (42.9%, 95% CI 39.8% to 46.0%) using the composite metric in higher frequency compared with other countries and income and wealth (19.0%, 95% CI 16.7% to 21.6%) in lower frequency than other countries. Childhood conditions was selected in higher frequency in Germany (26.7%, 95% CI 24.1% to 29.6%) compared with other countries. Genetics was selected in higher frequency in Germany (25.4%, 95% CI 22.8% to 28.2%) and the USA (27.3%, 95% CI 24.7% to 30.1%) compared with other countries. Respondents in Egypt selected culture (33.1%, 95% CI 30.3% to 36.0%) in higher frequency compared with other countries. Respondents in Brazil selected politics (38.2%, 95% CI 35.3% to 41.2%) in higher frequency compared with other countries (figure 2). Differences between countries were statistically significant.
The results observed when examining the top three determinants did not change when we considered a single top determinant of good health. One notable shift was that education was cited as the single important determinant in higher frequency in Egypt compared with other countries (online supplemental appendix figure 2).
Differences between respondents’ choices and their perceptions about decision makers
There were differences between what respondents considered as important determinants of good health and what they perceived their decision makers considered as important determinants of good health. Overall, respondents ranked six determinants—healthcare, education, early life and childhood conditions, genetics, built environment, and income and wealth—as important to their good health in higher frequencies compared with decision makers. Conversely, respondents ranked four determinants— politics, social support, employment conditions and culture—as important to their good health in lower frequency compared with decision makers. Differences were statistically significant (p value <0.001) except for income and wealth (p value=0.59) (figure 3).
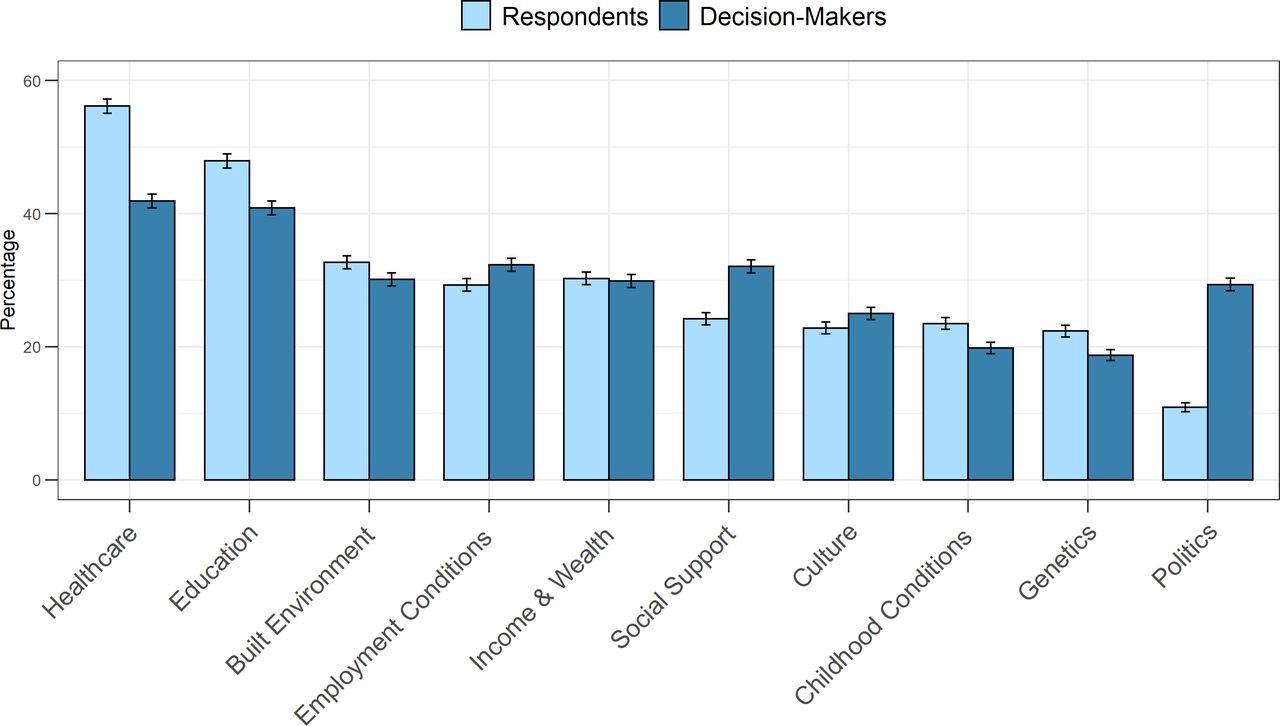
Rankings of determinants as the most important* for good health for respondents and their perceptions of what decision makers think. *A composite of the first, second or third choice for important health determinants for good health.
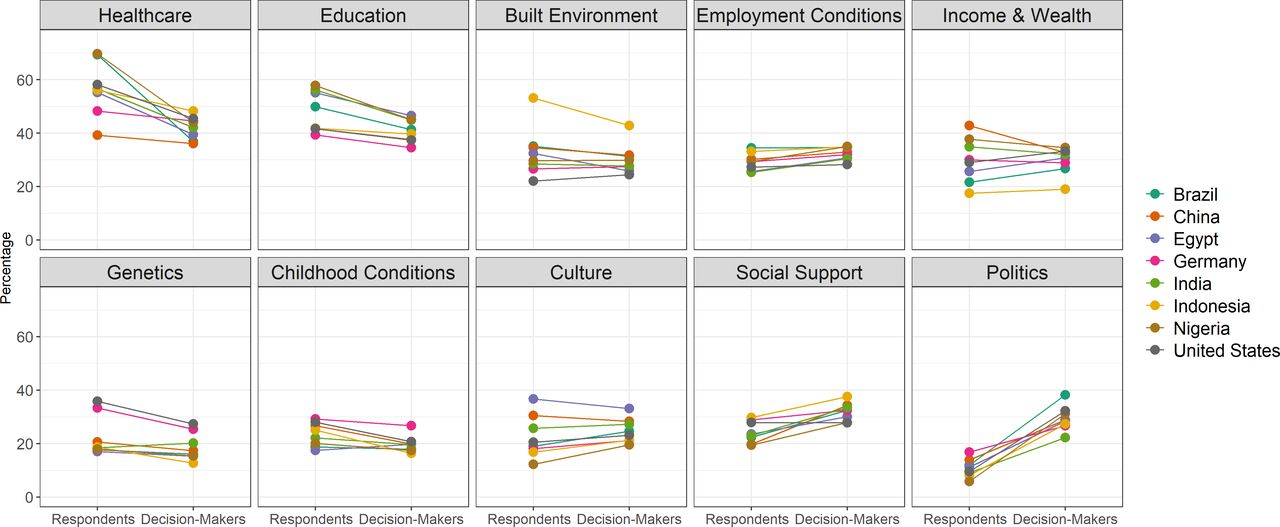
The differences within countries followed a similar pattern. The importance of healthcare and education decreased (selected in lower frequency for decision makers) in all countries with the largest absolute decrease for healthcare in Brazil (−32.6%, 95% CI −36.6% to −28.6%) and for education in Nigeria (−12.9%, 95% CI −17.2% to −8.6%). The importance of genetics decreased in all countries except India (1.8%, 95% CI −1.4% to 5.0%). The importance of politics and employment increased (selected in higher frequency for decision makers) in all countries with the largest absolute increase for politics in Brazil (26.3%, 95% CI 22.8% to 29.8%) and employment in Nigeria (5.6%, 95% CI 1.7% to 9.7%). The importance of social support increased in all countries except the USA (−0.1%, 95% CI −3.9% to 3.7%). The differences in perceptions about culture, and income and wealth increased in some countries and decreased in others (figure 4 and online supplemental appendix table 2A–H).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rankings of determinants as the most important* for good health for respondents and their perceptions of what decision makers think stratified by country. *A composite of the first, second or third choice for important health determinants for good health.
Discussion
This analysis shows that respondents across eight countries considered healthcare to be what matters the most for good health. Similarly, but to a lesser extent, respondents perceived that decision makers consider healthcare the most important determinant of good health.
This broad public perception that healthcare is what matters most for good health aligns with existing literature. A survey of adults in Wisconsin, USA, in 2009, showed that 75.3% of respondents believed health insurance was among the most important factors affecting health.29 A national survey in the USA found that the majority of adults viewed access to affordable healthcare (73%) as one of the strongest determinants of health.30 Another national poll found that while US adults did not identify a single factor as the most important cause of health problems, one of the top causes was lack of access to high-quality healthcare (42%).31 In the UK, a 2017 survey showed that participants were more likely to think that free healthcare (73%) had a ‘very large’ impact on health compared with SDoH such as education (24%).32 This indicates that the perception that healthcare is the most important factor for good health is present in countries with broad government sponsored healthcare coverage such as the UK as well as in those without such coverage, including the USA.33
Our survey also showed that perceptions about the salience of politics as a determinant of health were the opposite of perceptions about the salience of healthcare. Across the board, respondents did not select politics as a factor that mattered for their good health, but they viewed it as a factor that decision makers considered mattered for health. This lack of linkage between politics and health outcomes is consistent with the literature that shows that people’s views of what determines health are often skewed towards downstream rather than upstream factors. For example, multiple studies have shown that personal behaviour is perceived as more important than SDoH in determining health outcomes and as a solution to poor health.29–31 34 35 Conversely, a survey of 23 countries, mainly HICs, collected between 2011 and 2013 found that fewer than half (47%) of all participants agreed that poverty leads to severe health problems.35
Our findings were largely consistent across countries, with some exceptions. Notably, respondents in HICs, Germany and the USA, viewed genetics as an important determinant of good health more than respondents from other countries. This is consistent with an analysis from 29 countries that found that average income of a country was positively associated with selecting genetics as a determinant of heath.17 This suggests the need for more research on how factors such as individual and country level income and wealth, and geographic region are associated with perceptions of what is most important for good health.
There are several limitations to this analysis. First, similar to all internet-based surveys, our results are not representative of the populations within the countries we surveyed and are thus not generalisable. Excluding persons without access to the internet may have led to systematic bias in our results. However, our analysis was meant to add to the scarce literature and provide representation across a wide range of countries. Second, the drop-out rate was higher than in surveys with a financial incentive. We mitigated some of this effect through the use of various measures to maximise engagement and retain online respondents, including optimising the survey instrument for ease of participation on all device screens and bandwidths and using native languages, as well as concise language for immediate comprehension. Moreover, the response rate for our survey was comparable with other similar surveys.36 Third, there is a large gender gap in the response rate. This gap is consistent with other surveys administered using the RIWI technology and highlights a more foundational limitation to this method of collecting data.37 38 We presented unweighted data in this analysis to ensure that the gender gap in data collecting does not skew the results. Fourth, the list of determinants provided to respondents was by no means exhaustive, despite our inclusion of a list of factors that are most cited in the literature on SDoH. Future research could fruitfully consider more nuanced and detailed choices to help provide a clear understanding of public perceptions of what shapes health.
Notwithstanding these limitations, our analysis highlights the fundamental observation that the majority of persons in the general public consider healthcare the primary determinant of health, with social determinants being a secondary consideration. These results are perhaps understandable given that the majority of research on SDoH is tailored to reach policymakers or other academics. A scoping review of SDoH-related literature found that 41.7% of publications focused on policymakers, 34.3% on public health workforce and 13% on academia as the target audience.21 Improving the health of populations requires enacting policies and programmes that address SDoH and such actions will require broad public support. This highlights the need for more investment in communication efforts to the general public around the importance of SDoH. Furthermore, more research is needed to better understand how public perceptions are associated with policy implementation, how perceptions change over time and how they are linked to changes in health indicators.
Data availability statement
Data are available on reasonable request. Data are available on reasonable request
Ethics statements
Patient consent for publication
Ethics approval
Boston University’s Institutional Review Board (IRB) reviewed the research protocol and exempted it from detailed ethical review due to the anonymous nature of data (Protocol Number: H-40806).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @SalmaMHAbdalla, @fmshaffi, @ensoesie, @SandroGalea
Contributors SMA and SG designed the study. SMA, SFK and GR designed the questionnaire. SMA, MH, SFK and SBR analysed and summarised the data. SMA wrote the first draft, which was then reviewed and edited by SG. All authors contributed to the revision of the draft and agreed on the final manuscript. SMA is the guarantor of the study and had full access to the data.
Funding The research was funded by the Rockefeller Foundation-Boston University 3-D Commission (grant number 2019 HTH 024).
Disclaimer The Rockefeller Foundation had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; or the decision to submit the manuscript for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.