Article Text

Abstract
Introduction Prompt access to emergency obstetrical care (EmOC) reduces the risk of maternal mortality. We assessed institutional maternal mortality by distance and travel time for pregnant women with obstetrical emergencies in Lagos State, Nigeria.
Methods We conducted a facility-based retrospective cohort study across 24 public hospitals in Lagos. Reviewing case notes of the pregnant women presenting between 1 November 2018 and 30 October 2019, we extracted socio-demographic, travel and obstetrical data. The extracted travel data were exported to Google Maps, where driving distance and travel time data were extracted. Multivariable logistic regression was conducted to determine the relative influence of distance and travel time on maternal death.
Findings Of 4181 pregnant women with obstetrical emergencies, 182 (4.4%) resulted in maternal deaths. Among those who died, 60.3% travelled ≤10 km directly from home, and 61.9% arrived at the hospital ≤30 mins. The median distance and travel time to EmOC was 7.6 km (IQR 3.4–18.0) and 26 mins (IQR 12–50). For all women, travelling 10–15 km (2.53, 95% CI 1.27 to 5.03) was significantly associated with maternal death. Stratified by referral, odds remained statistically significant for those travelling 10–15 km in the non-referred group (2.48, 95% CI 1.18 to 5.23) and for travel ≥120 min (7.05, 95% CI 1.10 to 45.32). For those referred, odds became statistically significant at 25–35 km (21.40, 95% CI 1.24 to 36.72) and for journeys requiring travel time from as little as 10–29 min (184.23, 95% CI 5.14 to 608.51). Odds were also significantly higher for women travelling to hospitals in suburban (3.60, 95% CI 1.59 to 8.18) or rural (2.51, 95% CI 1.01 to 6.29) areas.
Conclusion Our evidence shows that distance and travel time influence maternal mortality differently for referred women and those who are not. Larger scale research that uses closer-to-reality travel time and distance estimates as we have done, rethinking of global guidelines, and bold actions addressing access gaps, including within the suburbs, will be critical in reducing maternal mortality by 2030.
- maternal health
- health services research
- obstetrics
- hospital-based study
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In sub-Saharan Africa, limited and conflicting evidence exists on the effect of travel time and distance on maternal mortality. The available evidence is based on research conducted in rural areas which used straight-line distances, assuming the women went to the nearest facility or health worker ‘guestimation’ of travel time.
WHAT THIS STUDY ADDS
Our findings in this study using closer-to-reality distance and travel time estimates showed that in Lagos, almost two-thirds of maternal deaths occur among pregnant women who travelled ≤10 km directly from home and arrived at the hospital in 30 mins.
There was a higher likelihood of maternal deaths with a 10–15 km distance and travel to a hospital that principally served suburban and rural areas. The odds of maternal death were statistically significant even when travel of 10–29 min was required for those referred.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Functional health facilities must be available within 10 km of every woman, with particular attention placed in the suburbs. Across board, robust systems are needed to support travel of pregnant women from the community to a health facility with capacity for emergency obstetrical care, with or without referral.
The 2-hour benchmark recommended by the WHO warrants a careful review with consideration given to more symptom-specific thresholds, urbanicity and recognition for the other delays that women may experience, including at referring facilities.
Introduction
Globally, 295 000 maternal deaths occur every year due to complications related to pregnancy and childbirth, including bleeding, hypertension, infection and abortion.1 These complications also lead to some pregnant women delivering babies in their third trimester who are born dead, otherwise referred to as stillbirths. It is estimated that approximately 2 million stillbirths occur annually.2 Approximately 70% of maternal deaths occur in sub-Saharan Africa (SSA), with Nigeria alone accounting for more than two-fifths of the global burden of maternal deaths.1 For stillbirths, over 40% occurs in SSA, with those occurring in Nigeria being about 10% of the worldwide burden.2 At present, the consensus strategy to reduce deaths related to pregnancy and childbirth, re-emphasised by the Sustainable Development Goals (SDGs), has predominantly focused on increasing access to prompt emergency obstetrical care (EmOC) provided by skilled health personnel (online supplemental tables S1 and S2A,B).3 4 Available research evidence indicates that prompt access to EmOC can lead to as much as a 50% reduction in intra-facility maternal deaths and a 45%–75% reduction in stillbirths occurring after the onset of labour but before birth.5 However, before a pregnant woman arrives at a health facility, delays in the decision to seek care (first delay), travel to reach appropriately equipped health facilities (second delay) and delay in receiving care (third delay) can increase the risk of death of the pregnant woman or that of her yet unborn child.6
Supplemental material
In 2009, the WHO recommended that health facilities be ‘available within 2–3 hours of travel for most women’, highlighting that this is the time it takes from onset of symptoms to death for a woman with postpartum haemorrhage as a complication of childbirth.4 Despite recognising the implication of travel delays on maternal mortality, studies on association of distance and travel time on maternal mortality are limited. When such studies have been conducted in SSA, they have been situated in rural settings and focused on travel time or distance.7–10 It is critical for studies attempting to understand the second delay to assess both travel time and distance, as though it is intuitive to expect both variables to increase or decrease together, some pregnant women travel for a long time despite living near a health facility.11 This is even more of an issue in urban and peri-urban settings, where traffic, poor road conditions and high population density are common features.11 Indeed, focus on these urban settings is crucial now more than ever before as almost 40% of the projected additional 2.5 billion urban residents globally are expected to concentrate in Africa.12 Our objective in this study was to assess the association between distance, travel time and maternal mortality among pregnant women who presented with obstetrical emergencies at public hospitals in Nigeria’s most urbanised state, Lagos.
Methods
Study design
Our study was a retrospective cohort study of pregnant women who presented as obstetrical emergencies at 1 of the 24 public hospitals (20 non-apex referral and 4 apex referral hospitals) in Lagos State (online supplemental tables S3 and S4).4
Setting
Lagos State, located in the southwestern part of Nigeria, has various geographical terrains (including land and water) and settlement types (including a central metropolis, suburbs, towns, slums and informal settlements) (online supplemental table S3). While primarily urban, the state has some rural parts in its extreme east and west. The state has 20 local government areas (LGAs) with population ranging from 117 542 (Ibeju-Lekki LGA) to 11 456 783 (Alimosho LGA). Population across the state was estimated to be about 26 million in 2019, with researchers projecting the state’s population will triple by the year 2050.13
The most recent national estimate of maternal mortality ratio (MMR) in Nigeria is 917 per 100 000 live births.1 However, there is no recent state-level MMR estimate. In Lagos State, a ratio as high as 1050 (95% CI 894 to 1215) per 100 000 live births has been reported in one of its urban slums.14 Institutional MMR between 987 to 2111 per 100 000 live births have also been estimated in Lagos public hospitals. More than one-third of maternal deaths are associated with delayed presentation of pregnant women at facilities.15
In Lagos, the most typical mode of transport is by road. However, in many parts of the state, the road infrastructure is poorly maintained, as evidenced by several potholes that sometimes make some roads impassable. Severe traffic congestions are common, with flooding during the rainy season making conditions worse. Road repair works are at best stopgaps and sometimes lead to more travel disruptions.16–18
Public health facilities manage more than two-fifths of all births in the state.19 However, many pregnant women use and indeed prefer public hospitals for many reasons, including the availability of 24/7 care, greater concentration of highly skilled health personnel and equipment and sometimes ‘free’ or reduced hospital cost.20 In emergencies, many pregnant women travel to the hospitals without health personnel support.11 If they require a referral, the Lagos State Ambulance Service occasionally help to transfer pregnant women between public hospitals.11 19 However, its effectiveness for patient transfer is limited by the traffic congestion and lack of willingness among other commuters to give way to ambulances.21
Data sources
Data were extracted from patient records over 6 months by the in-country research team, all of whom were qualified medical doctors, including consultant obstetricians, resident doctors and medical officers who had clinical experience working in the obstetrical units of the hospitals and were familiar with the patient records system in Lagos public health facilities. All team members were trained on using the pretested online data collection tool and ethical procedures guiding the research.
Participants
In each hospital, we identified and included all pregnant women who presented with an obstetrical emergency, because of themselves or their babies, between 1 November 2018 and 30 October 2019. Women who had an obstetrical emergency while on admission in the hospital were excluded, as their hospital journeys were not deemed critical to the pregnancy outcomes of women or their babies.
Variables
From the case notes, we extracted routinely reported data on socio-demographic characteristics, obstetrical history, travel to the hospital (including the day and period-of-day of travel, street name of women’s self-reported address, referring points of care, if any, and the final facility of care), obstetrical complication, mode of birth and pregnancy outcome. These data were collected because they helped us understand key characteristics of each included woman, allowed us to be able to map their journeys in an emergency and establish the outcome of care. All data apart from the pregnancy outcome were treated as dependent variables.
We categorised obstetrical complications in the case notes following WHO’s Monitoring EmOC guidelines, which highlights five major complications: obstetrical haemorrhage (antepartum or postpartum haemorrhage), hypertensive disorders in pregnancy (pre-eclampsia or eclampsia), pregnancy-related infections (sepsis), pregnancy with an abortive outcome and prolonged/obstructed labour (online supplemental table S1).4 We categorised pregnancy complications outside these broad categories, including premature rupture of membranes, oligohydramnios, polyhydramnios, ectopic pregnancy, footling breech, and previous surgical scar, as ‘other complications’.
Additional data gathering involving the estimation of driving distance and travel time using Google Maps (Google, Mountain View, California, USA), which offers closer-to-reality estimates compared with other commonly used methods,22 were required to characterise travel of pregnant women to the hospital fully. To achieve this, we geo-located the place of residence, referral points and destination facility for each woman in the application. For undiscoverable addresses on Google Maps, we contacted persons acquainted with the localities to check for spelling errors and re-attempted to locate the street. In cases where it was impossible to find specific travel points of the women, we labelled the case as untraceable (4% of cases). For those with traceable journeys, we extracted distance (in kilometres (km)) and travel time (in minutes (mins)) from Google Map using its ‘typical time of travel’ feature for the period-of-day of travel. We used specific time slots to collect travel time estimates for each period (09:00, 15:00, 18:00 and 21:00 for morning, afternoon, evening, or night journeys, respectively). In cases in which we could not tell the period-of-day of travel (33% of cases), travel time was extracted for the afternoon (15:00), as it was a mid-point estimate between the two known travel peak periods in Lagos (06:30 and 11:30 (morning peak period) and 15:00 and 19:30 (evening peak period)).23 We assumed that all used four-wheeled motor vehicles for travel since these are widely used by pregnant women in emergencies in SSA,24 25 and alternatives like motorcycles and tricycles had been banned in Lagos at the time of this study.11 26
For the dependent variable of maternal death, we aligned with the 10th edition of the International Classification of Diseases which defines maternal mortality as ‘the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes’.27
Data analysis
Following data cleaning and validation, we calculated cause‐specific case fatality rates and conducted descriptive analysis for pertinent demographic, obstetrical, travel and facility-related variables. In addition, we conducted a comparative analysis of median distances and travel times for pregnant women who travelled directly to the hospital and those referred. We prioritised median values, as these are known to be robust to outliers. We compared median distances and travel times of actual paths to care for referred pregnant women with an assumed scenario if they travelled directly to the hospital. We also compared travel distance and time for various obstetrical complications and types of referral institutions by outcome.
After converting age, travel time and distance into categorical variables, we conducted bivariate logistic regression to test the null hypothesis that there is no association between independent variables and maternal death, presenting crude ORs. By including statistically significant variables and others that have been shown as potential predictors of maternal death but not statistically significant in our analysis, we conducted multivariable logistic regression to determine the relative influence of the independent variables on maternal death while controlling for other variables. We used the Wald test to check if the independent variables in the model were significant. Model 1 incorporated relevant socio-demographic, travel-related and facility-related variables. Model 2A and model 2B are subgroup analyses that stratified model 1 by referral status for non-referred and referred women, respectively, as travel paths to care for both vary (online supplemental table S5). We reported both p values and 95% CIs of adjusted ORs derived from regression coefficients to show the strength of evidence and considered differences observed as statistically significant when p<0.05. Missing data were excluded from the analysis.
We mapped the location of public hospitals and maternal deaths disaggregated by referral status, using ArcGIS V.10.6 (Esri, Redlands, California, USA). All other analyses were done in Stata SE V.16.1 (StataCorp, College Station, Texas, USA).
Patient and public involvement
Patients and the public were not involved in the design, conduct, reporting or dissemination of this research.
Results
A total of 4181 pregnant women who presented with obstetrical emergencies in Lagos public hospitals were included in the study. Of the total sample, 182 (4.4%) were maternal deaths. Of the maternal deaths, 140 (76.9%) were women who travelled directly to the hospital, the other 40 (23.1%) were referred. Of the maternal deaths who were referred, 17 (40.5%), 10 (23.8%) and 8 (19.1%) were women who first travelled to primary health centres (PHCs), private hospitals and traditional birth attendants (TBAs), respectively. Most maternal deaths occurred in public hospitals based in the suburbs (129 (71.0%)), followed by rural areas (40 (22.0%)). Disaggregated by referral, deaths in both hospitals in the suburbs (94 (72.9%)) and rural areas (35 (87.5%)) were mostly women who travelled directly to a hospital. Cause-specific case fatality rates were 3.3% (pre-eclampsia or eclampsia), 3.5% (haemorrhage), 3.5% (sepsis), 8.8% (ectopic pregnancy), 12.2% (abortion) and 2.6% (other complications).
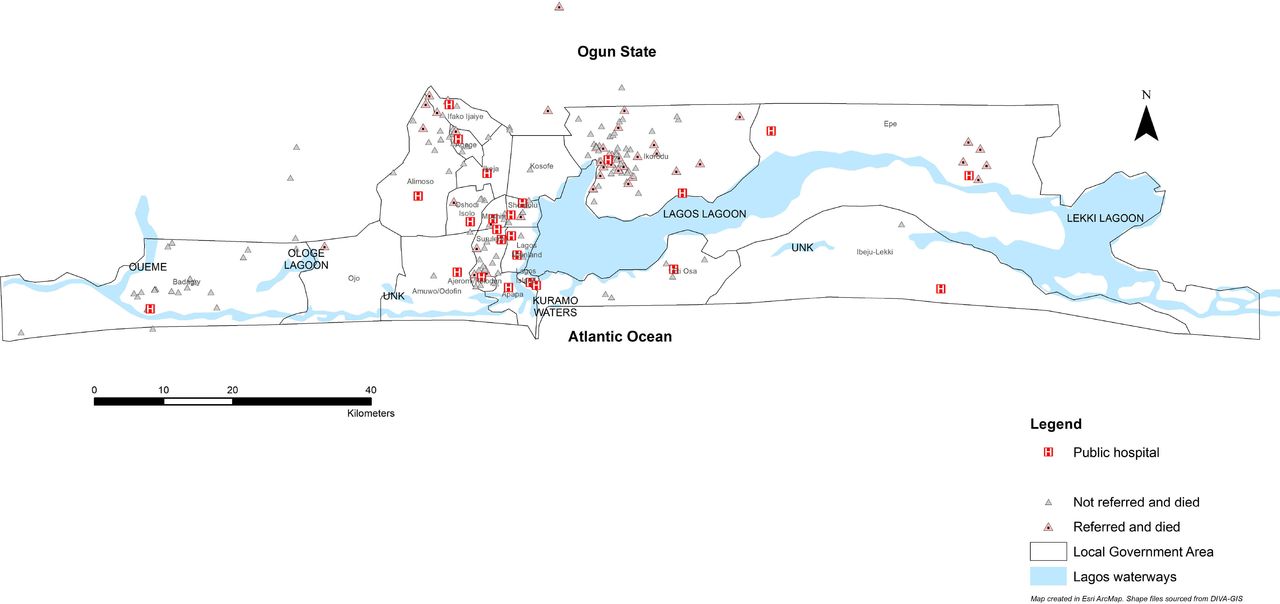
Maternal deaths involved women who lived across the entire state, with 8 of 182 (4.4%) coming from neighbouring Ogun State. Most maternal deaths occurred in the suburbs of Ajeromi-Ifelodun, Alimosho, Ifako-Ijaiye, Ikorodu, and in rural Badagry. Disaggregated by referral status, most maternal deaths among pregnant women who were referred occurred in suburban Ikorodu. All maternal deaths from rural Epe were referred, all of whom lived within 10 km of the hospital (figure 1).

Map of Lagos showing points of origin of referred and non-referred maternal deaths in relation to the location of public hospitals in Lagos.
Among the pregnant women who died, a greater proportion were aged 20–34 years (68.1%), married (86.3%) and self-employed petty traders (44.0%). Most women (93.4%) had no obstetrical complications in previous pregnancies. With the index pregnancy, most were multiparous (42.9%), had a singleton pregnancy (98.9%), were un-booked (ie, not registered for antenatal care (ANC) at the hospital they presented) (94.0%) and presented with abortion requiring evacuation (40.1%). For travel, most of those who died travelled on a weekday (80.8%), travelled afternoon or evening (58.6%) and travelled directly to the facility (76.9%). For those referred, most maternal deaths followed referrals from PHCs (40.5%). Majority presented in non-apex referral hospitals (90.1%), hospitals principally serving suburban areas (69.8%) and non-slum populations (75.8%) (table 1).
Socio-demographics, obstetrical history and characteristics of the index pregnancy
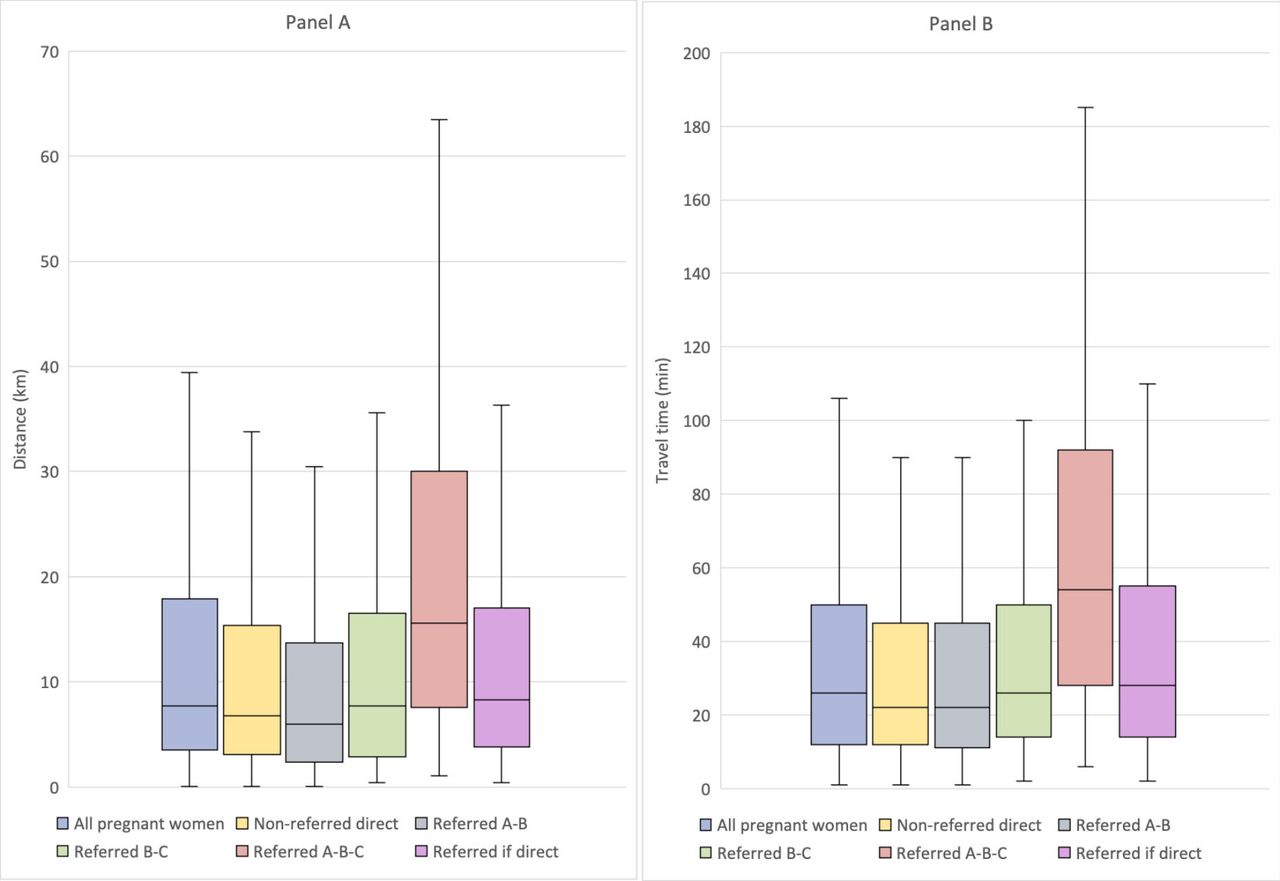
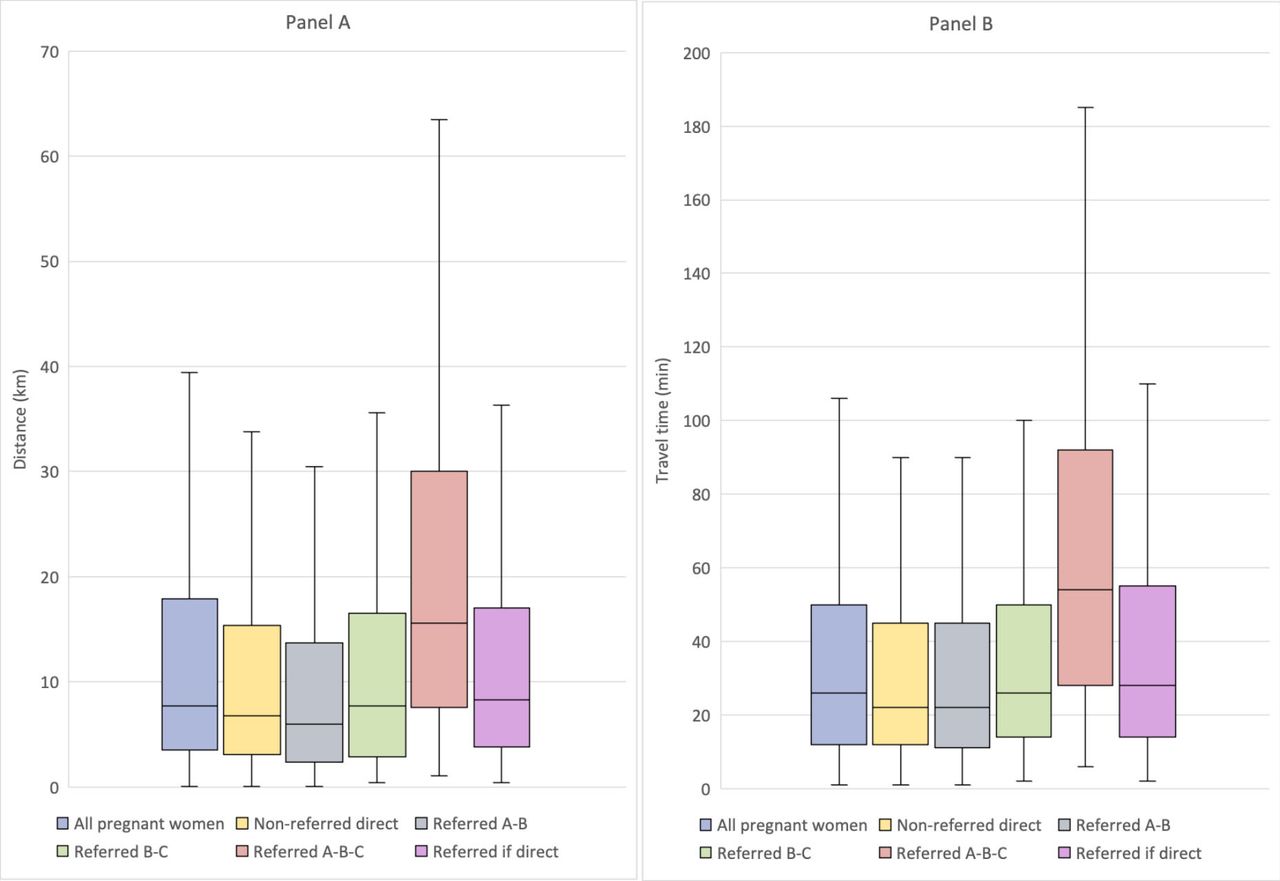
For all women, the median distance covered was 7.6 km (IQR 3.4–18.0), and the median travel time was 26 min (IQR 12–50). Pregnant women who travelled from home directly to a hospital travelled a median distance of 6.5 km (IQR 3.0–15.0) and required a median time of 22 min (IQR 11–45). Those who travelled from home to an initial facility before being referred to another travelled a total median distance of 15.6 km (IQR 7.6–30.0) and a median time of 54 min (IQR 28–92). Assuming these women had travelled directly to the final facility without being referred, they would have travelled a total median distance of 8.3 km (IQR 3.8–17.2) with a median time of 28 min (IQR 14–55) (figure 2). Women who presented as an emergency with a possible fetal complication and died travelled a longer median distance (16.2 km (IQR 6.8–33.7)) and for a longer time to the hospital (44 min (IQR 28–67)) compared with other complications (online supplemental tables S6a,b). Additionally, women who were referred from PHCs covered the shortest distance from home through the referral to a hospital (13.2 (IQR 6.3–23.8)) while women who were referred from TBAs used the least travel time from home through the referral to reach a hospital (41 mins (IQR 28–58)) (online supplemental table S6c).
{kind=link}
{kind=link}
Box and whisker plot displaying distance and travel time to the hospital for pregnant women with traceable journeys. All pregnant women: Complete travel for all women. Non-referred direct: Travel from home directly to a hospital that could provide care. Referred A-B: Travel from home to initial point of care that then referred. Referred B-C: Travel from the initial point of care that then referred to the final facility that could provide care. Referred A-B-C: Total travel for referred women from home through the initial point of care to the final facility. Referred if direct: Total travel for referred women if the journey was tracked from home direct to final facility.
Among all the women who died, a larger proportion of them travelled ≤10 km if they came directly from home (60.3%) and arrived at to the hospital ≤30 min (61.9%). For women who were referred and died, 71.4% travelled ≤10 km to the initial facility with 71.5% getting there in ≤30 min, while 65.5% travelled ≤10 km from initial facility to final facility with 72.4% getting there ≤30 min (table 2).
Description of distance and time to a health facility, by maternal outcome
Age, marital status, a complication in a previous pregnancy, number of gestations, booking status, maternal complications, distance and time from home directly to a hospital, total travel time, mode of delivery and principal settlement served by the hospital were statistically significant from the bivariate analysis (table 3).
Bivariate analysis for maternal outcomes
In Model 1, factors that were significantly associated with maternal death were having an obstetrical complication in a previous pregnancy (0.41, 95% CI 0.22 to 0.77), being booked (0.21, 95% CI 0.11 to 0.42), travelling 10–15 km (2.53, 95% CI 1.27 to 5.03) and travelling to a hospital that principally serves suburban (3.60, 95% CI 1.59 to 8.18) and rural areas (2.51, 95% CI 1.01 to 6.29) and delivering via assisted vaginal birth (3.37, 95% CI 1.76 to 6.46) or by caesarean section (0.39, 95% CI 0.22 to 0.71) (table 4).
Logistic regression showing association between maternal death and the selected independent variables
In Model 2A (subgroup analysis), odds remained statistically significant for those travelling 10–15 km in the non-referred group (2.48, 95% CI 1.18 to 5.23). In addition, odds became statistically significant for those travelling 120–480 min (7.05, 95% CI 1.10 to 45.32). For the referred group (Model 2B), odds became statistically significant for those travelling 25–35 km (21.40, 95% CI 1.24 to 36.72) and >35 km (49.63, 95% CI 2.39 to 103.05). Odds also became statistically significant for those travelling 10–29 min (184.23, 95% CI 5.14 to 608.51), 30–59 min (74.82, 95% CI 3.42 to 163.79) and 60–119 min (13.83, 95% CI 1.11 to 171.51) (online supplemental table S7).
Discussion
This study set out to explore associations between maternal mortality and travel distance and time in Lagos, Nigeria—a geographical area that is Nigeria’s most urbanised state and includes SSA’s largest megacity. Our findings showed that in such a principally urban SSA setting, the odds of maternal death were significantly higher for all pregnant women with an obstetrical emergency who travelled ≥10–15 km to care. Disaggregated by referral status, similar to all women, those who travelled directly had a higher likelihood of death if they travelled ≥10–15 km to care. As no other study has been conducted in a principally urban SSA setting, there is no comparator to our finding. When a woman is referred, we found that the odds of maternal death significantly increased when ≥25 km was travelled. This aligns with results from studies conducted in rural Guinea-Bissau and Tanzania.9 10 However, our findings contrast with a previous rural Burkina-Faso study, which concluded that there was no association between maternal mortality and distance.7 The discord might relate to the fact that this study focused on pregnancy-related deaths and not direct causes of maternal mortality.
Disaggregated by referral status, women who travelled directly to the hospital of care in our study had significantly higher odds of maternal death if they travelled ≥120 min. This travel time of statistical significance is lower than findings from a previous rural Mali study which reported a statistically significant association between institutional MMR and travel time only after women had travelled ≥240 min to a hospital.8 The observed difference might relate to the rural population selected or the method of determining travel time which involved guestimates from hospital workers. In our study, for those referred, odds of maternal death, which were statistically significant, increased appreciably when travel of ≥10 min was required. Keeping in mind that for women who died, over 60% travelled ≤10 km or ≤30 min for both referred and non-referred groups, this significantly increased odds of maternal deaths for women who were referred and travelled ≥10 min. This finding may suggest that they experienced a significant delay in the initial facility before being referred, at which point, so little could be done to improve their odds of survival. In SSA, care delays at referral points have been attributed to long waiting times, lack of skill and shortage of equipment and supplies in health facilities.6 Also, poor case management involving wrong assessment of risk, diagnosis or treatment has been reported, especially with private facilities and traditional birth attendants.15
Though our results support that there is an urban–rural divide, it also shows that even within hospitals situated in suburban areas, the odds of maternal death are even higher than those in the rural areas for all women, irrespective of their referral status. This suggests that there are issues even in the relatively urban–suburban areas. In Lagos, most pregnant women with obstetrical emergencies living in the peripheral rural areas usually travelled to public hospitals around them.28 In a separate study, we found that travel to care in this settlement type is typically prolonged in the suburbs.28 This blurring of the so-called ‘urban advantage’, or at least the ‘suburb advantage’, may explain the higher odds of maternal death in hospitals situated in the suburbs.
For other factors before and after travel to the hospital, our results showed a maternal death odds-reducing effect of having a previous obstetrical complication, booking and caesarean birth. It might be the case that knowledge and experience gained from previous pregnancies or following booking resulted in comprehensive birth preparedness plans for the index pregnancy, including timely decision to seek care, invariably reducing travel time to a facility.11 Caesarean birth was ‘protective’ from maternal death in our study. Contrarily, assisted vaginal birth led to significantly increased odds of maternal death. A clinical audit of these deaths is warranted to understand this association better.
To the best of our knowledge, this is the first study conducted in a principally urban SSA setting that explicitly and comprehensively explored association between travel time, distance and maternal mortality. Our study used driving distance and travel time estimates from Google Maps, which are more reflective of reality, compared with other estimation methods.22 Previous similar studies used Euclidean (straight-line) distances, assuming the women went to the nearest facility or health worker guestimates of travel time.7 9 10 However, evidence in the literature queries the realism and accuracy of both approaches to travel time and distance estimates. Women do not always go to the nearest facility, and if they do, their journeys are typically a lot more convoluted than travel in a straight line. Furthermore, since health workers did not make the journeys, they are not likely to make accurate travel time and distance estimates. Even if women themselves were asked, issues of recall bias have been raised by researchers.28–30 In addition, our study included women with emergencies across the entire pregnancy period and disaggregates by referral status, reflecting the different journeys that women follow to care.31 These are some of the key strengths of our study.
However, there are some limitations to keep in mind in interpreting our findings. First, while we mapped women’s journeys to health facilities based on data reported in their case notes, we cannot be sure that the women took the routes mapped in Google Maps or to other points of care not reported. Second, though Google Maps has been shown to provide closer-to-reality estimates of travel time and distance, it is still not perfect reality, especially in rural and remote areas.22 However, as already established, our setting for this research is principally urban, where networks of tarred roads allow for improved accuracy with Google Maps.32 33 Third, while we collected data for a year and accounted for diurnal variations using Google Maps, we could not account for seasonal variations, as this is not a functionality that is presently available on the application. Also, we have not captured the time women could have spent deciding to seek care (delay I). In addition, we did not have data reflecting the time between presentation at the hospital and the initiation of care or referral, as needed (delay III). Though these delays all contribute to maternal death,6 they would have occurred for both referred and non-referred women. As such, it does not significantly influence our findings. Additionally, we have not included private hospitals as endpoints of care, although public hospitals are recognised as the cornerstone for EmOC in SSA.34 Moreover, we could not fully capture women’s socio-economic and educational characteristics, which are also essential factors that influence access to care. However, both data are not routinely reported inpatient records in many SSA health systems.35 Furthermore, being a facility-based study, our study does not include pregnant women who died in transit. Finally, we observed wide CIs around the travel time and distance estimates for referred women. However, these wide intervals do not alter the validity of our findings, as it relates more to the absolute number of maternal deaths than the sample size.36 In any case, our conclusion regarding the association between travel time and distance and maternal death remains true across the interval. Considering this limitation, while recognising that maternal deaths remain a rare event in Africa,37 larger-scale research that includes more maternal death events, especially among women referred to care, is warranted for future research.
There are some implications for policy and practice for SSA health systems, as our study was conducted in the largest metropolis of the subregion. Before travel is even warranted for an emergency, engaging with ANC early in the pregnancy remains pivotal for optimising pregnancy outcomes. Skilled health personnel need to discuss danger signs, hospitals with the capacity to manage specific emergencies should they arise and travel plans with couples as part of birth preparedness. In addition to other points, this discussion should highlight the urgency of travel straight to a hospital for women even if they are only concerned about the health of their unborn child. Furthermore, negative experiences of health facility delivery that cause women to bypass nearer facilities in emergency to travel further need to be minimised.11 38 Efforts also need to be geared to reduce intrafacility delays at referring points of care to minimise maternal deaths among referred women. For governments, it is not enough to say health facilities have been ‘strategically placed’,39 facility location needs to be evidence-based. Planning geographical distribution of health facilities needs to ensure a functional health facility within 10 km of every woman and a robust referral system supported by patient transfer services to public hospitals. Some authors have suggested that the way forward to achieve the SDGs is to focus on hospital-level care instead of PHCs.40 Recognising concerns with costs associated with building new hospitals and the need for such investments to demonstrate value for money and be sustainable,41–43 we argue that close-to-community PHCs need to remain the fulcrum for SSA health systems. Sufficient training should be conducted with PHC health workers to help them better recognise complications, resuscitate and refer promptly.44 Any such capacity-building intervention for PHCs and private sector facilities needs to particularly focus management of abortion, which had the highest cause-specific case fatality rate in our study. As an alternative, governments in principally urban SSA settings should establish partnerships with quality-assured private providers who can be integrated into the EmOC referral network. This will be particularly crucial as private providers manage between 5% (Lusaka) and 64% (Lagos) of facility births in urban SSA settings.45 In addition, as every minute counts for the mother and her unborn child,46 ambulance services within the referral network need to be fully optimised to transfer women with obstetrical emergencies efficiently and effectively to hospitals that can manage them. This transfer should also be done at no cost to them, as many women already find the cost of care too high.47 For those travelling from their homes, access should not be a choice between ‘too far’ or ‘too poor’ to afford travel to an appropriate facility.48 In responding, governments also need to recognise that suburban might be the new rural and should therefore address access issues in the suburbs.
At a global level, our finding of statistical significance at a travel time of 120 min for pregnant women travelling directly to a hospital with the capacity to provide the care needed partly supports the applicability of the globally agreed benchmark of 2-hour travel.49 However, with many maternal deaths involving women who travelled less than an hour, there is a need to expand these guidelines to reflect delays permissible at referring facilities, recognising that women still face a median additional time of an hour even if they make it to hospitals that can provide the care needed.50
Conclusion
In conclusion, distance and travel time influence maternal outcomes following pregnancy and childbirth in different ways for women who are referred and those not. Leaving no one behind in achieving global targets of 2-hour travel to a hospital with the capacity to provide essential anaesthesia and surgical services, including caesarean for 80% of the population by 2030,3 49 will require more research like ours replicated in the many sprawling urban areas of SSA, rethinking of global EmOC geographical access guidelines and bold actions to get women closer and quicker to functional health facilities.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
We obtained ethical approval from the Research and Ethics Committees of the Lagos University Teaching Hospital (ADM/DCST/HREC/APP/2880) and Lagos State University Teaching Hospital (LREC/06/10/1226). The risk of identifying pregnant women in the study was substantially reduced by not collecting identifiers such as names and specific street numbers.
Acknowledgments
We are grateful to the Lagos State Government, in particular, the Lagos State Ministry of Health and the Lagos State Health Service Commission, for their support in gaining access to all state-owned facilities. We also thank the leadership of Federal government-owned facilities (Federal Medical Centre Ebute-Metta and Lagos University Teaching Hospital) included in our study for their support. We are indebted to the medical officers and residents who helped with collating case notes of pregnant women to be included in the study. We also thank the AXA Research Fund for supporting this research. The funder of the study had no role in study design, data collection, data interpretation or writing of the report.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @abankethomas, @AvokaKeon, @drmbalogun, @Coolgynae, @acameh
Contributors AB-T conceived the study. AB-T, CK-oA and CA designed the study. AB-T, KW, MB, TTF, AO and BBA coordinated data collection across the public hospitals. AB-T, CK-oA and UG-A did the statistical analyses with support from KW, MB and CA. AB-T, CK-oA, UG-A and CA wrote the first draft of the article. All authors critically reviewed the article, contributed to the interpretation of findings, saw and approved the final version of the article. AB-T is the guarantor.
Funding This research was funded by a grant provided by AXA Research Fund.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographical or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.