Article Text

Abstract
Background Patient rights aim to protect the dignity of healthcare-seeking individuals. Realisation of these rights is predicated on effective grievance redressal for the victims of patient rights violations.
Methods We used a critical case (that yields the most information) of patient rights violations reported in Karnataka state (South India) to explore the power dynamics involved in resolving grievances raised by healthcare-seeking individuals. Using interviews, media reports and other documents pertaining to the case, we explored the ‘governmentality’ of grievance redressal for patient rights violations, that is, the interaction of micropractices and techniques of power employed by actors to govern the processes and outcomes. We also examined whether existing governmentality ensured procedural and substantive justice to care-seeking individuals.
Results Collective action was necessary by the aggrieved women in terms of protests, media engagement, petitions and follow-up to ensure that the State accepted a complaint against a medical professional. Each institution, and especially the medical professional council, exercised its power by problematising the grievance in its own way which was distinct from the problematisation of the grievance by the collective. The State bureaucracy enacted its power by creating a maze of organisational units and by fragmenting the grievance redressal across various bureaucratic units.
Conclusion There is a need for measures guaranteeing accountability, transparency, promptness, fairness, credibility and trustworthiness in the patient grievance redressal system. Governmentality as a framework enabled to study how subjects (care-seeking individuals) are rendered governable and resist dominant forces in the grievance redressal system for patient rights violations.
- Health policies and all other topics
- Health policy
- Health services research
- Health systems
- Qualitative study
Data availability statement
Data are available in a public, open access repository. Data are available on reasonable request. Some data are available in the public domain. Remaining data is available on a reasonable request to the authors.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Health policies and all other topics
- Health policy
- Health services research
- Health systems
- Qualitative study
WHAT IS ALREADY KNOWN ON THIS TOPIC
Effective remedial systems are essential to redress and deter patient rights violations.
Care-seeking individuals face several barriers to raise and pursue complaints concerning their healthcare encounters at the health facility level in high, low, and middle-income country settings.
WHAT THIS STUDY ADDS
An array of practices deployed by the medical profession and the State bureaucracy served to ultimately gain and maintain power over the governing practices and outcomes of grievance redressal systems.
Domination by the medical profession and the State bureaucracy compromised procedural and substantive justice in the formal grievance redressal processes.
There were opportunities and constraints for the collective of care-seeking individuals to counter the entrenched medical and bureaucratic power during grievance redressal processes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Grievance redressal systems for patient rights violations should assure accountability, transparency, promptness, fairness, trustworthiness and credibility.
In settings with domination by the medical profession and the State bureaucracy, collective efforts of care-seeking individuals will need to apply creativity and perseverance to subvert the unjust governing practices in the formal grievance redressal systems.
Background
Patient rights are one of the many ways of applying human rights principles in healthcare and are aimed at protecting the dignity of care-seeking individuals.1 Patient rights charters used in health facilities vary across and within countries. Charters (across various contexts) often prescribe list of rights that include right to informed consent, privacy, confidentiality, dignified treatment, access medical records, information and redress. These rights are derived from one or more core ethical principles such as autonomy, beneficence, non-maleficence, patient-provider fiduciary relationship, justice, sanctity and dignity of human life.2
Within the theory and practice of human rights, State has the responsibility to formulate laws to remedy rights violations. Some scholars contend that any right without a remedy is only a declaration of social value that may or may not be implemented.3–5 In this regard, several countries have developed institutional arrangements intended to receive, examine and resolve the complaints raised by individuals about their healthcare encounters.6 Care-seeking individuals can raise grievances concerning technical aspects of care (eg, clinical care provided) or non-technical aspects of care (eg, staff-patient relationships and management-related issues). Few qualitative studies found that exorbitant costs, lack of time to raise and follow-up the complaints, lack of or inadequate practical and emotional support to pursue complaints, inadequate financial resources deter care-seeking individuals from availing grievance redressal services. In addition to the list mentioned above, poor knowledge on complaint procedures, perceived feeling of powerlessness, a suspicion that a complaint will not bring any change, fear of being seen as trouble-makers by the care providers and potential negative consequences on the care received owing to the complaint raised are barriers for care-seeking individuals to raise complaints.7–15 This is why care-seeking individuals who come forward to raise a complaint against a healthcare professional or a health facility often complain informally to frontline workers directly or prefer other informal channels for complaint resolution. Mirzoev and Kane14 posit that the rise in informal complaints is because the formal institutional arrangements for grievance redressal are either not accessible or people have lost trust in existing mechanisms for grievance redressal or in the institutions that established them.
The scholarship on patient grievance redressal systems from India and other low-and middle-income countries (LMICs) is limited6 14 and is mostly focused on awareness of patient rights.16–20 Some studies explored the functioning of patient complaint management at the health facility level. For example, a study from Vietnam focused on the complaint management processes at the health facility level and highlighted issues such as inadequate resources for complaint management procedures, poor oversight mechanisms, limited public awareness about the channels for complaint management, power asymmetry, bureaucracy involved in complaint procedures and pressure on the health facilities to safeguard reputation at any cost especially in settings where litigation is likely.21 Another study from Bangladesh demonstrated that the complaint management systems within the government health facilities suffered from unclear lines of accountability, lack of policy direction, poor documentation and political interference.22 Nonetheless, a critical examination of power dynamics involved, especially when aggrieved care-seeking individuals reach out to formal complaint bodies that exist beyond the health facilities particularly (in LMICs) is scarce.
In this article, we aim to understand whether and how power dynamics influence the patient grievance redressal system. The laws related to remedies for rights violations are intertwined with notions of justice. Legal scholars assert that the laws related to remedies for any rights violation should ensure procedural as well as substantive justice.23 24 Procedural justice refers to justice in the processes and procedures within the juridical-legal mechanisms and substantive justice denotes the justice of outcomes of the remedial system. The justice of outcomes should assert dignity and equality for victims of injustice.23 Shelton24 contends that the law of remedies should minimise or reverse the harm done by wrongful acts such as violations of one’s rights through appropriate compensation and/or punishment. It should also deter people from violating human rights. We examined whether the grievance redressal system ensures procedural and substantive justice to protect patient rights in health facilities using the case of alleged patient rights violations by a medical professional in a government health facility in Karnataka, a state in southern India. The collective of aggrieved women, with the support from two community-based organisations (CBOs), pursued the case in several patient grievance redressal forums and other institutions available. Between 2016 and 2017, civil society organisations in Karnataka advocated for a legally binding patient rights charter and pitched for a patient-centric legislation to regulate the private health sector in Karnataka.25 All these taken together, the case of alleged patient rights violations lends itself to an exploration of power relations that shape the contours of patient grievance redressal system in an LMIC setting such as Karnataka, India.
The governmentality lens to study power dynamics
Power theorists either have conceptualised power with the focus on sources (ie, where power comes from?) or on the processes, strategies and techniques of power(ie, how power is practiced or exercised?).26 Foucault27 conceptualised governmentality as a form of power that is cautiously orchestrated by dominant actors through a combination of tactful measures such as norms, beliefs, institutions, (in)formal procedures, rules and regulations on a specific population to govern and achieve a specific result. Power is exercised through direct control, in visible ways, and also operates through indirect and subtle ways (eg, through beliefs, norms, standards, procedures, institutions) so as to shape people’s behaviour.28 The State is not the locus of power, rather power is pervasive and multicentric in nature. Foucault29 emphasised how governing comes into being, as an “art” by which ‘some people are taught to govern others and some let themselves be governed’. Governmentality encompasses all the microprocesses and instruments to govern. The governed do not easily question the status quo as the governing processes are internalised, for example, through norms, institutional practices and beliefs.30 In the domain of healthcare, the governmentality way of analysing power is applied to explore healthcare organisation,31 integrated healthcare,26 health promotion,32 medicalisation of society,33 health policy analysis34 and in critical public health studies.35
Foucault is often critiqued for not providing sufficient room for collective agency that upsets dominant power and catalyses social change. But some scholars36–39 contend that Foucault offers a theory of resistance or collective agency in his work. Pickett36 and Flohr37 argue that since power is everywhere in governmentality, it also opens microspaces of resistance. To govern in a governmentality sense entails that one has the power to create or shape possible fields of action for others. Hartmann38 and Flohr37 posit that if governmentality defines the field of possible action for subjects within which the subject is free to act, then resistance is about the subject’s effort to redefine the fields of possible action. Legg39 supports this by positing that resistance is a form of power within the “geographies of governmentality” that extends from “the royal courts and the democratic assembly to the public square and streets”. Thus, resistance itself could be studied from a governmentality perspective. We applied governmentality as an analytical tool (figure 1) because it captures the practical expression of power through processes and practices involved in domination and resistance specifically in the grievance redressal for patient rights violations.

Intersecting fields of governmentality.
We analysed how governmentality defined by the dominant actors, harboured resistance among the collective of care-seeking individuals as they used certain practices and strategies to redefine the governmentality of the grievance redressal for patient rights violations. The main aim of the research was to examine if the governmentality of grievance redressal for patient rights violation in settings such as Karnataka, secured procedural and substantive justice to aggrieved care-seeking individuals.
Methods
We used a single case study design.40 The study setting is Karnataka (described in box 1). We used a critical case of an alleged patient rights violation in a government health facility in Karnataka (see box 2). This is a critical case because (i) methodologically, it offers a rich account of practices and processes involved and highlights notable outcomes, successes or failures of the patient grievance redressal system, (ii) it generated collective action on the part of community/civil society based organisations at the local and state level, (iii) it was widely covered in media and caught the attention of state policy makers and (iv) it was one of the triggering events to amend a law meant for regulating private health sector in Karnataka between 2016 and 2017.6
The case study setting: Karnataka, India
Karnataka is a state in southern India with a population of about 61 million.78 For administrative purposes, the state is divided into 31 districts and 177 subdistricts (taluks). The state contributes to 8% of the country’s Gross Domestic Product(GDP).79 Considering the human development index, Karnataka has been a middle ranking state.80
The state has a pluralistic mixed health system. It has three tier public health system which constitutes a network of health subcentres, primary healthcare centres, community health centres (secondary level healthcare facilities) and district hospitals (tertiary level healthcare facilities). Alongside, the private health sector is well-represented comprising of small clinics run by single practitioners to large corporate hospitals. However, the health infrastructure is unevenly distributed. More often than not, the rural and the remotest parts of the state are catered by informal healthcare providers and/or professionals of AYUSH (non-allopathy) systems of medicine . State’s public expenditure on heath remains very low at a meagre 0.87% of the state GDP. Therefore, individuals and households are burdened with high out-of-pocket (OOP) expenditures for health.81 The evidence on the effectiveness of the state’s response to curb high OOP expenditures on health in the form of social health insurance schemes is mixed.82 83 The few health system studies conducted, indicate serious health governance issues such as healthcare regulatory deficits, lack of accountability, corruption in health service delivery and variable quality of care in public and private health facilities in Karnataka.6 45 84
Case description
In June 2016, a group of rural women along with the support of a CBO staged a protest in the premises of a government health facility located in one of the subdistricts of Karnataka. They alleged that Dr X, who is not a gynaecologist, conducted unwarranted hysterectomies on many poor rural women between 2010 and 2016. The protestors complained that Dr X unnecessarily conducted hysterectomies on these women, that their age was misquoted in the discharge summaries and most women were not provided proper medical records for the surgery. They further alleged that the surgeon instilled fear and persuaded them to undergo the surgery. The women also claimed that the surgeon in connivance with a private pharmacy located opposite to the government hospital collected money to perform the surgeries. They demanded stringent action against the surgeon and monetary compensation. The District Health Officer (in-charge of the health district where the government hospital was located), as a follow-up to the protest, appointed a committee of medical and paramedical professionals to conduct a formal inquiry. The CBOs representing the aggrieved women felt that the district health authorities were attempting to hush up the case and so approached the then health minister. The group of poor rural women waiting to meet the health minister was widely reported in the print media. The issue was also debated in the state’s legislative assembly. Since 2016, the two CBOs along with the aggrieved women had approached various elected representatives, institutions at district and state level seeking redressal of their grievances. Following the petitions by the CBOs, state level authorities and elected representatives had visited the government health facility where Dr X worked. Dr X was suspended twice from the service. He was provided part of his salary during the suspension period. The suspension was not an outcome of the formal inquiry; it was rather a temporary measure pending disciplinary action on charges of dereliction of duty and misconduct levelled against Dr X. Further, the government requested the state medical professional council to cancel the practicing license of Dr X. The medical professional council on its own inquiry warned Dr X not to perform hysterectomies and warned him to practice within his competency. After a brief period of suspension, the surgeon was reinstated into service and was sent to a government health facility in another district of Karnataka. The CBO representatives continue to seek monetary compensation for the aggrieved women. They reported that their collective action was interrupted temporarily due to the COVID-19 pandemic.
The first author became aware of the case during her visits to the Karnataka State Human Rights Commission to get a general idea on various categories of health care related grievances as part of a study on patient rights implementation in health facilities. The media coverage of the case helped us to identify some participants for interviews. The participants identified other potential participants (ie, snowball sampling). We obtained documents and media articles (especially articles in Kannada, the regional language) pertaining to the case from the members representing the CBOs who supported the aggrieved women to pursue the case with various actors in Karnataka since 2016. Thus, there were three main data sources: (i) five key informant interviews, (ii) legal and administrative documents pertaining to the case and (iii) 35 media reports (labelled as MA-1–MA-35). We conducted interviews with members of two CBOs and a doctor who first reported the incident in the media. One of the two CBOs had around 50 members from the local community and the other CBO had around 1500 members from both local community and other districts of Karnataka. Both CBOs work on a range of community welfare issues. We also interviewed a member from another voluntary organisation which pursued a lawsuit on unwarranted hysterectomies reported in another state of India and a member from the health activist collective in Karnataka to get a broader perspective on patient rights and grievance redressal. We requested the members of CBOs and the doctors to describe the case as they know it and their perspectives on the different positions of the actors involved in the case. Each interview lasted for 30–45 min. Until we reached data saturation, we held four to five follow-up interviews with the members of the CBOs to clarify the sequence of events, collect and understand the case related documents and media reports and validate some facts pertaining to the case. Due to COVID-19 pandemic related restrictions, all other interviews except one were conducted via online platforms and phone calls. All interviews were audio-recorded, transcribed and translated. The details about the documents and media reports used are available in online supplemental file 1. We developed a detailed case description in Kannada, shared with the CBO representatives and sought their feedback. Media reports Kannada were also translated. MP analysed the content of the interviews, documents and the media reports and developed the initial coding manually. All authors discussed the emerging findings periodically. Using deductive and inductive approach, the major themes and subthemes were refined iteratively. All authors are qualitative researchers having experience in the field of health policy and systems research. The study is reported following the COREQ guidelines.41
Supplemental material
Patient and public involvement
The aggrieved care-seeking individuals were not involved in the design, conduct or reporting of the study. For data collection, we approached CBO members who represented and pursued the grievance with several public institutions on behalf of the collective of aggrieved care-seeking individuals. We have provided the key findings of the study and the detailed documentation of the case in Kannada to the CBO representatives. This could help the collective of care-seeking individuals and CBOs to reflect and plan their future course of action.
Ethics
We sought informed consent from all participants. The informed consent form provided information regarding the researchers, institutions involved, funding, purpose of the study, risks and benefits involved,research dissemination, and archiving plan. Some legal documents such as the case order from the Karnataka Medical Council and the lawsuit on Dr X from the High Court of Karnataka are available in the public domain.
Results
The governmentality space in grievance redressal is mainly defined by the medical profession and the State bureaucratic apparatus. We first describe the micropractices of the actors: the medical profession (individual medical professional and the medical professional council) and the State bureaucratic apparatus (state, district and subdistrict officials of the Department of Health and Family Welfare and other State institutions). We then show how the collective of aggrieved women along with the CBOs exhibited counterpower to redefine the governmentality of grievance redressal for patient rights violations. The themes and the subthemes are aligned with the theoretical framework (figure 1).
Dominant actors defining the governmentality of grievance redressal
Medical profession
Medicine is one of the most revered professions in India and often medical professionals are given a godly stature (MA-29, KII-5). One participant(KII 3) quoted:
“…doctor is the God; they are also called Gods who are visible to eyes”
In Karnataka, the state/district/subdistrict health authorities who deal with complaints received from the individuals seeking healthcare are usually medical professionals. The aggrieved women and the CBOs first approached the district health officer (DHO) (who is a doctor) to raise a grievance on Dr X of the government health facility. Following a protest by the affected women and CBOs, the DHO instituted an inquiry committee. The inquiry committee mostly comprised of medical professionals. Later at the state level, another inquiry committee led by a district magistrate(judge) was appointed. The CBOs and the media asserted that none of these official inquiry committees spoke to the affected women (KII-3, KII-4). With respect to this allegation, a media article (MA-18) reported that an official from the district health administration cited lack of time, non-availability of the contact details of the aggrieved women and chaotic situation at the hospital premises on the day of inquiry as reasons for not talking to the aggrieved women. In addition, the official was quoted in the same media article as saying ‘the DHO never asked us to probe whether the hysterectomies were unwarranted’. Further, the media article (MA-18) noted that the police complaint against Dr X filed by the district health office did not ask for an investigation on whether the hysterectomies conducted by Dr X were unwarranted or on the probability of medical negligence. District health authorities and the police maintained that as the investigation would proceed, relevant sections of the law will be invoked. The collective and the media questioned the fairness and credibility of the first formal inquiry by the district authorities. Yet, the High Court of Karnataka cited the completion of the formal inquiry against Dr X as the reason to reinstate Dr X and instructed the State to do so.42
KII-1, a medical professional and a health activist illustrates the underlying interest of the powerful medical profession in the grievance redressal processes that is, as devising ways to address the issue in such that it is not detrimental to medical power. KII-1 highlighted the need for diversity in the formal committees so that there is a better understanding of non-medical aspects of the grievances raised by care-seeking individuals.
“…the whole idea is not to address the issue at all. You form a committee of doctors who know nothing about social, cultural, economic and political issues, so they won't look at it; they won't address this and the problem…they should have some sociologists they should have an economist who has worked at the micro-level too. Understand voice and the concern of the women in what a petty condition the women are living in. So, this is just a farce setting up a committee, and you know, asking some doctors sitting in Bangalore(city) to do this it’s just a nautanki (gimmick)”
Like in many settings, the medical professionals in Karnataka are expected to self-regulate through an autonomous medical professional council. The media and the collective of aggrieved women problematised the act of Dr X as unethical, unwarranted and illegal. But the medical council problematised the act of Dr X as a matter of clinical incompetency. It warned Dr X not to perform hysterectomy surgeries as it is not within the scope of their competency. But the council was silent on the question, whether the women who already underwent surgery by Dr X are eligible for a remedy.43 In the words of a health activist (KII-5), the medical professional councils tend to be more protective of the medical professionals than of care-seeking individuals.
“It (medical professional council) is a quasi-judicial body. It is a court. There is a saying that the fence itself consumes the field. medical council is like that. It should give justice. It should establish professional practice, warn those medical practitioners who err, then it must regulate. Does any one of these is happening?”
Another participant (KII-2) highlighted the unwillingness of the medical community to discuss medical ethics related issues among themselves such as the hysterectomy case reported in this study. In their words,
“…a number of (medical) conferences take place every year and you don't come across a single session where such issues are discussed. These are often huge conferences, held in five-star hotels and in very exotic localities so a huge amount of money is spent and there is absolutely no self-criticism, self-analysis, course correction nothing of that kind.”
Thus, within the governmentality space for patient grievance redressal, the medical professionals possess substantial authority at district and state level. Furthermore, institutions such as the medical professional council reaffirm medical power through the State bureaucratic apparatus and used its discretionary powers while dealing with grievances raised by care-seeking individuals. Combined with political influence, the power of the medical profession further gets strengthened in ways that can shape the course of formal grievance redressal processes often in favour of the medical profession.
Bureaucracy
At different points of time or at times parallelly, at least 11 institutions dealt with the grievance raised against Dr X (figure 2). Some of the statutory institutions meant for grievance redressal are geographically inaccessible for poor women living in a rural setting. See, for example, the Karnataka State Human Rights Commission, Karnataka Medical Council, Karnataka State Commission for Women which are all exclusively in Bangalore, the state capital without any outreach office elsewhere in the state. For follow-up, the aggrieved women and the CBO representatives had to travel 300 km. In addition, most of the women who underwent surgery were illiterate and poor. The social worker Mr N (KII-3) who petitioned on behalf of the aggrieved women said:
“out of all the people with me I am the only educated and informed person. Even to draft a letter I alone have to do it”
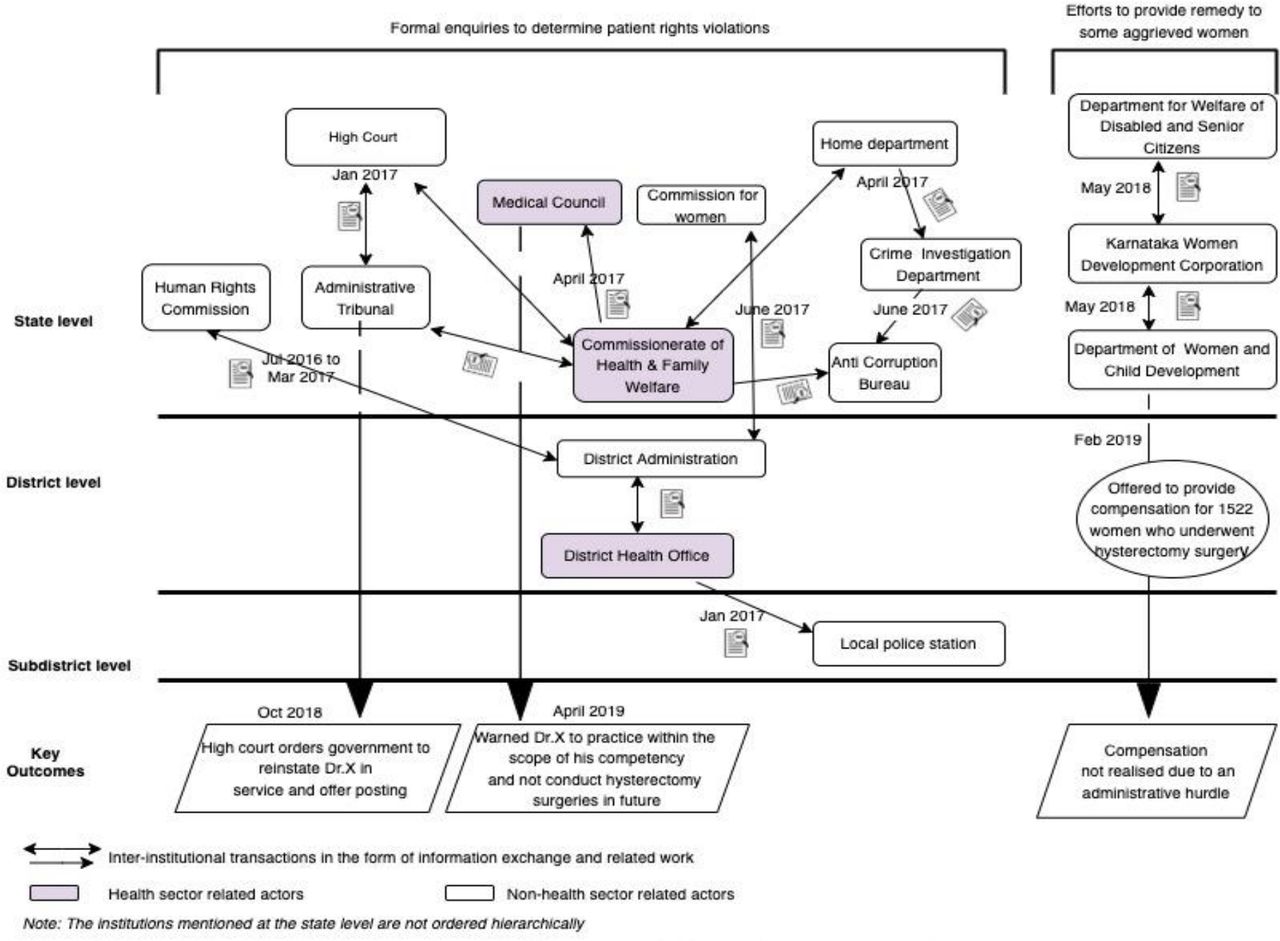
Scheme showing the outcomes of bureaucratic maze, administrative delays and siloed bureaucratic action on the grievance raised against Dr X.
All actions of the bureaucrats are supposed to be bound by law. Yet, there were a series of administrative delays and the case got mired in complex bureaucratic procedures. The case also exemplified siloed bureaucratic thinking and action (figure 2). For instance, the anticorruption bureau was examining whether Dr X collected bribes from the women who underwent hysterectomy. On the other hand, the state human rights commission was enquiring if any action was taken by the state and district authorities on the grievance raised. Meanwhile, the Karnataka Administrative Tribunal and the High Court of Karnataka examined if it was necessary to suspend Dr X from service necessary and whether the government followed due procedures while passing the order to suspend Dr X. The progress of the legal cases against Dr X is unknown to the collective who raised the grievance. Follow-up inquiries and visits by the collective to the police yielded no response (KII-3, KII-4).
In the bureaucratic maze, the answer to the key question whether Dr X conducted unwarranted hysterectomies and collected bribes from the aggrieved women remains unclear. The collective assert that Dr X had conducted more than 10 000 hysterectomy surgeries between 2010 and 2016. But the suspension order of Dr X records 530 hysterectomy surgeries between 2013 and 2016. The discrepancy in the number of hysterectomies reported by the dominant actors and subjects (aggrieved care-seeking individuals) appears to symbolise the gravity of the issue to them. Nonetheless, after almost 3 years, the State came forward to offer some compensation in the form of a special employment programme to 1522 aggrieved women. However, the administrative procedure stipulated the aggrieved women to get a medical certificate from the administrative head of the concerned government health facility which was perceived as a major hurdle. Only 60–70 women (approximately 5% of those who were assured compensation) were able to get the certificate and at the time of writing this paper, the women still await the assured compensation.
In summary, procedural and substantive justice did not accrue to the collective of aggrieved rural woman due to labyrinthian bureaucracy hampering access, undue administrative delays and fragmented bureaucratic thinking and action on the grievances raised. Further, the bureaucracy adopted a biased approach by not providing an opportunity for the aggrieved women to assert their rights during the formal grievance redressal processes. A lack of transparency was apparent in the formal grievance redressal processes.
Efforts of the collective of care-seeking individuals to redefine the governmentality of grievance redressal
The collective of aggrieved women was dissatisfied with the way the grievance against Dr X was handled. Therefore, in pursuit of procedural and substantive justice, the collective with the support of two CBOs employed microprocesses and techniques such as protests, media engagement, approaching multiple actors, follow-up inquiries and visits to counter the dominant medical and bureaucratic power.
Protests and mass gatherings organised by the collective
The following quote illustrates the use of protests and mass gatherings by the collective as the key strategies to have their voices heard.
“For the work to happen we have to protest. This is like crying baby gets the milk. Once we start making sound, the government feels that we are taking trouble to them” (KII-3).
But participating in the protest is not without risk. The State filed a police case against a CBO member who played a prominent role in the protests against Dr X. The State alleged in its litigation that the CBO member obstructed public movement and breached public peace. After 2 years of legal battle, the local court acquitted the CBO member of all charges citing that the failure of the prosecution to prove the guilt beyond reasonable doubt.44 The members of the CBOs (KII-3, KII-4) maintain that the legal case proceedings were an effort to muzzle their voices.
Initially, a CBO spearheaded the protests/mass gatherings in the premises of the government health facility to bring pressure on the authorities to act on the grievances raised against Dr X. This had an impact, as the then DHO assured in the presence of journalists that a formal inquiry committee would be set up (MA-14, MA-15). Meanwhile, media covered the social worker Mr N along with 20 aggrieved women was seen waiting in front of the iron gates of the state legislature to meet the then health minister for more than 12 hours (MA-13). When the administrative medical officer of the government health facility hesitated to issue the medical certificate for the aggrieved women, the collectives held a hunger strike (MA-26, MA-33, MA-34). Following that, the local elected representative facilitated a meeting between the collective and the district administration to discuss the issue (MA-30).
Media engagement
The media played a major role. The collective submitted the media reports on Dr X in their petitions to appraise the seriousness of the issue to the government authorities and institutions. The collective held press meets to highlight their demands with respect to the case of Dr X. Furthermore, the media highlighted the physical and psychosocial effects of the surgery on the aggrieved women and their families (MA-9, MA-13, MA-19, MA-11).
Many media articles explained the allegations against Dr X by the aggrieved women (MA-9, MA-19, MA-2, MA-11, MA-13, MA-10). Media articles drew attention on the acts of procedural injustice such as the biased inquiry of the formal committee set by the district health authority (MA-2, MA-14), efforts to muzzle the voice of collective using laws and legal actions (MA-33), (indirect) support rendered to Dr X (MA-2, MA-24), administrative delays, (MA-34, MA-35), administrative hurdles to avail remedy (MA-18, MA-26, MA-33, MA-34), lack of transparency in the grievance redressal processes, evasion of responsibility by the state institutions (MA-18) and state privileges enjoyed by Dr X even during their suspension (MA-22).
In one media article, health activists critiqued the state government’s ‘shoddy’ response to similar allegations of unwanted hysterectomies in other parts of Karnataka. Media reported that the collective of health activists was surprised because a committee formed by the government admitted to unnecessary hysterectomies but did not punish the guilty and compensate the victims (MA-16). The media also portrayed the affective, emotive and the moral dimensions of the grievance raised by the collective against Dr X (box 3).
Moral beliefs and attitudes on the grievance raised by the collective (as reported in the media).
None of the formal inquiry committees provided opportunity to the aggrieved women to explain their grievances. But the print media gave the required space and time to the collective to air their grievances on Dr X. The media narratives examined the grievances raised against Dr X from a moral point of view.
Dr X’s act was portrayed as “medical avarice”’; “barbaric act” (MA-11); “shameful …inhuman act” (MA-2, MA-29); “heinous act” (MA-2);“dereliction of duty”(MA-21) and “bad act” (MA-12, MA-13, MA-20, MA-23, MA-28).
The hysterectomies done by Dr X on the rural women were indicated as “unwarranted, unwanted, and illegal” (MA-12, MA-13, MA-18, MA-20, MA-23, MA-25, MA-26, MA-28, MA-30, MA-33, MA-35).
Further, it was reported that such incidents reveal “the ugly face of the private healthcare creeping into the government health system”(MA 11); Few other media articles reported “socioeconomically backward women victimised due to the bad act of Dr X”; “unwanted hysterectomies done due to greed on money” (MA-12, MA-13, MA-20, MA-23, MA-28); “Dr X was thirsty for money” (MA-6); “the doctor collected unauthorised money from patients on the pretext of conducting surgeries” (MA 14); “Dr X fleeced poor patients” (MA-14, MA-15, MA-17); “Dr X cheated the women” (MA-28); and“the women were subjected to injustice” (MA-6). When Dr X was suspended from the service, the collective expressed that “it’s a honour for justice” (MA-25).One media article stated “innocent women lost money and health but Dr X collected crores of money and leading a luxurious life” (MA-35). “Dr X name is a dreaded one in villages” quoted one media article (MA-22).
Mostly, the collective and at times some elected representatives expressed the need for monetary compensation for the (aggrieved) women (MA-9, MA-18, MA-19, MA-26, MA-28, MA-30, MA-33, MA-3, MA-2) and demanded that Dr X to be imprisoned (MA-19, MA-2).
Thus, the media predominantly favoured the collective, attempted to expose the deceptive practices of the medical profession and the bureaucracy, and invoked moral arguments on the grievance raised against Dr X.
Approaching multiple actors
The collective made several petitions to elected representatives and State institutions (figure 3). The collective had included medical literature on indications for hysterectomy in their petition to the Karnataka State Human Rights Commission to show how Dr X deviated from the normal standards of medical care. This can be seen as an attempt to counter medical power (medical knowledge is one of the key instruments of power used by the medical profession).
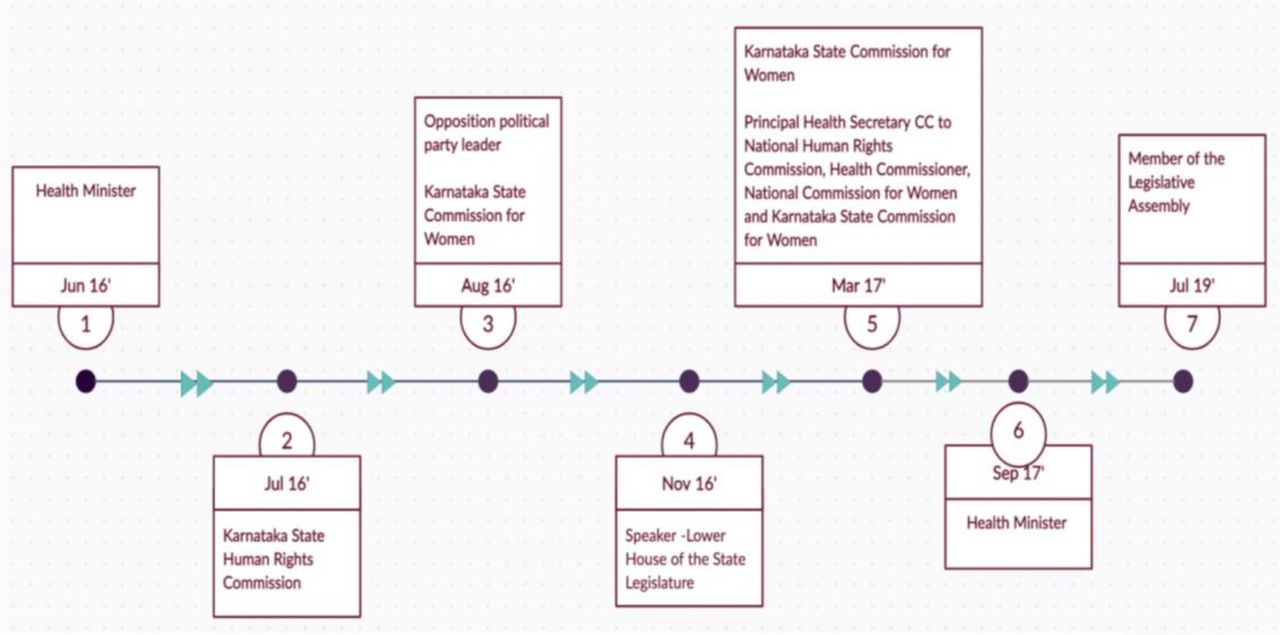
Timeline of the petitions made by the collective to various State actors.
Garnering support from elected representatives
The CBOs representing the affected women often sought the support of the elected representatives belonging to both opposition and ruling parties to intervene and ensure justice for the aggrieved women. It was partly because of the then leader of opposition in the legislative assembly of the state, the issue got the spotlight in the state legislature and was debated, following which Dr X was suspended from service for a short period. Every time the collective met the elected representatives, they were assured that Dr X would be sanctioned and the women would be compensated.
Nonetheless, the bureaucracy was more powerful than the representative political power in this case. This was evident with the health minister and the leader of opposition expressing their frustration in legislature over the revocation of suspension order against Dr X (MA-10).
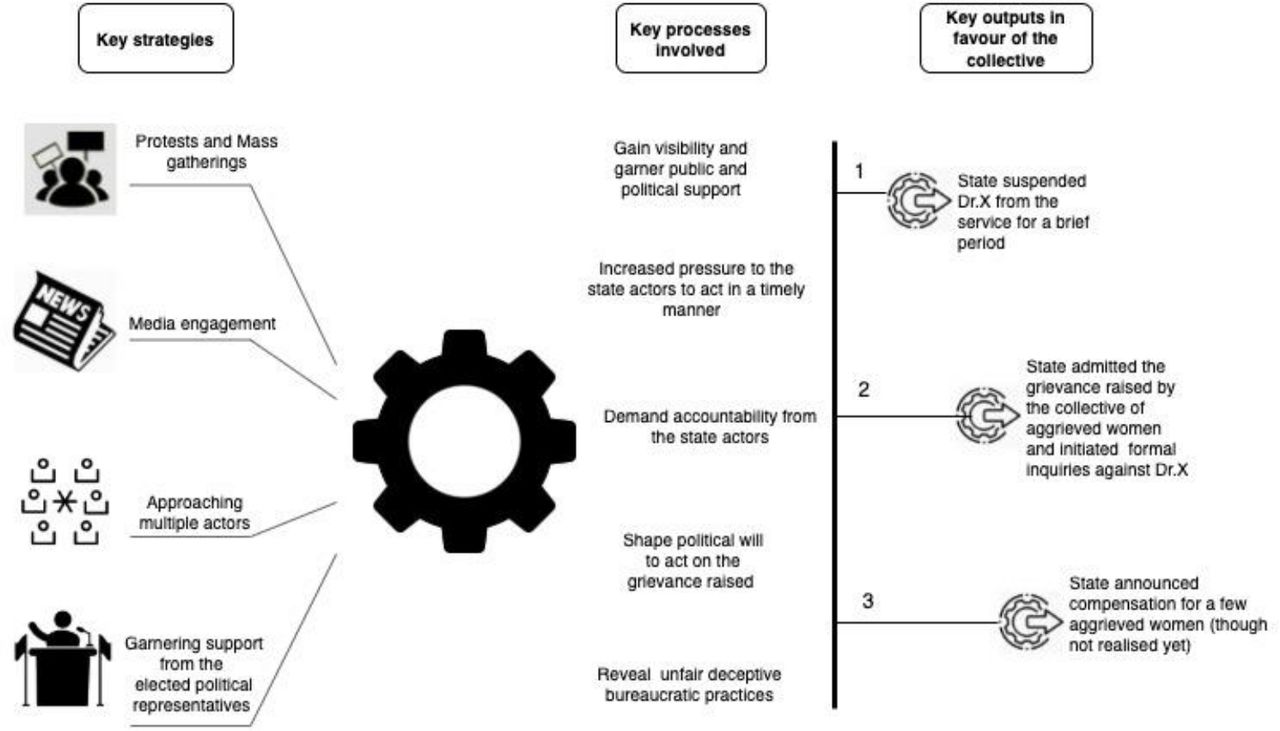
The countermeasures such as the protests, media engagement, approaching multiple actors and institutions and garnering political support were successful in terms of providing visibility to the issue and highlighting gaps in the grievance redressal that deterred or denied procedural and substantive justice to the aggrieved women (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Key strategies, processes and outputs of the collective action of the aggrieved women on the grievance raised against Dr X.
Discussion
Hysterectomy in the historical sociopolitical context
The praxis of governing (governmentality) occurs within a specific context. It is important to situate the alleged case of unwarranted hysterectomy among the rural women used in the broader historical and sociopolitical context of India. Indeed, the case reported in this research is not a single event. Media articles and research studies show unwarranted hysterectomy surgeries conducted even in young and premenopausal women in several districts of India.45–52 The factors driving high prevalence of hysterectomy include poor quality of sexual and reproductive health services for women, female illiteracy, myths surrounding menstruation, public attitude towards family planning and usefulness of uterus as an organ after menopause, lack of knowledge on the side effects of hysterectomy and misuse of health insurance.53 54 Other factors such as the profiteering motive of the hospitals, unethical medical practices and an inefficient healthcare regulatory environment lead to rising number of hysterectomy cases in India.45 47 High prevalence of hysterectomy was associated with female illiteracy, women’s employment, rural residency, higher age and parity, caesarean section and higher wealth status among women aged 15–49 years.53 In this case study too, we find that mostly illiterate rural women belonging to marginalised communities reported unwarranted hysterectomy.
Contrary to standard treatment guidelines, hysterectomy is used as a treatment option even for benign medical conditions such as excessive menstrual bleeding.55 56 Women who receive hysterectomy tend to be younger in India. Some studies reported that hysterectomies in India are conducted at an average age of 29 years (rural Andhra Pradesh)57and 36 years (Gujarat)50 whereas in high-income settings such as Denmark, USA and Australia, women undergoing hysterectomy are aged between 44 and 54 years56 58 59 . Prusty et al53 showed the association between high prevalence of hysterectomy and permanent family planning method for women (sterilisation). They hypothesise that hysterectomy was replacing sterilisation. The historical global health agenda for population control has in part contributed to women in India having to be shouldered the burden of family planning and contraception. Family planning programmes have excessively relied on female sterilisation to attain fertility goals in India. In 1976, when the government turned its family planning strategy towards men, it experienced a major backlash and was voted out of power.60 Ever since, women continue to be easy targets for population control through sterilisation procedures in India.55 High prevalence of hysterectomy is a major concern in some high income country settings as well.56 58 59 Some scholars and activists in literature posit that hysterectomy is a “hoax”61 and reflects a culture of providing irrational medical care to women and profit motive of medical establishments.45 62–64 In addition, deep-rooted gender inequities in India can explain partly the apathy towards grievances on patient rights violation raised by a collective of aggrieved women such as the one reported in the current study. India ranked 140 among 156 nations in gender equality. In health and survival sub-index of gender equality index, India is one among the bottom five countries.65
Exposing (hidden) power-the governmentality way
The governmentality perspective brings the power contestations to fore through hidden processes and techniques employed by the medical profession, State bureaucratic apparatus and the collective of aggrieved care-seeking individuals during grievance resolution.
First, collective action was necessary by the aggrieved women in terms of protests, media engagement, petitions and engagement with several actors and State institutions to ensure that the patient grievance redressal system accepted a complaint against a medical professional.
Second, even when the grievance was considered admissible, each institution especially the medical professional council exercised its power by problematising the grievance in its own way different from the problematisation of the grievance by the collective. Historically, self-regulation in medical profession is formally institutionalised through the establishment of professional councils. Thus, the problematisation of the grievances and the remedy prescribed by the medical professional council appeared credible and legitimate in this case.
Third, the medical profession wielded power through a wide range of control techniques. We indicate the most significant ones among them. The medical professionals held legitimate key administrative positions in the grievance redressal system at all its levels. The medical professionals of the first formal inquiry committee set up by the district health authority (a medical professional) justified their decision not to talk to the aggrieved women citing reasons such as non-availability of the address of the aggrieved women, time constraints and orders of the higher authority. Further, the medical professional council had a legal mandate (cf. the Karnataka Medical Registration Acts and Rules 1961–2019)66 to critically examine if the conducted hysterectomies were medically unwarranted, yet it refrained from doing so. These illustrate the passive use of bureaucratic power to safeguard the reputation of the medical profession at any cost. In this case, there is a deep- seated solidarity logic among the medical profession keeping its members at the risk of being ostracised if behaving otherwise. This logic could be driving the defensive behaviour among medical professionals and the medical professional council when it comes to redressal of the grievances raised by care-seeking individuals. In line with the findings of this study, the medical profession has been criticised for abusing its privileged status and using ‘collegiality’ in the name of self-regulation as a means to protect incompetent and unethical practices.67–71
Fourth, the power of bureaucracy was enacted through two main strategies: (i) creating a maze of organisational units to deal with grievance and (ii) fragmenting the grievance across bureaucratic units. The collective had to shuttle between several actors at the district, state and national level to get their grievance heard. Different bureaucratic units dealt with different aspects of the grievance raised by the collective. The fragmented approach enabled the bureaucratic units to shirk responsibility by allowing one unit to attribute administrative delays to another bureaucratic unit. The bureaucratic units also exercised their power through both action and inaction. See, for instance, the police institution’s promptness in investigating the case filed against a CBO member who spearheaded protests in the government health facility which came to a logical conclusion in the court of law. But the same promptness was not evident in investigating the case filed against Dr X. In addition, opaqueness of internal administrative procedures, undue administrative delays and biased approach in the inquiry display the hidden power of the bureaucracy at work compromising procedural justice in grievance redressal processes.
The aggrieved women together with the CBOs challenged the existing governmentality through their collective efforts in the form of protests, media engagement, petitions to several institutions and actors. The resistance was successful in terms of getting the attention of the bureaucracy and the elected representatives on their grievance, resulted in the suspension of Dr X for a brief period, and pressurised the state to award compensation (though had not materialised at the time of writing due to bureaucratic hurdles and fluctuating political will). The collective also employed indirect techniques of power possible within their social field of action, such as citing medical expertise in the form of literature on hysterectomy in their petitions; invoking moral implications of the acts of Dr X using emotive and affective language in media reports, petitions, and during protests; relentlessly following up with State actors and institutions and mustering support from elected representatives and media. Interestingly, for the care-seeking individuals, getting trapped in a bureaucracy is like being in an endless loop. However, the collective used the same maze to pressurise the State actors to act on the grievance and demand accountability.
Thus, the contestations in the governmentality space are inherently political in nature and marked by moments of winning and losing for the actors. However, an array of practices deployed by the medical profession and the bureaucracy in particular served to ultimately gain and maintain power over the governing practices and outcomes of grievance redressal. The domination by the medical profession and the bureaucracy compromised procedural justice in the formal patient grievance redressal processes. When procedural justice is not ensured, substantive justice of achieving equality and dignity in the outcomes especially for the care-seeking individuals through grievance redressal policies is doubtful.
(De) linking rights and remedy
Principally, in human rights, jurisprudence establishing (patient) rights violation is a prerequisite for awarding a remedy that is proportional to the nature and the severity of rights violation.72 A maze of actors dealt with the grievance raised by the aggrieved women and CBOs. Yet, the formal grievance system failed to arrive at an official verdict about whether Dr X violated the rights of the aggrieved women. The nature and the severity of patient rights violation is not formally established in this case. Nonetheless, there were episodic, although unsuccessful attempts outside the formally established system and its procedures to award remedy to the aggrieved women in the form of employment opportunities. The constitutions and the legal systems emphasise the importance of remedy if the right(s) are violated. On the contrary, the case used in this analysis exemplified how the governmentality of the grievance redressal system as shaped by the medical profession and the bureaucracy counters the possibility of reaching a verdict in the case whether a right was infringed or not.
Limitations
We could not interview the elected representatives and bureaucrats who dealt with the alleged unwanted hysterectomy case or Dr X as they were either unavailable or were not accessible to researchers. Instead, we relied on data sources such as documents, lawsuits and media reports to explore their perspectives and insights on the actual proceedings on the case until the time of writing this manuscript. The current data set does not capture the internal power dynamics of the collective of the aggrieved women with(in) the CBOs. We acknowledge that these dynamics could also shape the governmentality space. One might question if the power dynamics illustrated using the critical case of patient rights violations represent the grievance redressal processes in a typical case (where an individual care-seeking individual or their family members approach the system seeking remedy for their rights violated in the health facilities). We argue that despite the collective efforts of the care-seeking individuals, the case of alleged patient rights violations did not arrive at a conclusion in the existing grievance redressal system and the grievance against Dr X continues to fester. That being said, the critical case of patient rights violation reported by the collective would be a gross underestimation of the power struggle in a typical individually focused case. Also, the power dynamics might play out differently for grievances raised against other cadres of health professionals such as nurses, lab technicians, occupational therapists and so on.
Implications of the study
We recommend two important governance reforms to counter the pathologies identified in the existing governmentality of patient grievance redressal in Karnataka. (i) In the short-term, the formal inquiry committees set up for grievance redressal should comprise of a mix of representation including non-medical personnel, lay communities and civil society organisations. The benefits of such a representative committee are twofold. First, it could address the medical hegemony in the governance processes of grievance redressal. Second, it could enable examination of non-clinical aspects of patient rights violations. (ii) As a long-term solution, a major governance requirement is to have institutional arrangements that consolidate multiple grievance redressal processes under a single organisational unit or agent. Indeed, the Indian judiciary is available as the single organisational unit to deal with the healthcare-related grievances. However, the Indian judicial system deals with all kinds including healthcare related grievances. It is often criticised for delays in the dispensation of justice owing to poor infrastructure, manpower shortages, complexity in the procedural laws and various other challenges.73 Therefore, we recommend a single organisational unit that is exclusive for healthcare related grievances and truly representative of multiple stakeholders and not just the members from the medical and healthcare profession. Further, the single organisational unit should be cascaded to district and subdistrict levels to enable care-seeking individuals to access formal grievance redressal systems. Such an arrangement will significantly reduce administrative delays, transactional costs and facilitate comprehensive examination of grievances raised by care-seeking individuals. But enabling physical access without ensuring the measures for procedural justice is meaningless. Procedural justice in grievance redressal systems for patient rights violations requires accountability, transparency, promptness, fairness, trustworthiness and credibility. If this happens, then the justice of outcomes (ie, substantive justice) such as equality and dignity for all individuals (and not just for the elites) is reified.
In the eyes of medical profession, engaging non-medical personnel in grievance redressal processes is seen as ‘external regulation’ which is often challenged by the medical profession.74 Nonetheless, in the wake of wide access to medical information, increasing frequency of medical negligence reports, accountability demands and complexity of healthcare provision, many European countries and Australia have introduced external regulation as one of the tiers of professional regulation and it is often linked with wider healthcare quality.75 76 In some settings such as UK, cases of serious professional misconduct are subjected to open public hearing.77 Such measures are efforts to put in place adequate checks and balances so that no one actor becomes too powerful in the grievance redressal systems.
At a theoretical and abstract level—governmentality as a framework enabled not just to study how subjects (care-seeking individuals) are rendered governable but also the opportunities and constraints of the subjects to subvert dominant forces that shape the patient grievance redressal processes and practices. Even organised forms of collective action cannot always result in success always. A crying baby may not always get the milk. Nevertheless, the governmentality analysis indicates to the labour of innovation, courage and commitment required by those who struggle to redefine the (unjust) governmentality.
Conclusion
The governmentality lens was helpful to explore the many manifestations of power by examining the actual micropractices ordering actor(s)’ behaviour within the patient grievance redressal system. It also exposed invisibilised power dynamics, especially of the medical professionals and of the bureaucracy in the name of standard operating procedures in grievance redressal. The Indian medical profession, through its social status, administrative positions and legitimate institutional machinery (eg, medical professional council) to a large extent determined the outcomes of the grievance redressal concerning patient rights violations reported in Karnataka. Political clout augmented medical power. Centralised locations of public institutions (ie, medical professional councils, human rights commission, women commission) and standard operating procedures are an indirect display of power as they render the institutions of grievance redressal physically and psychologically inaccessible to certain population. Further, the bureaucracy through the maze of institutions, its discretionary power, fragmented bureaucratic action, sometimes its inaction and opaque inquiry processes made the quest for remedy more elusive to the aggrieved care-seeking individuals. The collective efforts of the aggrieved rural women attempted to redefine the governmentality of grievance redressal yet with little success. The study provides evidence for the need to assure procedural and substantive justice in formal grievance redressal processes for patient rights violations in health facilities in settings such as Karnataka.
Supplemental material
Data availability statement
Data are available in a public, open access repository. Data are available on reasonable request. Some data are available in the public domain. Remaining data is available on a reasonable request to the authors.
Ethics statements
Patient consent for publication
Ethics approval
The study obtained ethical clearance from the Institute of Tropical Medicine, Antwerp, Belgium (study ID-1429/20) on 01/10/2020 and the Institute of Public Health, Bengaluru (study ID—IEC-ER/04/2020) on 16/10/2020. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank Dr B N Prakash for his administrative support in carrying out the PhD project. We are grateful to all the participants of the study who enthusiastically participated and made this project possible. We also thank the organisers and participants of the write-shop held at the Institute of Public Health, Bengaluru for providing feedback on the initial drafts of this manuscript. We thank Praveen S Rao for his help in graphic designing of the figures. We have provided author reflexivity statement in the online supplemental file 2.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Valery Ridde
Twitter @prashanthns
Contributors MP contributed to planning, conduct, analysis and reporting of the study. AK, NSP, NE, BC and SVB contributed to planning, analysis and reporting of the study. MP takes the responsibility for the overall content as the guarantor.
Funding This work is supported by the PhD fellowship offered to MP by the Institute of Tropical Medicine, Antwerp, Directorate general of Development Cooperation, Belgium. The time and the contributions of PNS for this project are supported by the DBT/Wellcome Trust India Alliance Intermediate Clinical and Public Health Research Fellowship awarded to him (IA/CPHI/16/1/502648). SVB is supported by FWO senior postdoctoral fellowship (1221821N).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The reflexivity statement for this paper is linked as an online supplemental file 2.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.