Article Text

Abstract
The field of ‘refugee health’ is generally understood in terms of the efforts of health professionals from a host country to provide care for humanitarian entrants. This paper attempts to undermine that idea, focusing instead on the service that health workers from refugee background communities are able to render, both to their own communities and to broader society, when barriers to their participation are made more equitable. The point of departure for this Practice paper is the 2019 pilot ‘Observership Program’ that was initiated by Mater Refugee Health in Brisbane, Australia. This was in response to, and in collaboration with, international medical graduates from refugee backgrounds. The two doctors who advocated for the programme had already independently embarked on a series of advocacy initiatives aimed at facilitating health workforce participation for members of their communities. In what follows we: outline the barriers to their medical registration and employment in Queensland, Australia; describe the process of setting up a 9-month clinical observership for two participants; and we reflect on the implications of the programme from a health policy and systems perspective. Ultimately, our contention is that because health systems are complex and adaptive, increased health workforce participation by members of marginalised communities has the potential to change the culture of the health system, making it more adept and responsive. Such, we propose, are the ‘ripple effects’ of addressing the obstacles to health workforce participation by members of refugee background communities.
- Health education and promotion
- Health policy
- Health services research
- Health systems
- Public Health
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
For international medical graduates (IMGs), entry into the Australian health workforce can be labyrinthine, with regulatory, cultural and economic costs that bar otherwise good doctors.
Members of refugee background communities ought not be understood solely as potential recipients of health services, but also as potential healthcare providers.
With the expenditure of some social capital on the part of established institutions, barriers to health workforce participation faced by IMGs from refugee backgrounds can be overcome.
Modest investments can lead to cultural change and improved responsiveness.
Introduction
What comes to mind when you think ‘refugees’, ‘members of refugee communities’ or ‘humanitarian arrivals’? Now think ‘health’ alongside ‘refugee’.
The conjunction ‘refugee-health’ typically generates a predictable set of responses: the need to take precautions1–3; concern for the vulnerable4–6; questions of obligation and charity7; concerns around systemic barriers to health equity8–10; and so forth. These are all crucial matters. Consider however, the ways in which the figure of ‘the refugee’ is cast in each of the responses above. Each set of responses yields a passive figure, although conceived as: occasion for preventative health system reform; the paradigmatic object of primary care and preventative health; basis of political deliberation; or grounds for review of the adequacy of the health system in place. The general understanding of health with respect to members of refugee communities is one that does not adequately account for the agency and the power—power understood in the simplest terms of the ability to do work or effect change—held by those within refugee communities.11 This is troubling. More so when one considers the lament of psychiatrist and philosopher of liberation, Frantz Fanon, that ‘the condemned of the world’ are ‘acted upon’.12–14
The following Practice paper offers a series of reflections by administrative and medical staff members of Mater Refugee Health (MRH), an urban, Australian refugee health service, on their Observership Program. Following a series of discussions with an independent academic, the authors documented their recollections and thoughts on actions taken by and alongside international medical graduates (IMGs) from refugee backgrounds, in order to establish a pathway for medical registration in Queensland, Australia. These were further deliberated at a subsequent workshop, with a focus on the pragmatic (what more can be achieved within existing system constraints) and the normative (what high-income health systems owe to migrant communities). The pages that follow present less a series of knowledge claims or research findings, but the learnings and considered reflections of practitioners eager to be in dialogue with others grappling with similar issues. In so doing, we contribute our understanding of what a health system like Queensland’s has to learn from migrants, thereby promoting ‘learning health systems’.15 In addition, online supplemental appendix 1, ‘Overview of barriers and enablers to employment for International Medical Graduates from a Refugee Background in Queensland’, is an analysis of the status quo led by Dr Butoyi, who along with Dr Aqrawe, advocated for the development of and pioneered the Observership Program. This provides further insight into the genesis of the programme, particularly the thinking which drove it, while respecting the independence of those doctors.
Supplemental material
Genesis
Between 2003 and 2005, there were numerous deaths of surgical patients at Bundaberg Base Hospital in Queensland, who were in the care of an Indian born American surgeon. The highly publicised series of court cases that followed, including a 2010 conviction which was subsequently quashed in 2012, unsurprisingly resulted in a regulatory and attitudinal shift.16–19 A new national body, the Australian Health Practitioner Regulation Agency (AHPRA), commenced operations in July 2010 and in 2012, the Queensland-based Recruitment, Assessment, Placement, Training and Support (RAPTS) programme for IMGs ceased.20 21
Seven years after the RAPTS pathway closed, two IMGs from refugee backgrounds led the process that would see MRH setting up an Observership Program.
At our first meeting JB explained that he was looking for some supervision or placement. He had expressed a desire to do an observership, but this again was not something we had ever considered. Some months passed and I didn’t connect with JB again until I saw him at a primary care event. It sounded like he was getting some experience in a general practice but mainly volunteering with new arrivals from his own community. JB was still looking for a hospital observership but again I was not sure how to go about it (DS).
Around the same time, MA was independently pursing a similar opening.
I was invited by the Department of Home Affairs to a meeting that was initiated by their community engagement team after meeting MA at a settlement forum. The meeting was attended by a few government representatives, settlement providers but no Hospital and Health Services representatives besides me, as a Mater Hospital person. MA spoke about her experience and those of several other doctors from refugee backgrounds. She explained about her career and her passion for medicine and how in the short time she had been in Australia, she was desperately working towards re-entering her profession. As the meeting progressed it seemed clear that the missing piece was access to local workplace experience and networks (DS).
The path to medical registration for these two IMGs thus involved initiating contact with senior health service administrators and policymakers, advocating on their own behalf and on behalf of others in similar situations. This is in keeping with the finding that: ‘[i]n addition to navigating the AMC (Australian Medical Council) and MBA (Medical Board of Australia)/AHPRA processes’, IMGs must often also negotiate ‘a range of other government and non-government organisations to formalise their […] employment arrangements’.22 The road to health workforce participation for migrants in general, and those from refugee communities especially, often demands a heavy toll.23–26
I am an IMG and I relate to the barriers that IMGs face when trying to enter the Australian medical workforce. I tell you; it is not an easy or cheap process at all. The only thing I have achieved thus far is creating a profile for the AMC which took me ages, with a bit of back and forth with them, not to mention that I have already spent around $1000, just on creating that profile and verifying my certificate. I have been trying to contact my Medical School back in Kenya to help with the verification process, but no one has ever picked up my call or responded to my email. So, I’m in limbo. It is frustrating to say the least, but I am not giving up yet (MN)!
The hefty administrative costs—the demand that individuals bear the financial burden of medical registration where the benefits of that registration are likely to accrue to the common good—robs the health system of the benefit of those qualified workers from diverse backgrounds for whom the required sums of money are out of reach. The resulting loss is both clinical and cultural. It is also counterproductive, given Australia’s heavy reliance on IMGs. Granted, it is difficult to get an accurate picture of this reliance. For instance, a recent study noting that 40% of the regional, rural and remote general practitioner (GP) workforce in Australia is made up of IMGs draws on a 2012 report27; another, noting parity with the USA and the UK, draws on a 2005 study to suggest that around a quarter of all doctors in Australia received their medical training abroad28; while a third proposes that 42.9% of doctors in Australia are migrants, based on a 2014 WHO report which in turn appears to have based that figure on 2001 data.29 Nevertheless, while the statistics are blurry, the general picture that emerges from the synthesis of the evidence at hand is of a health system that substantially supplements an inadequate domestic supply of medical personnel and an uneven distribution of healthcare workers with IMGs.19
The Observership Program
In 2019, a pilot Observership Program was initiated at the Mater Hospital with the support of willing clinical supervisors from various departments, managed within existing resources of the MRH (online supplemental appendix 2).
Supplemental material
My instinct was to call upon the Mater networks. JB helped to draft a paper outlining the barriers for IMGs from refugee backgrounds and why an observership would be a positive steppingstone (online supplemental appendix 1). I shared this with Mater directors and doctors in the relevant areas and we collectively crafted the idea of a ‘pilot’ Observership Program. Being a ‘pilot’, we were able to be targeted but at the same time this was uncharted territory and we were very careful to not over promise how the Mater could make a difference. Over the next 9 months, MA and JB started their observership in Emergency, General Practice, Anesthetics, Cardiology and Infectious Diseases (DS).
This initial Observership Program lasted for 9 months and provided the two doctors an induction into the Australian Healthcare system, taking little for granted and beginning with basic institutional and clinical concerns (online supplemental appendix 3). They observed clinical care and institutional culture across a range of settings. On completion of the programme, both successfully applied for Junior House Officer positions in Queensland Health hospitals. In keeping with findings elsewhere, the relationships and insights developed during the observership helped to both mitigate barriers and facilitate entry into a new system.30 31 Yet, it is important to note that even with this additional support,
Supplemental material
There continue to be many barriers to employment that have largely been unseen, many of which I was simply unaware of, or to be honest, hadn’t considered carefully enough. It feels like there is this mass of complex issues that we really do need to unpack, and we’re starting to, but there is clearly significant bias in the system that we need to better understand and address (RF).
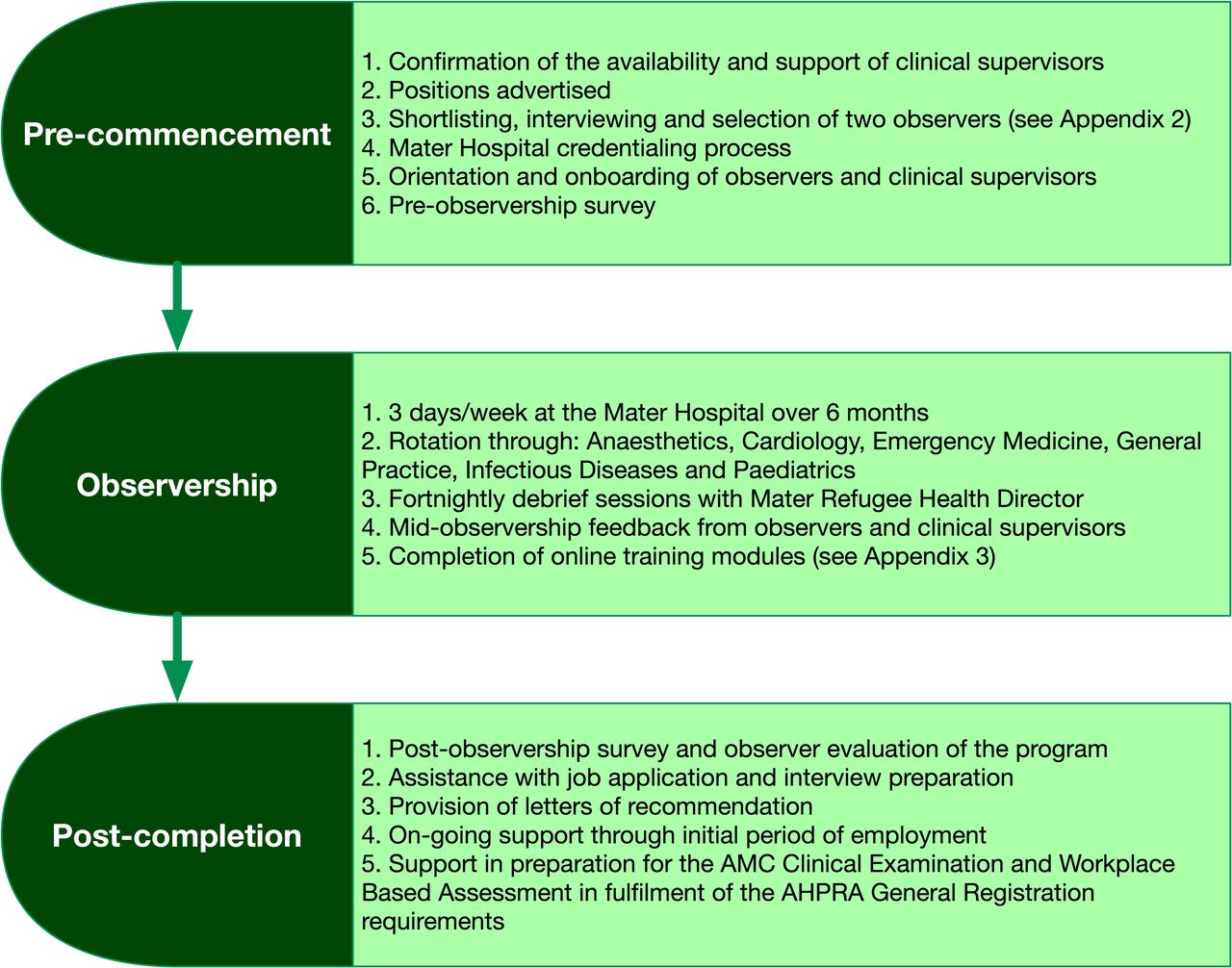
In late 2020, a proposal was drafted to allow for a more formal and structured Observership Program for IMGs from refugee backgrounds at the Mater Hospital (see figure 1), which was subsequently approved by Mater Executives in early 2021. MRH secured philanthropic funding to enable the implementation of this programme, which aims to support both the IMGs from refugee backgrounds and their clinical supervisors during the observership period. At present, the programme only accommodates two IMGs per observership duration, but with the institutional learning that is expected over subsequent iterations, the model in place is expected to expand. Not only may there be more IMGs entering the programme, there may also be scope to recruit nurses and allied health professionals from across refugee communities (see figure 2). In fact, a pilot Assistant In Nursing Internship for refugee background nurses to assist in the transition to working in the Australian Healthcare system has already been initiated.

Operational overview of the Mater Observership Program. AHPRA, Australian Health Practitioner Regulation Agency; AMC, Australian Medical Council.

{kind=link}
{kind=link}
Conceptual outline and anticipated benefits of the Mater Observership Program. IMGs, international medical graduates.
Lessons
The establishment of the MRH Observership Program has resulted in important learnings for all involved. These revolve around the reconfiguration of the relationship between a health service provider and the communities that it serves, focusing on complexity, the importance of peer-support and institutional leadership.
The healthcare setting is not only a site of the operation of prevailing social forces, but also a site of the generation and reiteration of social hierarchies.32–34 However, as with all complex, adaptive systems, an intervention at one site can lead to change at multiple other locations, and even fundamentally alter the entire system.35 36 Change at any site within the system is likely to produce ripple effects (see figure 2). Therefore, greater incorporation of members of refugee communities into the health workforce, along with the collaboration and close contact with longstanding members of that system that this entails, offers the possibility of that basic human contact that Fanon pleads for at the end of Black Skin, White Masks. The change that such contact can engender was evident as colleagues came to better understand the refugee journey and the experience of medical professionals who have worked in different healthcare settings. Not only does this leave open the prospect of a shift in horizons at one hospital, which impacts responsiveness and patient care there, it also suggests the possibility of wider cultural change across the health system.37 38 Yet as Fanon also makes clear, this work of enlightenment is a heavy burden to bear. Moreover, the experience of human contact can be violent.34 39 40
The second lesson has to do with leadership. From inception, the Observership Program was predicated on the value of the selected IMGs to the institution, given their experience. While attending to refugee health is in keeping with the Mater Hospital’s social justice mission, where the distinction between justice and charity is extremely important,41 a strong message was sent from leadership across the hospital that the observers were valued professionals. Clinical supervisors supported this by identifying, and exploring with the observers, gaps in knowledge and areas where there was a risk of being misunderstood. For example, one supervisor spent time practicing interview skills with observers to unpack cultural expectations, both with respect to medical hierarchy and patient perceptions. There were also multiple, candid discussions about the complexities of medical culture within the Australian health system. This is a difficult area for further investigation, given the tumultuous operations of power which are at play beneath the veneer of culture, as well as the too prevalent conflation of cultural norms and clinical skills—or as Dall’Alba puts it, the ontological dimensions of learning to be a medical professional in a particular context.42 43
Leadership at the individual, person-to-person level, was extremely important and yielded tangible results, the effects of which are still palpable. Institution level interventions also proved fruitful. For instance, the structure of the Observership Program included a networking component with other hospitals throughout Queensland. This was undertaken to facilitate employment pathways and to share learnings. In addition, discussions with medical administrators across a variety of health settings, with Directors of Clinical Training, and with general practices, opened opportunities for multi-hospital and primary care observership opportunities. Work is also being done at the policy level to embed workforce strategies through the Refugee Health Network Queensland in collaboration with Queensland Health, which is currently updating the Refugee Health and Wellbeing Policy and Action Plan (2017–2020).44
Finally, there was the key learning regarding peer support. The value of having two observers, rather than just one, was increasingly apparent, becoming most obvious as the two doctors began to apply for and then transition into their medical jobs within Queensland Health. Further study is needed to investigate the stressors that the two observers may have experienced which were not apparent to the MRH team. What seems clear at this stage, however, is that the presence of a companion undergoing the same process is helpful.
Conclusion
I feel personally that the journey to practice for these doctors needs to be told, and their skills and strengths recognised within the Australian medical system. I think that if we can do this and develop pathways and some small cultural change within our system, that might be a step towards bigger change (RC).
Many would accept that among the goals of the health system, the provision of care ought to be a high priority. Few would argue against the benefits of having a body of heath care providers who are representative of and proximate to the communities they serve.45 46 Fewer still, one hopes, would bemoan a health workforce that is not only as diverse as the population it serves, but which also models fluency in intercultural communication and exchange. The discussion above provides an insight into one attempt to work towards this. We hope that it will encourage others in their attempts to effect positive change to global health, however small the interventions.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The Mater Hospital National Health and Medical Research Council registered Human Research Ethics Committee declared this project exempt on 8 October 2021. Review Reference: EXMT/MML/79865(V3).
Acknowledgments
The Mater Hospital Observership Program would not have been possible without the participation and assistance of many people at the Mater, nor the financial assistance of the Bennelong Foundation. Their contributions are sincerely appreciated and gratefully acknowledged. We also extend our sincere appreciation to Dr Jean De La Croix Butoyi and Dr Manal Aqrawe for their leadership through this process.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Stephanie M Topp
Twitter @NMMoraa, @bryanmukandi
Contributors All authors conceived and contributed to the writing and revision of this manuscript. All authors approved the final version of the manuscript. BM, as guarantor, accepts full responsibilty for the conduct of this study.
Funding The Mater Refugee Health Observership Program was supported by the Bennelong Foundation. This article emerged in part as a result of work on the Australian Research Council DECRA project, ‘Seeing the Black Child’ (DE210101089).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.