Article Text

Abstract
COVID-19 brings uncertainties and new precarities for communities and researchers, altering and amplifying relational vulnerabilities (vulnerabilities which emerge from relationships of unequal power and place those less powerful at risk of abuse and violence). Research approaches have changed too, with increasing use of remote data collection methods. These multiple changes necessitate new or adapted safeguarding responses. This practice piece shares practical learnings and resources on safeguarding from the Accountability for Informal Urban Equity hub, which uses participatory action research, aiming to catalyse change in approaches to enhancing accountability and improving the health and well-being of marginalised people living and working in informal urban spaces in Bangladesh, India, Kenya and Sierra Leone. We outline three new challenges that emerged in the context of the pandemic (1): exacerbated relational vulnerabilities and dilemmas for researchers in responding to increased reports of different forms of violence coupled with support services that were limited prior to the pandemic becoming barely functional or non-existent in some research sites, (2) the increased use of virtual and remote research methods, with implications for safeguarding and (3) new stress, anxiety and vulnerabilities experienced by researchers. We then outline our learning and recommended action points for addressing emerging challenges, linking practice to the mnemonic ‘the four Rs: recognise, respond, report, refer’. COVID-19 has intensified safeguarding risks. We stress the importance of communities, researchers and co-researchers engaging in dialogue and ongoing discussions of power and positionality, which are important to foster co-learning and co-production of safeguarding processes.
- COVID-19
- health policy
- public health
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. Data sharing not applicable as no datasets generated or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
COVID-19 has amplified relational vulnerabilities and safeguarding risks in global health research for all (researchers and participants); yet to date there is limited conceptual and practical discussion of approaches and strategies to mitigate these amplified risks.
COVID-19 safeguarding risks include the increase in different forms of violence across the Accountability for Informal Urban Equity hub study sites (at a time when many support services are out of reach); threats to participants’ safety during online and digital research interactions and enhanced stress and vulnerabilities for participants, co-researchers and researchers.
In participatory action research, where the boundaries between the researcher and the researched are often blurred; and co-researchers (locally recruited researchers) experience a combination of risks and responsibilities an inclusive approach to safeguarding to prevent harm is crucial.
Adopting a reflexive approach that recognises new and intensified vulnerabilities experienced by research participants, co-researchers and researchers allows for ongoing learning, adaptation and practical action to address amplified risks against the mnemonic of the ‘the four Rs: recognise, respond, report, refer’.
Within research consortia, co-learning and co-production of safeguarding processes supports buy-in and responsiveness to new challenges; innovative solutions need to be identified by research consortia to ensure continuity of care for survivors of abuse and research teams need to consider how they will respond and refer in situations where services are negatively affected or unavailable.
Introduction
COVID-19 both alters and amplifies relational vulnerabilities with wide reaching impacts. Relational vulnerabilities emerge in situations where there is a power differential that makes an individual or group particularly vulnerable to violence or abuse.1 Incidence of sexual and gender-based violence (SGBV) and gender-based violence (GBV), intimate partner violence (IPV), violence against children (VAC) and authority-based violence (eg, police violence) has increased across many contexts during the COVID-19 pandemic.2–4 Relational vulnerabilities have also been exacerbated for certain marginalised groups, such as migrants or persons with disabilities, largely as a result of amplification of pre-existing inequities and ongoing structural violence.5 The nature and processes of global health research have also changed, with much research going remote—that is, online or telephonic—and that which remains face-to-face necessarily including COVID-19 prevention and safety measures. This makes working with marginalised and disadvantaged populations such as those living and working in urban and informal spaces ever more challenging, particularly through research approaches that prioritise co-production and collective action.6 Researchers and research teams have also been affected by changing circumstances. Reports show increased levels of stress, anxiety and exhaustion, with women researchers, who are often balancing caring responsibilities, particularly affected.7–9 Changing vulnerabilities and shifts in the global health research landscape create new safeguarding challenges, impact existing ones and necessitate new or adapted safeguarding responses. This requires discussions, critical self-reflection and cross-learning on the strategies being used to promote safeguarding and how well these are working, to identify ways in which they may be adapted and improved.
While there is some guidance on addressing COVID-19 or humanitarian crises in safeguarding in international development research and humanitarian action,10 11 there is very little experiential learning from specific research programmes. This paper outlines the safeguarding approach adopted by Accountability for Equity in Urban Health (ARISE) (see box 1), an international research hub focusing on accountability, health and well-being in informal settlements.
Accountability for Equity in Urban Health (ARISE) and partnership with co-researchers
‘ARISE is a research consortium launched in January 2019 and funded by UK Research and Innovation’s Global Challenges Research Fund for 5 years. The research consortium consists of 11 partners from a range of backgrounds and disciplines, led by the Liverpool School of Tropical Medicine. The vision of ARISE is to catalyse change in approaches to enhancing accountability and improving the health and well-being of poor, marginalised people living and working in informal urban spaces in Bangladesh, India, Kenya and Sierra Leone’.
Working with co-researchers: one of the core strategies adopted by ARISE is promoting capacity strengthening of urban marginalised people to generate, collect and use evidence as new localised knowledge to instigate change. In all action sites, ARISE has recruited community members as ‘co-researchers’, who are partnering with professional researchers and community development organisations across all stages of the research process, including collecting and analysing data from participatory research methods and Geographic Information Systems mapping.
Throughout this article, in our discussion of safeguarding in international development research, we use the United Kingdom Collaborative on Development Research (UKCDR) definition as preventing and addressing ‘any sexual exploitation, abuse or harassment of research participants, communities and research staff, plus any broader forms of violence, exploitation and abuse… such as bullying, psychological abuse and physical violence’.12 This UKCDR guidance also includes safeguarding roles and responsibilities for different actors in research process.
The ARISE safeguarding approach and action plans10 were developed prior to the advent of COVID-19. This paper does not describe how to carry out research into safeguarding, but is a practice implementation piece, which aims to share our experiential learning from prioritising safeguarding within international health research in the context of COVID-19. Sharing learning in this way builds on our arguments that safeguarding is a reflexive journey and not a tick-box exercise.10 Given the focus of the ARISE hub, these learnings are related to research conducted on health, well-being and accountability in informal urban spaces in Bangladesh, India, Kenya and Sierra Leone. We are mindful that safeguarding issues can occur anywhere within the ARISE partnership and involve any partners, researchers, co-researchers as well as participants living and working in informal urban spaces.
Our reflexive approach
The adaptation of our safeguarding approach in response to COVID-19, and the learning distilled in this practice piece, were informed by the following processes: (i) ongoing online ‘check-in’ meetings of the ARISE safeguarding leads (at least one per research partner institution) that provided a safe space to share experiences, reflect on challenges emerging, support each other and problem-solve; (ii) reflection through discussion across the whole ARISE hub; (iii) learning from the findings of an ARISE-wide partnership survey which included questions on whether ARISE colleagues felt safe and supported in their ongoing work during the COVID-19 pandemic; (iv) sharing experiences with other hubs, and people working in this area including partaking in UKCDR’s research and development of safeguarding guidelines in international development, and development of an addendum on responses during COVID-1912 and (v) adapting institution-specific country safeguarding action plans.
We structure this commentary around two inter-related areas of action and learning identified through these processes, which respond to the changing contexts and challenges brought about by COVID-19: (i) identified new challenges that emerged in the context of the pandemic and (ii) recommended action points for addressing these challenges.
Identified new challenges that emerged in the context of the pandemic
Exacerbated relational vulnerabilities in informal settlements create dilemmas for researchers
SGBV, child abuse and neglect are rising; service delivery gaps and deficits present moral dilemmas for researchers in how best to support vulnerable populations
Social and economic stresses associated with COVID-19 such as lockdowns and restrictions of movement have led to increases in SGBV, including IPV, referred to as the ‘Shadow Pandemic’ by UN Women (2020); this global trend4 is reflected in our study sites. For example, in Sierra Leone, exposure to SGBV has intensified during COVID-19 as during the 2014–2016 Ebola epidemic, and in many other crises globally, particularly those involving restrictive public health measures; resulting in increased teenage pregnancies, early marriage and transactional sex.13 These restrictive public health measures are exacerbated by the challenges of informal urban living, such as lack of a daily wage, lack of extended family/support networks, overcrowding, rapid/unplanned return to rural areas, particularly for the poorest residents living in informal settlements.14 In Kenya, increased occurrences of SGBV have been reported among adolescent girls and young women in general. In two of programme sites in Western and Nairobi run by Liverpool Voluntary Counselling and Testing (LVCT) Health, an ARISE partner, and working with 38 470 and 27 173, respectively, a total of 793 adolescent girls and young women beneficiaries reported cases of violence over a span of 1.5 months post-COVID-19 onset. One in 20 experienced sexual violence including attempted rape, defilement (sexual penetration of a child) and sexual harassment; half experienced emotional violence including verbal abuse, discrimination and harassment; two in five experienced physical violence; one in five reported IPV; three in five reported cases were perpetrated by a family member. In Bangladesh, BRAC Human Rights and Legal Aid Clinics reported receiving a total of 25 607 GBV cases across Bangladesh from January to October 2020, which was 24% more than in the previous year.15 ActionAid, an international non-governmental organisations (NGO), has identified a 10-fold increase in SGBV from April to May 2020 through their network of support services in Bangladesh.16 Furthermore, people with disabilities have been at increased risk of SGBV in all ARISE countries, and experiences of violence are known to lead to considerable physical and mental sequalae. However, the evidence on how to prevent and respond appropriately to violence in general is limited.6 17 18
Reports of increases in child abuse have also been noted globally, as well as in the four ARISE partner countries.13 With schools and child-care centres closed, children are especially vulnerable to physical, emotional, sexual abuse and neglect, particularly as pressures on parents increase due to employment loss, food shortages and the subsequent impacts on mental well-being. During lockdown in Sierra Leone, schools were closed, but parents and caregivers, especially those working in the informal sector, had little choice but to continue going to work, leaving children at home vulnerable to abuse by co-tenants, other family members and neighbours. Without the contact with teachers, childcare providers, health workers and other key community members who might otherwise spot the signs of child abuse or neglect, children’s paths to protection are impaired or cut-off. These impacts on childcare as explored by Zar et al,19 have an impact on early childhood development for under-5 children, and also on the health and mental well-being of older children.
An increased incidence of violence in ARISE study sites was occurring at the same time as support services were closing or reducing operations due to funding and logistical challenges; or were inaccessible to communities. Furthermore, tensions between disadvantaged communities seeking daily wage labour outside their localities and the police tasked with maintaining lockdown restrictions on movement may have prevented people seeking police help for interpersonal violence. This puts research teams in a challenging situation with respect to preventing and responding to violence and referring appropriately. It raises moral dilemmas, such as: What do we do if quality services are not in reach and SGBV is on the increase? Is it ethical to continue with such research? How do we understand and navigate new tensions and complexities, in which the very nature of what it means for authorities to protect citizens is undergoing transition? And how do we navigate existing community-based structures that are in place to address violence and neglect?
SGBV, IPV within informal settlements: formal and informal structures, decisions and dilemmas
Across our ARISE action sites, even where formal services for survivors of SGBV have been available (eg, Rainbo in Sierra Leone), there have been very few referrals from informal urban settlements either prior to or during the COVID-19 pandemic. There are a range of alternative community-based systems and structures in informal settlements which can intervene in cases of SGBV, such as elders and religious leaders, who may institute counselling and some sanctions.20 For example, in an informal settlement in Freetown, men who beat their wives are fined heavily, which our research participants believe has led to a decrease in the reports of IPV.
On the one hand, community-based mechanisms create a strong platform for action if they can be supported and strengthened. On the other hand, community action and response surrounding COVID-19 can exacerbate ethical dilemmas for researchers working with communities to address the challenge of violence. They often leave researchers feeling challenged when we are concerned that these community response mechanisms reinforce pre-existing power imbalances or perhaps fall short in addressing the complex medical and social support needs those survivors of such abuse have.
For example, how far should researchers work within these informal structures when the researchers perceive a situation to be a case for the police, and communities may wish to protect the perpetrator? Community members report that in some cases where the police have been involved, no action has been taken. This can be difficult for the research team and some community members who bear witness to ongoing social injustice yet feel constrained in the supportive action that they can take. This dilemma is further amplified when undertaking research that aims to foster trust and equitable partnership with communities to co-produce action for social change.
The changing face of research: using virtual and remote research methods
COVID-19-related restrictions varied in levels, timing and sequence across and within all ARISE contexts. There was increasing academic discussion of the challenges and opportunities associated with virtual qualitative and participatory research processes, with key issues including ethics, dealing with sensitive matters, quality and timeliness.21–24 Within ARISE, country teams’ decisions about stopping research or continuing (either virtually or face-to-face) were taken in line with country guidance, and reviewed as appropriate in programme management meetings, with risk registers and safeguarding procedures updated. We used virtual research methods due to lockdown/curfew and travel restrictions in all our action sites. Research teams in Bangladesh, India, Kenya and Sierra Leone all undertook remote interviews with residents in informal settlements. For example, The George Institute in India conducted telephone interviews with waste pickers, to understand the lived experiences of health, livelihood, provision and social support during the pandemic. In all partner countries, emotional distress was common in interviews during and related to the COVID-19 pandemic. Many participants became emotional when sharing experiences of livelihood challenges and GBV.
There are also challenges related to digital safeguarding. In our safeguarding check-ins and ARISE discussions, key safeguarding difficulties related to virtual methods included limited opportunity for building trust and rapport that would facilitate disclosure; inability in remote, non-visual communications to perceive non-verbal clues from research participants that could alert the research team to safeguarding concerns and unclear communication owing to technological glitches.
COVID-19 and new vulnerabilities for researchers
There is a growing body of literature on the impacts of COVID-19 on the academic and research community, including stress, anxiety and burn out, and how the effects can be gendered and felt more acutely by those on short-term contracts or with less power.7 8 To mitigate this and support the development of equitable partnerships, we conducted an ARISE partnership survey (July 2020), which included questions related to the safety and well-being of the ARISE hub members. All colleagues in partner institutions in the ARISE hub were invited to participate anonymously. There were 44 respondents, of whom 42 specified their location—15 in the UK, and 27 in African or Asian institutions.
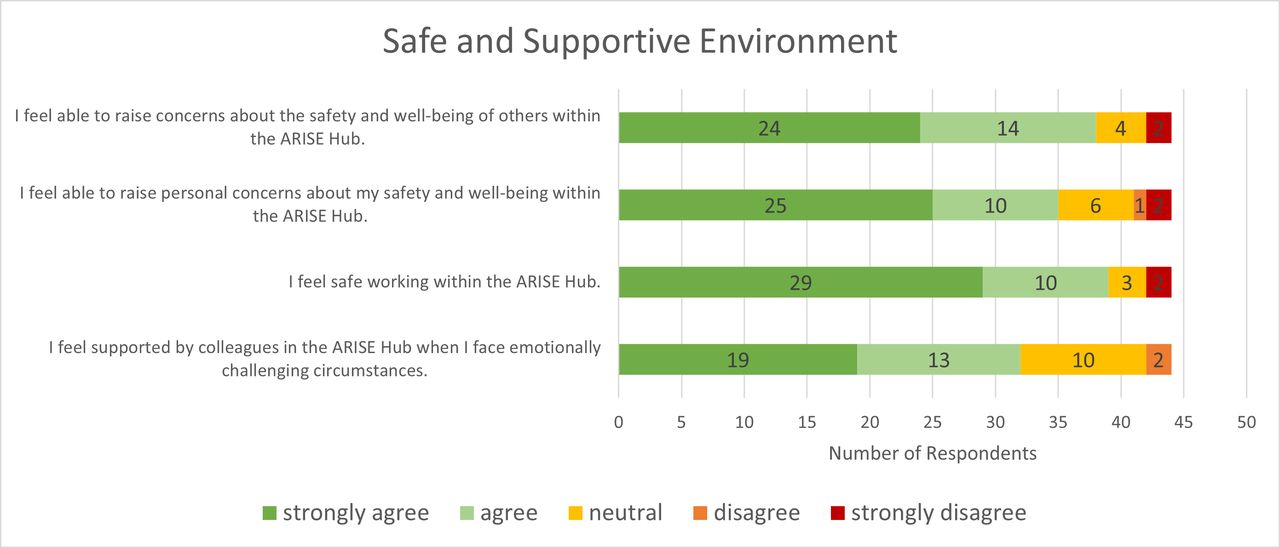
On the whole, the responses to the 2020 ARISE partnership survey were very positive, including belief in the hub’s commitment to ethical research and safeguarding, and an appropriate response to COVID-19. However, some responses were concerning: a minority of participants said that they did not feel safe, or able to raise concerns about their own safety and well-being, or that of others (figure 1). Some individuals strongly disagreed with the statement that they feel practically and emotionally supported by the ARISE hub (figure 2).

Responses to questions on a safe and supportive environment in the 2020 Accountability for Equity in Urban Health (ARISE) partnership survey.
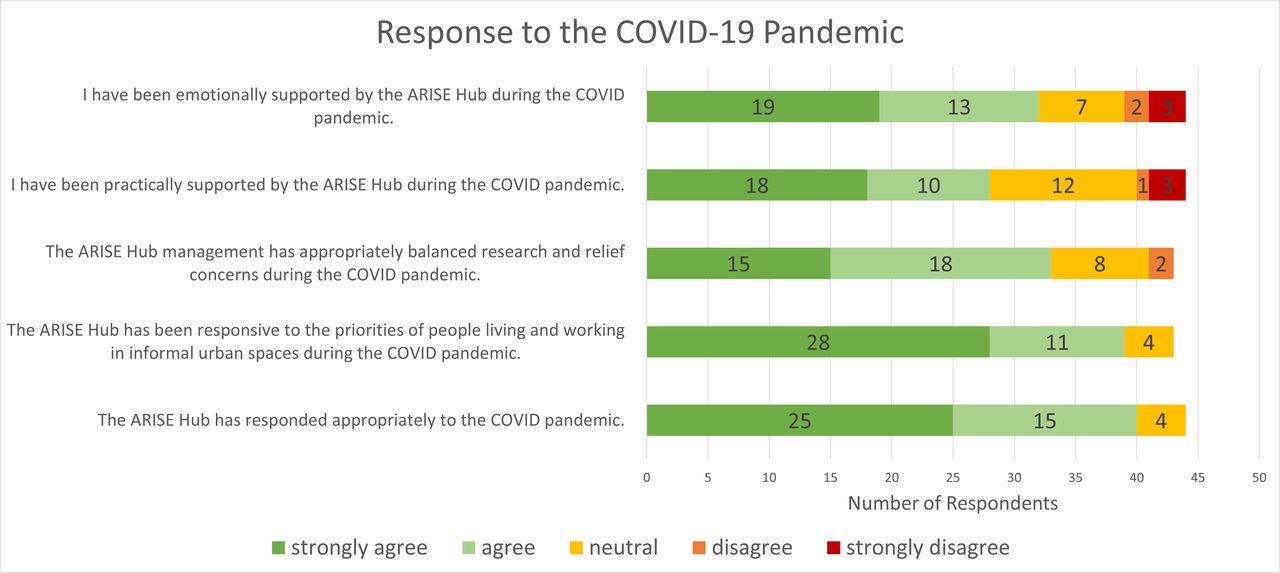
Responses to questions on the Accountability for Equity in Urban Health (ARISE) hub’s response to the COVID-19 pandemic in the 2020 ARISE partnership survey.
Recommended action points for addressing emerging challenges
Working in partnership to respond to intensified relational vulnerabilities
In the context of challenges to adequately respond to SGBV, child abuse and neglect posed by increased reports and the reduced availability of services due to the pandemic, we discovered some innovative actions taken by communities across our partner sites. For example, community health workers, who are a key community cadre, trusted by many, that link to the health system, can make referrals to ensure that survivors can access the support they need where they would like to receive it. In some informal settlements in Nairobi, women referred themselves to community-based organisations and NGOs; and reported perpetrators to authorities where they felt this was appropriate. In one of our ARISE action sites, Mathare, an informal settlement in Nairobi, Kenya, Médecins Sans Frontières is well known in the community for referral for treatment of SGBV cases, while Shining Hope For Communities is known for counselling and case follow-up with the authorities. Another trend that was highlighted by co-researchers that, from a sense of self-protection and a desire to avoid stigma, survivors often preferred to seek services away from where they were living. Hence, it can help to provide referrals to a range of services in different geographical locations, where possible. Devries et al25 however highlighted the challenges in finding appropriate services to refer victims to, especially child victims of abuse. Knowing what services are available and being provided at a particular time is imperative, pointing to the need for service maps or directories as living documents with frequent updates. In Slum Dwellers’ International (SDI) programmes for youth skills training, we observed that when a safe space is created for young people at a distance from their communities, for example, having sessions away from their neighbourhoods, it creates an opportunity for them to talk about serious issues that they are facing such as kidnapping, extrajudicial killings and forced marriage.
Case study 1: partnership with co-researchers for support strategies to respond to extreme distress in Kenya
An early (prepandemic) ARISE hub activity was community mapping of various local resources. In the course of a project interaction during the pandemic, a woman research participant with disability reported being confined to the household, expressed suicidal ideation and demonstrated significant knowledge gaps about COVID-19. Co-researchers and researchers discussed a range of formal and informal structures mapped by the community as avenues for support with the participant. The participant chose structures offering spiritual support, specifically the church, and was connected to church members by the co-researchers. Three months later, researchers noted that the participant had received support over several visits by church members and had gone on to begin operating a small business next to the church (ARISE debrief sessions with co-researchers, Social mapping).
We have presented our key learnings and our reflexive approach in the mnemonic ‘the four Rs: recognise, respond, report, refer’ (table 1). Across ARISE, we agree on the importance of logging incidents and referral/action as appropriate.
The four Rs: recognise, respond, report, refer: supporting global health research to address issues of abuse and neglect, and examples from ARISE
Supplemental material
Supplemental material
Ensuring trustworthy interactions to promote safeguarding in digital, remote and face-to-face interactions
To navigate the issues presented by applying virtual data collection methods, we discussed non-verbal clues of distress that could be picked up on the phone, which included some hesitation in answering questions; going quiet or a sudden lowered tone; unanticipated refusal to participate and becoming uncomfortable when talking, described by an ARISE team member as ‘stressed voice, short and sharp, like there is no capacity on their side to deal with an interview because they deal with a stressful situation’. The research team learnt to identify who else was in the room, and how to talk to participants about trying to find a safe space where they could complete the interview, at a different time if required, so as not to put themselves at risk should someone overhear the conversation. This included learning more about verbal and non-verbal signals for help used in other contexts. The team familiarised themselves with the London Metropolitan Police phrase ‘Ask for Angela’ and the Canadian Women’s Association’s ‘Violence at Home Signal for Help’, which involves holding your palm towards a person, tucking in your thumb and making a fist with your thumb obscured (figure 3). As both these signals enable a participant to stop a conversation if someone comes into the room and to discreetly indicate their vulnerability without actually saying anything that might alert a potential perpetrator, discussions then focused on how best to apply this across the hub and in different country contexts. As in our previous piece on safeguarding,1 we note the synergies among ethical processes, safeguarding and credible ‘trustworthy’ qualitative research. Putting in place strategies to build rapport, and to ensure that participants feel comfortable and can truly express themselves, are important for all these reasons. With a specific focus on safeguarding, we found that the four Rs are important to act on in remote as well as in-person interactions (table 2). Although recognise, respond, refer and report all remain important, in relation to supporting research, far more emphasis needs to be placed on research institutions and the necessary support provided to recognise and respond.

{kind=link}
{kind=link}
{kind=link}
The Canadian Women’s Association’s ‘Violence at Home Signal for Help’.
The four Rs: recognise, respond, report, refer: supporting global health research to respond to vulnerabilities in virtual interactions
Face-to-face interactions previously widely used prepandemic also had to be adapted to safeguard the research team and participants. ARISE teams aimed to prioritise safety and prevent transmission of COVID-19 when discussions, or debriefings are carried out face-to-face. We followed three linked strategies for this: (i) developing standard operating procedures for conducting research during infectious disease outbreaks; (ii) provision of personal protective equipment (PPE) to researchers and co-researchers for every training and data collection activity and (iii) guidance and experience-sharing about staying safe through internal webinars early in the pandemic, and establishing hotlines and SMS services for community members to contact with questions related to COVID-19. Across all study sites, ARISE partners have also developed a mitigation and response strategy for informal settlements, provided technical support for evidence-based COVID-19 information, negotiated demands for PPE and advocated for systems-level interventions to minimise the community impact of COVID-19. For instance, partners in Kenya have built on existing governmental relationships to advocate for attention to socioeconomic vulnerabilities; SDI Kenya and CODOHSAPA Freetown have developed tools to monitor COVID-19 and other cases of health vulnerability in informal settlements in order to inform government and city responses.
Supporting the health, safety and well-being of ARISE hub staff and co-researchers
To respond to the findings from our partnership survey, and in line with our safeguarding best practices, we discussed them in the ARISE executive committee and encouraged further discussion at partner level. This led us to establish an ‘early career researcher network’, where self-identified early career researchers could discuss issues related to feelings of insecurity or vulnerability in more detail. We also further advertised, and made as accessible as possible, access and referral to our mental health support draw-down funds, so that researchers or co-researchers who were facing emotional distress could apply confidentially for funds to seek relevant and appropriate counselling and support, either internationally or in their home location.
Among our safeguarding leads, we also continued to reflect and share based on these findings within our regular check-in calls. Through this process, we also decided to accelerate existing plans to broaden our safeguarding activities for the research team to also include our co-researchers. We felt that this was critical as dealing with SGBV and relational issues and vulnerabilities can be particularly challenging for co-researchers who span the research-community relationship. Their unique positionality needed to be considered in responding to these issues. Many co-researchers were struggling with the information that they were receiving, so supporting them became a key priority. There has been discourse in the literature on the risk of secondary traumatic distress experienced by professionals and violence researchers.26 27 Recognising that our co-researchers who may be burdened by living in close proximity with both victims and alleged perpetrators may be experiencing frustrations of helplessness, we have held debrief sessions in supportive spaces, facilitated reflections and developed buddy systems. For example, the APHRC team hold a ‘huddle discussion’ at the end of each week to determine the mental well-being of co-researchers so as to respond, report and refer where necessary. In many instances, solutions have come from the co-researchers and the researchers, with a professional counsellor attending the session once a month to provide support on the issues raised. We are still reviewing and working to strengthen these support structures further to ensure that safeguarding training needs are considered.
We are actively evaluating the extent to which these additional safeguarding measures for our researchers and co-researchers have supported the improvement of well-being, and we will continue to share learning in this area. We will also document change through our annual partnership survey and continue to strengthen systems and structures for safeguarding within our research partnership and host institutions.
Conclusion
Safeguarding is arguably particularly nuanced and complex in participatory action research, as employed by ARISE, where co-researchers undertake research activities within their own communities. Within participatory research, which actively aims to reduce distance between researcher and the researched, boundaries are blurred; therefore, an inclusive approach to safeguarding to prevent harm is crucial. This calls for constant consultation between co-researchers and researchers, capacity building of co-researchers on safeguarding and a pragmatic approach that prioritises open, clear and transparent processes and disclosure. A platform for communities, researchers and co-researchers to hold critical discussions of power and positionality is important to foster co-learning and co-production of safeguarding processes.
COVID-19 has reshaped the relationships between state authorities and informal settlements as well as redefined what it means for authorities to protect citizens. The pandemic has brought uncertainties, economic challenges and new precarities for both communities and researchers, which have amplified safeguarding concerns. Recognising the unique needs of the participants involved in our study, safeguarding responses need to be tailored to meet emerging challenges, and opportunities to report safeguarding incidents made available to everyone across the consortium, irrespective of capabilities, formal education attainment or social status. Referrals should be made to support networks that have been confirmed as currently in operation and accessible to community members, with sociocultural dynamics and community-based justice acknowledged. Research teams do not have to provide these services themselves but in all projects an initial mapping of available services at the start of research is essential to ensure safe referrals. COVID-19 has intensified the interplay among safeguarding, ethics and health and safety, and the need to strengthen processes and deepen learnings is critical. Safeguarding therefore should not be an isolated event and need to be tied to the realities and focus of the project.
At a minimum, mapping and risk assessment, as well as regular review of concerns and procedures should be done by all research programmes. Although the ARISE safeguarding approach is arguably appropriate for all programmes, it is particularly pertinent for participatory processes and studies exploring issues where boundaries between researchers and researched overlap, as well as for marginalised populations facing multiple situational vulnerabilities. Funding implications need to be considered early in research planning the provision of dedicated and sufficient funding will ensure research teams are equipped with the training and resources to better manage safeguarding challenges.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. Data sharing not applicable as no datasets generated or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors would like to thank all in the ARISE hub who are taking forward safeguarding. The authors would like to thank the partners, co-researchers and communities. The authors would also like to thank Faye Moody for support with formatting and referencing.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @BintuMansaray9, @Laura_Deano, @helenelsey
Contributors BM, ST and LD led on drafting the paper with inputs from all coauthors. All coauthors have read and signed off the content.
Funding This work was supported by the UK Research and Innovation (UKRI). The GCRF Accountability for Informal Urban Equity hub ('ARISE') is a UKRI Collective Fund award with award reference ES/S00811X/1.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.