Article Text

Abstract
Introduction Despite the high burden of mental disorders among adolescents and the potentially lifelong consequences of these conditions, access to mental health services remains insufficient for adolescents in low-income and middle-income countries. We conducted an economic modelling study to quantify the potential costs and benefits of mental health interventions to prevent or treat anxiety, depression, bipolar disorder, and suicide among adolescents.
Methods We developed a Markov model that followed cohorts of adolescents (ages 10–19) from 36 countries to assess the impact of addressing anxiety, depression, bipolar disorder, and suicide during adolescence on health and non-health outcomes through their lives. We estimated the costs of interventions using an ingredients-based approach and modelled impacts on education and employment and the resulting economic, morbidity, and mortality benefits.
Results Implementing the selected interventions offers a return on investment of 23.6 and a cost of $102.9 per disability adjusted life year (DALY) averted over 80 years. The high return on investment and low cost per DALY averted is observed across regions and country income levels, with the highest return on investment arising from treating mild depression with group-based cognitive behavioural therapy, prevention of suicide attempts among high-risk adolescents, and universal prevention of combined anxiety and depression in low-income and lower-middle income countries.
Conclusions The high return on investment and low cost per DALY averted suggests the importance and value of addressing mental disorders among adolescents worldwide. Intervening to prevent and treat these mental disorders even only during adolescence can have lifelong health and economic benefits.
- Mental Health & Psychiatry
- Public Health
- Other study design
- Health policy
- Health economics
Data availability statement
Data are available in a public, open access repository. Code and datasets are available at https://github.com/rdstelmach/AMHIC-global.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Mental disorders are a significant cause of morbidity and mortality among adolescents, with an estimated 75% of lifetime mental disorders appearing before the age of 24.
Interventions to prevent and treat adolescent mental disorders have proven cost-effective in the short term in high income countries.
WHAT THIS STUDY ADDS
For every $1 invested in the full set of interventions, we expect $24 in health and economic benefits to be returned to the economy over the course of 80 years, with the highest return on investments (ROIs) and lowest costs per disability adjusted life year averted obtained in low-income and lower-middle income countries.
The interventions with the highest ROIs were treatment of mild depression and school-based prevention of anxiety and depression.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Interventions to prevent and treat many mental disorders among adolescents have lifelong health and economic benefits and warrant further research to determine how interventions can be tailored and successfully implemented at scale in low-income and middle-income countries.
Introduction
About 254 million adolescents and young adults in the world suffer from mental and substance abuse disorders; however, the vast majority remain undiagnosed and untreated.1 The causes of mental disorders among adolescents include multiple complex modifiable and non-modifiable risk factors. Compared with adults, adolescents face greater risks from lack of autonomy, peer pressure, explorations of sexual identity, socioeconomic problems, and use of tobacco, alcohol and other substances.2 Although the WHO provides guidance on adolescent mental health programmes, which have shown economic benefits, up to 80% of adolescents globally lack access to needed treatment.3–5 Unmet need reaches as high as 100% in many low-income and middle-income countries (LMICs).6
Unlike some non-communicable diseases caused by risks initiated in adolescence, significant health harms from mental and neurological disorders emerge early in adulthood and persist across time if left untreated.7 An estimated 50% of lifetime mental disorders emerge before the age of 14, and 75% by the age of 24.8 The health harms can include lifelong and progressively debilitating mental ill-health from disorders that frequently co-occur.9 Furthermore, mental disorders are sometimes accompanied by serious comorbidities such as cardiovascular disease and diabetes, caused in part by risk exposures such as tobacco and excess alcohol use that are initiated in adolescence.10
Beyond harming health, mental disorders in adolescence create barriers to healthy life development, such as education, employment, and the formation of stable families. As such, mental illness in adolescence can stymie an individual’s human development before they reach maturity.11 Finally, the stigma of mental illness can mean that even with diagnosis and available treatments, adolescents with mental disorders are inhibited from accessing treatment or living full lives.6
However, prior intervention studies have demonstrated the effectiveness of interventions to prevent and treat mental disorders among adolescents,12 13 and economic evaluations have demonstrated their cost-effectiveness. Chisholm et al conducted a global mental health investment case and determined that scaling up treatment for depression and anxiety in people aged 15 and older would lead to an additional 43 million extra years of healthy life and produce a net economic value of $399 billion at a cost of $147 billion between 2016 and 2030.14 A 2018 Australian study found a net savings of $90 million could be gained in the short term from investing in prevention and early treatment for depression and anxiety in all ages as well as loneliness in older adults.15 Greater investment in cost-effective and adolescent-specific interventions are needed to address the high burden of these conditions.6
Methods
Model overview
We developed an economic model to quantify the costs and potential benefits of interventions to prevent suicide and prevent or treat anxiety, depressive and bipolar disorders. Anxiety, depression and bipolar disorders constitute 88% of disability-adjusted life years (DALYs) attributed to mental illness among adolescents.16 Self harm, including suicide, was the second leading cause of death among adolescents in 2019.16 We programmed a bespoke Markov model in R (V.4.1.2) with the package heemod.17 We examine the 80-year health and economic impacts, including education and employment, of intervening on adolescents aged 10–19 years. Costs and benefits are discounted at an annual rate of 3% and expressed in 2019 US$.18
Step 1: cohort composition
The model cohort includes adolescent men and women in the 36 countries that together account for 80% of the burden of anxiety disorders, major depression, self-harm and bipolar disorder among 10–19-year-olds in terms of DALYs.19 20 We divide the cohort into groups that reflect the prevalence of acute major depressive disorder, anxiety disorders and bipolar disorder (by age, sex and country) according to the 2019 Global Burden of Disease (GBD) study. Because almost 42% of people experiencing depression also report having anxiety within the previous 12 months, our model includes separate states of anxiety, depression and both together.9 See online supplemental file 1 for more detailed discussions of the model structure and assumptions.
Supplemental material
Step 2: model structure and outcomes
The model uses the probability that adolescents will move between different health states over time. For a diagram of the health states and transition flows, see online supplemental figure A1. The incidence of each condition and probabilities of recovery and remission in the absence of interventions are drawn from peer-reviewed literature and publicly available global databases from the World Bank, the WHO, and the United Nations Population Division (table 1).
Supplemental material
Cohort parameters for epidemiological, educational and economic outcomes associated with adolescent mental disorders
We evaluate the impact of mental health on three main outcome areas: health, education and employment.
Intrinsic value of health
To value health impacts, we include impacts on morbidity and mortality. We follow established methods for estimating the intrinsic value of health. We used the disability weights from GBD 2019,16 which value each state on a continuum where 0 is perfect health and 1 is death. We also account for background morbidity—or disability due to conditions other than our conditions of interest—by country, age, as an independent variable affecting all states. We calculated the utility weight of each health state by subtracting the disability weights from 1, which results in a scale where 1 is perfect health and 0 is death. Following Lee et al, we use weighted averages by severity for the disability weights for anxiety and depression.21 We did not include asymptomatic cases. To convert these health values into 2019 US$, we multiplied each health state’s utility weight by the 2019 PPP-adjusted GDP per capita, times a multiplier of 1.0 (minimum 0.5, maximum 1.0).14 22
Educational attainment
Because mental ill-health can limit educational attainment in adolescence, we assess the impact of mental health on educational attainment. We calculated the change in probability of completing educational milestones for adolescents with each mental disorder. For each country, age, and sex group, we drew from ILOSTAT the probabilities of a person having completed a given level of education. We then determined the effect of each mental disorder on the probability of completing the educational milestones. We used a recent systematic review of the effects of these anxiety and depression on early school leaving.23 We made the conservative assumption that comorbid anxiety and depression had the same effect as depression alone, varied to a maximum of an additive effect of the two conditions in the sensitivity analysis.24
Bipolar disorder usually manifests in people older than the standard ages for secondary school, so we could not find data on its impact on secondary-school graduation rates. As a proxy of the effect of bipolar disorder on adolescent educational attainment, we drew the reduction in probability of completing a tertiary (ie, advanced) degree from a USA study of college students with bipolar disorder matched with controls on age, sex, ethnicity, and parental education levels.25
Wage returns to education
We assess the impacts of both educational attainment and health on employment and earnings.
To determine the impact of each additional year of education on expected wages, we first draw the base probability that a person with a given level of education will be employed for each country, age, and sex group from ILOSTAT.26 We assumed that no one under the age of 15 (the international standard for age of entering the labour force) would be employed. To capture the effects of educational attainment on adult wages for those who are employed, we use the method developed by Montenegro and Patrinos, which provides the expected marginal return to an additional year of education by age, sex, and education level for many countries.27 We assumed that the wage of a person with zero years of education was equal to the mean wage earned by the 10th percentile of wages (or consumption if wages were unavailable).28 We calculated the expected wage for an individual using the percentage growth formula over the person’s years of education, compounded each year.
In addition to the enduring effects on wages, our model accounts for the short-term effects of an acute episode of mental illness in both adolescence and adulthood by adjusting expected productivity among those in the workforce. Acute episodes of mental illness would include being in the state of anxiety, major depression, or the manic or depressive states of bipolar disorder.
We drew the reduction in productivity from absenteeism due to anxiety, depression, and the non-euthymia states of bipolar disorder from World Mental Health survey data.29 To calculate losses associated with presenteeism—a reduction in productivity while at work—due to depression, we used the ratio from a study of workers in eight high-income countries (HIC) and middle-income countries (MIC).30 For anxiety, we conservatively assumed no presenteeism in the base case, varied to the depression base value in sensitivity analysis.31 For bipolar disorder, systematic reviews estimate a 60% reduction in the probability of employment, but no evidence of additional losses due to presenteeism after accounting for absenteeism.32 33
For unvarying parameters across countries, see online supplemental file 2. For the actual values of parameters that vary across country, age, and sex groups, please see online supplemental file 3.
Supplemental material
Supplemental material
Step 3: interventions
With the model states and transition probabilities established, the next element of the model is the interventions, which influence the probability that an adolescent will develop or recover from a given mental disorder.
Identification of interventions
Interventions were identified from the peer-reviewed literature, international best practice guidelines (such as WHO mhGAP Intervention Guide) and consultation with mental health experts. We first conducted a systematic literature search for studies of adolescent mental health interventions that included an economic evaluation. The search strategy is detailed in online supplemental file 1. This search returned two interventions for the universal and indicated prevention of depression. However, the search did not provide any adolescent-specific intervention studies with cost information for the prevention of suicide or anxiety, or the treatment of anxiety, bipolar disorder, or major depression. We conducted additional non-systematic searches in PubMed to identify cost-effective intervention approaches published prior to 2010. The identified studies were used as the basis for each of the model interventions to identify each resource (including provider time, supplies, and medicines) required for implementation. Guidance for the use of medications among adolescents came from the mhGAP Intervention Guide and the British National Formulary for Children.3 34 The interventions included in the model include a range of approaches (table 2, online supplemental file 1).
Interventions, effect size estimates and costs by condition
Cognitive behavioural therapy (CBT) is a psychological treatment that attempts to address psychological problems by reshaping patterns of thinking and behaviour.35 Several forms of CBT are included for treatment of anxiety and indicated prevention and treatment of major depression. Our analysis includes CBT delivered individually in person, in a group in person, and individually using an internet-based communications platform such as Skype. Treatment of anxiety and mild depression also includes an internet-based guided self-help intervention, based on the principles of CBT delivered through self-guided modules.36 The interventions for the indicated prevention depression also include a step to screen adolescents and identify those with elevated symptoms, suggesting they are at high risk of developing major depression. Treatment for major depression includes individual in-person CBT and the addition of fluoxetine, an antidepression medication indicated for use among adolescents.
Family-focused treatment for adolescents is a psychological treatment that helps adolescents, their caregivers, and any siblings to understand bipolar disorder, identify triggers, and develop response plans for depressive and manic episodes.37 This treatment also includes medication as appropriate for the adolescent’s current state.
Alternate models of intervention delivery
The available evidence regarding adolescent mental health interventions comes largely from high income countries and from clinical settings, which are not likely to be scalable in LMICs with limited numbers of specialist providers. We adapted the selected interventions to LMIC settings in several ways. The mhGAP intervention guide recommends task shifting of mental healthcare to non-specialist health workers, which has proven cost-effective in LMICs.38–40 Other delivery models include providing services in places that reach adolescents, such as schools.13 41 42 Telehealth delivery of interventions have proved equally effective compared with in-person treatments in HICs and could work in LMICs, although they are not yet in widespread use.43 The requirements of social distancing under COVID-19 have accelerated implementation of virtual interventions. Due to limitations in available evidence, we assume comparable effectiveness for these alternate models of delivery.
Estimated coverage
For clinical interventions, our standard scenario assumes that 20% of adolescents with symptoms receive the clinical treatment (minimum 10%, maximum 50%). While this estimate is low relative to need, it likely represents a scale-up of services from current conditions in most countries.5 We scale the coverage of internet-based treatment so that it never exceeds the proportion of people in the country with access to the internet.44 Where multiple interventions are available for a condition, we assume that the same number of adolescents receive each available treatment. For the hospital-based intervention for suicide, we assume the intervention is provided to 20% (minimum 10%, maximum 50%) of the adolescents who receive medical attention for self-harm [41% (minimum 35%, maximum 49%) of the adolescents who commit non-lethal self-harm in each country, as defined in Refs. 16 and 35]. Finally, for school-based interventions, we assume that 20% of adolescents in school receive the intervention (minimum 10%, maximum 50%).45
Costing approach
Lacking examples of costed adolescent mental health interventions, we drew the intervention ingredients from studies conducted in HICs and adjusted for LMIC settings. We considered only direct costs to providers (including schools for school-based interventions) and transportation for providers to attend in-person interventions. For each intervention, we developed a standard list of resources and unit quantities based on the published studies, international guidelines and consultation with experts. Costs included health workers’ salaries for time to deliver the intervention and complete required training,46 teacher salaries,47 medications,48 laboratory tests,49 computer equipment,46 Internet access,50 online platform development and maintenance,24 51 printed materials52 and transportation.53–58
Consistent with the task-shifting approach described above, we assume the lowest appropriate level of provider would deliver each intervention. We assumed an annual attrition of 8.8% for doctors and 4.7% for community health workers.59 60 All health workers providing interventions receive monthly supervision in a group setting.
For each intervention, we calculated the monthly intervention cost per adolescent treated, which we assumed to remain constant throughout a year. We also calculated the costs of initial and refresher trainings for providers. In the first 12 months of the model, we assume that all people delivering the interventions require an initial training. In subsequent years, we assume that all people receive a refresher training except for departed providers, whom we assume to be replaced with people who require a round of initial training in their first year.
Unit costs of non-tradeable goods were converted to the local currency unit using the study year exchange rate, inflated to 2019 using the country Consumer Purchasing Index, converted to US$ using the 2019 exchange rate, and finally adjusted for purchasing power parity using the country 2017 conversion factor. This adjusted unit cost was then increased by 50% to account for facility-level system costs and a further 17% for above facility-level system costs.61
Unit costs of tradeables were converted to the local currency unit using the study year exchange rate, inflated to reflect change to 2019 using the global inflation rate and converted to US$ using the 2019 exchange rate. Physical goods were then adjusted for supply chain and distribution costs using the WHO CHOICE price multipliers for the appropriate region.62
The average monthly cost of each intervention by country income level is included in table 2. See online supplemental file 3 for all intervention unit costs and costs by country.
Step 4: follow up in adulthood
To capture the lifetime effects of preventing and treating mental disorders during adolescence, the model follows each age cohort by month for 80 years. The selected interventions are in effect only during each of the cohorts’ adolescent years (10–19). Based on the evidence from the literature, the intervention effects endure up to 18 months after the intervention ends. There are no studies that explore the effects of such interventions’ mental health outcomes in adulthood. However, while the intervention effects on disorder incidence will end by the time the cohort reaches 20 years and 6 months of age, the cohort starts adulthood healthier than they would have without the interventions, resulting in several additional years of health and economic productivity benefits.
When the adolescents enter adulthood, we track disease episodes only in those who developed a condition of interest before age 20, as those who remain healthy until the age of 19 would not be affected by our interventions. The two exceptions are people who develop either anxiety or depression before age 20 and then develop the other in adulthood, and individuals who die by suicide.
Step 5: sensitivity analysis
For each parameter varied in our probabilistic sensitivity analysis (PSA), we assigned a distribution, using the lognormal distribution for ORs, risk ratios and HRs and using the PERT distribution for all other parameters. We then generated a Latin hypercube sample (LHS) of 100 000 rows for each intervention with all parameters that varied in our sensitivity analysis.63 Where values differed by country, sex, and/or age at start, the LHS drew from the appropriate distribution. We then ran the model 100 000 times per intervention, drawing the values from a random row of the appropriate LHS each time. We present the median, range and IQR (the 25th and 75th percentiles) of these simulations.
These estimates differ from the base case estimates due to their methods of calculation. While in the base case, each of the estimates derive from the sum of the costs and benefits across all populations in the model or subset, the PSA considers the distribution of possible return on investments (ROIs) when looking at a single randomly-selected permutation of sex, age at start, and country.
Results
Results by country income, WHO region, sex, age and total appear in figure 1. Across all 36 countries included in the model, the return on investment for the package of interventions was 23.6 over 80 years (figure 1). This ROI means that for every $1 invested in the interventions, we expect $23.6 of health and economic benefits to be returned to the economy. By World Bank income levels, the highest ROIs were found in low-income (97.8) and lower-middle (94.6) income countries; geographically, the highest ROIs were to be found in the SEARO (128.3) and AFRO (125.6) regions. In general, these differences appeared to be driven by lower costs of the interventions, such as lower costs for labour.

Return on investment and cost per DALY averted for adolescent mental health interventions by subgroup, 2019–2099 (all costs in 2019 US$). DALY, disability adjusted life year.
Across all countries, the cost per DALY averted was $102.9. Similar trends hold for this measure, with the lowest cost per DALY averted coming in low-income ($2.5) and lower-middle ($4.7) income countries, and in countries in the SEARO ($3.5) and AFRO ($3.8) regions.
We also examined results based on the adolescent’s age at the start of intervention implementation. The ROIs are very similar for 10-year-olds (22.7) and 19-year-olds (21.3), which indicates the value of intervening for even a short time in late-adolescence. Although the ROI appears slightly more favourable for females than for males, this difference was small.
The ROI and cost per DALY averted vary for the different mental disorders and interventions. Anxiety alone is the most common condition among adolescents in our set of 36 countries, followed by mild depression. The effects of anxiety, however, are less severe than the effects of depression, so the ROI for treatment interventions for mild depression exceeds the ROI of the same intervention for anxiety (figure 2). In-person group-based CBT leads to a better ROI than individual CBT delivered through telemedicine and internet-based guided self-health interventions. For treatment of mild depression, group CBT has an ROI of 1692.6 and costs only $1.2 per DALY averted. This difference across forms of CBT is at least in part because the per person cost for the healthcare provider is lower. Additionally, for anxiety treatment, the OR of remission is higher for in-person CBT than for the internet interventions.23 24 Treatment of severe depression demonstrated a promising ROI and modest cost per DALY averted but cost more than the group treatment interventions due to the cost of medications and individual provider time. Three interventions have an ROI less than 1 for the overall cohort: individual treatment of anxiety (0.7), treatment of bipolar disorder (0.3), and indicated prevention of depression (−0.9). These interventions did demonstrate more promising outcomes in LMICs (see online supplemental file 4).
Supplemental material

Return on investment of adolescent mental health interventions by disorder. CBT, cognitive behavioural therapy; DALY, disability adjusted life year.
Universal prevention interventions for anxiety, depression and suicide also had a high ROI. The school-based intervention for anxiety and depression was the most cost-effective (147.4). Targeted suicide prevention intervention for adolescents treated for self-harm (62.0) and the universal, school-based suicide prevention programme (3.5) are also attractive investments.
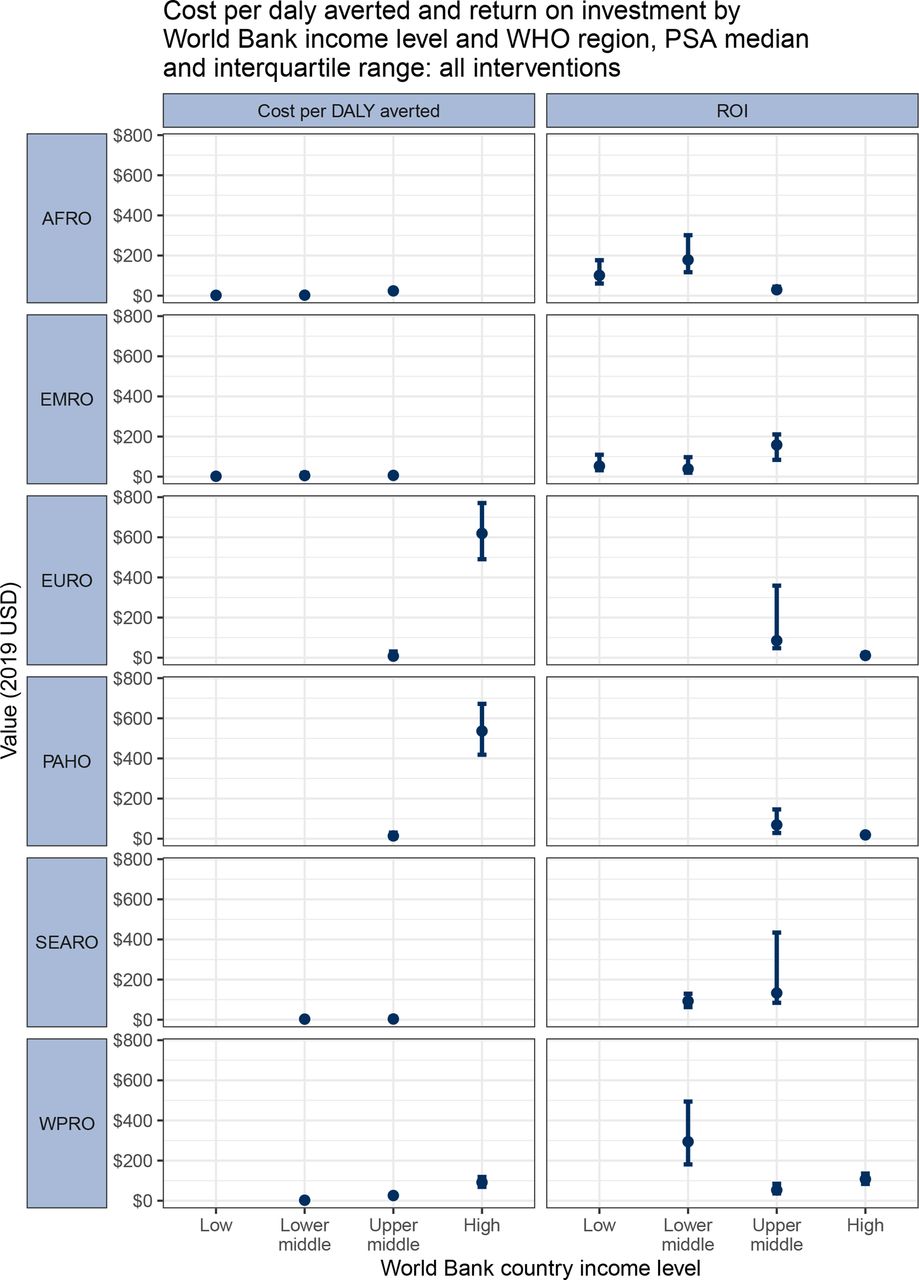
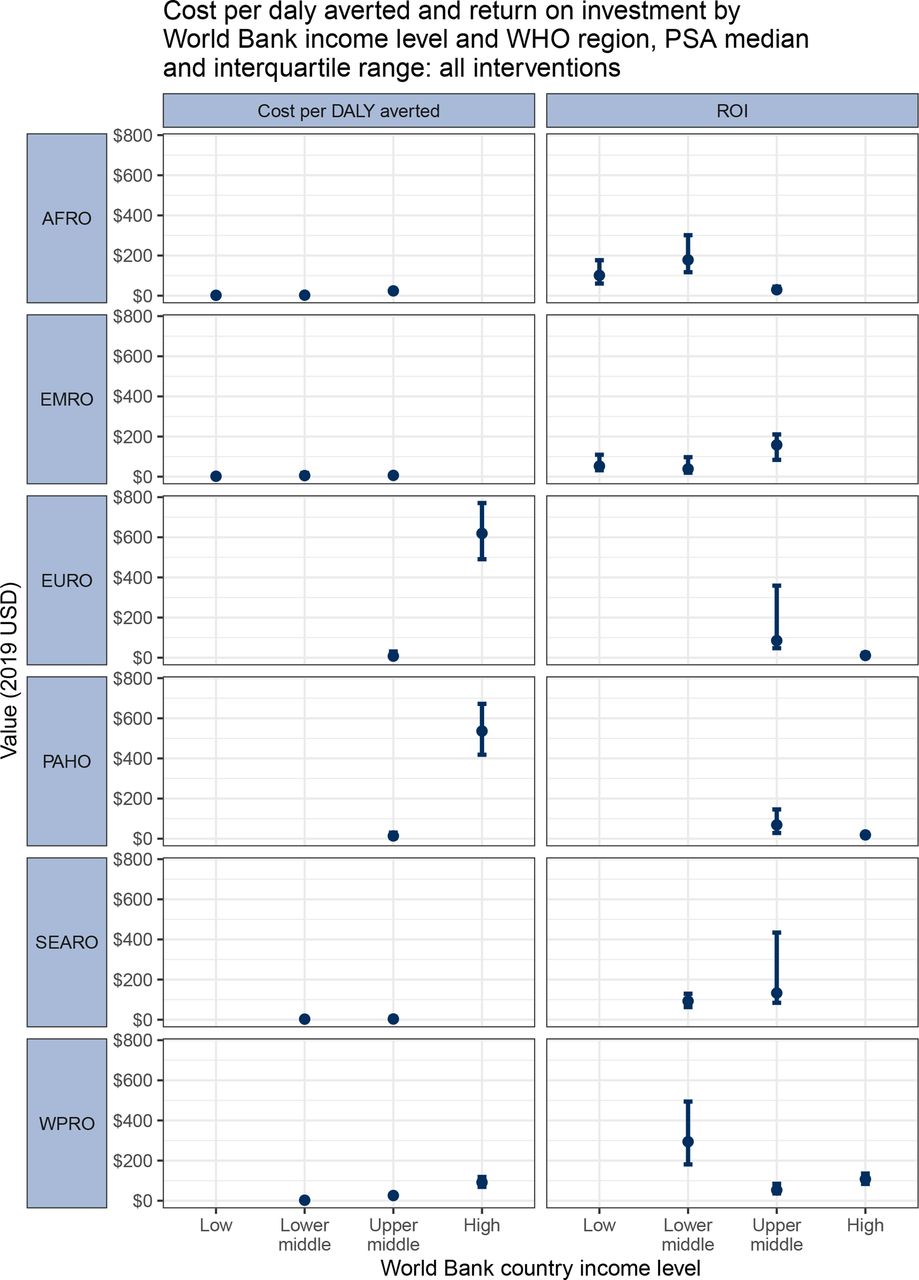
The results of the PSA showed a relatively high degree of uncertainty in the cost per DALY averted and the ROI for the all-interventions package (figure 3). Results varied by country income level and geographic region, with uncertainty lowest in the HICs, which had high costs per DALY averted and lower ROIs, and in the LICs, which had generally higher ROIs and lower costs per DALY averted. MICs showed the highest degrees of variation and uncertain, driven by each country’s specific balance between intervention costs (driven by labour) and benefits (driven by country GDP per capita and expected wages). In all country income and region subgroups, however, the IQR for the ROI remained higher than 1, which suggests a positive ROI in at least 75% of all simulations. Please see online supplemental file 5 for detailed PSA results.
{kind=link}
{kind=link}
{kind=link}
Probabilistic sensitivity analysis results of cost per DALY averted and ROI for all interventions by WHO geographic region and World Bank income level (2019 US$). DALY, disability adjusted life year; ROI, return on investment.
Discussion
The results of our study indicate significant economic benefits from implementing interventions to prevent and treat mental disorders among young people. The highest ROIs were observed for low-income and lower-middle income countries, reflecting the lower implementation cost in these settings. Nonetheless, ROIs for the package were substantial across all countries, indicating the economic value and health importance of investing in young people’s mental health in all countries. However, the ROI for the package of interventions obscures important differences in the ROI for individual interventions. Treatment of mild depression with in-person, group-based CBT had by far the highest ROI and a low cost per DALY averted. Treating mild depression results in reduced risk of death by suicide, which is the reason that mild-depression treatments have a higher ROI than the comparable interventions for anxiety, which affects more young people but has a much weaker association with suicide.64 In comparison, indicated prevention of depression and treatment of bipolar disorder had poorer ROI. Although all of the included interventions can meaningfully improve individuals’ lives, the ROIs and costs per DALYs averted in this analysis highlight the most powerful interventions from the societal perspective.
Across interventions, provider salaries are the greatest driver of intervention costs. For this reason, interventions delivered individually had a lower ROI than those delivered in a group or though guided self-help. Treatment of bipolar disorder and major depression requires a greater number of individual appointments with a more specialised provider—a physician rather than a lay health worker—to prescribe and supervise the needed medications and thus are resource intensive. However, the severity of consequences of a disorder also influenced the ROI, which remains high for interventions treating depression.
Our model estimated larger ROIs than previous analyses. A previous investment case for mental health prevention in Australia estimated that an internet-based anxiety prevention intervention for school aged students (11–17 years) had a 10-year ROI of 3.06.15 A similar school-based depression prevention programme for students in Australia had a 10-year ROI of 1.19.65 These ROIs are likely lower than our estimates due to the shorter time horizon and the inclusion of only healthcare cost savings and productivity gains, and not averted deaths by suicide which are a large contributor to the benefits captured in our results.
Economic evidence for adolescent mental health interventions in LMICs remains sparse, reflecting insufficient research on this issue, but also limited prioritisation of and investment in prevention and treatment for young people in LMICs. Adolescent-specific mental health services are crucial to address these gaps and prevent the loss of adolescents in the transition between services designed for children and those for adults.66 A range of interventions to prevent or treat the most prevalent conditions have proven effective, and this study provides an economic as well as an ethical and health case for implementing them.12 Programme designers in LMICs must adapt and test the modified interventions in their specific national circumstances before costing and planning for scale. Some mental health interventions have already been tailored to work within existing systems and delivery modes to reach young people in LMICs.67 68 The challenge, however, lies in making widely available youth-friendly mental health services the norm in all communities, rather than the exception.
The youthful demography of LMICs emphasises the need to ensure that untreated mental disorders do not impede the health, social and economic potential of young people.69 Adolescent mental disorders worsen the life chances and experiences of individuals and their families as well as their contributions to society. Preliminary evidence suggests that the COVID-19 pandemic will further exacerbate these effects.70 71 This study provides additional evidence for larger investments in adolescent mental health in line with political commitments made within Sustainable Development Goals and other global resolutions.72 73 Some of these interventions provide large, lifelong returns that accrue to both the individual and society. Although the investments needed to implement these services come largely from the health sector, the returns accrue largely in the economic sectors, which emphasises the need for a whole-government approach to adolescent mental health promotion.
Our analysis faced many limitations. First, the available effectiveness and cost-effectiveness evidence for adolescent-specific mental health interventions derives from HICs. These interventions are relatively untested in LMICs and require adaptation to LMIC resources, needs and capacities within different sectors, particularly health and education. Due to data limitations, we assumed comparable effectiveness of interventions between specialised settings in HICs, for which we had data, and the less-specialised models of intervention delivery used in this model. While task-shifting has proven effective for delivery of mental health interventions in LMICs,38–40 there may be associated impacts on quality and implementation fidelity with these approaches. The breadth of the IQRs generated in the PSA displays the uncertainty associated with many of the parameters in this model; better empirical data, especially data from LMICs, would allow for more accurate modelling.
One critical area in which data are limited is the coverage of mental health services and interventions. Our base case assumption was 20% coverage of interventions, which is based on a 2002 study that estimated that the unmet need for mental health services among children and adolescents in the USA was nearly 80%.5 We then vary the coverage estimates in the PSA between 10% and 50%, which was selected as an aspirational target in line with the coverage targets in the Sustainable Development Goals for services for other conditions. Although we based these estimates on older data from a HIC, our aim is to evaluate the costs and benefits of scaling up services, and the 20% base case target likely represents a scale up in coverage, especially for LMICs.
We applied our analysis to all adolescents in the 36 countries and did not distinguish those most at risk, such as those affected by conflict. In addition, since our cohort was constructed based on the raw number of DALYs lost by country, the cohort is biased towards larger countries and may not be representative of all countries. We have also not accounted for the lack of diagnostic capacity or other health system barriers that limit access to these mental health interventions. In this sense, our analysis illustrates the potential benefits of scaling up adolescent mental healthcare but does not capture the specific startup costs required to address limitations in system-level capacity in every country. Future country-specific analyses could better adapt coverage and capacity estimates and scale-up scenarios for a given country context.
Finally, for the purpose of this analysis, we assume that interventions start and end in adolescence. Mental health requires appropriate interventions throughout the life course, and greater economic benefits would be achieved by continuing the provision of high-quality mental health services into adulthood.
Conclusion
We present the economic case for investing in a strong package of care for adolescent mental health, in which the costs of implementation are repaid to the economy 23.6 times over on average. Current investments in mental health are inadequate, especially in LMICs, which spend an average of less than $2 per person a year on mental healthcare, as opposed to more than $50 in HICs.10 Investment is required to strengthen and expand existing mental health services and to implement innovative models of care, such as the task-shifting and internet-based interventions we include. The specifics of these interventions must be tailored to each context to ensure that services meet the mental health needs of adolescents and are accessible in the given setting. The COVID-19 pandemic has heightened the stress and uncertainty of adolescence, which further increases the need for promoting mental health among adolescents. Investing in mental health promotion during adolescence has lifelong health and economic benefits and should be a priority in further investment.
Data availability statement
Data are available in a public, open access repository. Code and datasets are available at https://github.com/rdstelmach/AMHIC-global.
Ethics statements
Patient consent for publication
Ethics approval
This study did not receive nor require ethics approval, as it does not involve human and animal participants.
Acknowledgments
We would like to thank Hae Jeong Cho, Grace Gordon, Enzo Nervi, Sri Ramesh and Shella Zhou who contributed to literature review in the early stages of the project. We would also like to thank Dr Kenneth Carswell, Dr Devora Kestel, Dr Chiara Servili, Dr Inka Weissbecker and Dr Lawrence Wissow for advising the authors on the most appropriate treatment protocols and interventions for mental disorders among adolescents; Dr Dan Chisholm, Dr Yong Yi Lee and Dr David Watkins for providing guidance on the development of the costing methodology; and Dr Donal Bisanzio and Evan Patterson for guidance on defining and running the probabilistic sensitivity analyses.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @angiembjm, @rachelnugent
Contributors RN conceived and designed the study and is the guarantor. RS developed the model and analysed the data. RS, ELK and IK collected the data. All authors interpreted the data. SS and AMJ-M contributed to the design of the study and interpretation of the results. RS, ELK, IK and AMJ-M wrote the first draft of the manuscript. All authors reviewed the draft and revised it for important intellectual content.
Funding Funding for this work was provided by the Charities Aid Foundation through a grant from AstraZeneca Young Health Programme. Neither organization had any role in the conceptualization or conduct of the work.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.