Article Text

Abstract
Introduction Primary postpartum haemorrhage (PPH) is the leading cause of Nigeria’s high maternal mortality rate. This study investigated the effectiveness of a set of multifaceted interventions to manage and reduce PPH in selected secondary referral health facilities in Nigeria.
Methods This is a quasi-experimental study using an interrupted time-series design to assess a set of multifaceted interventions that address factors identified by stakeholders as associated with PPH. Interventions were implemented at two regional general hospitals, with a general hospital in the same region as the control. Intervention participants were women during antepartum and clinical and administrative staff. Cases of PPH were determined in women at delivery. The outcomes measured were the incidence of primary PPH and related deaths during the study period. Analyses included a comparative description of characteristics of the women, trend of time-series data at intervention and control hospitals, and multivariable analysis of factors associated with PPH occurrence.
Results Monthly numbers of primary PPH were collected at participating hospitals over 21 months for 18 181 women. Intervention hospitals represent 54% vs 46% in control hospitals. Time-series analyses show a significant downward trend in intervention hospitals. The overall incidence of primary PPH was lower in the intervention hospitals than in the control hospitals. Multilevel regression adjusted for hospital-level effect showed a 68% reduction in odds of PPH cases at intervention compared with control hospitals. There were 12 PPH-related maternal deaths in one of the control hospitals, with no deaths in the intervention hospitals.
Conclusion We conclude that multiple interventions that address identified challenges in the prevention of primary PPH can potentially effectively reduce reported primary PPH in Nigerian referral hospitals. This approach is relevant for scaling the development of policies and programmes to prevent primary PPH and maternal mortality in Nigeria.
- Maternal health
- Prevention strategies
- Intervention study
- Obstetrics
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is evidence that primary postpartum haemorrhage (PPH) is one of Nigeria’s leading causes of maternal mortality.
Lack of adherence to recommended WHO and International Federation of Gynecology and Obstetrics (FIGO) guidelines for PPH prevention and management is prevalent in Nigerian hospitals.
A practical approach to reducing and managing PPH must address multiple codependent patients, providers and administrative factors.
WHAT THIS STUDY ADDS
An intervention that addresses multiple PPH predisposing factors is associated with reduced PPHs and PPH-related deaths.
The use of oxytocin was prevalent in participating control and intervention hospitals.
Lack of antenatal care and initiation of birth in non-hospital settings are risk factors for PPH and potential adverse events.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
An approach to mitigate the occurrence of PPH and PPH-related adverse outcomes should include patient, provider and hospital administrative factors.
The top leadership of the health facilities in Nigeria and relevant stakeholders should be involved in designing PPH prevention interventions.
Government policies should provide incentives for poor and women with low education to use antenatal care and have hospital births, which will expose them to antenatal training on PPH risks.
Introduction
An estimated 58 000 maternal deaths were reported in Nigeria in 2015. Evidence indicates that primary postpartum haemorrhage (PPH) is one of the leading causes of maternal mortality in Nigeria,1–4 with over 20% attributable to PPH.5 6 Due to the increasing use of new technologies based on the recommended WHO and FIGO guidelines, it is apparent that the incidence and fatality due to PPH may be declining in other parts of the world.7–9
By contrast, the incidence and case fatality attributable to PPH continue to rise in Nigeria and other sub-Saharan African countries,10 which we believe is attributable to the poor use of the recommended guidelines and women’s inappropriate maternal healthcare-seeking behaviour.
In 2018, the Nigeria Demographic and Health Survey reported that only 43% of women used skilled birth attendants during childbirth.11 This implies that a predominant proportion of pregnant women using unskilled and untrained traditional birth attendants would not obtain appropriate care to prevent or manage PPH at delivery.
Even for those receiving skilled delivery care, the inadequate use of PPH prevention and management protocols has remained a major concern in Nigeria. In a previous study,12 we showed that most cases of PPH in a referral facility in Nigeria were attributable to women who had not received antenatal care and who had intended to deliver outside a healthcare facility.
Consequently, in 2016, we began the implementation of research aimed at reducing maternal mortality in Nigeria’s referral hospitals, with a specific focus on preventing and reducing deaths due to PPH and other leading complications of pregnancy.13
Using mixed methods (qualitative and quantitative) research in eight purposefully selected Nigerian hospitals from four geopolitical zones of the country, we identified several factors associated with the high rate of PPH and related maternal deaths. These included (1) the lack of a strategy and commitment by hospital managers to prevent and manage PPH and other causes of maternal mortality,14 (2) limited knowledge among providers of the current recommended methods and protocols for the prevention and treatment of PPH,15 (3) shortage of drugs and facilities (including regular blood supply) for the management of obstetric emergencies as recommended by the WHO,16 and (4) inadequate counselling and education of pregnant women on the prevention and treatment methods for PPH.17 18 We likewise undertook a retrospective confidential review of maternal deaths occurring in one of the hospitals, the Central Hospital Benin City, during the period.2 Of the 18 maternal deaths reviewed during the period, 10 deaths were due to PPH, while in all cases of death, the lack of blood or blood products in the hospital was the ancillary-associated cause of death.2
Based on these results, we began an intervention study collaborating with key management staff of two referral hospitals—the Central Hospital, Benin City, and the General Hospital, Minna—to address PPH and PPH-related maternal deaths. We held a series of meetings with all staff of the maternity sections of the hospitals, discussed potential challenges, and consequently developed a strategic plan to reduce and prevent PPH and reduce associated maternal mortality by 50% over 2 years.18 The chief medical directors of the hospitals then led the implementation of a set of mutually agreed interventions in collaboration with relevant hospital departments (obstetrics and gynaecology, child health, laboratory services, blood transfusion services, etc) over 2 years.
This paper aimed to report the results of the analysis comparing reported cases of PPH and indicators of PPH quality of care management between the two intervention hospitals with two control hospitals of similar status where the interventions were not carried out. We believe the results of this study will help develop substantive policies and practices for improving the quality of maternal care for the prevention of PPH and related deaths in Nigeria.
Methods
The study was quasi-experimental research that included specific interventions in two referral hospitals (one in southern Nigerian and the other in northern Nigeria), while two referral hospitals in comparable locations in southern and northern parts of the country served as the control hospitals. The baseline research consisted of mixed-method qualitative and quantitative research to inform the intervention on the incidence and determinants of PPH-related morbidity and mortality in the hospitals. The design of the study and the results of the formative research have been reported elsewhere.13
Intervention versus control hospitals
The Central Hospital in Benin City, South–South Nigeria, and the General Hospital in Minna, Niger State, in the North–Central part, served as the intervention hospitals. By contrast, the Central Hospital Warri, South–South Nigeria, and the General Hospitals in Suleja and Abuja, in the North–Central region, served as the control hospitals. The four hospitals are referral hospitals that serve large populations of women in four states and two geopolitical zones of Nigeria. We decided to use two intervention and two control hospitals to ease management, ensure data accuracy and maximise local efforts. The Central Hospitals in Benin City and Warri are 80 km apart and serve similar populations of women. Similarly, Abuja, Suleja and Minna hospitals are in the same sociocultural and geographical area and are only 120 km apart. The Abuja hospital was discontinued as a control due to logistics and operational challenges after 9 months, and the Suleja hospital was substituted. Hence, this ensured the sociocultural characteristics of the women and the structure of intervention and control hospitals in the same region are comparable. The Benin and Warri hospitals have comparable annual maternal mortality (AMM) and caesarean section rates. The Minna hospital’s volume of deliveries and AMM rate double that of the Abuja hospital because it serves a broader population (see online supplemental appendix 1 for data). Both midwives and doctors attend to deliveries in all participating hospitals.
Supplemental material
Intervention activities
We commenced a series of interventions in October 2017 to prevent and improve the quality of PPH management in intervention hospitals. The interventions were codesigned by administrators and clinical staff in relevant clinical and diagnostic departments of the hospitals and were led by the chief medical directors and the directors of administration of the hospital. This was to ensure the rapid uptake and sustainability of the intervention activities. Study coordinators submitted reports of intervention activities to the research centre periodically so that the research director could evaluate the fidelity of intervention activities. The specific activities included the following.
Development of a strategic plan
This activity took place over 3 months before the commencement of the intervention. It involved a community conversation with the stakeholders that raised the issue of high maternal mortality attributable to PPH in the hospitals. We identified the strengths, weaknesses, opportunities and threats in enabling the hospitals to tackle the problem and conducted structured and unstructured interviews with clinical staff in the maternity departments of the hospitals to identify their knowledge, attitudes and practices of WHO-recommended procedures for preventing and managing PPH. The results have been published elsewhere.14 These interviews identified the challenges related to PPH prevention and management, which were used to develop a strategic document to prevent maternal mortality and PPH in the hospitals.15 The strategic document was shared with all staff and health providers to reduce PPH and related maternal mortality by 50% in the two hospitals over 2 years. We discussed the challenges of providing optimal maternal healthcare in the hospitals and identified shared strategies in the strategic plan. Workshops were delivered in the intervention hospitals to disseminate the strategic plan to the staff and to agree on the planned remediating activities.
Staff retraining
We implemented two workshops 6 weeks apart, each lasting 2 days, to improve the knowledge and skills on prevention and management of PPH for doctors, nurses and midwives in the hospitals. The training focused on the provision of maternal healthcare and the active management of the first, second and third stages of labour. We specifically focused on providing training on the FIGO and WHO recommendations for managing the third stage of labour, especially active management using intravenous oxytocin as a first-line drug, ergometrine as a second-line drug, and misoprostol as third line and adjuvant treatment.7 Attendees at the workshops also underwent training on management of traumatic causes of PPH (including cervical and vaginal lacerations), respectful and non-abuse care, patient counselling, the use of treatment PPH algorithms for decision-making, risks assessment and management, and the management of emergency obstetrics care, especially concerning PPH. A multimodal approach that included lectures, discussions, case and scenario studies, role plays, demonstrations and hands-on sessions was used. Finally, we produced an algorithm on PPH management (see online supplemental appendix 4) and distributed it to all health workers in the hospital’s maternity sections and displayed it in the labour wards to remind health providers.
Supplemental material
Blood donation drive
Blood shortage for transfusion was repeatedly mentioned as a major cause of maternal mortality due to PPH in hospitals. Hence, we revised the blood use policy in the hospitals to prioritise the availability of blood and blood products for pregnant women. Working with the hospitals’ haematology and blood transfusion units, we fielded an intensive blood donation drive and stored it in blood banks for future use in the hospitals. We advertised on radio and TV, and a blood donation day was launched by the commissioners of health and the chief medical directors of the two hospitals. In addition, during weekly health talks of pregnant women with their spouses, family members and attendees were informed of the blood donation efforts in the hospitals, and they were encouraged to participate. Within weeks of launching the blood donation drive, the supply of blood significantly improved such that the lack of blood became a rarity in the hospitals.
PPH education program
We redesigned the health education for pregnant women to include PPH prevention activities. We introduced monthly health talk programmes on Saturdays over 3 hours that allowed adequate time to share relevant information and answer questions raised by the women. Experts in the field delivered the health talks, and invited attendees were pregnant women registered in the hospital, their spouses and all health providers in the hospital, hospital managers, policymakers, and other interested persons. Programme activities included distributing information leaflets and other behavioural change communication materials on the causes and prevention of PPH and the importance of skilled delivery to prevent and treat PPH. We also developed a specific information booklet titled Answers to Frequently Asked Questions by Pregnant Women. The booklet included answers to the women’s questions on PPH and related issues. It was printed and shared with the women and their spouses and translated to the Hausa language for women in Niger State, who predominantly speak Hausa. We conducted 22 monthly health talks in the hospitals, with over 2500 pregnant women attending during the period.
Maternal death reviews and surveillance (MDRS)
Clinical and nursing staff were trained to use the Federal Ministry of Health protocol for conducting MDRS. The methodology has been reported elsewhere.19 All maternal deaths, including those due to PPH that occurred in the hospitals during the period, were reviewed to determine deaths’ medical and social causes. We subsequently implemented specific remedial measures to correct the deficiencies in clinical management that led to maternal deaths.
Data collection
We collected monthly data prospectively in participating hospitals that included the number of deliveries, the number of deliveries complicated by PPH, cases adequately managed according to standard WHO protocols and the number of PPH-related maternal deaths. These data were collected with a standard protocol by trained data collectors in the hospitals over 21 months. The first 3 months represented the baseline period. Intervention and follow-up activities occurred in the 6 months that followed. The study timeline chart is shown in online supplemental appendix 2. The data were collected with CAPI software installed on smartphones, which were returned to the central processing unit at the Women’s Health and Action Research Centre for collation and data analysis.
We used a structured questionnaire to obtain information on sociodemographic characteristics of all women who delivered in the participating hospitals. Process and outcomes data included receiving oxytocin immediately after birth. Data on ergometrine and misoprostol use, birth outside the health facility, the mode of delivery (whether vaginally or by C-section) and referral-out from the hospitals to other health facilities were also collected. Other data collected included PPH cases, maternal deaths due to PPH and maternal death due to other causes.
Patient and public involvement
Clinical staff, administrators and women and family members who attended antenatal clinic at the intervention hospitals participated in intervention activities.
Data analysis
Analyses consisted of describing characteristics of women who delivered at intervention and control hospitals. We used the t-test and Wilcoxon rank-sum test to determine the difference in means of age (parametric) parity and gravidity (non-parametric) between intervention and control hospitals. χ2 was used to assess the difference in the distribution of categorical variables. We also described differences in the counts of PPH-related deaths and the use of oxytocin and misoprostol.
Time-series analysis was used to determine trends and differences between control and intervention hospitals. We aggregated time-series data by month for the count of PPH and rates of PPH/1000 (monthly count of PPH divided by a monthly total of women who delivered). We explored various smoothing methods (simple exponential smoothing, double simple exponential and 3-month moving average) to smooth the roughness in the series and potentially reveal any underlying trend. Unmeasured hospital factors may influence when and how the intervention is implemented, and operational differences may affect PPH occurrence. Therefore, we used multilevel regression to determine the effect of the intervention activities on PPH occurrence among the women in the intervention compared with control hospitals while controlling for potential hospital-level cluster effects and patient-level factors.20 A random intercept model was fit with patient factors at level 1 and hospital at level 2.21–23 We expected hospital staff to implement intervention activities as they complete the training starting from the fourth month of the study duration. Therefore, we estimated the intervention effect would gradually increase as the duration of the study increased. We segmented the study duration into baseline (1st–3rd month), intervention (4th–9th month) and immediate postintervention (10th–15th month) and (16th–21st month) to assess if the effect of the intervention varies with time. The baseline period served as the reference. In addition, we explored the interaction between segments of study duration and the intervention to see whether the odds of PPH vary at the intervention and control hospitals over time. We assumed combining all samples in the primary multilevel analysis might obscure the effect of study duration on PPH occurrence and expect the effect of intervention activities on PPH occurrence will increase with time in the intervention hospitals. The results of this analysis are presented in table 1. All analyses were conducted using SAS V.9.4.
Logistic regression adjusted odds of reported postpartum haemorrhage in intervention and control hospitals with an interaction term
Results
Descriptive
Data were prospectively extracted from 18 181 women during the study period. Of these, 54% were from intervention (General Hospital in Benin and Minna), while 46% were from control hospitals (General Hospital in Warri, Abuja and Suleja). Control and intervention hospitals were significantly different in most characteristics. Women in control hospitals were slightly older, employed, had higher gravidity, did not receive antenatal care, lived in rural areas and had a higher % of women who had PPH than the intervention hospitals (4.14% vs 2.14%). Intervention hospitals had a higher percentage of women with antenatal care (23.42% vs 18%), higher average parity than in the control hospitals (2.27, SD 1.77, vs 1.85, SD 1.62); 99.2% were married and were urban residents (90.5%) (table 2). Of all women diagnosed with PPH, 14 died. Twelve deaths were due to PPH, and two were due to other causes. All PPH-related deaths occurred in General Hospital, Warri. Almost all women received oxytocin during delivery in intervention and control hospitals, 94% in Suleja and 100% in the other hospitals. In addition, misoprostol was widely used for all PPH cases in the intervention and control hospitals. The correlation coefficient of misoprostol use and the count of PPH in the control hospital was 0.95, while it was 0.98 in the intervention hospitals.
Descriptive characteristics of women who received care at intervention and control hospitals
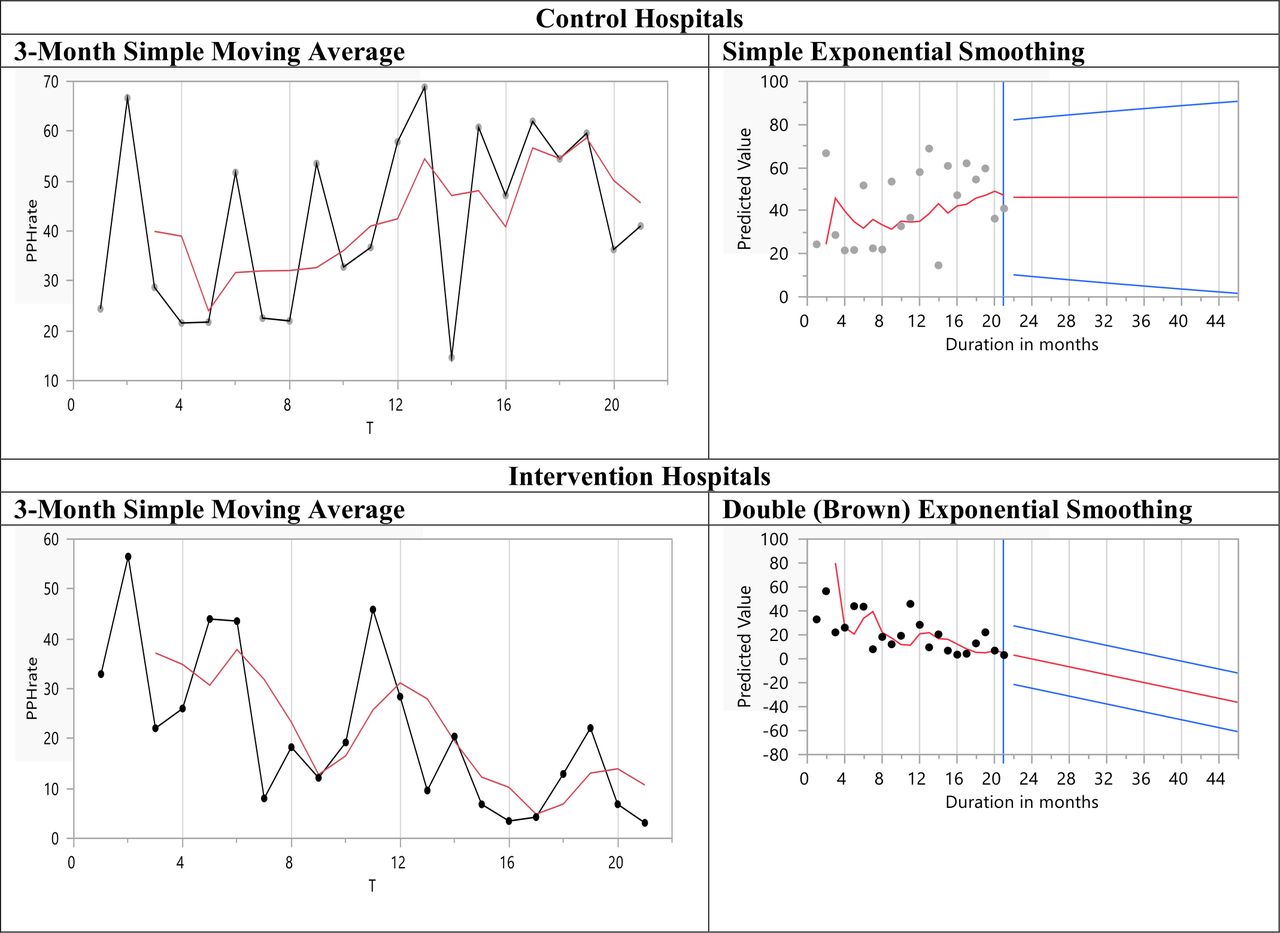
Time-series analysis shows that PPH rates vary, and there was no clear trend in the 15 months of the study in both intervention and control hospitals. There was a considerable overlap of PPH rates in the first 8 months. The rates diverged in the 14th month, with rates slightly up in the control hospitals and decreasing in the intervention hospitals. The trend during this period was not sustained or significantly different between the control and intervention hospitals (online supplemental appendix 3). The smoothed plot of the series further supports a downward trend in the intervention hospitals compared with the control hospitals (figure 1).

Plots of postpartum haemorrhage rates over the study duration in control and intervention hospitals. Simple exponential smoothing and double brown exponential smoothing methods have the lowest mean absolute percentage error and mean average error for the control and intervention hospitals, respectively. Months 1–3 represent the baseline period.
Multivariate results
Multilevel regression was used to evaluate the likelihood of PPH among women in the intervention hospitals (table 3). The result shows that the intervention was associated with a 68% decrease in PPH (OR=0.32, 95% CI 0. 0.23 to 0.44). Factors associated with lower odds of PPH include antenatal care (OR=0.51, 95% CI 0. 0.42 to 0.63), non-referral for care as compared with those referred from other facilities (OR=0.22, 95% CI 0. 0.42 to 0.63) and education beyond the primary level. Increasing parity was associated with 23% increased risks of PPH. Results from the regression model that assessed the interaction of study duration and the interventions show significantly decreasing PPH odds with time in the intervention compared with control hospitals. The odds of PPH in intervention hospitals decreased as the study duration increased. There was a 31% reduction in PPH odds during the intervention period compared with baseline that further decreased by 47% immediate postintervention and by 63% reduction in the last months of the study period (see figure 2 and table 1).
Multilevel regression adjusted odds of reported postpartum haemorrhage among women at intervention compared with control hospitals

{kind=link}
{kind=link}
Probability of postpartum haemorrhage by time segments in intervention and control hospitals between October 2017 to June 2019. T1, baseline, 1st–3rd month; T2, 4th–9th month, intervention period; T3, immediate postintervention, 10th–15th month; T4, 16th–21st month.
Discussion
The study’s objective was to assess the effectiveness of a set of multifaceted interventions in reducing the prevalence of PPH in two intervention referral hospitals compared with two hospitals without the interventions. The results show a lower incidence of PPH in the intervention hospitals in a time-series comparison that lasted 21 months after the onset of the intervention. After multivariable analysis that controlled for potential confounders between the intervention and control sites, the results suggest interventions were at least 68% effective in decreasing PPH incidence during the period.
The study identified the risk factors for PPH in both intervention and control sites to be the non-use of antenatal care, a referral from other health facilities, increased parity and decreased maternal education level. These results are consistent with published studies on PPH risk factors from other sub-Saharan African countries.24 25 Being a multifaceted study, it is difficult to identify the specific aspects of the intervention that accounted for the reduced prevalence of PPH as reported in this study. However, a multifaceted design that addressed the multiple factors predisposed to PPH was the preferred choice because stakeholders identified various predisposing factors during the formative research and the intervention planning stage.
The intervention components were strategic planning with hospital managers, the retraining of providers on PPH prevention and management, intensive drive for blood donation, the health education of pregnant women and their family members about PPH and the institution of MDRS. The initial strategic planning was helpful as it provided a forum for the hospital workers to identify the challenges related to the high prevalence of PPH and to have a stake in the change process. The involvement of the hospital’s top leadership in developing and leading the programme activities galvanised the project’s effectiveness and would likely help sustain the activities over time.
The training of health providers on the use of active management of labour (including the third stage of labour) was also likely an enabling factor. Formative research had reported inadequate knowledge of doctors and midwives working in the units on the recommended WHO protocols as a leading challenge in the prevention of primary PPH.15 These protocols were therefore revised, taught and made available to the health workers in the intervention hospitals during the period. Additionally, PPH management in the intervention hospitals ensured that oxytocic drugs, including oxytocin, ergometrine and misoprostol, were available in the maternity wards throughout the period, with no stock-outs reported. However, at the project’s conclusion, the availability of oxytocic drugs between the intervention and control hospitals was similar. Both groups of hospitals reported equal proportions of women treated with various oxytocic drugs during the project cycle. The reduced incidence of PPH in the intervention hospital may therefore be due to better compliance in the use of the drugs for the active management of the third stage of labour in the intervention hospitals compared with the control hospitals.
The health education of the pregnant women and their home caregivers about pregnancy and its complications was also a major component that may have contributed to the relative success of the intervention. Compared with control hospitals, women who registered and received antenatal at intervention hospitals had much lower odds of having PPH than women in control hospitals, suggesting a benefit from participating in health awareness sessions. Indeed, within the intervention hospitals, higher odds of PPH occurred in women who did not receive antenatal care in the hospitals but who were transferred in labour from other hospitals. The evidence that PPH incidence was significantly lower in booked women who received antenatal further illustrates the effectiveness of the intervention and delivery care in intervention hospitals compared with similar women in the control hospitals. The education and counselling of women during pregnancy likely ensured pregnant women’s compliance with labour management and PPH prevention methods.
Strengths and limitations
To the best of our knowledge, this is one of a few purposefully designed intervention research that seeks to prevent PPH, focusing on care professionals, pregnant women and health facilities in sub-Saharan Africa.26 27 Previous reports often focus on single interventions that test the effectiveness of new drugs or other single components in preventing or managing PPH.16 28–30 The design of our intervention that involved local stakeholders in identifying the challenges relating to the prevention of PPH in a set of institutions, followed by the codesign of interventions with hospital managers, likely propelled the project’s effectiveness, which will likely enhance the long-term sustainability of the project. One of the project activities was establishing confidential reviews of maternal deaths and surveillance, which was previously not in place in the hospitals. The heightened commitment of the hospital management to prevent PPH and maternal mortality enabled the establishment of this accountability process that was designed to identify and resolve specific causes of maternal mortality in the intervention hospitals. Despite the end of the project activities, these processes have continued in the hospitals due to the way and manner the intervention was designed and implemented. The study did not specifically focus on elucidating the effect of the intervention on case fatality and PPH-related maternal mortality. This was because we conjectured that the effect of the intervention on mortality would take some time to manifest and may likely not occur during the immediate period. However, the study documented that all 12 PPH-related deaths occurred in one of the control hospitals, with no deaths in the intervention hospitals during the period. Although these results were not subjected to statistical significance testing or statistical modelling because of their small numbers, they suggest that the intervention may reduce the number of PPH-related deaths and maternal mortality in the hospitals over time. Other limitations include our use of only two hospitals in the control and intervention arms of the research, limiting the generalisability of findings. In addition, hospitals selected were not randomised, and PPH cases were not observed firsthand but determined prospectively from records. Also, while the patient characteristics in the two regions may differ, the intervention and correspondent control hospitals were in the same region, which minimises the differences across regions. We also do not have data on anaemia, blood transfusion, coagulation disorders, uterine anomaly, other potential clinical indicators and incomplete ergometrine data, which do not allow a deeper understanding of intervention effects on PPH management. We hope to explore these factors in a future follow-up study.
Conclusion
This study indicates that multiple interventions that address the identified challenges in preventing PPH can reduce reported cases of PPH in Nigerian referral hospitals. The involvement of the top leadership of the health facilities and the codesign of the interventions with relevant stakeholders in the hospitals increased the project’s effectiveness and sustainability. This approach is suitable for scaling the development and implementation of interventions to prevent PPH and maternal mortality in Nigeria and similar regions worldwide.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by WHO and the National Health Research Ethics Committee (NHREC) of Nigeria (number NHREC/01/01/2007-16/07/2014, renewed in 2015 with NHREC 01/01/20047-12/12/2015b). The participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seema Biswas
Contributors Conception of the study: FEO; design and execution of intervention activities: FEO, RO, WI, HG and LFCN; formative research: OE, RO, LFCN and HG; manuscript development and preparation: OE, BE and CE; data analysis: BE; supervision of the study and data collection: OE, VO, KA, BI and LFCN. FEO accepts responsibility for authoruship and contributorship of the manuscript.
Funding The project was funded by the Alliance for Health Policy and Systems Research, WHO, Geneva through its programme on improving implementation research on maternal health in developing countries (protocol ID A65869).
Competing interests None declared.
Patient and public involvement Patients and the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.