Article Text

Abstract
The WHO’s report Health literacy development for the prevention and control of non-communicable diseases (NCDs) delivers practical what-to-do how-to-do guidance for health literacy development to build, at scale, contextually-relevant public health actions to reduce inequity and the burden of NCDs on individuals, health systems and economies. The key premise for health literacy development is that people’s health awareness and behaviours are linked to lifelong experiences and social practices, which may be multilayered, hidden and beyond their control. Meaningful community engagement, local ownership and locally driven actions are needed to identify health literacy strengths, challenges and preferences to build locally fit-for-purpose and implementable actions. Health literacy development needs to underpin local and national policy, laws and regulations to create enabling environments that reduce community exposures to NCD risk factors. Deficit approaches and siloed health system and policy responses need to be avoided, focusing instead on integrating community-based solutions through co-design, cognisant of people’s daily experiences and social practices.
- Health education and promotion
- Public Health
- Control strategies
- Prevention strategies
- Health policy
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
The WHO has introduced a framework for health literacy development to improve the prevention and management of long-term conditions such as cancer, diabetes, heart disease, lung disease and mental health problems (also known as non-communicable diseases, NCDs). The WHO report https://www.who.int/publications/i/item/9789240055339
Health literacy development takes a global health approach that respects all people worldwide, prioritising their local wisdom to drive bottom-up and top-down processes to improve health policy and health services and to reduce health inequity.
The framework recognises that families and communities already work together to avoid NCDs, and that governments must invest and build better ways to help the health system (including community health workers, family doctors, hospitals) support people by making it easier to find, understand and use health information and health services.
Health literacy development must underpin local and national policy, laws, and regulations to create enabling environments that reduce people’s exposures to NCD risk factors promulgated through misinformation, disinformation and advertising by commercial groups with vested interests.
The framework provides countries with current and practical evidence to improve the health literacy responsiveness of services, strengthen the health literacy of the community and undertake targeted programmes to support priority groups who may be missing out on receiving or easily accessing health information or healthcare.
Introduction
Non-communicable diseases (NCDs) are the world’s largest cause of mortality and account for over 74% of the global burden of disease.1 From 2000 to 2019, NCDs led to 277 million premature deaths among people between the ages of 30 and 70 living in low-income and middle-income countries.1 This global burden is exacerbated by the COVID-19 pandemic and the rapid rise of misinformation—easily propagated through technology and social media—and which has disrupted NCD prevention and control efforts and exacerbated health inequity worldwide.2 3 The excess of misinformation (and disinformation) can be overwhelming, making health-related choices challenging, even for well-educated people. Moreover, advertisements from commercial groups with vested interests in unhealthy commodities such as alcohol, tobacco and sugary drinks are persuasive and abundant. In addition, many people who could benefit from preventive or curative services may not know about them or about their entitlements to access these services.
NCDs are complex, variable, generally evolve over decades, and are linked to genetic, physiological, environmental, and behavioural risk factors.4 The diverse risk factors that perpetuate NCDs often have little or no obvious connection to people’s daily lives, and adverse health outcomes can take years to become evident. Furthermore, people often pay little attention to preventing future NCDs or to managing existing NCDs because they are dealing with daily struggles, challenging social circumstances and stresses linked to socioeconomic disadvantage. The disconnect between daily activities and future NCD development, and the impediments to doing something now for what might be a health problem in the future, can prevent people from taking action to minimise their exposure to pervasive NCD risk factors.
Although many interventions seek to provide information and strategies to prevent and control NCDs, most do not lead to sustained behaviour change,5 and they leave many people behind, especially those with health literacy challenges.6–8 Efforts to prevent and control NCDs must engender community trust9 to develop health literacy as a community asset and as a responsiveness feature of health service organisations, as well as creating innovative processes for developing the health literacy of individuals.10 Public health initiatives must be informed by and address community and individual health literacy needs, and take into account the daily social, economic, environmental and commercial determinants that, while not always obvious to people going about their daily activities, expose them to NCD risk factors. Widespread whole-of-society prevention measures based on health literacy development are central to improved global NCD health outcomes. Proliferation of health literacy development within and between communities, and within and across national policies and sectors, will be instrumental to thwarting future onslaughts of misinformation because already known, trusted and safe networks for dissemination of health information will be recognised.3 9 10 To support direct impact on the prevention and control of NCDs, the WHO calls for action on health literacy development (box 1).
Call for action: The what-to-do how-to-do call for the prevention and control of non-communicable diseases
The WHO’s report Health literacy development for the prevention and control of non-communicable diseases calls for a health literacy development approach that involves practitioners, organisations, health systems and policy makers meaningfully engaging with and supporting communities to create and sustain health enabling environments based on local needs and within social practices and resources.10
Health literacy development
Health literacy development refers to the ways in which enabling environments are created by health workers, services, organisations and cross-sector government policy makers to build the knowledge, confidence and comfort of people to access, understand, appraise, remember and use information about health and healthcare within the contexts and environments of their daily lives.10 A health literacy development approach considers the influential components of people’s daily lives (box 2) that support them to be aware of and understand the chronic nature of NCDs, the impact of NCD risk factors on their life course and the role that public policies have in minimising people’s exposure to these risks. Equipped with this awareness and understanding, people can determine if they are at risk and then make daily health-related decisions to prevent and control NCDs for themselves, their family and their community. They are also equipped to hold relevant stakeholders accountable for providing enabling environments. If countries around the world adopt a health literacy development approach, then impacts on global prevention and control of NCDs are more likely to reach a wider range of community members and reduce inequity, thus contributing to leaving fewer people behind.
Key health literacy definitions that underpin health literacy development10
Community health literacy
Community health literacy refers to health literacy-related assets (knowledge, resources and abilities) including:
The knowledge that is held by people in the community.
The extent to which knowledge is trusted, circulated and adapted freely in a community.
Health promoting customs embedded in cultural beliefs and norms, as well as in traditional or emerging practices of daily life.
The relationships that the community has with outside sources of information.
Family, peer and community conversations and interactions are central
Health literacy responsiveness
Health literacy responsiveness refers to the extent to which health workers, services, systems, organisations and policy makers (across government sectors and through cross-sectoral public policies) recognise and accommodate diverse traditions and health literacy strengths, needs and preferences to create enabling environments that optimise equitable access to and engagement with health information and services, and support for the health and well-being of individuals, families, groups and communities.
Health literacy of an individual
The health literacy of an individual, as viewed from a globally relevant perspective, is people’s knowledge, confidence and comfort—which accumulate through daily activities, social interactions, and across generations—to access, understand, appraise, remember and use information about health and healthcare, for the health and well-being of themselves and those around them.
Health literacy development
Health literacy development refers to the ways in which health workers, services, systems, organisations and policy makers (across government sectors and through cross-sectoral public policies) build the knowledge, confidence and comfort of individuals, families, groups and communities through enabling environments. Enabling environments support people to access, understand, appraise, remember and use information about health and healthcare, through verbal, written, digital and other communication channels and social resources, for the health and well-being of themselves and those around them, within the circumstances and demands of their daily lives.
Taking a globally relevant perspective of health literacy
For health literacy to have impact in global health, an understanding of how it is positioned in people’s lives, including how it develops and can be used over time is required. This perspective must be inclusive, avoiding epistemic injustice, that is, the ‘…structural exclusion of marginalised producers and recipients of knowledge’.11 Epistemic injustice in academic global health relates to public health initiatives that are not based on what a community or society knows or how they see the world.11 Health literacy development is based on, and strongly influenced by, understanding the social practices, contexts, settings, and systems in which people are born, grow, live, work and age.12–15 Therefore, health literacy development requires that we (as global health academics and practitioners) co-lead or enable locally led genuine engagement with people to understand how they view their world, what they know and to seek their interpretations of how the determinants of health in their context influence the ways in which they (as individuals, groups, communities, organisations and societies) access, understand, appraise, remember and use health information and services.
Policies and initiatives in some countries have progressed health literacy in some areas of health.10 16 17 However, theories and research about health literacy have been mainly developed in North America, Europe and Australia,16 17 which means health literacy policies and initiatives are based on Western notions of individual choice and autonomy about health and well-being and, consequently, narrow definitions of health-related reading and numeracy skills. This has resulted in individualistic approaches to health literacy, such as programmes, interventions and activities that focus on changing the knowledge and behaviour of individuals. Recognising health literacy as a social practice is important. For much of the world’s population—about 7 billion of nearly 8 billion people in the world—health behaviours and actions are integral components of the communal behaviours and actions of families, groups and communities (eg, geographical, sociocultural), with health decisions frequently guided by a range of factors including local and cultural processes, practices, beliefs and religious teachings.12–14 18 19 In these settings, individualistic approaches to health literacy development may not be relevant or effective because these approaches may be inconsistent with an individual’s worldview, do not recognise important social practices; do not recognise and respond to community strengths (eg, individual, community, regional, national health assets), challenges (eg, areas of need at individual, local and national levels) and preferences (eg, preferred ways of learning and using information and services); and can miss opportunities to design policies and environments to effectively improve health outcomes and reduce health inequities.10 Therefore, a globally relevant perspective of health literacy is needed to encompass the real-world experiences of people, embracing their relevant determinants of health, whether they live in communal, individualistic or mixed societies.
A globally relevant perspective of health literacy requires contextual factors to be integrated into health literacy development initiatives. The WHO report Health literacy development for the prevention and control of NCDs uses the Integrated Conceptual Framework for Health Literacy Development (the Integrated Framework, figure 1). The Integrated Framework provides five Action Areas in which locally relevant, fit-for-purpose, and sustainable health literacy development initiatives can be co-designed and embedded into local, regional and national policies and systems.
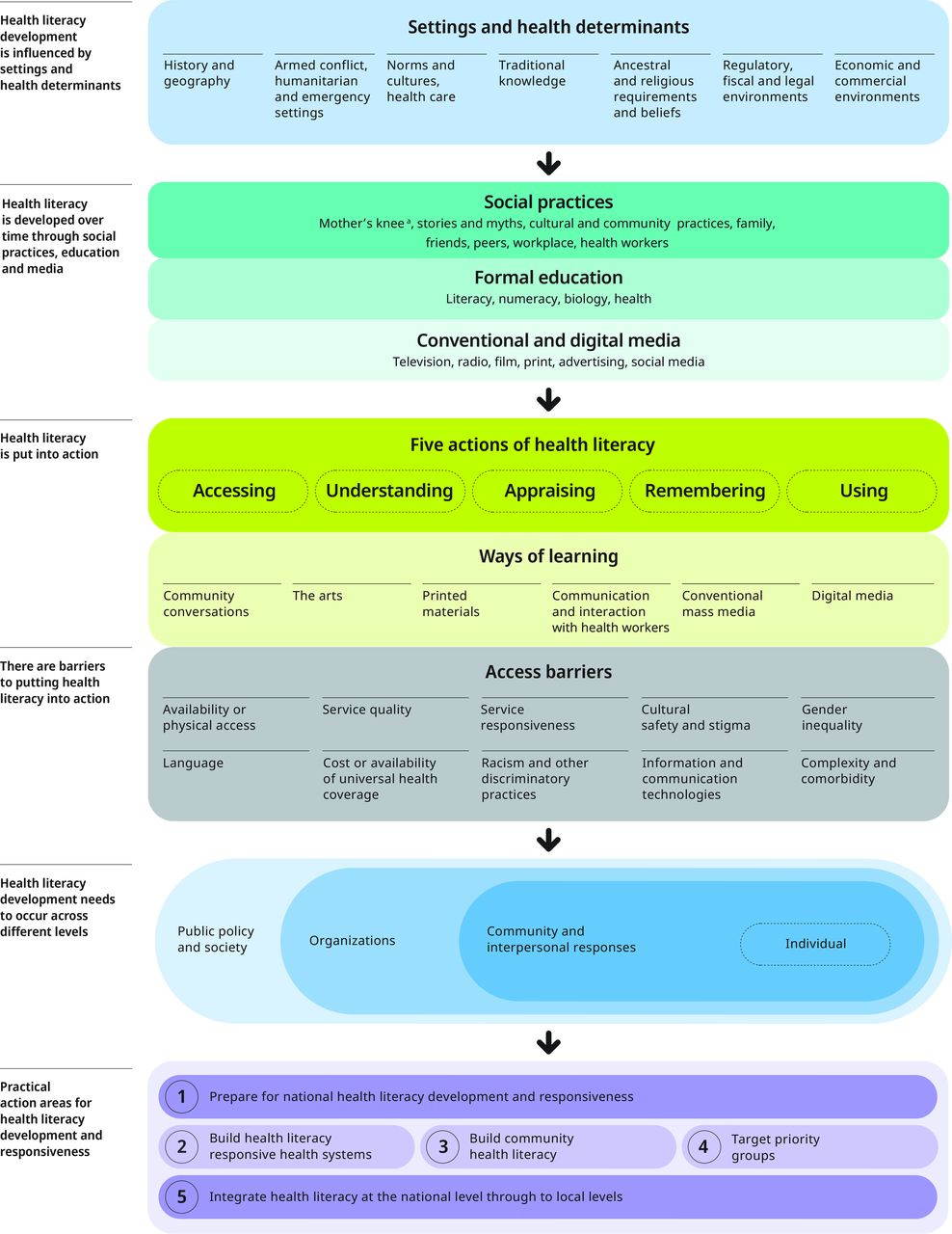
Integrated conceptual framework for health literacy development (reproduced with permission).10
At the top of the Integrated Framework sit the determinants of health and settings in which people live. Countries and regions have their own intricate networks of influence on health and health behaviours through historical, geographical, political, environmental, sociocultural, traditional, ancestral, religious, legal, economic and commercial factors.
As children grow and develop, they learn the prevailing social practices, influences, and traditions, including taboos, about health.20 People are educated (or not) through schooling systems including teachings about biology and its relation to health. People are also influenced by health information (and misinformation and disinformation) through conventional and digital media. The ways in which people learn determines their use of health information and services. The main ways of learning are through community conversations, interaction with health workers, printed materials, the arts (such as stories and creative activities), conventional mass media and digital and social media. Consequently, for many people, a centralised print media or television communication campaign will not be enough on its own and will privilege, for example, those with greater education and resources, and may disadvantage people not from the dominant culture or language groups.10
It is well established that provision of health information alone (eg, media campaigns) is insufficient for wide-spread and inclusive health literacy development because of structurally and socially embedded access barriers. These barriers include, but are not limited to, lack of or poor access to universal healthcare or physical/digital health services and usable information, and language, cultural and other socially discriminatory barriers. Access to healthcare may be impeded by poor quality of services or the inadequate responsiveness of and interactions with health services. The complexity and comorbidity of people’s health conditions can make it difficult for people to understand and manage their health and communicate with others about their health information and healthcare needs.
Health literacy development cannot be a one-size-fits all approach because contextual determinants and barriers must be addressed as part of any solution. It is essential to understand local influences on health knowledge, behaviours, barriers to accessibility and availability, and to determine how health knowledge is held, exchanged, and acted on within and between communities.10 Working with communities to identify local needs, particularly the needs of people experiencing vulnerability and disadvantage, and to co-design fit-for-purpose solutions to create health enabling environments will help manage barriers and facilitate access to health information and services. The levels at which health literacy development needs to occur, including the settings in which people learn and the settings in which learning might be stymied, are shown towards the bottom of the Integrated Framework (figure 1). Importantly, actions need to take place across public policy and society, organisations, community and interpersonal settings, as well as with individuals.
Action Areas to accelerate health literacy development
The Integrated Framework (figure 1) depicts five practical Action Areas to develop health literacy in ways that are appropriate, meaningful and useful in different community and country contexts. The five Action Areas have the potential to enhance or replace activities already underway in communities or countries, including ways to commence health literacy development work. Activities relevant to each of the Action Areas are presented in table 1.
Activities recommended for five health literacy development action areas10
Action Area 1: prepare for national NCD health literacy development and responsiveness
Public health workers and services around the world implement health and health promotion activities that may already align closely with health literacy thinking. Action Area 1 considers the activities and initiatives already in place to build on what is already working well: review current policies and programmes, assess health worker skills and capacities, and plan for future local and national actions for health literacy development. Health literacy is a complex concept and involvement of key stakeholders in the development of a contextually appropriate term for health literacy can help to stimulate interest in and sensitise people to the concept. Preparation may be best conducted through a national cross-sector health literacy coordination unit that oversees and is responsible for preparation activities.10
Action Area 2: build health literacy responsive health systems
Health literacy responsiveness is the extent to which health workers, services, systems, organisations and policy makers (across sectors and with cross-sectoral policies) recognise and accommodate diverse traditions and health literacy strengths and needs in order to create enabling environments that optimise equitable access to and engagement with health information and services.10
Being responsive includes health services and practitioners having and actively using a deep understanding of the strengths, needs, preferences and beliefs, traditions and cultures of communities, especially groups of people most at risk of or experiencing vulnerabilities. Governments and services should respond through codesign capacity building to identify which strategies will work for whom, in which circumstances and why.
Action Area 3: build community health literacy
Community health literacy is centred around family, peer and other daily community conversations. It is reliant on developing community assets related to health literacy, such as the health knowledge held by community members; the extent to which this knowledge is trusted, circulated and adapted in the community; the ways in which health promoting customs are embedded in cultural beliefs, social norms and traditional or emerging daily practices; and the kinds of relationships and interactions that community members have with outside sources of information and influence.10
Local and regional authorities need to have active dialogue with communities to understand local health literacy strengths, needs, and preferences and build on community assets by strengthening the competencies of trusted community influencers, leaders and connectors.
Action Area 4: target priority groups that are not receiving or easily accessing health information or healthcare
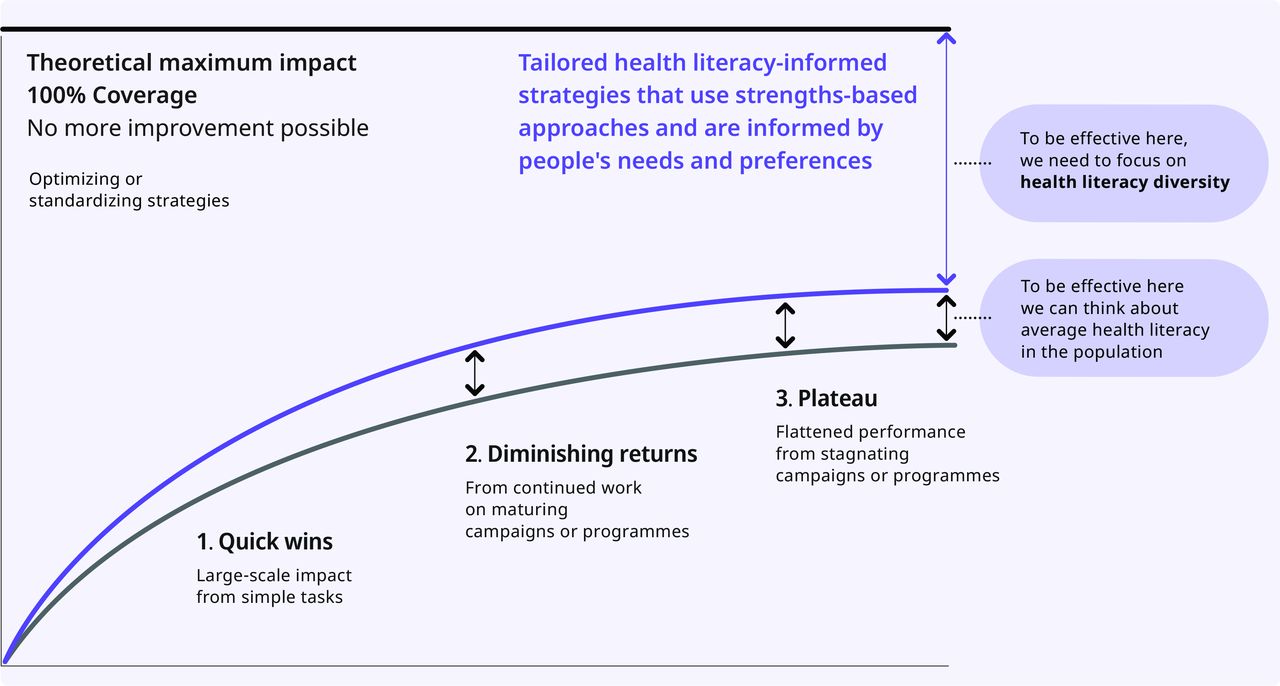
In every country, there are groups of people who are missing out on health information and healthcare. There are people who do not (but need to), cannot, or who find it difficult to access health information and care. These are people whose needs are not being met by the existing health service mechanisms. Many programmes and services designed to prevent and control NCDs are developed and implemented using a one-size-fits-all approach that is suitable for easy-to-reach populations. However, these programmes and services are often inaccessible for people with specific or complex health literacy challenges because their needs were not considered during the development stage. Assessment of and responses to the diversity of health literacy challenges can support health literacy development, reduce barriers, and improve equitable access to health information and healthcare (figure 2).10
{kind=link}
{kind=link}
Health literacy diversity explains why one-size-fits-all programmes are effective for some, but not for all people (reproduced with permission).10
Action Area 5: integrate health literacy development at national through to local levels
A national cross-sector health literacy coordination unit, recommended in Action Area 1, is best placed to conduct national integration of health literacy policy and initiatives across jurisdictions. National efforts for policy integration are stronger when co-designed among stakeholders such as governments, non-government organisations, academic institutions, civil organisations, through to local health and community setting, and people living with NCDs. Policies and programmes that are systematically and genuinely informed by people with lived experiences, as well as by organisational, research and local and national government information, are more likely to resonate with and be useful and meaningful for people who are usually left behind.9 10 Integration of health literacy development across societal structures will strengthen the reach, inclusiveness, and effectiveness of NCD prevention and control initiatives.
Conclusions
Health literacy development—based on a globally relevant perspective of health literacy—is central to the prevention and control of NCDs and to mitigating the spread of misinformation. Achieved through integrated bottom-up, codesign and top-down approaches, health literacy development is informed by and addresses the health literacy strengths, needs, determinants and preferences of people at risk of, living with, and impacted by NCDs and their risk factors and determinants.
To operationalise the integrated health literacy development approach described in this Practice paper, a series of WHO National Health Literacy Demonstration Projects are underway in several countries and regions.10 These initiatives aim to create inclusive, locally owned, locally relevant, fit-for-purpose, equity driven and potentially scalable health literacy-informed NCD prevention and control strategies to ensure no one is left behind.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Handling editor Seye Abimbola
Twitter @richardosborne4, @4MelanieHawkins, @MaristelaMont18
Contributors RHO and MH conceptualised the manuscript and wrote the first draft. GF and BM established work programs and methodology to develop content. RHO, RGN, RWB, SE, MH and CCC conceived the idea of health literacy development. All authors contributed to conceptualisation of the manuscript, revised and critically reviewed drafts. CCC and MH edited the final draft. All authors approved the final draft for submission.
Funding This study was funded in part by National Health and Medical Research Council (Principal Research Fellowship APP1155125).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.