Article Text

Abstract
Background As the populations of lower-income and middle-income countries age, multimorbidity is increasing, but there is little information on its long-term consequences. We aimed to show associations between multimorbidity and outcomes of mortality and hospitalisation in Iran, a middle-income country undergoing rapid economic transition.
Methods We conducted a secondary analysis of longitudinal data collected in the Golestan Cohort Study. Data on demographics, morbidities and lifestyle factors were collected at baseline, and information on hospitalisations or deaths was captured annually. Logistic regression was used to analyse the association between baseline multimorbidity and 10-year mortality, Cox-proportional hazard models to measure lifetime risk of mortality and zero-inflation models to investigate the association between hospitalisation and multimorbidity. Multimorbidity was classified as ≥2 conditions or number of conditions. Demographic, lifestyle and socioeconomic variables were included as covariables.
Results The study recruited 50 045 participants aged 40–75 years between 2004 and 2008, 47 883 were available for analysis, 416 (57.3%) were female and 12 736 (27.94%) were multimorbid. The odds of dying at 10 years for multimorbidity defined as ≥2 conditions was 1.99 (95% CI 1.86 to 2.12, p<0.001), and it increased with increasing number of conditions (OR of 3.57; 95% CI 3.12 to 4.08, p<0.001 for ≥4 conditions). The survival analysis showed the hazard of death for those with ≥4 conditions was 3.06 (95% CI 2.74 to 3.43, p<0.001). The number of hospital admissions increased with number of conditions (OR of not being hospitalised of 0.36; 95% CI 0.31 to 0.52, p<0.001, for ≥4 conditions).
Conclusion The long-terms effects of multimorbidity on mortality and hospitalisation are similar in this population to those seen in high-income countries.
- epidemiology
- public health
- cohort study
Data availability statement
Data are available on reasonable request. Information about the study design, updated interim analyses, ongoing substudies and relevant publications are available at www.ddrc.ac.ir. Specific proposals for national and international collaborations are welcomed. Initial proposals, which include the aim of the proposed study, the required data and a time-table, should be submitted to RM (ri.ca.sma@kelam) or PB (rf.crai@atteffob). The proposals will be discussed within the steering committee, which includes the principal investigators of the study and, if necessary, other experts according to the proposal’s theme.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known about the subject?
In high-income countries (HICs), multimorbidity is prevalent and has been associated with serious long-term consequences such as mortality and increased hospitalisation.
As life expectancy increases, multimorbidity is now increasing in lower-income and middle-income countries (LMICs), but little is known about the long-term consequences.
These consequences may not be the same as in HICs, and given the effects of poverty, preceding undernutrition, and infectious diseases in LMIC settings, there is a chance the long-term consequences could be even worse.
What does this study add?
This is one of the first studies to show the long-term effects of multimorbidity outside of a HIC setting.
This study shows that in Iran, a country going through rapid economic growth and transitioning from a lower-middle to an upper-middle income country, multimorbidity gives increased risk of mortality and hospitalisation.
The study quantifies the effects of difference demographic and behavioural factors on long-term outcomes of multimorbidity.
How might this impact on clinical practice?
This study shows multimorbidity has a detrimental effect on long-term outcomes in a middle-income country going through rapid economic growth. Future research is needed to determine whether low-income countries will face similar issues as they develop.
The quantification of the effects of demographic and behavioural factors on long-term outcomes, allows better planning of health interventions.
Politicians and policy-makers in low-income countries, and global health funding, need to focus on chronic conditions and multimorbidity in the years to come in order to avoid the massive burden multimorbidity is likely to place on health systems.
Introduction
Multimorbidity is most commonly conceptualised as the presence of two or more conditions in an individual or it can be defined in other ways such as count of conditions.1 2 It encompasses comorbidity, which refers to two or more chronic conditions that are causally or pathologically linked.1 2 In high-income countries (HICs)—where most of the research on multimorbidity has focused1 3 it is increasingly recognised as a major health issue. Several longitudinal studies have shown strong associations between the presence of multimorbidity and adverse outcomes such as death or hospitalisation.4–8 Understanding the relationship between multimorbidity and outcomes and developing interventions to improve management of patients with multimorbidity to moderate outcomes is a major research focus in HICs.1 3
Multimorbidity has received less attention in lower-income and middle-income countries (LMICs).1 3 9–13 During the Millennium Development Goal era, health research and financial aid in LMICs focused on reducing communicable diseases, and improving maternal, neonatal and child health.14 These successful efforts have combined with increasing country economic development and reductions in poverty resulted in a growing population of older people, who are more likely to have multimorbidity, in LMICs.15 In addition, urbanisation, increasingly sedentary life styles and changes in dietary habits towards consumption of larger amounts of calorie dense food have led to a growth in population prevalence of obesity and associated chronic non-communicable diseases (NCDs).11 16 These chronic NCDs often co-occur in the same individual, but also occur on a background of a high prevalence of communicable diseases.1 10 Hence, multimorbidity in LMICs is growing in prevalence.
Nevertheless, outside of the HIC setting, the epidemiology and consequences of multimorbidity is a relatively unexplored area, and evidence on the health consequences of multimorbidity in LMIC settings is needed to increase the priority given to this issue. These consequences may not be the same as in HICs, and given the effects of poverty, preceding undernutrition and infectious diseases in LMIC settings, there is a chance the long-term consequences could be even worse.1
Cross-sectional analyses have shown a high prevalence of multimorbidity in a few countries, although most of these studies defined multimorbidity using only a limited number of conditions.10 11 Some studies have shown cross sectional associations of multimorbidity with disability, low quality of life, poor physical performance, number of hospitalisations and mortality.11 17 18 We are only aware of two longitudinal studies on the outcomes of multimorbidity, both of which were done in China, with limited numbers of participants.12 13 In order to prioritise planning for health systems that can deal adequately with the increasing burden of multimorbidity in LMICs, it is important to understand the relationship between multimorbidity and long-term health outcomes.
A lack of longitudinal, routinely collected, data in many LMICs limits the ability to report long-term outcomes of multimorbidity. However, data collected as part of a longitudinal cohort study in Iran over the time period where the country transitioned from lower-middle-income to upper-middle-income status, afford the opportunity to assess the outcomes of multimorbidity in a middle-income country going through rapid economic growth. Iran became an upper-middle-income country (UMIC) in 2009, as a result of a rapid and continued period of development. This economic transition and accompanying demographic change is likely reflective of that which will be experienced by many LMICs in the near future. Our aim was to show how presence of multimorbidity is associated with longitudinal outcomes of mortality and hospitalisation in Iran, and explore how this relationship is affected by individuals’ demographic and economic characteristics and behavioural factors.
Methods
This is a secondary analysis of data from the Golestan Cohort Study (GCS), a prospective study which was set up to study risk factors for oesophageal cancer (a highly prevalent cancer in this region). The extensive data collection protocol allows comprehensive study of multimorbidity.
Study setting
During the study period, The Islamic Republic of Iran was a lower-middle-income country in Western Asia with 83 million inhabitants.19 In the last 20 years, it has developed and urbanised, life expectancy has risen and there is an increased risk of exposure to tobacco, unhealthy diets and physical inactivity.20 21 Poverty is decreasing, but poverty headcount rates remain higher in rural areas (27%) than urban areas (6%).19 The prevalence of NCDs has increased along with economic growth; multimorbidity is prevalent.20 22
Golestan province is in the north-east of Iran. Urban participants of GCS were recruited from Gonbad City, (population 126 797 inhabitants in 2004) and rural participants from villages in Gonbad, Kaleleh and Aq-Qala counties. The life expectancy in Golestan (Women 72.36 and Men 67.71) in 2004 was similar to the rest of the country.23 The majority of the population live in urban areas and are educated.24 Access to healthcare has improved after the introduction of the ‘Health transformation plan (HTP)’, an initiative from the government to increase universal health coverage (UHC).25
Participants and sampling
The GCS recruited participants aged 40–75 years who were free from any gastrointestinal (GI) cancer between January 2004 and June 2008. The study aimed to recruit equal numbers of men and women, with 20% from urban areas, and 80% from Turkmen ethnicity.21 People unwilling to participate, temporary residents, or those with a current or previous diagnosis of any upper GI cancer were excluded. The sampling strategy has been described in detail elsewhere.21 26 In brief, in Gonbad city, participants were selected randomly from the five areas in Gonbad by systematic clustering based on household numbers. For rural areas, all 236 villages contained within Golestan province were included in the sampling frame and participants within these villages were selected by cluster sampling. All consenting adults in each household were invited to participate.
Data collection
For the baseline data collection, participants were contacted by trained healthcare workers and invited to attend the GCS Centre for completion of a questionnaire and collection of anthropometric and blood pressure data. The questionnaire collected information including: (1) Demographic characteristics: sex, age, ethnicity, marital status, educational level, rural or urban location, and information on 15 household assets; (2) personal history of all medication use in the last 6 months (participants were asked to bring medications to the visit); (3) self-report of the following diseases: rheumatic heart disease; angina, myocardial infarction, or heart failure; stroke; hypertension; diabetes; chronic obstructive pulmonary disease; kidney disease; intestinal disease; liver disease; serious infectious diseases (mainly tuberculosis); major disabilities; and history of surgery; (4) tobacco use; and (5) physical activity.27
Height in centimetres was measured while standing upright using a stadiometer and weight in kilograms was measured without shoes and in loose clothing using a Mechanical Seca 762. Blood pressure was measured using a Richter mercury sphygmomanometer twice on both arms while the participant was seated. The average of all four readings was used to derive blood pressure.
All participants in the study were followed up by telephone call every 12 months from enrolment to the present and any hospital admission since the last follow-up was recorded, and annual follow-up is ongoing. Participants were also instructed to notify the study team at the time of hospitalisation to limit issues with recall. The dataset used in this analysis was locked for analysis on 29th December 2019, which gave a minimum 10-year follow-up period for all recruited participants.
Definition of variables
Demographic characteristics and lifestyle factors
Age was described as a categorical variable, in groups <40, 40–49, 50–59, 60–69 and ≥70 (the age group <40 was created to include people who on attending the study centre indicated that they were younger than 40—most were people aged 38 and 39). It was used as a continuous variable in the models. Education level was dichotomised into no-education (no education) or education (including one or more years of education). Marital status was categorised as single (including single, widowed, divorced or separated) or married. Wealth quintiles were calculated from data on household assets ownership using multiple correspondence analysis which is widely accepted and used method.28 29 Ethnicity was dichotomised into Turkmen or other. Smoking was categorised as non-smoker, ex-smoker or current smoker. Alcohol consumption was low and this variable was not used in the analysis.
Body mass index (BMI) kg/m2 was calculated from height and weight and defined as underweight (<18.5 kg/m2), normal (18.5–25 kg/m2) and overweight or obese (≥25 kg/m2). Physical activity categories were derived by combining activities during employment, leisure and transport based on the amount (intensity and duration) of activity performed during a week based on metabolic equivalents of task, and categorised as previously described into tertiles: low (1), medium (2) and high (3).30
Definition of disease states
Hypertension was defined as either self-reported diagnosis, being on treatment or average measured systolic blood pressure of ≥140 mm/Hg or diastolic blood pressure ≥90 mm/Hg. Liver disease was identified by symptoms (jaundice), self-reported diagnosis or being on medication. All other conditions were identified by self-report or use of medication history as follows. First, medications which were specific to conditions self-reported by participants were removed from the list of an individual’s treatment. Then, if the participant was on medications specific for a condition not captured on self-report, they were assigned that condition. Remaining medications that were not used to treat specific diagnoses, but potentially used for a diagnosis that the participant had already been assigned were assumed to be given for that diagnosis and removed from the medication list. Finally, patients on any remaining medications that had not been accounted for by the above processes were assigned the condition which the medication is most likely to be used to treat. This process was conducted using reference to the British National Formulary and by agreement between authors (see online supplemental appendix tables 1 and 2 for assignment of diseases to participants).
Supplemental material
Participants were categorised as having any (or no) conditions in the domains of NCDs (conditions in the system categories of cancer, cardiovascular disease (CVD), endocrine, GI, respiratory, renal, neurology, rheumatology, unspecified conditions needing immunosuppressant or other NCDs (vitamin/mineral deficiency or benign prostatic hyperplasia)); communicable diseases (tuberculosis, hepatitis or HIV); or any mental health conditions.
Defining multimorbidity
Multimorbidity was defined using two internationally accepted definitions: first as the count of conditions, second as two or more conditions.1
Outcomes
The primary outcome was mortality, defined as death within 10 years of study entry. Secondary outcomes were (1) time to death and (2) number of hospitalisations. We chose to study both odds of death within 10 years of enrolment and survival (time to death), given different likely uses of this information. While odds of death may be useful to clinicians when discussing future outcomes with patients, survival analyses may provide information that is more useful for healthcare planners.
Statistical analysis
All analyses were done using R Studio software V.1.2.5019 using ‘survival’, ‘pscl’, ‘ggplot2’ and ‘boot’ packages. Variables were described using mean and SD if normally distributed and median and IQR if not. Categorical variables are given as numbers (n) and percentages (%). Heat maps were developed to show multimorbidity pairings for the most common disease systems. We used complete cases of independent variables in the analyses. For each analysis, we used backwards elimination and included an interaction term for age and sex dependent on the effect on the model fit, captured by the Akaike information criterion (AIC). In all analyses, multimorbidity was defined in two ways; as a count of conditions, or binary outcome (yes or no). For ordinal variables, we selected the lowest variable category as the reference category, or for other variables the reference category was chosen arbitrarily.
Primary outcome
Binary logistic regression models were fitted to explore the associations between multimorbidity and death within a 10-year period after study entrance, controlling for sex, age (as a continuous variable), education level, marital status, urban or rural location, wealth, ethnicity and behavioural factors of smoking status BMI, physical activity status. The best model was chosen, using χ2 tests and through backward elimination ending when all the variables in the model were significant. Only participants who were followed up for the full 10-year period or died within the 10-year period were used in this analysis. Results are given in odds ratios (ORs) with (95% CIs).
Secondary outcomes
Cox proportional hazards models were fitted to explore the associations between multimorbidity and survival during the 10-year study period after checking the plausibility of the proportional hazard assumption. Covariables entered into the model were sex, age (as a continuous variable), education level, marital status, urban or rural location, wealth, ethnicity and behavioural factors of smoking status, BMI, and physical activity status. The best model was selected by improving the AIC through backward elimination. Backward elimination ended when all the variables in the models were significant. An interaction term between age and sex was inserted to improve the model fit. Participants who were lost to follow-up were censored at the last date of follow-up. Results are shown as hazard ratios (HRs) with 95% CI.
Poisson logistic regression models with a zero-inflation component were used to explore the associations between multimorbidity as a count of conditions and number of hospitalisations in a 10-year period. The AIC was used to justify the addition of the zero-inflation component to this model. Backwards elimination was done for both the binary model and the count model ending when all the variables in the models were significant. Results were generated using bootstrapping and are given as ORs with 95% CI for the zero-inflation component of the model, and incidence rates with 95% CI for the hospitalisation count part of the model. Only participants who were followed up for the full 10-year period or died within the 10-year period were used in this analysis. Covariates entered into the model were sex, age, education level, marital status, urban or rural location, wealth, ethnicity and NCD risk factors of smoking status, BMI and physical activity status.
Patient and public involvement statement
Participants were not directly involved in planning the study.
Results
Out of the 50 045 individuals in the original sample, 2162 participants were removed before analysis; 8 were missing BMI data, 2096 were missing physical activity data, and 58 had incorrect follow-up data (follow-up date entered incorrectly) leaving 47 883 cases for the analysis. 2297 participants were lost to follow-up during the 10-year period and were excluded from the binary logistic regression for 10-year mortality and analysis of numbers of hospitalisations within 10 years of follow-up (leaving n=45 586 complete cases for these analyses). These individuals were, however, included in the survival analysis (n=47 883) (figure 1). The demographic, lifestyle and disease characteristics of participants are shown in table 1.
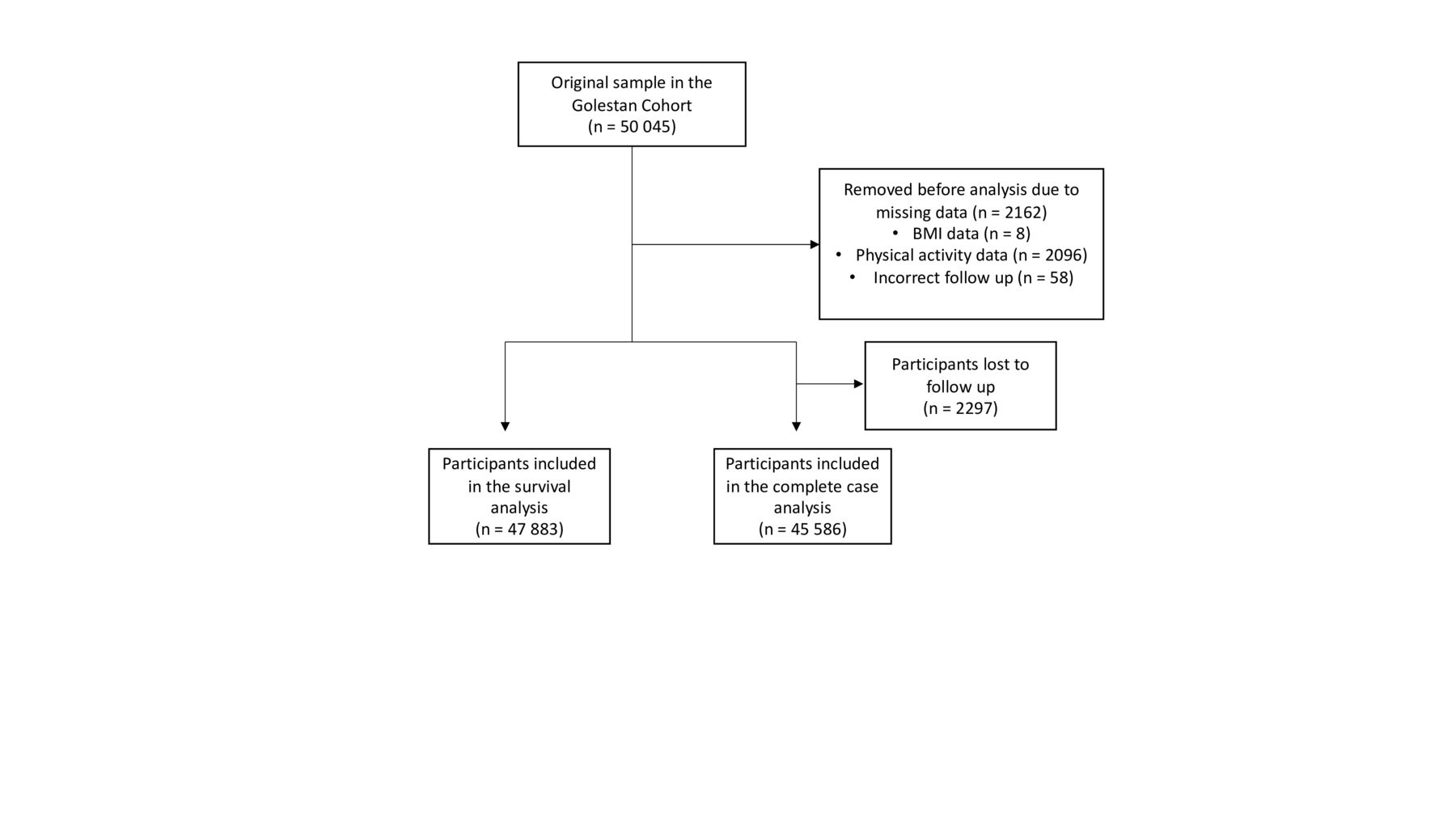
Study flow diagram showing the numbers of people who were included in the survival analyses and the complete case analysis. BMI, body mass index.
Demographic characteristics, NCD risk factors and morbidity categories of the participants included in the study (n=47 883)
Among the 45 586 individuals included in the complete case analysis, most were female (57.04%) and the mean age was 51.93 (SD 8.85) years. The majority of the participants had no schooling (69.88%), and most were married (88.09%). Eighty per cent of the sample lived in rural areas, and 75.53% were of Turkmen ethnicity. 14.08% were current smokers with a mean of 16.90 (18.25) pack years. 59.28% of people were overweight or obese with a BMI ≥25 kg/m2.
The average number of morbidities per participant was 1.05 (SD 1.19) and 59.45% had a least one morbidity. When categorising multimorbidity as two or more conditions 12 736 (27.94%) of the participants had multimorbidity (table 1). The most common disease domain was NCDs (56.65%) with CVD (37.15%) being the most common NCD system affected and hypertension (27.90%) the most common condition (online supplemental appendix table 3 shows conditions within disease domains). Having at least one condition in the GI system was also common (22.13%). At least one mental health condition was present in 8.62% of the population, but the condition was not possible to ascertain from the survey or medication information. The percentage of communicable diseases in the study population was 3.22% and tuberculosis constituted the majority (99.59%) of these. No medications were taken by 41.29% of the population, while 9.76% were on ≥4 medications. The most common combination of diseases systems was mental health and CVD (figure 2).

Multimordibity pairings for the most common disease systems (complete cases only n=45 586). The most common disease systems and their pairings are shown. Red indicates common pairings and blue, less common.
When considering complete cases, during the 10 years of follow-up, 5 411 participants died, 17 855 had one or more hospitalisations and the mean time to death was 5.52 years for those that died. The demographic information of the participants who died during the study period and occurrence of outcomes by demographics, lifestyle factors, condition and multimorbidity are shown in online supplemental appendix table 4. The characteristics of multimorbid versus not multimorbid participants in complete cases are found in online supplemental appendix table 5.
In multivariable analysis (table 2), the odds of being dead within 10 years after study entry increased significantly with increasing number of conditions, after controlling for age, sex, education, wealth, physical activity, smoking history and BMI. The OR was 3.57 (95% CI 3.12 to 4.08, p<0.001) for participants with four or more conditions compared with those with no conditions at baseline. Being male, older, unmarried, poorer, ever having smoked, less physically active and having a lower BMI were all significantly associated with greater odds of death within 10 years compared with their referent categories; area of living and ethnicity were not significantly associated with the outcome and was therefore excluded from the model. When categorising multimorbidity as a dichotomous variable (two or more conditions vs fewer than two conditions), multimorbidity was again significantly associated with increased odds of being dead within 10 years (OR 1.99, 95% CI 1.86 to 2.12, p<0.001) when controlling for other variables (online supplemental appendix table 6).
The OR of dying within 10 years, by demographic characteristics, NCD risk factors and number of conditions
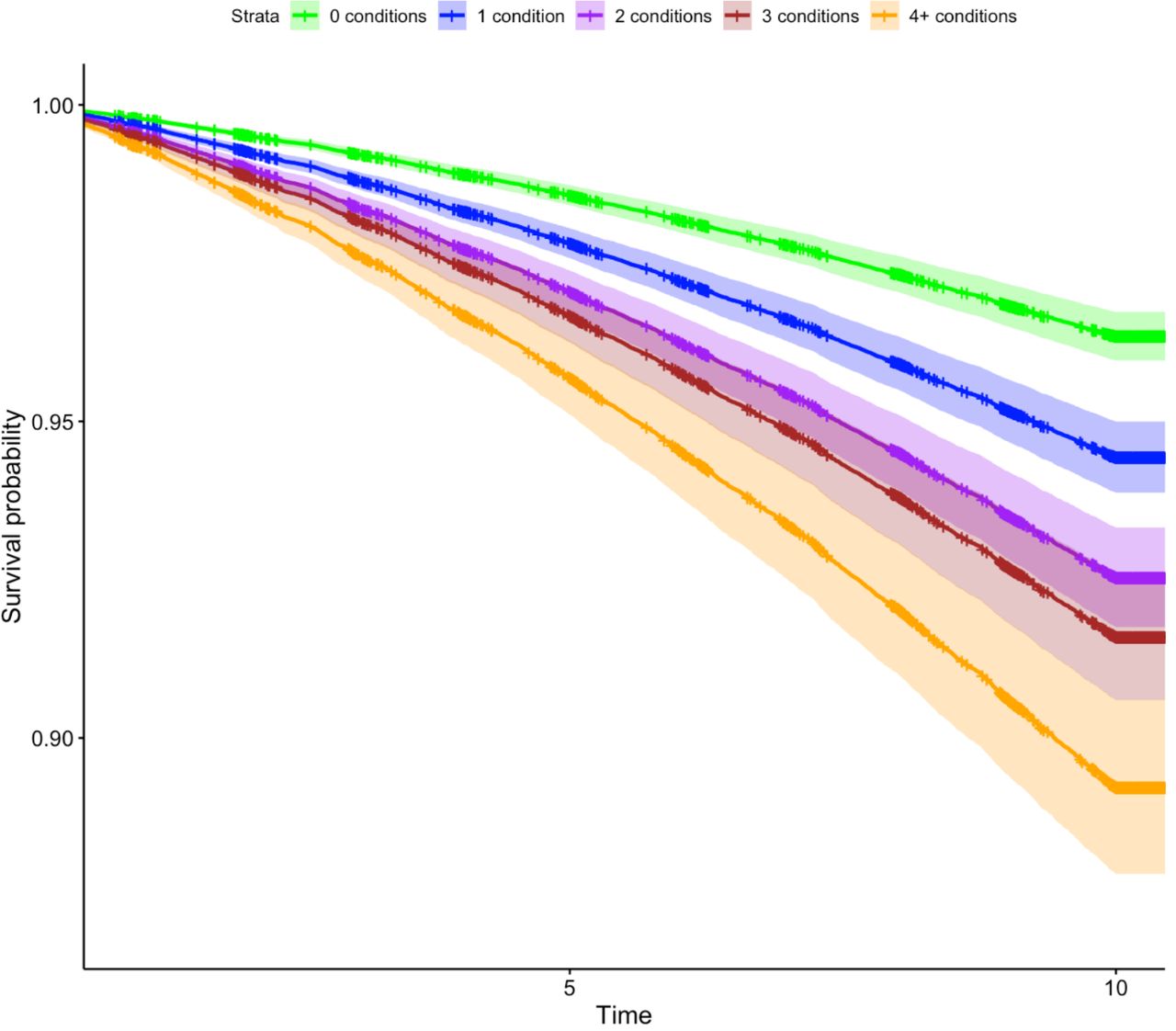
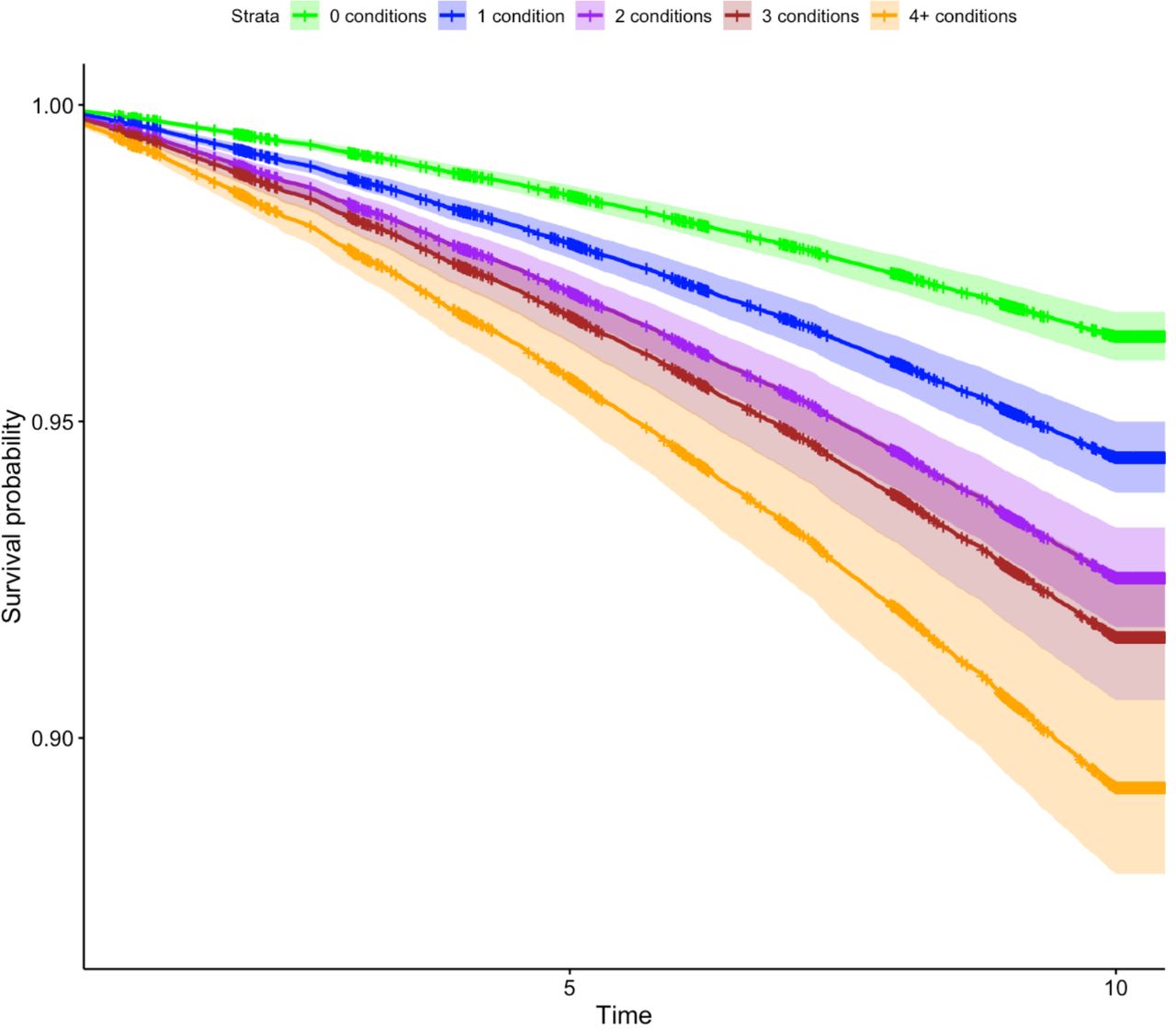
Results from the Cox regression analysis to explore association between multimorbidity and survival, including a term capturing the extra risk each year experienced by males to optimise model fit, are shown in table 3. Area of living was again excluded from the model due to lack of significance. The factors associated with the highest HR were multimorbidity with four or more conditions (HR 3.06, 95% CI 2.74 to 3.43), male (HR 3.17 95% CI 2.22 to 4.53), ever having smoked (HR 1.37, 95% CI 1.28 to 1.47) and older age (HR 1.08, 95% CI 1.07 to 1.08). The Kaplan-Meier plot for participants with 0, 1, 2, 3 or 4+ conditions is shown in figure 3. When categorising multimorbidity as a dichotomous variable (two or more conditions vs fewer than two conditions), multimorbidity was again significantly associated with an increased hazard of dying when controlling for other variables (HR 1.81, 95% CI 1.71 to 1.91, p<0.001) (online supplemental appendix table 7 and figure 1).
The HR of dying within the study period by demographic characteristics, NCD risk factors and number of conditions
{kind=link}
{kind=link}
{kind=link}
Survival of participants by number of conditions (n=47 883). Plots are shown controlling for demographic characteristics and behavioural factors.
The binary component of the zero inflation model (table 4) showed that the OR for being in the group who were not hospitalised decreased with number of conditions and also decreased with age, wealth, being non-Turkman ethnicity and ever having smoked. Having education, having a BMI between 18.5–25 kg/m2, and having a higher level of physical activity were protective against being hospitalised. Backwards elimination of the binary component of the zero-inflation model removed gender, marital and area of living. Also BMI categories were changed to BMI 18.5–25 kg/m2 vs not to improve model fit. The count component of the zero inflation model (table 4) showed that the number of hospital admissions an individual had significantly increased with the number of conditions when controlling for demographic and behavioural factors. The number of hospitalisations also increased with male sex, age and having education, being non-Turkman, smoker and BMI ≥25. The number of hospitalisations decreased with increased physical activity. Backwards elimination for the count part removed marital status, area of living and wealth. Also BMI was changed to BMI 0–25 kg/m2 vs 25+, and physical activity was changed to 1–2 vs 3 to improve the fit.
Zero inflation model of number of hospitalisations within a 10-year period of entering the study
Discussion
We found that multimorbidity was common in this large population of older adults from Iran. It was strongly associated with a greater chance of death within 10 years of follow-up, a lower hazard of survival, and a greater chance of hospitalisation and number of hospitalisations within the study period. The lack of access to good quality data from electronic health records in most LMICs means that most studies of multimorbidity use survey data—as we have done—which limits the ability to include severity of conditions in any analyses. Nevertheless, the definition of multimorbidity of the presence of two or more chronic conditions in an individual is internationally accepted.1 2 We chose to additionally categorise multimorbidity as a count of conditions. There was a strong dose response relationship between adverse outcomes and increasing number of conditions, with odds of death for those with four or more conditions being almost double that for those categorised as having multimorbidity based on having two or more conditions. Hence, this demonstrates that the impact of multimorbidity risks being under-estimated if the count of conditions is not used.
Many countries are attempting to achieve the Sustainable Development Goals (SDGs) by 2030, and in the last few decades Iran has implemented various reforms in order to achieve UHC, which is a key component of the health-related SDGs.31 The HTP which was initiated in 2014 has contributed by expanding insurance coverage, and enhancing financial protection.31 In fact, the out-of-pocket (OOP) expenditure on health in Iran was halved from 1995 to 2018, although it remained high at 35.83% in 2018 (the most recent year for which there are data).19 32 The Iranian healthcare system has a well-defined three-tier structure of primary, secondary and tertiary facilities, and even though the HTP was initially only implemented in hospital-based settings, it was later expanded to primary healthcare, which is where most patients with multimorbidity receive routine care. Thus health services development in Iran has accompanied economic growth. Although, some issues more familiar to countries that have less developed health services or economies remain, for example, there are no mechanisms to collect health insurance contributions from people without consistent income, thus compulsory health insurance coverage is not fully implemented.31 Moreover, many diagnostic services are only offered by the private healthcare sector which is not supported by the HTP, leading to high OOP for some people, and more mechanisms are needed to extend free health insurance coverage to the ones in need.31 Multimorbidity has been shown to be associated with greater mortality, hospitalisations, disability and low quality of life in HICs,1 5 17 33–35 but has been a neglected area in health research in LMICs with little evidence available on long-term outcomes of multimorbidity in these settings. Although it is likely that the long-term consequences of multimorbidity will be at least as hazardous in LMICs as in HICs, it is important to show this to raise the priority of managing multimorbidity in health system planning. Iran, being a rapidly developing country which has transitioned from being a lower-middle-income country to an UMIC during the study period may be an exemplar of the situation in other developing LMICs. Additionally, given the double burden of prevalent infectious diseases and rapidly rising prevalence of NCDs on a background of poverty, it is possible that the outcomes of multimorbidity will be worse in LMICs than HICs. Indeed, although the HRs found in our study were within the range of what was found in the previous studies from China,12 13 the association between number of conditions and mortality was stronger in our study than seen in studies done in HICs.36–38
As far as we are aware, our study is the first to look at hospitalisation as a long-term consequence of multimorbidity outside of an HIC setting. Our results from Iran are similar to what has been found in HICs, with increased number of conditions being associated with greater chance of hospitalisation per se and increased number of hospitalisations.35 39 These findings may well be an indication of what will be experienced in many other rapidly developing LMICs in the near future, and our evidence of the high proportion of multimorbidity and its strong association with serious long-term consequences, is therefore troubling.
The baseline proportion of multimorbidity (defined as two or more conditions) in our study is similar to previously estimated in Iran and other LMICs in similar age groups.9 11 40 41 Our finding that NCDs, especially CVDs, were the most common is to be expected, given global disease patterns.42 We have also shown that diseases in different domains (non-communicable, mental health or communicable) or disease system categories (eg, cardiovascular, GI, neurological) often co-occur. This lends weight to calls to develop health system-platforms of care, requiring a shift in emphasis from providing care for single diseases to an array of diseases.43 It is also important that UHC is broad in its coverage of conditions to address the issue of multimorbidity.44 However, caring for patients with multimorbidity is challenging, putting a burden on the health services and patients—who often are required to attend for multiple medical follow-up appointments. Delivering patient centred care—with fewer healthcare visits—needs to be balanced with the financial reality that many developing health systems face. As explained previously, Iran is still struggling to achieve UHC even after implementation of the HTP, and some of the poorest or more fragile people in the community might not be accessing healthcare due to lack of insurance and high OOP. To achieve UHC and deal with the burden of multimorbidity and its consequences which we have found will require continued political and financial commitment. The drive to ensure that care for chronic conditions is focused in primary healthcare settings will help achieve this balance, indeed, other middle income countries, such as South Africa, have embraced this approach with their Ideal Clinic programme.45 The Ideal Clinic programme was initiated in 2013 to improve the quality of primary healthcare facilities, even though the programme is new, and has to be strengthened, the preliminary results are promising.46 Moreover, stakeholders and policy-makers in LMICs can learn from some of the triumphs and errors of HICs.47
Although our main aim was to explore associations between multimorbidity and outcomes, there are other findings worthy of note. In particular odds of death were three times as high for men as for women when defining multimorbidity as count of conditions. Sex did not influence the risk of being hospitalised in our study, but did have an effect on the number of hospitalisations, with men having more hospitalisations. Our results are thus similar to findings in other studies.4 12 13 48 Even though women are generally more likely to have multimorbidity than men,11 35 49 differences in healthcare utilisation between women and men may be the reason for worse outcomes in men compared with women.50 51 We also found that wealth was associated with a lower risk of adverse outcomes—as have other studies using cross sectional data from LMICs.11 52 Low socioeconomic status is a well-known risk factor for CVD, multimorbidity and mortality in HICs.2 13 52 53 Hence ignoring the increasing burden of multimorbidity may increase inequalities in Iran and other LMICs.19
Although studies in HICs have found a U-shaped relationship between BMI and outcomes,54 we found that low BMI was associated with the highest risk of death within 10 years, reduced survival and increased number of hospitalisations. Being overweight had the lowest risk of adverse outcomes. Our findings are in thus line with studies which have demonstrated the ‘obesity paradox’, that is, being overweight is associated with improved survival in older age groups.54 Also the finding that low BMI is associated with a higher odds of death in our study may be due to reverse causality, with lower BMI occurring in people who are more severely ill. Being in a higher tertile of physical activity was associated with better outcomes, a finding which is in line with others who have shown that exercise, even when ageing, improves outcomes.55 56
Our study has several limitations. Polypharmacy has been associated with an increased risk of death in other studies.57 However, given that we defined the presence of conditions based on the use of medications it was not possible to reliably disentangle the contributions of polypharmacy or multimorbidity to outcomes in this study. Unfortunately, our study did not investigate the association with concordant (two or more conditions in one disease domain) or discordant (two or more conditions in a different disease domain) multimorbidity. Discordant multimorbidity has been found to have adverse outcomes on frailty, disability, and quality of life in a previous cross-sectional study from Burkina Faso.11 However, information on numbers of conditions in the communicable or mental health domains was not sufficient to enable such an analysis in this study. A major limitation is that we only had access to data on multimorbidity and physical measurements at baseline, and were not able to determine the effects of changes in multimorbidity status over the course of follow-up on outcomes. Another major limitation is that the study was set in the Golestan province which is largely populated by Turkmen, especially in the rural areas. Turkmen is a minor ethnic group in Iran forming around 2% of the total population. Turkmen may have a different diet, lifestyle and socioeconomic status to that of ethnic Persians which means our results may not be generalisable to the rest of Iran. Indeed, although ethnicity did not influence the odds of being dead in 10 years, there were—contrasting—effects of ethnicity on the hazard of death and hospitalisations. Nevertheless, removing ethnicity from our models did not substantially alter the relationship between our main independent variable of interest, multimorbidity and the outcomes (data not shown). Other limitations from our study include that the competing risk of death could have reduced the association between multimorbidity and hospitalisations, meaning that our estimates on hospitalisation are conservative. The prevalence of mental health conditions was surprisingly low, which could be due to under-reporting and stigma, meaning that the reported prevalence of mental health conditions (and hence multimorbidity) could be an underestimate. An additional reason for underestimation of multimorbidity is that the sample in the cohort was collected to study the incidence of oesophageal cancer, hence patients with GI cancers were excluded from the baseline sample. Upper GI cancer is a common cause of cancer related death in Iran, with gastric cancers being the most prevalent (0.2 and 100 per 100 000).58
That most of the conditions in this cohort were self-reported could introduce a risk of recall bias. However, the questionnaire was validated in a pilot and there was good correlation between self-reported food intake or opium use and biomarker measurements.26 59 Additionally, medications—which were recorded by data collectors—provided additional objective evidence of disease; although medications were assigned to diseases informed by the British National Formulary and clinical expert opinion, these assignments may not have been accurate in all cases. We could not ascertain reason for hospitalisation and specific cause of death using our data. Finally, to provide data in an important area where data are currently lacking, our study used a convenience cohort which was not nationally representative.
Conclusions
This is one of the first studies to report on longitudinal effects of multimorbidity in a middle-income country. Our study shows that the long-terms effects of multimorbidity on outcomes, such as mortality and hospitalisation, are just as hazardous, and potentially worse, in Iran as in HICs. Our results are relevant for future health policy and planning as there is a growing body of evidence on the increasing burden of NCDs and multimorbidity in LMICs, and given similar socioeconomic trajectories, low-income countries may face the similar issues of deleterious consequences of multimorbidity to Iran in the future. We recommend focusing more resources and global health funds around improving health system preparedness in LMIC settings to treat patients with multimorbidity in the years to come.
Data availability statement
Data are available on reasonable request. Information about the study design, updated interim analyses, ongoing substudies and relevant publications are available at www.ddrc.ac.ir. Specific proposals for national and international collaborations are welcomed. Initial proposals, which include the aim of the proposed study, the required data and a time-table, should be submitted to RM (ri.ca.sma@kelam) or PB (rf.crai@atteffob). The proposals will be discussed within the steering committee, which includes the principal investigators of the study and, if necessary, other experts according to the proposal’s theme.
Ethics statements
Patient consent for publication
Ethics approval
This was a secondary analysis of deidentified participant data. The initial study was approved by the ethics committee of the Digestive Diseases Research Institute, Tehran, University of Medical Sciences (OHRP-IRB-00001641). Before participation, a written informed consent was obtained from each participant, allowing investigators to use anonymised data for future analysis. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
MDW acknowledges support from the NIHR Newcastle Biomedical Research Centre. TM is supported by the National Institute for Health Research (NIHR) Applied Research Collaboration (ARC) West Midlands.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MLO and SI are joint first authors.
RM and JID are joint senior authors.
Handling editor Seye Abimbola
Twitter @drjackoids
Contributors SI statistically analysed the data. MLO and JID accessed and verified the data. MLO wrote the first draft of the manuscript with input from SI and JID. All authors contributed to the conception and design of the study, data interpretation and manuscript revision. All authors read and approved the submitted manuscript and had final responsibility for the decision to submit for publication. JD was the overall guarantor of the content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. This report presents independent research funded by the National Institute for Health Research (NIHR). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note RK and JID are joint last authors.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.