Article Text

Abstract
Lack of context-specific evidence and inadequate evidence-use for decision-making contribute to poor health. This paper reports on our work aimed at addressing the knowledge translation (KT) gap between evidence generators and users. We present our experiences of strengthening KT via technical advisory groups (TAGs) in parallel with increasing evidence generation through research fellowships and operational research. Vectorborne diseases (VBDs) impose substantial health and economic burdens in sub-Saharan Africa despite being preventable with vector control. The Partnership for Increasing the Impact of Vector Control aimed to reduce the burden of VBDs in Burkina Faso, Cameroon, Malawi and at regional and global levels. TAGs can promote evidence-use in policy and practice by engaging relevant stakeholders in both research and policy processes. TAGs and related activities are best facilitated by a coordinator with skills in research and policy. Contextual factors should influence the design and governance of TAGs, which will likely evolve over time. Relevant national stakeholders should be included in TAGs and be actively involved in developing research agendas to increase the relevance and acceptability of research findings for decision-making. The countries present three differing contexts with longer-term research and evaluation necessary to draw lessons on impact.
- Control strategies
- Public Health
- Health policy
Data availability statement
Data that support the findings are available within the article and supplementary materials, or from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Knowledge translation platforms promote interaction between evidence generators and evidence users, helping to increase evidence-use in policy and practice.
A multicountry programme to establish knowledge translation platforms for vectorborne disease control in three countries resulted in similar but distinct and evolving models.
Enabling researchers to identify key stakeholders, develop effective communication strategies and engage evidence users requires ongoing investment from early career stage.
Knowledge translation platforms can leverage national research capacity and deliver operationally relevant research and evidence.
Knowledge translation platforms can be combined with capacity strengthening initiatives to close the ‘know do’ gap and develop the next generation of influential research leaders.
Introduction
The global challenge of evidence-informed policy-making in health is perpetuated by the gap between researchers and policy-makers.1 2 Knowledge translation (KT) addresses this gap by promoting interactions that encourage policy-makers’ responsiveness to research and researchers to conduct policy-relevant research.3 The WHO supports global KT efforts through the Evidence-informed Policy Network that encourages countries to establish KT platforms (KTPs).4 For example, platforms such as immunisation advisory groups have been instrumental in influencing immunisation country policy changes through evidence promotion.5 Specific to vector control (VC), the WHO developed the Global Vector Control Response to guide the implementation of VC through stakeholder integration and evidence-use.6
This paper reports on experiences from a multicountry partnership aimed at setting up platforms for increasing evidence-use in national policy-making for vectorborne diseases (VBDs). We explored how context and targeted capacity strengthening efforts in policy engagement and evidence uptake shaped the establishment of Technical Vector Control Advisory Groups (Groups) as KTPs in Burkina Faso, Cameroon and Malawi.
Background
VBDs such as malaria and dengue remain major public health problems, especially in sub-Saharan Africa.7 Many of these diseases are preventable through VC,8 but implementation challenges remain: vertical administration of some VBD programmes results in duplication or conflict of activities and resource wastage,9 10 and a lack of support for evidence generation and use resulting in ineffective VC.11
In 2017, collaborators from the global south (Burkina Faso, Cameroon, Malawi) and north (UK) established a 5-year research programme called Partnership for Increasing the Impact of Vector Control (PIIVeC) (www.piivec.org) with funding from UK Research and Innovation Global Challenges Research Fund. The PIIVeC goal was to reduce the VBD burden through effective, locally appropriate and sustainable VC supported by locally generated evidence. The collaborating institutions included: Centre National de Recherche et de Formation sur le Paludisme (CNRFP) (www.cnrfp.bf) and Institut de Recherche en Sciences de la Santé (http://irss.bf/) in Burkina Faso; Centre for Research on Infectious Diseases (CRID) in Cameroon (https://crid-cam.net/); Malaria Alert Centre of the College of Medicine (MAC-COM) in Malawi (http://mac.medcol.mw/); the African Institute for Development Policy (AFIDEP) (www.afidep.org); and, Liverpool School of Tropical Medicine in the UK (https://www.lstmed.ac.uk/).
During preproposal needs assessment, southern partners’ responses to four questions (box 1) informed development of the programme and theory of change (figure 1: top panel). The theory of change comprised four streams: (1) individual capacity; (2) institutional capacity; (3) evidence base and (4) KT, delivered through five integrated work packages (WPs) (figure 1: bottom panel).
Key questions posed during needs assessment phase
How much dialogue exists between different VBD control programmes and how can it be strengthened?
What is the best way to strengthen partnership between researchers and national programmes?
What are the main obstacles to individuals developing a research career in vector biology?
What are the priorities for strengthening the support structures in your institution?
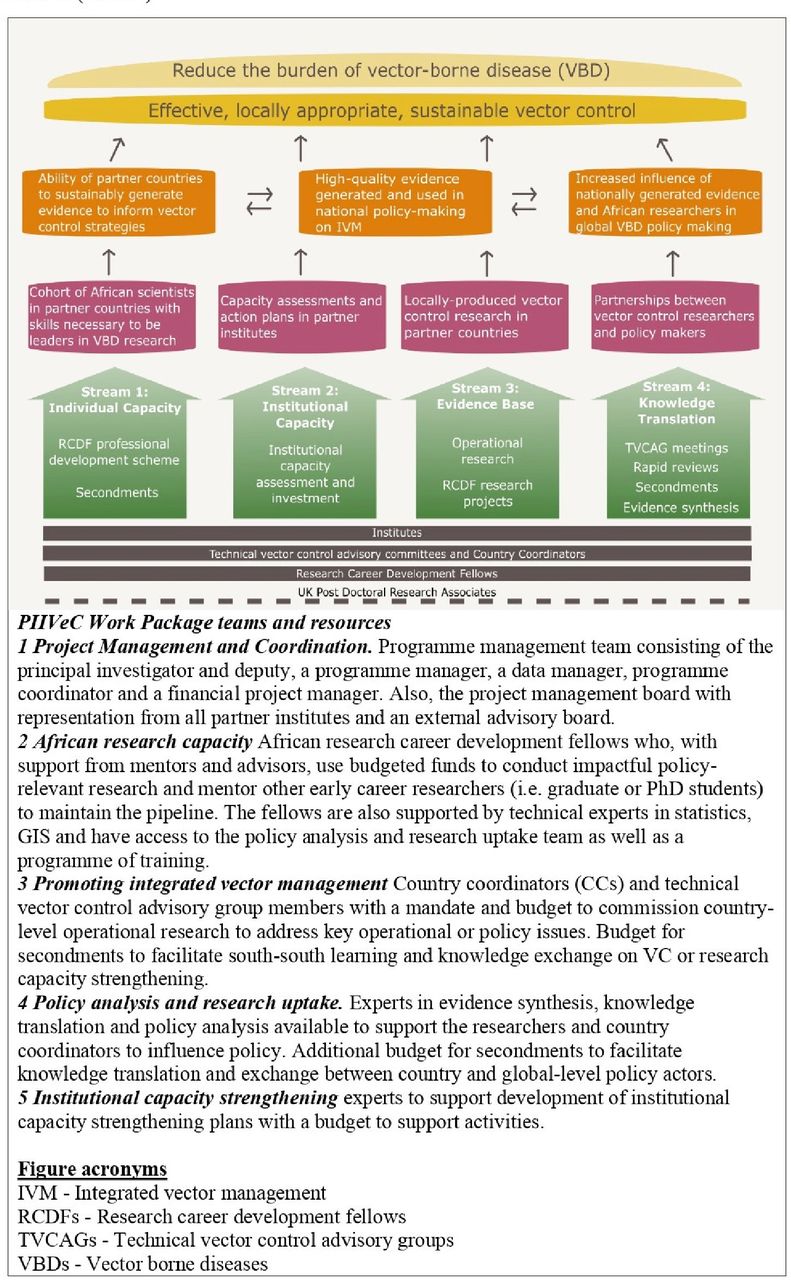
Theory of change and resources for Partnership for Increasing the Impact of Vector Control (PIIVeC).
We report on our experiences focusing on activities to increase the evidence base (stream 3) and enhance KT (stream 4) that were supported by the policy analysis and research uptake (WP4) team. We also describe a south-south engagement unit that emerged alongside programme implementation. We had intended to report on the impact of these efforts, however, the combined impact of COVID-19, and UK government cuts to overseas development assistance funding,12 which directly affected our programme duration, meant that we were unable to do so. Lessons from the professional development scheme (stream 1) and institutional capacity strengthening (stream 2) use a different theoretical framework and have been evaluated across multiple consortia, hence will be reported elsewhere. Figure 2 provides a Gantt chart of the PIIVeC planned and actual timelines for key activities.

Timelines of PIIVeC planned versus implemented activities. PIIVeC, Partnership for Increasing the Impact of Vector Control.
Knowledge translation
Technical VC advisory groups
PIIVeC appointed country coordinators (coauthors SN’f, FN and TM) who facilitated the establishment of technical VC advisory groups (groups) in each country. The primary objective of these groups was to share evidence and advise Ministries of Health (MoHs) and other stakeholders. The groups brought together relevant stakeholders, such as researchers, policy-makers and programme managers, to share experiences, collaborate, set research agendas and serve as KTPs. Hence, the coordinator position demanded skills in policy engagement, knowledge of the MoH, and VBD programmes and VC. Country-led recruitment processes for the coordinators were expected to be completed within 5 months (from November 2017), but took 10 months in Burkina Faso and Cameroon, and 12 months in Malawi. Burkina Faso recruited an influential government employee from within the MoHs Malaria research centre (CNRFP) as the coordinator. In Malawi, the lack of a suitable candidate resulted in the PIIVeC Malawian coinvestigator, affiliated to MAC-COM, doubling as a coordinator with additional administrative and programme management resources drafted in to support the increased workload. Cameroon opted to appoint a full-time coordinator, with an additional part-time deputy and a (consultant) programme advisor to provide a strong link with MoH.
Stakeholder analysis and engagement
Once appointed, coordinators initiated in-country desk-based stakeholder analyses guided by an analytical tool developed by the WP4 team (online supplemental appendix 1). The tool identified actors, with interest in VBDs, for engagement and potential group membership, and was intended to be continuously updated as stakeholder roles evolved, or when new stakeholders were identified.
Supplemental material
The preliminary Cameroon and Malawi analyses were available for review during a policy engagement and evidence uptake training, in October 2018, facilitated by AFIDEP. The interactive 5-day face-to-face training developed the coordinators’ and Research Career Development Fellows’ (fellows are described under the ‘Evidence generation’ section below) policy engagement skills to support KT. Coordinators presented preliminary analyses and discussions led to important revisions to the number and range of stakeholder institutions suggested for inclusion in the advisory Groups. While a formal analysis was not conducted in Burkina Faso, the coordinator verbally shared group plans.
The process of developing policy engagement strategies also started during the training. The strategies defined and documented plans to target key stakeholders with relevant evidence to aid KT. This was an iterative process led by the coordinators and supported by the WP4 team, who developed a tailored strategy framework to capture the objectives, stakeholders, engagement activities and monitor progress against indicators. The process was conducted alongside the groups’ establishment, with strategy documents being produced after seventeen months in Burkina Faso and Cameroon, and 10 months in Malawi. As with the stakeholder analyses, the strategies were supposed to be living documents and updated in response to new or evolving priorities.
Group governance, scope, structure and membership
Governance and scope are important in determining power and support. For effectiveness and sustainability, we envisaged that MoHs would govern the Groups. During implementation, Burkina Faso and Malawi retained the idea of MoH governance. However, in Cameroon, the group was established under the governance of CRID (a non-governmental research centre), guided by a memorandum of understanding with the MoH. This decision was primarily driven by previous lack of support to similar groups within MoH while the good relation between CRID and MoH made the arrangement plausible. Burkina Faso and Malawi had pre-existing exclusively malaria National VC technical working groups (VC TWGs) led by the National Malaria Control Programmes which offered the potential to expand their scope to cover other VBDs, rather than setting up entirely new Groups. In Malawi, 12 stakeholder consultation interviews were conducted (by coauthor CAM) to inform this decision. The findings highlighted concerns that simply expanding the malaria VC TWG risked malaria continuing to dominate the agenda. Hence, Malawi and Burkina Faso (for similar reasons) opted to create standalone groups to provide neutral platforms for all VBDs.
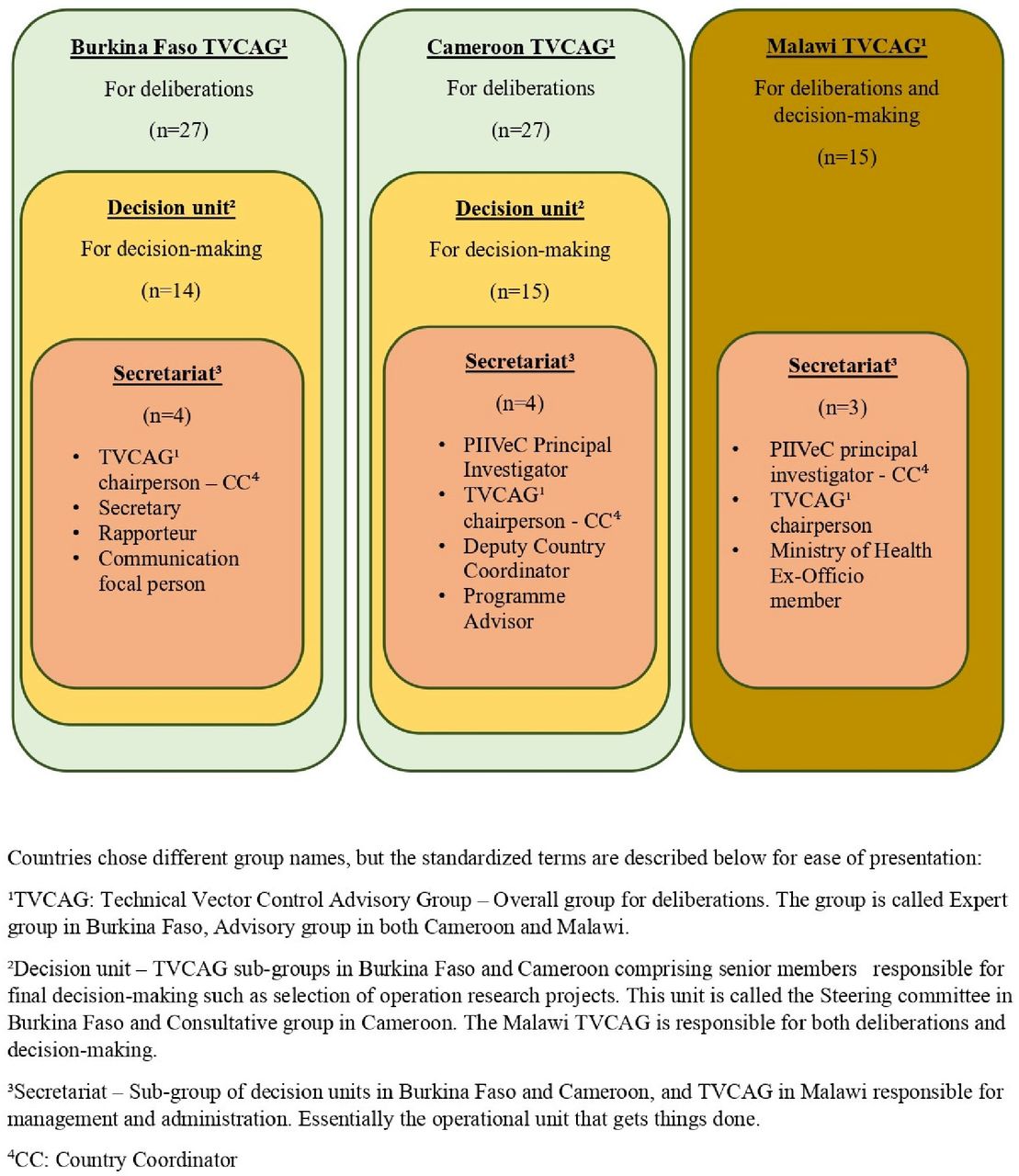
Each country established different group structures, all with secretariats responsible for management and administration (figure 3). Burkina Faso and Cameroon established two-tiered Groups with larger deliberation groups and smaller decision-making subunits, while Malawi established a one-tier group. The composition of the decision unit in Cameroon reflected that of the overall Group, whereas in Burkina Faso it excluded the private sector, and donor and partner institutions. In Malawi, the group included only two government representatives to facilitate the provision of independent advice to ministries.
{kind=link}
{kind=link}
{kind=link}
TVCAG structures in the three countries countries. PIIVeC, Partnership for Increasing the Impact of Vector Control.
The groups’ institutional membership in all three countries included government members (35% (9/26), 35% (9/26) and 13% (2/15) for Burkina Faso, Cameroon, and Malawi, respectively); academic and research (31% (8/26), 50% (13/26) and 53% (8/15), respectively); and, donor, technical and implementing partners (26% (7/26), 16% (4/26) and 33% (5/15), respectively). Only Burkina Faso included private sector partners (7% (2/26)) (table 1).
Membership and composition of technical Vector Control Advisory groups (groups) in Burkina Faso, Cameroon and Malawi
The groups were formally established (timeline from recruitment of coordinators to first meetings being held) within 10 months in Burkina Faso and Cameroon, and 19 months in Malawi. The process in Malawi was delayed by the stakeholder consultations, bureaucratic procedures and the political uncertainty following the May 2019 disputed general elections.13 In Burkina Faso, there were three different Ministers of Health during the life of PIIVeC, requiring new relationships to be built each time as senior health officials changed with the minister.
Rapid reviews and evidence synthesis
During the programme’s conception, we had anticipated the need for rapid reviews to inform Group decision-making, and the WP4 team included staff with this expertise. Despite this resource availability, there was no demand for rapid reviews, with countries preferring to commission operational research (OR) (described below under evidence generation).
Secondment programme
PIIVeC aimed to generate evidence and impact policy simultaneously at national and global levels. We envisaged that secondment of researchers to global policy-focused (eg, WHO Geneva) and implementation-focused institutions (eg, Global Fund) would provide further KT opportunities; increase the influence of African scientists on global policy; and support individual capacity strengthening. However, despite having agreements in place with relevant global partners, it proved challenging to achieve this, primarily due to matching relevant skills and expertise with the placements available and identifying clear objectives for the secondments that would benefit both parties plus, latterly, the COVID-19 pandemic. However, we promoted opportunities (vacancies) within global policy committees via the partnerships network which resulted in at least two additional African scientists (including one PIIVeC fellow) sitting on influential WHO committees. We also facilitated opportunities for staff from partner organisations to obtain specific skills (for example in laboratory management skills).
Evidence generation
The programme had two main strategies to generate evidence: OR commissioned by the groups; and academic research by fellows and early career researchers (ECRs) they supervised.
OR evidence
Prior to launching and first Group meetings, VBD programme managers in each country were invited to prepare presentations on the current disease statuses and identify critical evidence gaps. In Cameroon, after the presentations, meeting participants were grouped, based on disease expertise and interests, to further discuss and prioritise the evidence gaps, which were presented to the wider Group for review. Later, the decision unit convened to consolidate and prioritise the policy research themes for each disease. Prioritisation was in line with the MoH research strategic plan, disease impact (malaria with a high burden) and weakness of existing data (eg, arboviral infections). Urgent operational decisions, such as the choice between delivering piperonyl butoxide and pyrethroid bednets versus standard pyrethroid only bednets for malaria control were also given priority.
In Burkina Faso, a specially convened meeting by the decision unit was arranged to prioritise the research policy themes in alignment to the national and MoH research priorities, PIIVeC objectives and comprehensive approach to VC. In Malawi, the group held a session to identify themes that were aligned to the MoH research strategic plan and prioritise them based on gaps in funding availability in the respective disease programmes, meaning that malaria was given a low priority relative to other VBDs.
After consolidating the gaps into sets of priority policy themes (online supplemental table S1), the secretariats launched competitive calls to attract national researchers. The selection of project proposals was based on relevance, feasibility, impact, individual and institutional capacity and budget appropriateness. After establishing the groups, it took Burkina Faso 11 months to make the first OR call, while Cameroon launched a first call after 4 months, and a further call after 21 months. Malawi made the first OR call after 7 months, however, the limited applications received were more focused on individual capacity strengthening. Plans were made to relaunch the call with a greater emphasis placed on dialogue between applicants and the group to support stronger applications. Unfortunately, this did not occur due to the COVID-19 outbreak and response in Malawi.
Supplemental material
Seventeen OR projects were commissioned by groups in Burkina Faso (n=4) and Cameroon (round 1, n=7 and round 2, n=6). The OR portfolio featured a broad range of VBDs with 18% (3/17) focused on malaria, 12% (2/17) cutting across multiple VBDs and others on individual diseases (online supplemental table S1).
Academic research evidence
Academic research evidence was produced by a cohort of fellows and ECRs embedded in each country and supported by a professional development scheme (stream 2, figure 1). The fellows were recruited via competitive country-led processes in which postdoctoral researchers applied in response to broad thematic research questions aligned with key VBD research priorities. Each fellow developed their own research budget (within a ceiling), which included provision for appointment of ECRs (commonly MSc or PhD candidates) to address subcomponents of their research.
A total of 26 research projects were conducted by both fellows (n=11) and ECRs (n=15) in the three countries comprising 16 implementation and 10 basic research projects (online supplemental table S1). Malaria featured heavily in the portfolio of the fellows and ECRs with five (5/26, 19%) fellows’ projects focused on malaria or, malaria and lymphatic filariasis, and nine ECR (9/26, 35%) projects focused on malaria.
In addition to the preliminary policy and evidence uptake training conducted in October 2018 (described in Stakeholder analysis and engagement), the fellows received a 1-day virtual training focused on policy brief development in September 2020. This resulted in two policy briefs ((https://www.piivec.org/resources/the-role-of-vector-control-in-preventing-and-responding-to-rhodesian-human-african) and (https://www.piivec.org/resources/evidence-to-inform-how-new-bed-nets-can-be-used-to-prevent-malaria-in-malawi)) and a further four briefs in development. Two Malawian fellows became members of the malaria National VC TWG, and a Burkinabe fellow was involved in revising the national arbovirus control strategy.
South-south engagement
The concept of a south-south engagement unit emerged at the programme’s annual meeting in September 2019. The aim was to bring together southern partners including national PIs and coordinators for virtual monthly meetings to share experiences and identify synergies for collaborations. For example, this resulted in two fellows from Burkina Faso and Cameroon to collaborate on their similar projects. Unfortunately, these meetings were affected by many factors such as competing priorities, workload and intermittent internet connectivity, and only 5 out of a possible 23 monthly meetings were held. This was potentially a missed opportunity to strengthen partnerships among southern institutions to jointly conduct research of greater regional impact. It should be noted however that all southern partner institutes had representation in the programme’s management board, hence this was not the only mechanism for south-south engagement. Additionally, the collaboration between AFIDEP and all the African research partners will be maintained via a number of follow-on projects.
Reflections on lessons learnt
KT requires a mix of research and policy engagement skills
Mallidou et al14 articulate the core competences of KT champions, and the need for tailored hands-on trainings to strengthen these skills. Our experiences highlight the importance of identifying individuals with the technical expertise, research experience and policy engagement skills needed to facilitate KT. In line with Mallidou et al,14 we found that individuals with the critical skill mix were in short supply, especially in Malawi where we had to use the PI in this role.15 It seems that hiring well positioned, influential and established people to be the KT champions potentially avoided a challenge identified by a district level knowledge-brokering programme in Burkina Faso, where the broker had to become accepted before they were heard.16 Within the Groups, a skill mix was achieved by bringing together actors from government, academic and other sectors. The coordinators played critical roles in identifying potential group members, and the opportunity to share and discuss their plans resulted in changes to the planned sizes (smaller than originally intended for some countries) and composition (more diverse) of Groups, suggesting an added benefit of working across multiple countries.
Capacity strengthening in KT supports planned and opportunistic engagement opportunities
Strong networks linking researchers to policy-makers, technical expertise in the health-research domain and expertise in KT approaches are key to enhancing translation of research into useful formats for policy and operational decision makers. We used a tailored programme of capacity strengthening to develop the skills of researchers and ensure effective KT, which is prerequisite for similar efforts in immunisation advisory groups.17 Training and support underpinned the development of policy engagement strategies, which encouraged researchers to identify and engage key stakeholders from the start of their research. Policy briefs are useful and effective non-academic knowledge transfer strategies, and the ability to develop them is essential for researchers to facilitate evidence-use in policy.18 19 Our researchers were equipped with skills to develop policy briefs to frame issues and share findings, a skill which they will likely hone and develop throughout their careers. This concurs with Dagenias20 who observed that the inability for researchers to craft and communicate policy recommendations from research is an obstacle to evidence-use. Thus, they recommended targeted capacity strengthening of researchers in communication of findings to decision-makers, who inherently have challenges in accessing and deciphering scientific evidence.16
Other KT efforts have recommended or provided capacity strengthening to ‘consumers’ of research, for example, by training advisory group members in research and use of evidence.20–22 We did not provide formal training to Group members, however it is likely that the strategy of engaging them in commissioning research also aided their understanding of research methods and design. On the other hand, given there was no uptake for the available programme expertise in rapid reviews, perhaps we needed to invest in awareness raising and capacity strengthening to inform decision makers how this type of research could be useful in their decision-making context. This was planned in the form of face-to-face meeting and discussion with wider group members on what the programme could offer, unfortunately prevented by COVID-19 pandemic.
Secondment programmes have been identified as providing increased interaction at inter-organisational level, in support of policy engagement.23 24 Our global secondment activities did not happen as we anticipated. This may have been an overambitious strategy given the duration of the programme and the lack of previous exposure to global level institutions in our fellow cohorts. However, many more of the fellows are now ready for this step than at the start of the programme and we remain convinced that greater representation of African scientists within global institutions is essential per se, to enhance KT and to ensure policies are more effective and sustainable.
Responsiveness and adaptability to dynamic context is critical
KT efforts in immunisation have recognised the importance of identifying existing advisory groups to avoid duplication and tension when similar groups exist.25 Our experience also indicates the importance of identifying existing advisory groups and carefully weighing the options to either expand their scope or establish new groups. We did this using formal stakeholder analysis and qualitative methods, which helped us to uncover pre-existing power relationships that may have affected impact and sustainability. Lessons learnt from immunisation advisory groups also emphasise the importance of context and adaptability, and affirm that ‘one-size cannot fit all’.26–28
We also found that the appropriate model will be diverse in different countries, and can change over time within a country, and echo the importance of adapting processes and governance to dynamic national contexts for successful KT.19 29 The timelines for our policy engagement work were impacted by turnover of key ministers,29 periods of political uncertainty and the COVID-19 pandemic. Although the timing and exact nature of these events is not predictable, it is highly likely that such setbacks will occur and therefore risk management and mitigation plans which consider this would be worthwhile.
Regional collaborations
Regional bodies including the Economic Commission of the West African States and West African Health Organisation (WAHO) have been actively promoting evidence-based health policy19 21 28 and regional-level consultative committees comprising experienced researchers and policy-makers have also been proposed as a strategy to address ‘ceaseless management turnover’ and provide stronger coordination.21 We had planned to embark on a series of face-to-face discussions with Regional actors including Africa Centres for Disease Control and Prevention, WAHO and others to identify regional level opportunities for KT on VC and capacity strengthening, however, this was prevented by COVID-19. More positively, the Pan African Mosquito Control Association (PAMCA) which has chapters in a growing number of countries, is supporting efforts to continue and expand the advisory Group model. PAMCA has funding from the Bill and Melinda Gates foundation which will be used to support and expand the groups’ activities in Burkina Faso and Cameroon, (other research funds are being used in Malawi where a PAMCA chapter has recently been opened). Colleagues from the Cameroon PAMCA chapter will also be providing technical advice to the Central African Republic PAMCA chapter to support them to setup an advisory group.
National health agendas should be formulated in parallel with national research agendas
Evidence that responds to country needs is more likely to be translated30 and involving national programme managers in prioritising evidence gaps promotes ownership and political will that increases evidence-use.24 In-line with suggestions by other authors,19 our efforts to increase the evidence base on VBD control through OR were initiated by involving national disease control programmes to determine evidence gaps, commission the research (with PIIVeC funding) and engage with the process of conducting it. These efforts were conducted in parallel with our KT efforts, and countries invested substantial time in commissioning research from domestic research institutions, including those that were not consortium partners. This demonstrates how governments and national research institutions can work together to produce relevant, timely research to support policy agendas, while also leveraging and strengthening domestic research capacity, if funds are available to support this process.
We acknowledge the influence of the three different contexts on evidence generation and use. Differences were observed in progress of key activities which could be related to the interaction of context, governance models and country capacity. For example, Cameroon, with a Group managed outside of the MoH and additional staffing within the coordination team, made two OR calls while Burkina Faso made one call and Malawi was unable to complete the process. This could in part be attributed to the swifter decision-making processes outside of a public system,31 which benefitted Cameroon. At the time of writing, the government of Cameroon had signalled its desire to take on ownership of the Group in partnership with CRID and MoHs and agriculture; it will be interesting to see if this happens and how it may affect the speed and impact of activities. In Burkina Faso, our influential coordinator and the fact that the consortium partner is within the MoH enabled effective navigation through bureaucracy, in spite of political changes, suggesting that working within government can be an effective strategy. In Malawi, the externally affiliated coordinator had minimal influence within the government bureaucracy but relied on the government Ex Officio included in the group for follow-ups within the MoH. Political uncertainty, staff/minister turnover and COVID-19 affected progress in all countries.
It seems likely that the progress made by our groups hinged both on government support for evidence-use in decision making and, on our programme having resources to commission and fund relevant research. While continuation funding has been secured, it is notable that this is again from research grants. More effective and routine KT requires governments in low-income countries to mobilise more domestic resources rather than relying on external partners to fund research.28 This will need to be complemented by external funding to implement the research findings.20
Long-term follow-up than our project funding allowed would be needed to answer key questions about the sustainability and impact of the KT and evidence generation strategies in the three contexts including: Will the Groups be sustainable in the absence of research grant funding? What is the impact of KT activities on national and global policy for VC? What are the best strategies to increase the influence of nationally generated evidence and African researchers in global VBD policy making?
Conclusion
Promoting evidence-use in policy and practice requires ongoing engagement of evidence generators and users and the involvement of relevant stakeholders in developing research agendas increases the likelihood of evidence-use in policy and practice. The PIIVeC programme used this approach to support efforts to tackle VBD in Burkina Faso, Cameroon and Malawi.
Our strategy hinged on establishing groups that commissioned OR and promoted evidence-use by engaging key stakeholders. This required a suitable coordinator; consideration of contextual factors to determine group governance and composition; flexibility and adaptability. Strengthening researchers’ capacity to do policy engagement equipped them to transfer their knowledge on preplanned and opportunistic policy engagement activities. The countries present three differing contexts with longer-term research and evaluation necessary to draw conclusions on impact. There is a need for adaptability and flexibility, rather than rigid one-size-fits all approaches, to facilitate evolution in governance, ownership and leadership of KTPs.
Data availability statement
Data that support the findings are available within the article and supplementary materials, or from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge the technical contribution of Justin Pulford in guiding the paper’s structure.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Valery Ridde
Contributors CAM and EW conceptualised, designed and drafted the paper; CAM, EW, ET and JAQ acquired and analysed supporting information; RD, EW, HR, RO, TM, SN’f obtained the funding. JAQ, ET, NA, RO and EW provided technical support to implementation of the activities reported. All authors provided study materials and information, critically reviewed the manuscript for important intellectual content, and approved the final version of the paper before submission.
Funding The study was supported by the UK Global Challenges Research Fund that was awarded to a research programme called Partnership for Increasing the Impact of Vector Control (PIIVeC) (grant number MR/P027873/1).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.