Article Text

Abstract
In 2017, the national agency for health security (L’Agence Nationale de Sécurité Sanitaire—ANSS) in Guinea implemented the District Health Information Software (DHIS2) as the Ministry of Health national surveillance system to capture and report aggregate disease data. During 2019, the ANSS started using DHIS2 Tracker to collect case-based (individual-level) data for epidemic-prone diseases. In 2020, the capability was expanded, and it was used during the COVID-19 pandemic to capture data relevant to the COVID-19 response. When an Ebola virus disease (EVD) outbreak was announced in February 2021, the Tracker module was updated, and enhanced functionalities were developed to meet the needs for the emerging epidemic. This novel EVD module has components to capture information on cases, contacts, alerts, laboratory and vaccinations and provides a centralised site for all EVD outbreak data. It has since been expanded for use with future viral haemorrhagic fever outbreaks.
- viral haemorrhagic fevers
- public health
- infections, diseases, disorders, injuries
- epidemiology
- health systems
Data availability statement
Data sharing not applicable as no data sets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- viral haemorrhagic fevers
- public health
- infections, diseases, disorders, injuries
- epidemiology
- health systems
SUMMARY BOX
Based on experiences during the 2014–2016 Ebola outbreak, the Guinean Ministry of Health recognised the need to standardise and centralise information systems to be better prepared for future outbreaks.
When a new Ebola outbreak was reported in February 2021, the Guinean government decided that all data relevant to the outbreak should be managed in one country-owned system using the same platform as the national routine surveillance system.
The existing case-level District Health Information Software Tracker module was modified to capture and manage all data related to an Ebola virus disease (EVD) response, allowing response leaders to make data-driven decisions.
Guinea was successful in rapidly deploying an EVD module and enhancing it amid an outbreak response despite challenges such as limited resources and data quality issues, creating a module that will be a useful tool in future viral haemorrhagic fever outbreaks.
Introduction
In March 2014, forty-nine confirmed cases of Ebola virus disease (EVD) in southeast Guinea were reported by the WHO signalling the official start of the largest Ebola outbreak to date.1 2 Neighbouring West African countries of Liberia and Sierra Leone were also significantly impacted and by the end of the epidemic more than 2 years later, the total worldwide case count stood at 28 652 with 3 814 (13.3%) cases in Guinea alone.2 3
The magnitude of the 2014–2016 Ebola outbreak required the cooperation of international, regional, national and local partners.3 At the time, existing data systems in Guinea were focused on routine (indicator-based) public health reporting and not on managing case-level data for a major outbreak with thousands of cases and contacts spread throughout the country. This led to new and constantly evolving demands for data and for systems to manage the critical information.4 Coordination between groups focused on various aspects of the response such as surveillance or laboratory was challenging as common data needs emerged but unique requirements also arose depending on the group. This resulted in the generation of multiple databases and systems using various tools such as Excel to Epi Info Viral Hemorrhagic Fever application, creating operational challenges when trying to assimilate and analyse the data to inform decision makers in a timely manner.5
Based on this experience, the Guinean Ministry of Health (MoH) recognised the need to standardise and centralise information systems to be better prepared for future outbreaks. The national agency for health security (L’Agence Nationale de Sécurité Sanitaire—ANSS) was tasked with monitoring and responding to public health events that threaten health security. One of ANSS’ primary missions was to develop a nationwide data system for detecting and responding to potential events of public health concern. Through an evaluative process in which various platforms were compared with the country’s data needs, District Health Information Software (DHIS2), a web-based platform currently used by more than 70 countries was selected.6 This open-source system was deemed suitable and with the large community of practice including neighbouring countries, it was hoped that implementation of DHIS2 would contribute to cross-border sharing of information.
In 2017, ANSS piloted DHIS2 in two regions as the national surveillance system for routine indicator-based reporting of aggregate disease data.7 Expansion nationwide followed in 2018–2019, which included implementation of the DHIS2 case-based Tracker module for individual case reporting.8 Initially, collection and reporting of individual-level data using the module was inconsistent and not used routinely for all priority diseases. However, in 2020, the COVID-19 pandemic generated an urgent need for an outbreak management system capable of handling a large amount of case and contact data, as well as laboratory and potentially vaccination information. ANSS built on the existing Tracker module, and with the help of a joint internal and partner technical team created a Guinea-specific COVID-19 module to manage the country’s response to the pandemic. This module was successfully deployed from the national to the district and health facility levels, expanding country capacity for conducting case-level surveillance.
On 14 February 2021, the Guinea MoH reported a cluster of EVD cases in Gouecke in the N‘Zerekore region of southeast Guinea. This was the first reported Ebola outbreak in Guinea since the 2014–2016 West Africa Ebola epidemic, which also started in this rural forested region.2 Building on the successful experience with the DHIS2 module modified for COVID-19, ANSS immediately began enhancing the Tracker module to meet the emerging needs of Guinea’s EVD epidemic response. Through continual feedback from field teams using the system throughout the 4-month response, the EVD module was regularly updated, and features added even after the outbreak was declared over on 19 June 2021.
The purpose of the system was to capture and use case-level data during the EVD outbreak to provide timely and complete information to the response decision makers:
Collect all data relevant to the EVD outbreak and response in one system at the lowest operational level available.
Make valid data available in a useable format in a timely manner that can be used to prepare reports to inform the response structure.
Generate a system flexible enough to use for other infectious disease outbreaks in the future.
Understanding Ebola virus disease response needs
Although the time frame for roll-out was accelerated due to the urgent need for the application, updating the existing module was required to meet response needs. This was done by examining the revised MoH forms for case investigations and EVD alert notifications, reviewing EVD surveillance guidance and consulting with epidemiologists from ANSS and partner organisations like the Centers for Disease Control and Prevention, WHO and the African Field Epidemiology Network. Current case definitions were used to inform what data elements should be collected when entering a case. Probable or suspect status was entered manually, while confirmed status updated automatically when a positive laboratory result was entered to improve efficiency. Current systems’ data elements and data sources such as facility registries, vaccination registries and Ebola treatment units’ case management registries were also examined to understand what data are presently captured and how. This in turn informed what existing data collection processes should be streamlined or maintained to mitigate the introduction of too many new procedures (figure 1).
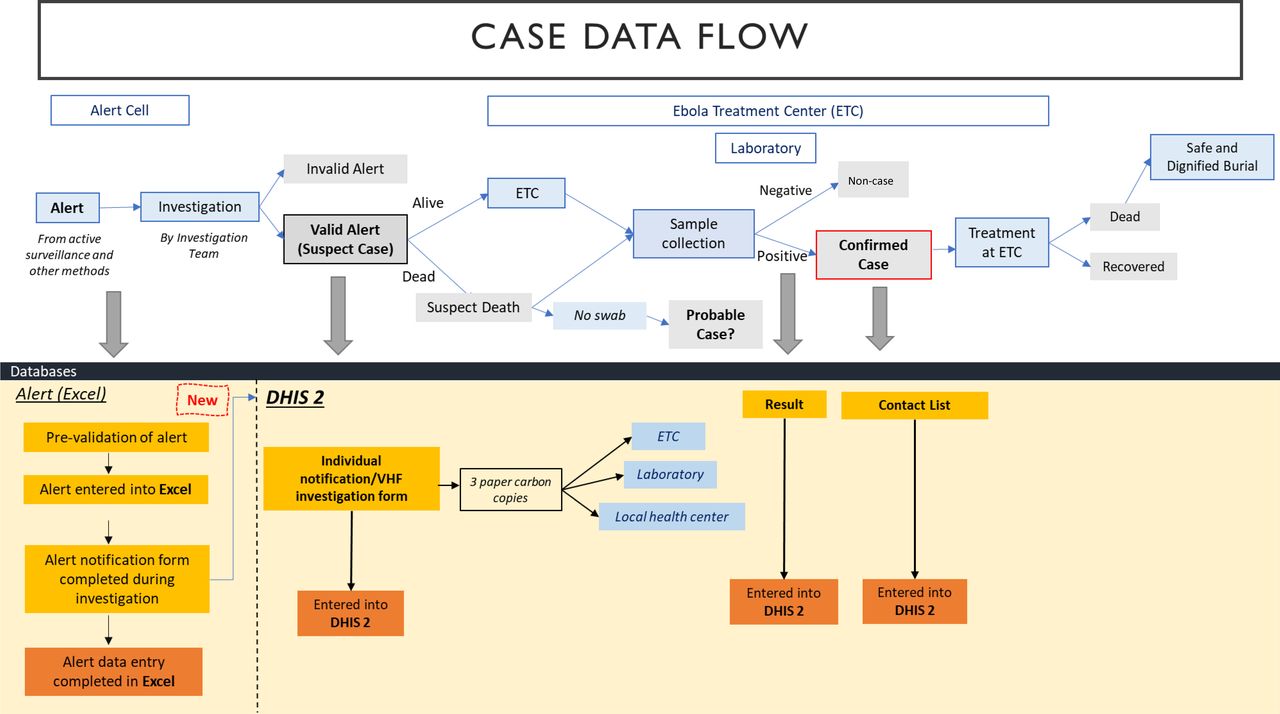
Data flow diagram for alerts, cases and contacts. An alert of a possible suspect case was most often raised from active case finding in health centres, although notifications also came from the community or via contact follow-up. Minimal information on the alert is collected on a notification form and entered in an Excel worksheet by the Alert Cell, an alert data management unit. An investigation team is then sent out to validate or invalidate the alert. If the person is deceased, a swab is taken for testing. In the event that no swab was collected, the case is investigated as a suspect case and may be considered a probable case if meeting the case definition. If the person is alive and the alert is validated, the person is considered to meet the suspect case definition and a more thorough investigation is conducted. For this, a comprehensive three-copy viral haemorrhagic fever (VHF) case investigation form is completed. One copy remains with the local health centre while two copies are sent with the suspect case to the Ebola treatment centre (ETC). A specimen is collected and sent to the laboratory for PCR testing by GeneXpert with one copy of the form. If the result is positive, the case is ‘confirmed’, and appropriate treatment is administered. All confirmed case deaths and probable cases are recommended for safe and dignified burials. Information from the alert notification form, the investigation form, the laboratory results and the contact list is entered into the District Health Information Software (DHIS2) Ebola virus disease (EVD) module.
Various user levels were employed to address data security concerns: view only, view and enter data or ‘super user’ access that would permit adding or editing variables. To meet reporting needs, a dashboard with real-time updates from entered data was built to provide essential numbers at a glance. Over time, the dashboard was modified to reflect epidemiological needs of the response such as adding epi curves and maps. Automatic validation of data within the system was minimal and limited to simple checks including verifying the number of digits entered or restricting the type of data certain fields would accept (eg, alphabetic characters, numbers). Manual data checks were the primary means of validation with subsequent plans created to incorporate more data entry restrictions and automated logic checks.
Prior to deployment, the system was tested by the information technology (IT) team and epidemiologists at the national level and final changes were made in preparation for implementation. A ‘super user’ was trained by the IT team and sent to the field to deploy the system and to train other users. Initially, 10 users were trained with subsequent users trained on arrival in the field. Training included how to input cases, contacts and related laboratory data on the offline Android application and web-based application on tablets. Follow-up training continued in the field with weekly instructional sessions that covered topics such as entering cases, contacts and how to link them, and any new functionalities or elements that had been added to accommodate new data analysis requests. Technical support was provided by the super user, other users including partners or the Conakry-based IT team.
Implementing and enhancing during an active Ebola virus disease response
Building and deploying a data management system during an outbreak can present challenges. It also offers a unique opportunity to field test and continually monitor and improve the tool, while still meeting operational needs. The Tracker module that was originally created in 2018 was updated to meet the new case reporting needs including adding contact and vaccination features and was deployed within 3 days after the first case was reported on 14 February 2021. Modifications continued throughout the outbreak based on user needs. By 19 June 2021, the official date for the declaration of the end of the 2021 Guinea EVD outbreak (4 months later), there was the capability to collect data on alerts, cases, contacts, laboratory and vaccination, features added to the original module, with ongoing efforts to allow linkages between these data.
Features added after initial roll-out of the system included new data elements, Global Positioning System coordinates for health facilities and a dynamic Ebola transmission module. A generic regional user access account was created to allow users to enter data from outside the immediate district. Further functionalities created included the ability to link one contact to multiple Ebola cases, and to add multiple contact follow-up time periods for the same person. This is a critical capacity as other tools have difficulty identifying and quantifying contacts whose 21-day monitoring period needs to be restarted due to new exposure.
To increase efficiency, a new component was designed to capture and manage EVD alert data which would automatically populate a case investigation report when an alert was investigated. To accommodate the need for capturing data related to rapid diagnostic tests (RDT), elements were added in May 2021 so that during entry of a suspect death, users could record RDT results, a picture of the determinate test cartridge, corresponding PCR results and whether a safe and dignified burial was administered.
Using the diverse data available in the EVD module, visualisations incorporating multiple facets were generated for use in reports and on the dashboard. The original dashboard contained mostly numerical data with some visualisations while later iterations incorporated more analyses shown in various graphics and maps (figure 2). By viewing the dashboard, users could see near real-time visualisations of the entered data.
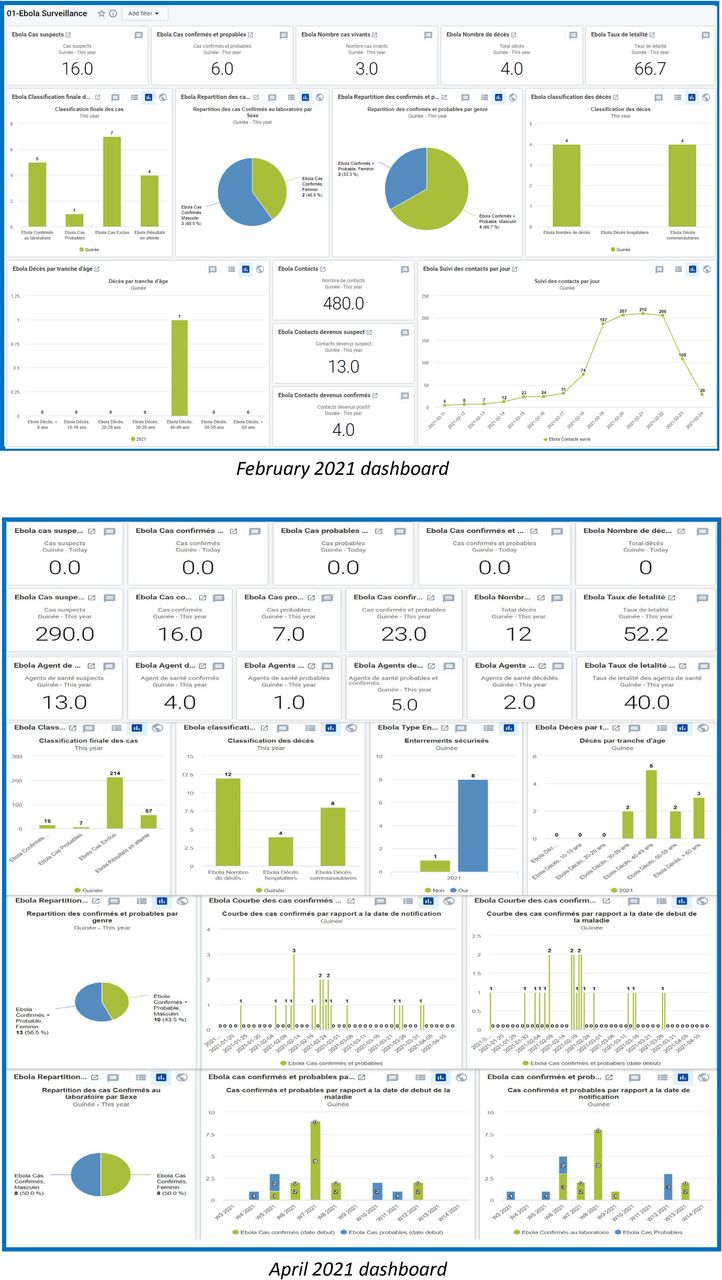
Visualisations created within the system and added to the dashboard over time.
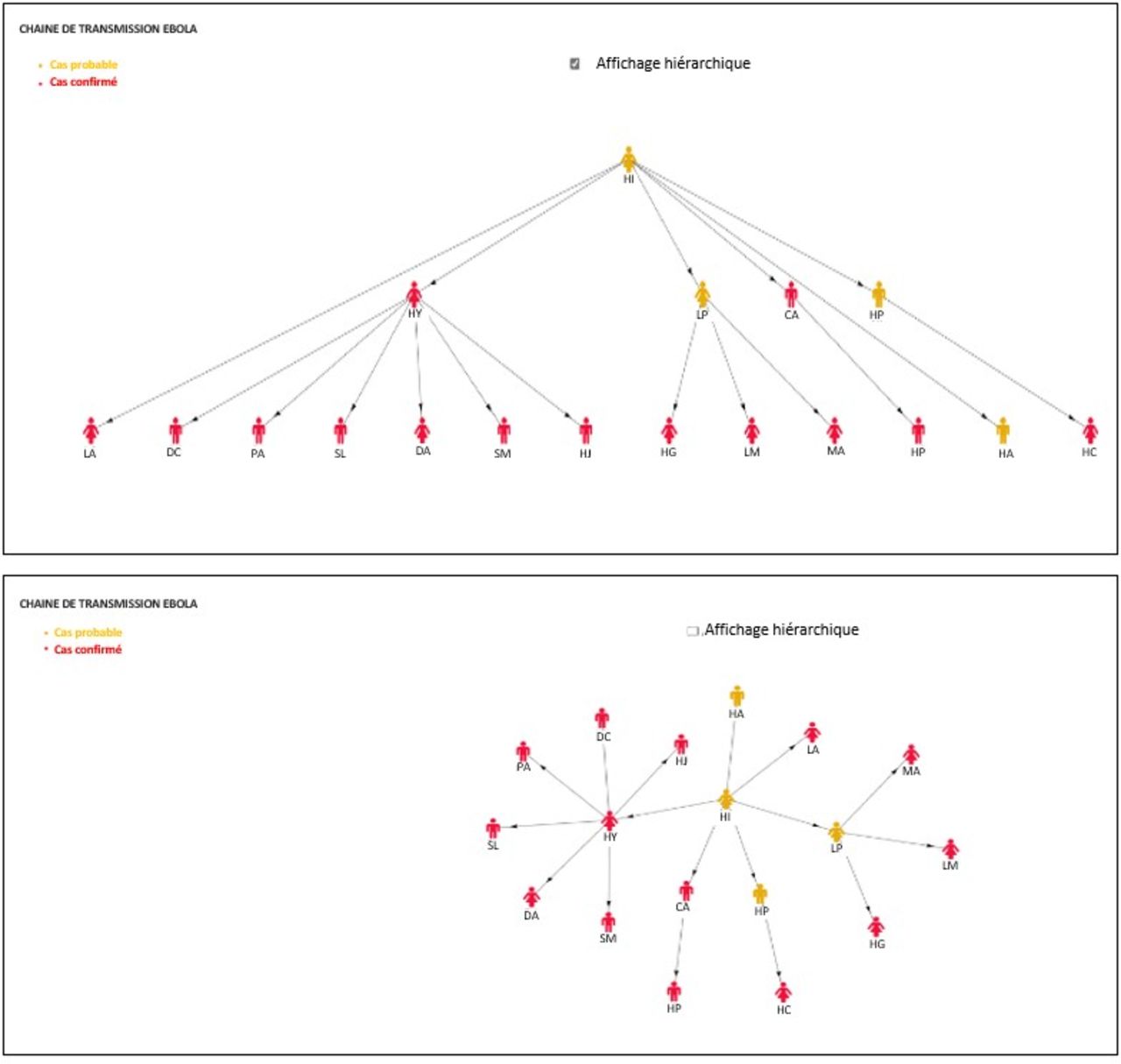
In response to the need for a way to visualise epidemiological links between cases, the team worked with responders to develop an add-on application to create dynamic transmission chains (figure 3). This application allows users to see cases with demographic data such as gender and age, their source case and any subsequent secondary cases. This assisted field teams in identifying cases that had not been linked to other earlier cases and quickly determining the total number of contacts each case produced.
{kind=link}
{kind=link}
{kind=link}
Transmission chain visualisations created to show relationships between cases and contacts.
Successes
By the end of the 2021 EVD outbreak on 19 June 2021, Guinea had successfully deployed a case-based EVD surveillance system. Individual-level data for all 23 cases as well as contact and vaccination information were managed in this centralised system with a dashboard of up-to-date information made available to decision makers. The system has since been modified to be used for viral haemorrhagic fever (VHF) outbreaks such as Marburg virus and Lassa fever.
Guinea went from piloting a new system for reporting aggregate disease surveillance data in two regions in 2017 to deploying the system nationwide and implementing a module during an outbreak to capture all case-level data related to an EVD outbreak in 2021. Consolidating multiple data sources into a single system means this module can be used for an entire EVD response and will not necessitate different databases or software for the various components. This achievement permits response leaders to make critical decisions based on timely data rather than on anecdotal evidence.
Reinforcement of the overall DHIS2 system rather than implementing externally managed, non-integrated data tools is a key MoH priority. By expanding the existing national surveillance platform to centralise outbreak data management, the EVD module strengthens the MoH-managed system. This ensures ownership of the data is fully within the governance of the country without undue dependence on partners. Partners can now coordinate efforts in support of a unified system for disease surveillance rather than a multitude of parallel systems.
The EVD-specific module is a novel application within DHIS2 to collect and manage case-level outbreak data for an EVD epidemic but due to the flexibility of the application and the trainings developed for it, minimal additions are needed to use this system for an outbreak of VHF caused by a different pathogen. Conclusively, by training on this application at subnational levels of the health system, surveillance capacity at local levels was increased, expanding preparedness for future events.
Challenges
According to The World Bank, health expenditure per capita expressed as a percentage of gross domestic product in Guinea was less than 4% (3.93%) in 2018, the most recent year for which data are available. This contrasts sharply with neighbouring country Sierra Leone (16.06%) and partner country the USA (16.89%).9 This makes sustainability of surveillance system improvements a major challenge and creates dependencies on partners to provide ongoing resources. As well, these improvements are often funded by partners in response to an outbreak once a deficit in reliable and timely data is recognised, versus the government preparing proactively through consistent funding of training and routine supervision.
Although one of the primary objectives of this module was to create a centralised repository for all outbreak data to eliminate multiple systems, duplicate databases with the same information persisted. Key reasons were that not everyone had access to the EVD module or endeavoured to use it. For example, parallel line lists for vaccination and surveillance contacts were created and maintained resulting in duplicative efforts and questions around the validity of both lists. Information did not match or was incomplete in one source or the other causing delays in presenting timely data as verification between sources was conducted.
Concerns around data quality attributes of completeness and timeliness also existed.10 While there are a minimum number of fields required to save an entry, many could be left unfilled until data entry was resumed on returning from the field each evening or even weeks later. Incomplete data meant that ‘real time’ dashboard values were potentially incorrect and that analyses had to be repeated frequently to ensure the most up-to-date information was being presented. Unreliable internet access also inhibited timely data upload even when all data were entered.
Readiness of capable users was another challenge as field teams changed and new users had to be trained. Official laptops were not available for data entry and there were varying levels of competency with electronic data entry on tablets, which led some team members to collect information on paper forms and then enter in the web-based application on returning from the field, even though offline data capture was possible. This produced errors in data entry such as name misspellings or inaccurate dates, leading to additional concerns around data accuracy. Because timely, complete and accurate data are critical to an effective emergency response, training field team members to effectively collect and input these data could have a major impact on how the outbreak progresses.
Conclusion
Several important learning points emerged from this experience. Had time allowed prior to deployment, it would have been beneficial to engage the end users in development. Their input on the data flow from point of collection to analysis and reporting could have streamlined the process and ensured the most efficient practices. Because user feedback happened after implementation, the system was then active and proposed changes had to be carefully weighed from a benefit to cost perspective in terms of how they might affect the ongoing emergency operations.
Advocating for an established and MoH-approved system promotes ownership and governance by the local government. In future EVD outbreaks, the country-endorsed DHIS2 system should be used by all response partners so that response and data analysis are coordinated. It is important to maintain the progress and to keep advancing, thus developing a sustainability plan is key. This includes instituting fully trained super users within ANSS and establishing dedicated internal funding sufficient for needed equipment and connectivity.
To inform system updates, an evaluation needs to be conducted to identify areas for improvement. Public health surveillance system attributes of timeliness, completeness, validity and flexibility are key aspects to examine.10 Regular monitoring of data quality could inform specific modifications such as incorporating more automated data validations or adding more drop-down features in key error-prone fields.
Future goals entail enhancing the EVD module to meet the needs for other epidemic-prone disease outbreaks such as for vaccine-preventable diseases managed by the Expanded Program on Immunization and linking it with the national routine surveillance DHIS2 system for streamlined reporting of all notifiable diseases. Guinea’s success in rapidly deploying an EVD module, field testing and enhancing it during an outbreak response, and its flexibility to include typically vertical response elements in an integrated manner is laudable. This module should be shared with other countries at risk for EVD outbreaks to encourage technology and data sharing within the region. In a country where resources for public health are limited, advocacy for the continued maintenance and expansion of an existing successful system should be supported.
Lessons learnt during the 2014–2016 West Africa epidemic fostered many improvements in surveillance of and response to epidemic-prone diseases in Guinea. Capacity-building efforts such as implementation of epidemiological training programmes for MoH staff and enhancements to the national and subnational surveillance systems likely contributed to earlier detection and response to the initial cases. While it is difficult to say if these efforts ultimately resulted in the substantially reduced case counts over the previous epidemic, it is anticipated that this experience and the resulting tool could be immensely valuable in detecting and responding to future outbreaks of similar epidemic-prone diseases.
Data availability statement
Data sharing not applicable as no data sets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Footnotes
Handling editor Seye Abimbola
Contributors All authors contributed to the design of the work and/or the acquisition, analysis and interpretation of the data, and/or contributed meaningfully to the drafting or revision of the manuscript, and provided approval for the publication.
Funding Center for Global Health, Centers for Disease Control and Prevention (GH20-2131).
Disclaimer The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the Centers for Disease Control and Prevention (CDC). Use of trade names and commercial sources is for identification only and does not imply endorsement by the US Department of Health and Human Services or CDC. References to non-CDC sites on the Internet are provided as a service to readers and do not constitute or imply endorsement of these organizations or their programs by CDC or the U.S. Department of Health and Human Services. CDC is not responsible for the content of pages found at these sites. URL addresses listed were current as of the date of publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.