Article Text

Abstract
The onset of the pandemic revealed the health system inequities and inadequate preparedness, especially in the African continent. Over the past months, African countries have ensured optimum pandemic response. However, there is still a need to build further resilient health systems that enhance response and transition from the acute phase of the pandemic to the recovery interpandemic/preparedness phase. Guided by the lessons learnt in the response and plausible pandemic scenarios, the WHO Regional Office for Africa has envisioned a transition framework that will optimise the response and enhance preparedness for future public health emergencies. The framework encompasses maintaining and consolidating the current response capacity but with a view to learning and reshaping them by harnessing the power of science, data and digital technologies, and research innovations. In addition, the framework reorients the health system towards primary healthcare and integrates response into routine care based on best practices/health system interventions. These elements are significant in building a resilient health system capable of addressing more effectively and more effectively future public health crises, all while maintaining an optimal level of essential public health functions. The key elements of the framework are possible with countries following three principles: equity (the protection of all vulnerable populations with no one left behind), inclusiveness (full engagement, equal participation, leadership, decision-making and ownership of all stakeholders using a multisectoral and transdisciplinary, One Health approach), and coherence (to reduce the fragmentation, competition and duplication and promote logical, consistent programmes aligned with international instruments).
- COVID-19
- Public Health
- SARS
- Prevention strategies
Data availability statement
All data relevant to this study are included in the article. Additional data can be got on request made to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
At the start of the pandemic, it was predicted that the African region would be hard hit with high morbidity and mortality; however, this scenario did not materialise.
There has been significant effort in ensuring optimum pandemic response by countries in the African region.
To adequately prepare to exit this public health emergency, countries need to strengthen their collective efforts to suppress the transmission of SARS-CoV-2, protect the vulnerable and save lives in a comprehensive, coordinated and equitable way.
Transitioning from the pandemic would require maintaining and consolidating COVID-19 response capacity through the sectoral and intersectoral coordination of response capacities and reinforcing and scaling up response capacities for COVID-19 and other major public health emergencies.
Harnessing the power of science, data and digital technologies, and research innovations would be essential to adequately guide the restoration and improvement of health service delivery and integrate lessons learnt/best practices into the formal health systems. Doing so makes it easy for countries to rebuild a resilient health system to address any future public health crises.
Investments in the response and transition are significant in the paradigm shift towards promoting health and well-being and preventing disease by addressing its root causes.
Introduction
It has been 26 months since the COVID-19 pandemic began in the WHO African Region. The first case in the region was reported in Algeria on 25 February 2020 and since this first detection the pandemic has evolved in four distinct waves, as of the writing of this paper in May 2022. The first wave was driven by wild type virus, and subsequent waves were largely driven by more transmissible variants of the SARS-CoV-2. In recent weeks, a surge of cases has been observed especially in the Southern African subregion, mainly driven by the spread of the BA.4 and BA.5 lineages of the SARS-CoV-2 Omicron variant.1 Additional contributing factors include the reduced adherence to public health and social measures (PHSM), easing of COVID-19 restriction measures by several governments, suboptimal vaccination coverage and inappropriate testing strategies, among other factors.2 Epidemiological analysis of the COVID-19 pandemic trend suggests that the current surge may propagate into a fifth wave if prompt response actions are not initiated and sustained for the greater WHO African region.3
The more transmissible Omicron variants (BA.1, BA.2, BA.3 BA.4 and BA.5) continue to drive the pandemic in the WHO African region.4 5 Since November 2021 when the variant was first detected in South Africa and Botswana, a total of 2.3 million confirmed COVID-19 cases have been reported, 27% of the 8.5 million cumulative COVID-19 cases reported in the region.6 Data as of 5 May 2022 sourced from the WHO African Regional Office (AFRO) epidemiological and laboratory surveillance team under the Emergency Preparedness and Response programme show that the Omicron variant is currently detected in 90% of countries in the WHO African region (43 out of 47).
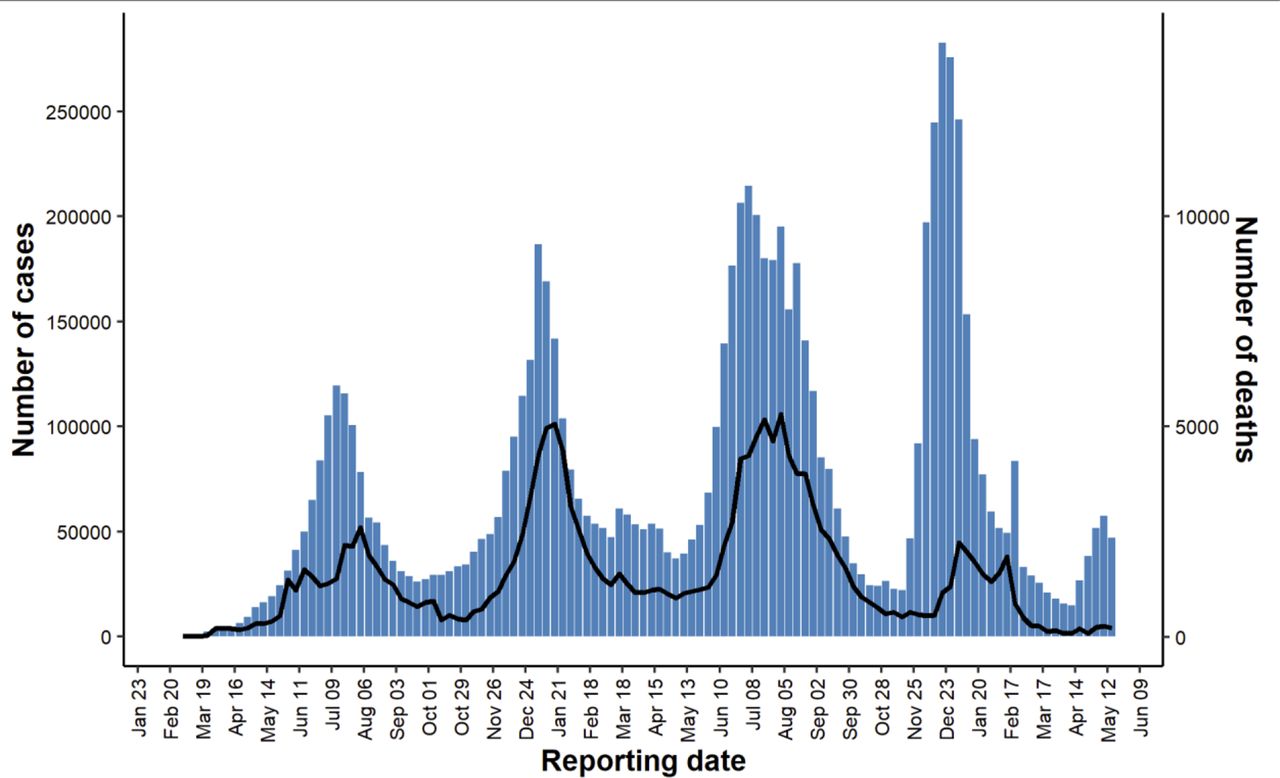
The African continent, as of 24 May 2022, has reported 11 841 926 cases and 253 774 deaths (case fatality rate 2.1%)) accounting for 2.3% and 4.0% of the global cases and deaths, respectively.7 However, these numbers may be an underestimate of the actual number of cases and deaths as it is postulated that only 14.2%—or one in seven—COVID-19 infections are being detected in Africa.8 Under-reporting has been linked to testing strategies favouring symptomatic illness with the bulk of asymptomatic and mild disease not being confirmed by testing, not unlike other countries (figure 1).

Weekly trend of COVID-19 number of cases and deaths in the WHO African Region (Data as of 24 May 2022) Data source: https://covid19.who.int/
The region has seen a consistently low vaccination coverage compared with the other continents (figure 2). Nonetheless, the population immunity is relatively high in the African Region. Recent seroprevalence estimates show 72.6% seropositivity, resulting from the combination of vaccination efforts and immunity as a result of infection demonstrating the magnitude of transmission of SARS-CoV-2 in the region.9 However, the seroprevalence estimates have significant variation in relation to geography (some subregions have higher seroprevelance than others and rural areas have lower seroprevalence); and age (children aged 0–9 years had the lowest seroprevalence).9
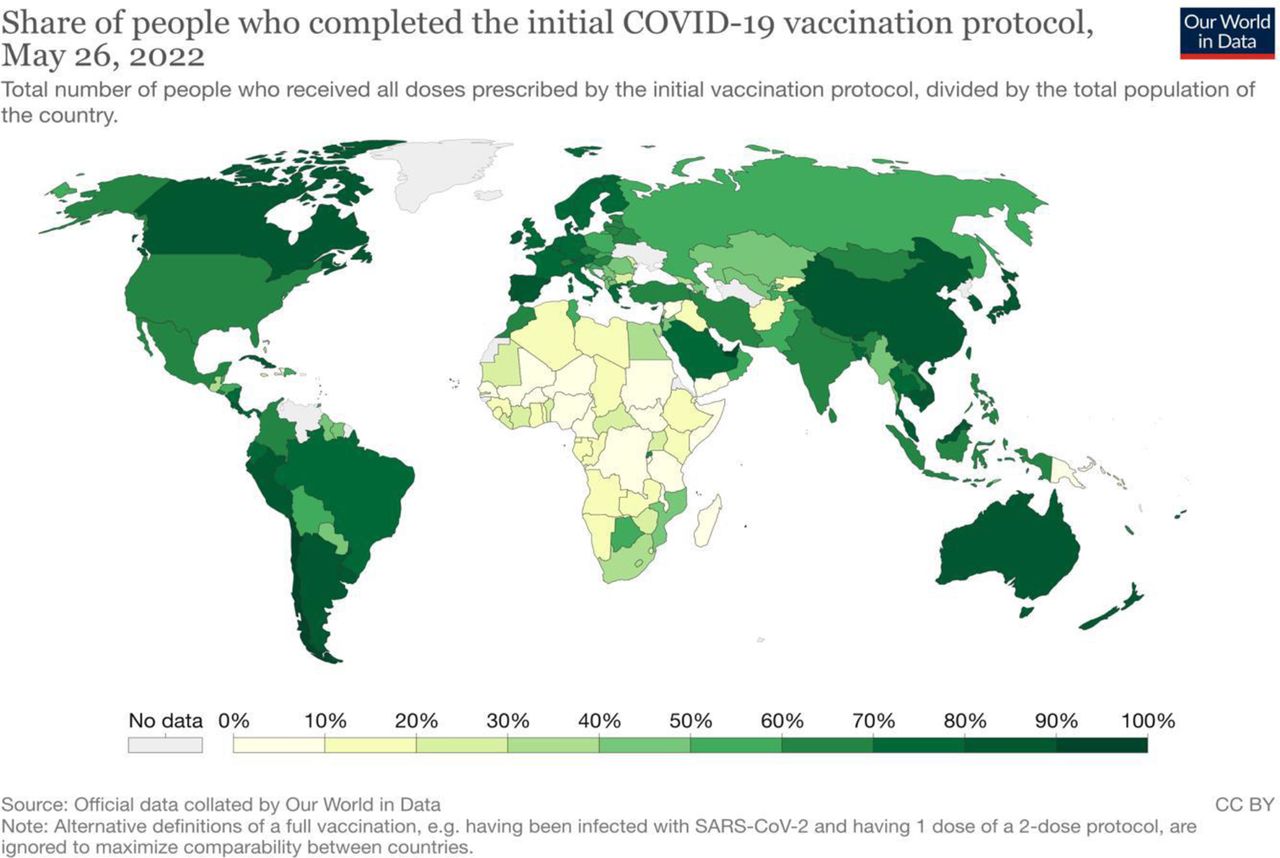
Global share of people who have completed the initial COVID-19 vaccination protocol. (The share of people who completed the initial COVID-19 vaccination protocol is defined as the total number of people who received all doses prescribed by the initial vaccination protocol, divided by the country's total population and the data from Our World in Data: https://ourworldindata.org/covid-vaccinations, accessed on 27 May, 2022.
Progress on the COVID-19 response in WHO Africa
At the start of the pandemic, it was predicted that the African region would be hard hit with high morbidity and mortality; however, this scenario did not materialise. Several factors may have contributed to the low burden of disease in the continent including demographic characteristics (a young population in the majority of countries), the difference in detection and identification capacities for cases and deaths,10–15 the possible contribution of pre-existing immunity to other coronavirus infections16 and weak surveillance systems.17 18 In addition, early institution of restriction measures with better compliance to lockdown measures in the early stages of the pandemic by many countries and rapid repurposing of outbreak response systems to manage the pandemic that may have played a role.2 In addition, the experiences of Member States and partners in the Africa region in managing the many outbreaks and public health emergencies contributed to the level of readiness and rapid responses to the current pandemic.19
The onset of the pandemic revealed the health system inequities and inadequate preparedness in the countries, especially in the African continent.20 21 Significant gaps were revealed, such as continued dependence on external production of vaccines and personal protective equipment (PPEs), insufficient intensive care unit beds, and the absence of medical oxygen and other materials essential to the treatment of the virus. Nonetheless, there has been significant effort in ensuring optimum pandemic response guided by the orientation outlined in the WHO Africa strategic document.22 For instance, at the onset of the pandemic, the supply chain issues related to supplying commodities, cargo space, and manufacturing posed a challenge to countries in the region. Subsequently, there was an activation of the Pandemic Supply Chain Network and the establishment of a coordination mechanism for global distribution, which enabled the reduction of the gap in distribution, especially in priority countries and areas where it is most needed.23 The United Nations (UN) Supply Portal (CSP) was launched on 28 April 2020 to address the procurement of standard items such as PPE, diagnostics, and biomedical and medical products through a global structured and centralised mechanism.24 The system has helped to revamp the capacity of the WHO and countries’ procurement in terms of supply chain mechanisms, assess locally manufactured medical supplies, and evaluate local manufacturing companies. Overall, the CSP has facilitated the procurement and shipment of 106.4 million pieces of PPE, 105.7 million laboratory test kits, 1687 patient monitors, 6671 oxygen concentrators and 416 ventilators in the WHO African Region as of the writing of this paper.
The deficiency in the clinical case management (CM) capacities, in terms of unskilled staff, oxygen deficiency, therapeutics and treatments and medical equipment, was observed in the region at the onset of the pandemic.25 To address the challenges, WHO, with the help of partners, has worked on the establishment of a regional stockpile of oxygen concentrators (800), oxygen cylinders (3800) and pulse oximeters (595) that are ready to be shipped to countries for urgent need. Regionally, more than 60 000 healthcare workers (HCWs) have been trained to manage critical and severe patients and the indications of rational oxygen use and other therapeutics and monitoring home-based and isolation care (HBIC). Countries in the WHO African region have been supported to access the therapeutics platform and procure the recommended therapeutics for COVID-19 treatment. As of May 2022, 34% of countries in the region are using these drugs to treat patients. In addition, many countries are moving and decentralising their treatment capacities by using the national emergency national teams (EMTs). Following the awareness and operationalisation of EMTs in January 2018 and its subsequent acceleration by the COVID-19, 34% (17 out of 47) of the WHO African countries (Algeria, Cameroon, DRC, Zambia, Burkina-Faso, Chad, Congo (Republic of), Eswatini, Ethiopia, Ghana, Madagascar, Nigeria, Sao Tome and Principle, South Africa, South Sudan, Zimbabwe, Senegal) received support in the management of severe and critical cases of COVID-19 at the different peaks of the response. In addition, there has been a platform for countries to share experiences on safe and sustainable clinical and HBIC, triage and referrals to tertiary hospitals through supportive supervision and bolster capacities in countries needing extra support and oxygen treatment (such as biomedical equipment).
In addition, given the increased oxygen demand26 (with an estimated 1.3 million COVID-19 patients needing oxygen) since the pandemic began,27 oxygen plants in the continent have increased from 68 to 115 and oxygen concentrators from 2600 to 6671 courtesy of partners and WHO through the UN platform (including 1517 shipments from WHO AFRO stockpile). The WHO AFRO have supplied and distributed 1517 oxygen concentrators to 22 countries in the last 2 months and 10 874 cylinders to 8 countries. Overall, 15 countries have been supported in the manufacturing, and delivery and maintainance of oxygen plants, and where plants have been set up, the oxygen costs have reduced by 40%. A series of capacity-building activities have initiated to improve the management of oxygen systems. For instance, 130 biomedical engineers and logisticians across the continent have been trained (1) to calculate oxygen requirements for different scenarios, (2) to map oxygen resources before an influx of cases occurs and hospitals are overwhelmed, and (3) to work on the maintenance of the various oxygen devices.
The onset of the COVID-19 pandemic placed the clinical laboratory and testing for SARS-CoV-2 at the front and centre of the response challenges in the region. As such, there has been the bolstering of the early detection of upsurges of cases through the widespread use of antigen rapid diagnostic tests (Ag-RDT) in all countries, coupled with increased ‘test and trace’ and SARS-CoV-2 PCR testing capacities.28 In addition, the COVID-19 sequencing laboratory network launched in September 2020 contributed to improving genomic surveillance in the WHO African region. Today, the region has seen a six-time increase in the number of sequences performed in 2022 compared with the last year.28 Equally, there has been an enhancement of community-based surveillance using Ag-RDT to scale up these cost-effective, easy-to-use diagnostics, which seeks to help to augment COVID-19 case detection and management in communities. The community-based surveillance initiative aims to reach more than 7 million people with Ag-RDT in the year and increase testing capacity in participating countries by 40%.
Correspondingly, WHO and countries are scaling-up research activities, notably through some serosurveillance and operational research studies, to better understand the dynamics of the COVID-19 pandemic and post-COVID-19 syndrome within the African region and generate evidence to inform operational planning and understand vaccine effectiveness.9 Equally, vaccination was added to the COVID-19 response package to rapidly increase the immunity of the population. However, its roll-out has been slower in most African countries than in other parts of the world. For instance, as of the writing of this paper, the WHO African Region had received 610 million doses of vaccines since the first shipment in late February 2021 and as of 22 May 2022, a total of 167 million persons (14.6% of the population) were fully vaccinated.29 Only seven countries (São Tomé and Príncipe, Mozambique, Tunisia, Cape Verde, Morocco, Botswana and Rwanda) had attained 40% coverage while two (Mauritius and Seychelles) had attained 70% coverage.29
Infection prevention and control (IPC) components have been enhanced through capacity building and the development of guidelines on IPC interventions in the context of COVID-19 resurgence targeting all 47 countries aiming to reduce incidences of COVID-19-associated infections in patients, HCWs and the population.30 Risk communication and community engagement (RCCE) activities have also been enhanced through social mobilisation and sensitisation to promote compliance with PHSM and vaccine uptake through partnership and capacity building to at least 13 Civil Society Organisations (CSOs) in at least 15 countries.28 In addition, strategic partnerships with social media companies and mobile network providers have been established to disseminate key health messages. In addition, strategic partnership with social media companies and mobile network providers have been established to disseminate key health messages. For instance, a partnership with Facebook and MTN reached at least 15 million Facebook users and 10 million mobile subscribers in 2022.28 These partners engaged with local community structures such as women’s and youth groups, traditional, political and religious leaders, influencers and other trusted people at the community level. In addition, the capacity building of over 6000 HCWs on enahcing RCCE initiatives has been achieved in the WHO African region.28 A Community-Based Response Initiative project in hotspot district areas in 17 African countries was initiated and has improved active case finding. Once cases have been identified, additional interventions/support is triggered, such as testing, genomic sequencing, home-based isolation and care, provision of community IPC kits, assessment of hotspot communities for compliance to public health and safety measures, vaccination and RCCE.
Overall, WHO AFRO worked with new operational partners (such as non-governmental organisations, private institutions, donors, CSOs and non-state actors) the in the different countries in the region to enhance the preparedness, readiness and response to the COVID-19 burden. The partnerships supported public health emergency governance with more inclusive and holistic cooperation and coordination with various actors for high-impact activities to benefit vulnerable communities. The engagement with other UN agencies has enhanced diverse aspects of the response. For instance, the expertise of UNICEF has helped advance vaccination, the World Food Programme has been key in the logistic shipment in humanitarian settings and hard-to-reach areas, and International Organisation for Migration has been a key response partner among vulnerable migrants population and improved cross-border response capacity. In addition, the WHO AFRO initiated innovative pilot projects with CSOs in response to COVID-19 in the region. In the past 26 months, 23 CSOs from 13 countries (Algeria, Burkina-Faso, Cameroon, Congo, Cote d'Ivoire, DRC, Ethiopia, Gabon, Kenya, Mali, Nigeria, Senegal and Zimbabwe) benefited from projects technical and financial support and have reached more than 4 million direct beneficiaries in countries.28
The position: proposed framework on transitioning to resilient health systems to respond better to public health emergencies
Guided by the WHO’s COVID-19 Strategic Preparedness and Response Plan (SPRP) for 2022,31 which has laid out the strategic actions, there is a need to prepare to exit this public health emergency. This requires that Member States strengthen their collective efforts to suppress the transmission of SARS-CoV-2, protect the vulnerable and save lives in a comprehensive, coordinated and equitable way, and guided by the SPRP. With many uncertainties around the ongoing circulation of different variants of SARS-CoV-2 and the potential threat of increased virulence the following scenarios should be considered:
The response scenarios
Base case: The virus continues to evolve. However, severity is significantly reduced over time due to sustained and sufficient immunity against severe disease and death. A further decoupling between cases and severe disease incidence leads to progressively less severe outbreaks. Periodic spikes in transmission may occur as a result of an increasing proportion of susceptible individuals over time if waning immunity is significant, which may require periodic boosting at least for high-priority populations; a seasonal pattern of peaks in transmission in temperate zones may emerge.
Best case: Future variants that emerge are significantly less severe, and protection against severe disease is maintained without the need for periodic boosting or significant alterations to current vaccines.
Worst case: A more virulent and highly transmissible variant or sub lineage emerges against which vaccines are less effective, and/or immunity against severe disease and death wanes rapidly, especially in the most vulnerable groups. This would require significant alterations to current vaccines and full redeployment and/or broader boosting of all high-priority groups.
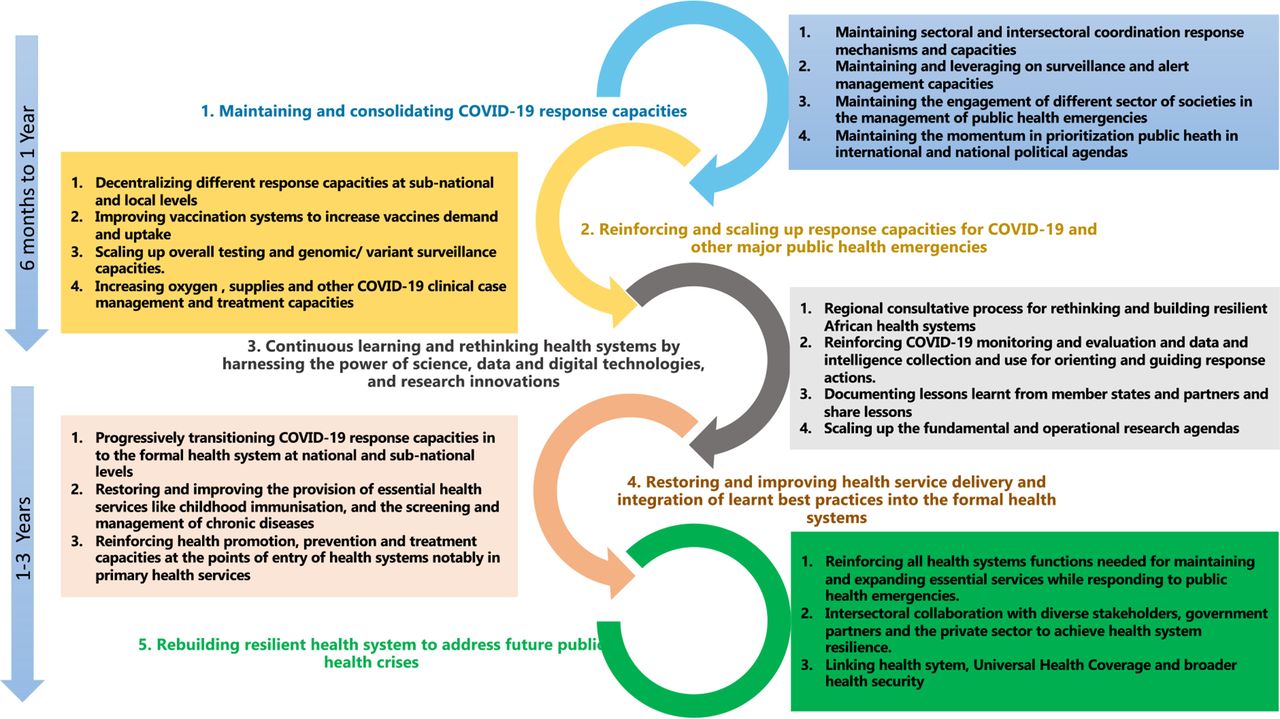
Guided by the WHO’s COVID-1931 31 and the priorities outlined at the 150th session of the executive board,32 and the Future of WHO COVID-19 Response Operations in Africa in 2022,22 postulating and positioning the future of the response envisions five components that need to be incrementally build on each other as illustrated in figure 3. The activities are proposed to ensure resilience of capacities and systems built to respond to COVID-19 as the transition is made from the acute phase of the pandemic to a recovery then interpandemic/preparedness phase.

{kind=link}
{kind=link}
{kind=link}
The proposed framework on transitioning towards resilient health systems to respond better to public health emergencies.
In component 1, we propose the need for maintaining and consolidating COVID-19 response capacity. This includes continuing with the sectoral and intersectoral coordination of response capacities and continuing surveillance and alert management. Everyone in society—governments, communities and individuals—has a part to play in maintaining the appropriate strategies and capacities and managing the current cases to reach a steady state of low level or no SARS CoV-2 transmission. Therefore, it includes maintaining the ongoing engagement of different sectors of societies in managing public health emergencies. We suggest that the appropriate surveilance strategies applied at the national and subnational levels must be flexible to adapt to changes in the viral landscape as the virus evolves in an unpredictable manner. This includes ensuring that all people, especially the vulnerable (such as migrants, refugees, displaced populations, and residents of high density and informal settlements, who are at particularly high risk from the interruption of already limited health and social services, are well protected), are protected against infection through full vaccination, continued use of IPC measures, observance of PHSM, and early detection of infection and access to high quality care.
In component 2, we propose, reinforcing and scalling up response capacities for COVID-19 and other major public health emergencies. The aim is to support countries to continue making increased investments for COVID-19 response, which is significant in the paradigm shift towards promoting health and well-being and preventing disease by addressing its root causes. In this component we propose the decentralisation of the different response capacities to the subnational and local levels For instance, we envisage that decentralisation will increase access to and uptake of vaccination and promotes complete vaccination of individuals while addressing causes of vaccine hesitancy among the public through the promotion of health literacy and community engagement, advocacy and ownership for COVID-19 vaccination. Further, the proposal includes reinforcing COVID-19 surveillance capacities (hospital surveillance for new cases and essential services implications) and scaling up COVID-19 testing and genomic/variant surveillance capacities. Continued improvement of the health workers' ability to identify and diagnose COVID-19 symptoms—not just for surveillance but also for isolating and providing care while protecting themselves and other users of health services, is essential. In addition, we envisage increasing oxygen and other COVID-19 CM and treatment capacities besides augmenting the medical and non-medical supplies and other material and equipment for addressing timely operational needs required by Member States. The critical care capacities, including indications and use of oxygen and monitoring critically ill patients built up for COVID-19, have, in many cases, accelerated improvements in long-neglected systems, especially in public care facilities, needs to be continued. In this component, we envisage that there is a risk of reintroduction and resurgence of the disease, and that it will continue; thus, there will be a need to sustainably control it through the rigorous application of public health interventions as the virus circulates between and within countries. In addition, there is a need to review and scale-up interventions to address low risk perception, misinformation, disinformation and politicisation of the pandemic that undermine positive behavioural adaptation and effectiveness of proven PHSM, therapeutics and vaccines. To continually break the transmission chain, this component involves the consistent use of proven PHSM as guided by context-appropriate socio-behavioural data.
Component 3 provides an important window of opportunity to continue to use research to inform future public health actions.33 In this component, there is a need for continuous learning and rethinking health systems by harnessing the power of science, data and digital technologies and research innovations as critical enablers of the aforementioned other priorities.32 This component focuses on documenting lessons learnt and adjusting capacities based on ongoing pandemic dynamics and predictive modelling. In addition, the action includes reinforcing and scaling-up fundamental and operational research to guide response actions that address both the known and unknown drivers of transmission and impact, guided by data, science and interventions that have been proven to work. As part of data management, there is the element of reinforcing COVID-19 monitoring and evaluation and data and intelligence collection and use for orienting and guiding response actions. In addition, it presents an opportunity to learn lessons from Member States and partners on what works and does not work to strengthen health systems and health security. Countries could share and promote innovative best practices, which can lead to significant changes in the health system’s capacity to respond and recover from health emergencies while maintaining essential health services.
As part of transitioning the response to pre-pandemic preparedness and in concert ensuring strengthened routine health systemsare in place in component 4, we envision restoring and improving health service delivery and integration of lessons learnt/best practices into the formal health systems. This will mean progressively transitioning COVID-19 response capacities into the formal health system at national and sub-national levels and restoring, expanding and sustaining access to essential health services, health promotion and disease prevention. In addition, it will include implementing an integrated approach to respiratory disease surveillance by continuing the integration of COVID-19 surveillance into senitnel surveillance for Influenza like illness and Severe Acute Respiratory Infection under the umbrella of the Integrated Disease and Response system with the national public health institutions playing a significant role. There is also a need to support countries to build capacities to use and or adjust pandemic response interventions based on available and accrued public health intelligence with the view to promoting health-seeking behaviour to ensure early diagnosis and entry into clinical care. We postulate ensuring that we maintain COVID-19 testing and genomic/variant surveillance capacities (although not typically associated with health service delivery but surveillance), and strengthen laboratory systems, for example, for sample transportation, sample storage, laboratory information, quality assurance and biosafety practices. COVID-19 CM investments have provided a platform to address critical gaps in healthcare, specifically with respect to oxygen production and delivery infrastructure and delivery of therapeutics. COVID-19 has also provided the impetus to strenghen, maintain and reinforce critical human resource capacities in Member States to address and respond to upsurge of COVID-19 cases. It is imperative, besides working on tackling the pandemic’s long-term impacts, including post-COVID-19 conditions (long COVID-19),to strengthen essential health services like childhood immunisation and the screening and management of chronic diseases like diabetes, hypertension, cancer, etc). There is a need to accelerate the development and integration of mental health and psychosocial services to reach those most affected for example, young people, women and those with chronic conditions. Investments in COVID-19 vaccination have improved vaccine delivery systems such as cold chain capacity however improvements need to be coupled with strengthened outreach activities so the most hard to reach children can be included with routine immunisation. Chronic care clinics for non-communicable diseases (NCDs) also need to be strengthened so that they reach vulnerable and at riskpopulations. For example, HIV infection and tuberculosis can be used to reach non-traditional target groups such as adults; and maternal and child health clinics to reach pregnant and non-pregnant women as well as male caregivers of young children. The COVID-19 pandemic has uncovered gaps in the linkages between NCDs and mental health areas which also need adequate attention. The gains made in areas of IPC, such as hand hygiene practices and waste management must be reinforced and sustained as they have benefits well beyond COVID-19. Strenghening of routine health services could address the direct mortality attributable to COVID-19, the indirect mortality caused by the overwhelming of health systems, the interruption of other essential health and social services, and the acute and long-term detrimental effects on health and well-being of the socioeconomic consequences of certain response measures.
Finally, in component 5, there is a call to action for rebuilding a resilient health system to address better any future public health crises. Resilient systems would be able to address more effectively future public health crises while maintaining an optimal level of essential public health functions and continuity of quality healthcare services. This includes launching a regional consultative process for rethinking and building resilient African health systems that can support all public health functions needed for maintaining and expanding quality essential services and reducing out of pocket expenditure while also responding to public health emergencies. It entails intersectoral collaboration with diverse stakeholders including, government, partners and the private sector to achieve health system resilience. It includes defining the major actions needed over the next 3 years to rebuild health systems for resilience based on lessons learnt from all countries and drafting a health system resilience strategy. By doing all these, we need to reinforce and diversify the collaboration and coordination with existing and new partners (academia, regional economic and political entities, CSOs, private sector organisations).
Conclusion
Considering the uncertainties surrounding the ongoing COVID-19 pandemic and the weaknesses in detection and management of cases and the complex nature of human behaviour, all Member States are urged to develop adaptable plans to address any upsurges of COVID-19 in humans. Therefore, much work is still needed to implement comprehensive surveillance and vaccination programmes to prevent the emergence and spread of SARS-CoV-2 and control further cases in our populations and in particualr among high-risk and vulnerable populations. Overall, the proposed elements will align the response in the region and ensure resilience of capacities and systems are built to continue to respond to COVID-19 and even future public health emergencies. The proposed transition framework is made from the acute phase of the pandemic to a recovery then interpandemic/preparedness phase. As countries considers the proposals, they are encouraged to consider the following three key principles to bolster the core capacities for Health Emergency Preparedness, Response and Resilience.34 35 These key principles: equity, inclusiveness and coherence should guide the actions. Equity ensures the the protection of all vulnerable populations with no one left behind. Inclusiveness to support full engagement, equal participation, leadership, decision-making and ownership of all Member States, communities and stakeholders using a multisectoral and transdisciplinary, One Health approach. And Coherence to enhance the reduction of fragmentation, competition, and duplication and promote logical, consistent programmes aligned with all existing international instruments such as the International Health Regulations 2005, and other global and regional frameworks, ensuring collaboration, coordination and synergy between institutions for the creation of robust and resilient health system.
Data availability statement
All data relevant to this study are included in the article. Additional data can be got on request made to the corresponding author.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge all COVID-19 Pillar lead and the pillar teams that participared in the WHO African regional office COVID-19 pillar leads meetings and made comments and corrections to the paper.
References
Footnotes
Handling editor Seye Abimbola
Twitter @AnokoJulienne, @kinzyomalley
Collaborators Not Applicable.
Contributors TB and BO conceptualised the study; BO drafted the initial manuscript, which was subsequently revised for important intellectual content by all authors. All authors participared in the WHO African regional office COVID-19 pillar leads meetings for which the paper discussed. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.