Article Text

Abstract
Background Long-lasting insecticidal nets (LLINs) are one of the key interventions in the global fight against malaria. Since 2014, mass distribution campaigns of LLINs aim for universal access by all citizens of Burundi. In this context, we assess the impact of LLINs mass distribution campaigns on malaria incidence, focusing on the endemic highland health districts. We also explored the possible correlation between observed trends in malaria incidence with any variations in climate conditions.
Methods Malaria cases for 2011—2019 were obtained from the National Health Information System. We developed a generalised additive model based on a time series of routinely collected data with malaria incidence as the response variable and timing of LLIN distribution as an explanatory variable to investigate the duration and magnitude of the LLIN effect on malaria incidence. We added a seasonal and continuous-time component as further explanatory variables, and health district as a random effect to account for random natural variation in malaria cases between districts.
Results Malaria transmission in Burundian highlands was clearly seasonal and increased non-linearly over the study period. Further, a fast and steep decline of malaria incidence was noted during the first year after mass LLIN distribution (p<0.0001). In years 2 and 3 after distribution, malaria cases started to rise again to levels higher than before the control intervention.
Conclusion This study highlights that LLINs did reduce the incidence in the first year after a mass distribution campaign, but in the context of Burundi, LLINs lost their impact after only 1 year.
- Control strategies
- Epidemiology
- Malaria
- Descriptive study
Data availability statement
Data are available on reasonable request. The analysis presented in this study is based on the malaria incidence between 2011 and 2019 using routinely collected surveillance data obtained from the National Health Information System. Data are aggregated at health district level. No information is available on severity nor gender.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Long-lasting insecticidal nets (LLINs) proved to be crucial in the global fight against malaria largely contributing to the worldwide decline in malaria prevalence between 2000 and 2015.
Several critical challenges relate to the success of this intervention but primarily the LLINs need to be available and properly used all the time. The serviceable lifespan of LLINs can vary widely among different households, net types and settings.
WHAT THIS STUDY ADDS
This study highlights that LLINs reduced malaria incidence in the first year after a mass distribution campaign in the context of Burundi, but the duration of functional effectiveness seemed to be much shorter than 3 years that LLINs should be biologically effective.
LLIN has the potential of being an effective vector control intervention in Burundi if the reasons for the fast loss of the impact are understood and can be tackled.
Over the period 2011—2019, we observed a non-linear increase in malaria incidence coinciding with an overall mean night temperature towards 16°C, which is the known threshold above which Plasmodium falciparum development in the mosquito can happen.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The study points to the need for continuous investment in improving the effective lifespan of LLINs or to adapt distribution campaigns to make ‘serviceable LLINs’ continuously available in the community.
Sustaining vector control is needed to keep transmission suppressed.
The study highlights the value of routinely collected data to monitor malaria to improve resource allocation and malaria control efforts.
Introduction
The distribution and use of long-lasting insecticidal nets (LLINs) are crucial in the global fight against malaria. Increased coverage of LLINs in Africa was an important driver of the decline in malaria prevalence between 2000 and 2015, accounting for an estimated 68% reduction of the more than 600 million clinical cases averted since 2000.1 2 However, several critical challenges relate to the success of this intervention. LLINs’ effectiveness largely depends on the behaviour of the vector species involved, with the highest impact on vectors that are feeding predominantly indoors on humans during the night.3 Further, LLINs need to be available and properly used to be effective. Several factors affect the use of LLINs such as discomfort, mosquito biting nuisance, perception of risk and social factors.4–6 WHO recommends free mass distribution of LLINs supplemented with delivery mechanisms through, for example, antenatal care clinics (ANC) and the Expanded Programme on Immunisation (EPI) to maintain coverage and access in the postdistribution phase needed because of new births, migration, and loss and damage to the nets.7 The effective lifespan of LLINs can vary widely among different households, net types and settings,8 which makes it difficult for National Malaria Control Programmes and other agencies to plan the frequency for mass distribution campaigns. WHO guidelines recommend replacement of LLINs every 3 years, unless empirical evidence suggests otherwise or the epidemiological situation has changed, for example, during humanitarian crises.9
In Burundi, malaria is the leading cause of health facility attendance and under-5 mortality, and the country has a history of devastating malaria epidemics in the highland areas.10 11 Since 2004, the Burundian National Malaria Control Programme (PNILP) has assumed an integrated malaria control strategy. This strategy is based on increased epidemiological surveillance, epidemiological stratification, improved case management with artemisinin-based combination therapy, strengthening health facilities, mass (3 yearly) and continuous distribution of LLINs through ANC the EPI channels, and targeted indoor residual spraying (IRS) in areas most at risk.12 The distribution of LLINs started in 2003 based on social marketing campaigns, and in 2005, it was then integrated into ANC and health facility-based vaccination services for children. Mass distribution started in 2009, focusing on children under 5 and pregnant women.12 Since 2014, mass distribution campaigns of LLINs have aimed at universal access for all citizens of Burundi.12
The efficacy of LLINs has been well studied and the evidence of their impact, when used under controlled conditions of a trial setting, has been documented in a number of systematic literature reviews.13 14 Effectiveness of LLINs has been evaluated in a variety of settings.15 16 Effectiveness assesses the performance of the intervention under real-life operational conditions. Hence, the results vary depending on the actual operational, epidemiological and socioeconomic context including human behaviour and maintenance of the LLINs.15 17 In Burundi, the effectiveness of LLINs has not been evaluated. This evaluation is needed to make informed decisions on malaria control and to guide planning and readjustments of the control strategy. This is of particular importance for Burundi as the provision and timely replacement of LLINs is considered a major intervention for the national malaria control programme. Routinely collected surveillance information, when available, can be used for such an impact evaluation.18 19
Therefore, we aimed to assess the impact of LLINs mass distribution campaigns on malaria incidence between 2011 and 2019 using routinely collected data obtained from the National Health Information System (NHIS). We focused on the health districts with the highest malaria burden where vector control is most needed. In order to put our findings in the current epidemiological context of Burundi, we also explored the correlation between the observed trends in malaria incidence with any variations in climate conditions. Malaria on African highlands is highly seasonal and related to climatic factors. Hence, changes of the climatic condition are expected to alter the malaria epidemiological situation.11
Methods
Study country
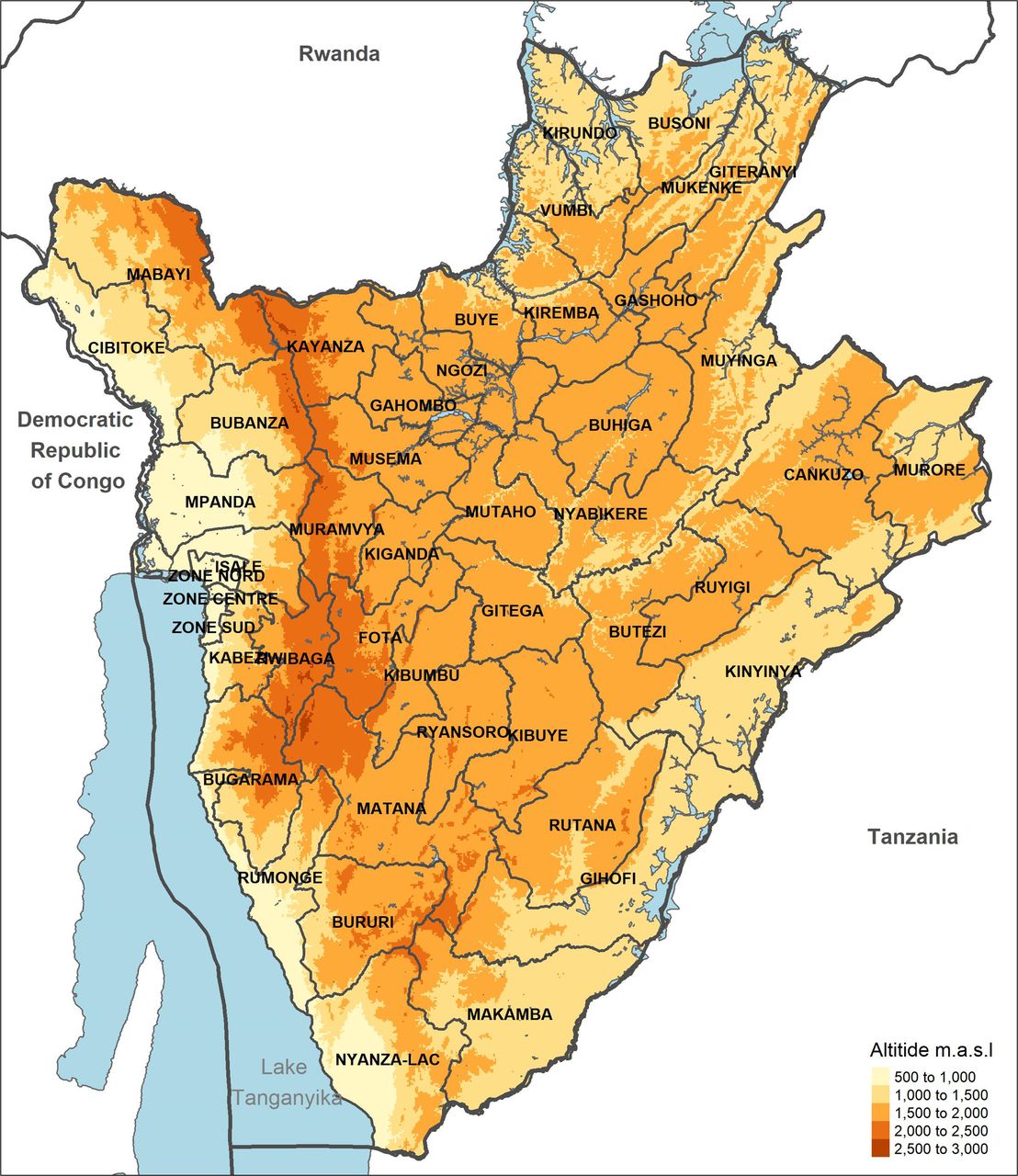
Burundi is a landlocked country in East Africa neighbouring the Democratic Republic of Congo, Rwanda and Tanzania. The country has about 11 million inhabitants, with a population density of around 315 people/km2. Burundi is a mountainous-hilly area with a median altitude of 1570 m (figure 1). It has a tropical highland climate with high variations in temperature and precipitation. Overall, the main dry season from June to August is followed by the short wet season from September to December, a short dry season from December to January and a long wet season from February to May. Anopheles gambiae and Anopheles funestus are the main malaria vector species which are primarily endophagic, endophilic and bite during the night.20 21 Most cases (90%) of malaria are due to Plasmodium falciparum.12 21 22

Topography of Burundi and indication of the health districts.
Up to 2017, Burundi had 46 health districts (figure 1). In 2017, the health district of Mabayi, Cibitoke Province, was split into two, but this split was not considered in the subsequent analyses. Each health district has a district hospital and on average 39 health centres that provide basic healthcare. Community health workers extend access to diagnosis and treatment of malaria, pneumonia and diarrhoea up to village level.21 23
Between January 2011 and December 2019, the government implemented three mass distribution campaigns of LLINs, aiming to provide one bed net per two people in line with WHO standards. The first distribution took place in June 2014 and the second one in September 2017 with, in both years, a distribution of a mix of permethrin (Olyset Net), alphacypermethrin (Royal Sentry) and deltamethrin containing LLINs (Netprotect and Permanet).12 The mass distribution of 2014 reached an overall coverage, that is, percentage of households that received an LLIN, of more than 98% and 2 weeks after the mass distribution 89% of the interviewed persons declared to have slept under an LLIN the night before the interview.24 In 2017, the coverage was 96.8% and almost 93% declared to have slept under an LLIN the night before the interview (2 weeks after the mass distribution).25
The third mass distribution campaign started end of 2019 and included pyrethroid-PBO LLIN in four health districts and Deltamethrin-based LLINs (Yorkool) in all other health districts. The 2019 mass distribution was not included in the analysis, as the available malaria incidence data covered the period January 2011 until December 2019.
Data
Malaria case data
Malaria cases for the period 2011—2019 were obtained from the NHIS. Before 2014, malaria data were sent as paper-based reports to the health district, where data digitalisation was performed. Since 2014, all the country’s health facilities record the data digitally using the District Health Information Software (DHIS2). The NHIS Office evaluates the completeness, timeliness and quality of the data. In 2018, the overall completeness of health facility reports was 92%.12 A moving average (mean of the previous and next data point) was used for the rare occasions for which we missed weekly malaria incidence data.
Malaria is suspected for any fever with an axillary temperature greater than or equal to 37.5°C or a history of fever within 24 hours with one or more of the following signs: headache, asthenia, chills, anorexia, aches and pains, and arthralgia.26 Confirmation before treatment is mandatory for all suspected malaria cases throughout the country and is based on Rapid Diagnostic Test (RDT) (Malaria Antigen HRP2 Card test) or thick smears.
The confirmed malaria cases were converted into incidence rates per 1000 population. Population data for the period 2011—2019 were derived from WorldPop, which provides open access spatial demographic datasets.27 The pixel values summed for each health district were used to calculate malaria incidence rates.
Altitude, climatic and land use data
The median altitude of each health district was calculated from the ASTER Global digital elevation model.28 The mean rainfall, and mean day and night land surface temperature were extracted per month over the period 2011—2019 from ERA529 and mod11a2,30 respectively. We calculated the annual percentages per health district (period 2011–2019) of the following land use categories: (1) LC10: cropland, rainfed agriculture; (2) LC20: cropland, irrigated or postflooding; (3) LC30: mosaic cropland (>50%)/natural vegetation (tree, shrub, herbaceous cover) (<50%) and (4) LC40: mosaic natural vegetation (tree, shrub, herbaceous cover) (>50%)/cropland (<50%). Data on land use were derived from Globcover.31
Information on LLIN mass distribution time periods was received from the PNILP.
Data analysis
Malaria incidence in function of altitude
The impact of elevation on malaria incidence was explored using a generalised additive mixed model (GAMM)32 with malaria incidence (weekly cases per 1000 population) as the response variable.
Effect of LLIN on malaria incidence in highland health districts
To evaluate the effect of the LLINs on malaria, we included the districts with substantial malaria endemicity based on the correlation analysis of altitude with malaria incidence. To investigate the duration and magnitude of the LLIN effect on malaria incidence, we developed a GAMM (E, Equation) with malaria incidence as response variable (h(malaria incidence)) and timing of LLIN distribution as explanatory variable (f1(Time since LLIN distribution)). We also added a seasonal (f2(Seasonal time)) and continuous time (f3(continuous time)) component as explanatory variables.32 33 We used a health district component as a random effect (b0(Health district)) to account for systematic and random natural variation in malaria cases over time and between districts. GAMMs were used because we expected non-linear responses for the LLIN and time effects. The model formulation was as follows:

‘Time since LLIN distribution’ was the primary variable of interest. It represents the number of weeks since LLINs were most recently distributed in mass distribution campaigns. For simplicity, the model assumed that LLINs were synchronously distributed in week 180 (June 2014) and week 350 (September 2017) in all districts, and that both campaigns and all districts had the same LLIN coverage. ‘Seasonal time’ represents the different weeks of the year and was included to account for existing seasonality in malaria incidence resulting from seasonal climate conditions. This variable was smoothed in a non-linear way using cyclic cubic regression splines (k=52), limiting discontinuity between the end and the beginning of a new year. The ‘continuous time’ variable was included to account for potential long-term effects on malaria incidence over multiple years, for example, due to climate change, land-use change and improved access to healthcare. Its df was heavily restricted to avoid confounding with the other time components (k=1). ‘Health district’ was included as a random effect to account for differences in average malaria incidence between districts. To ensure that the fitted values range from 0 to 1, we could not use a Binomial or Gaussian linear mixed-effects model and instead applied a model with a beta distribution, which can be used if the response variable is a continuous variable ranging from 0 to 1, with a logistic ‘link function’.32 33 The optimal amount of smoothing of the LLIN and seasonal time variables was determined by cross‐validation using the built‐in function of the R‐package MGCV.34
The importance of the explanatory variables was assessed based on χ2 tests (p values) and difference in Akaike information criterion (ΔAIC) by comparing the full model to the models with each of the respective variables removed. The effective df (edf), an estimate of the complexity of the fit, is presented with each final model. The final model fit was evaluated by assessing the R2 value and the diagnostic plots.32
To interpret if there was an increase or decrease in malaria incidence, depending on the explanatory variables, we drafted graphs where the fit and its confidence bounds are indicative.
Trends in climate and land coverage variables
To investigate whether variations in malaria incidence trends correlated with any variations in climate conditions, we developed three GAMMs with mean rainfall, day and night temperature per month as response variables (analysis done including the highland health districts only). For all the GAMMs, seasonal (cyclic cubic regression splines, k=52) and continuous-time components were included as explanatory variables, and a health district component as random variable in the same way as in the GAMM described above. Three additional GAMMs were developed to assess trends in land coverage variation over time. In these models, we used the different land coverage levels (LC10, LC30, LC40) as response variables, continuous-time as explanatory variable (smoothed in a non-linear way with k restricted to 3) and health district as random variable. We did not model LC20 because most of the health districts included only zero values throughout the period of the study.
Results
Spatial pattern of malaria incidence
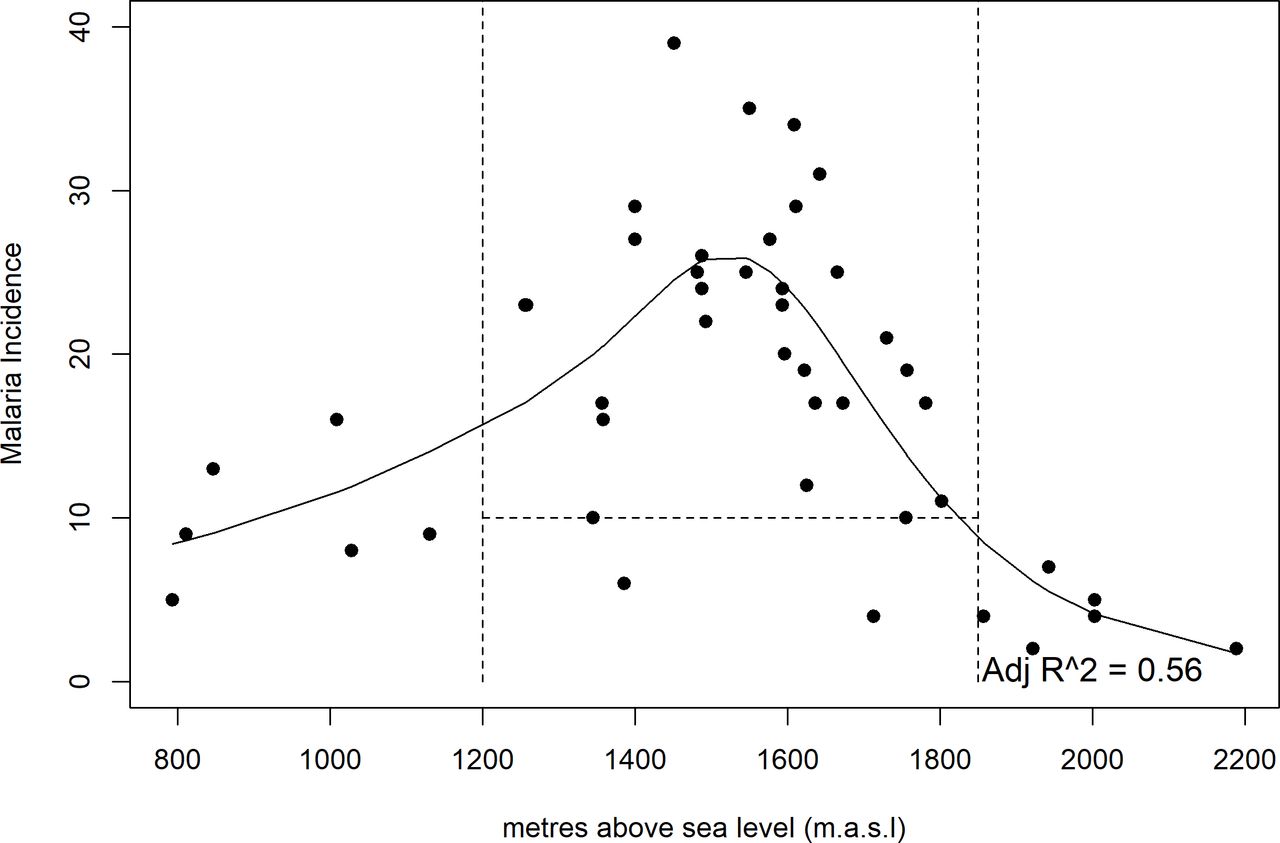
Malaria incidence varied with altitude, having the lowest incidence in health districts below 1200 m above sea level (m.a.s.l.) and above 1850 m.a.s.l. (edf=4, p<0.0001 ΔAIC=163). The highest incidence rates were reported from health districts located between 1500 and 1600 m.a.s.l. (figure 2). Districts between 1200 and 1850 m.a.s.l. with a mean weekly incidence >10/1000 population were included in the subsequent analysis and subsequently called ‘endemic highland health districts’ (ie, 24 health districts).

Median malaria incidence per 1000 population per health district in function of the elevation at the yearly malaria peak (2011–2019). The solid black line represents the median malaria incidence in function of elevation, as estimated by a generalised additive mixed model. Dotted lines represent boundaries where health districts were selected.
Effect of LLIN on malaria incidence in endemic highland health districts
The GAMM generally fitted the data well (R2=0.71), and no major deviations from the functional form or dependencies in the residual data were observed (online supplemental figure S1). The malaria incidence in endemic highland health districts showed a clear seasonal pattern (edf=16, p<0.0001, ΔAIC=1508). The seasonal pattern was characterised by a delayed (2–4 weeks) decrease in incidence after the start of the main dry season (June–August) and increased 2–4 weeks after the start of the short rainy season (September–November) (figures 3, 4A, 5B). A small incidence trough was found after the end of the short dry season in January–February (figure 4A).
Supplemental material
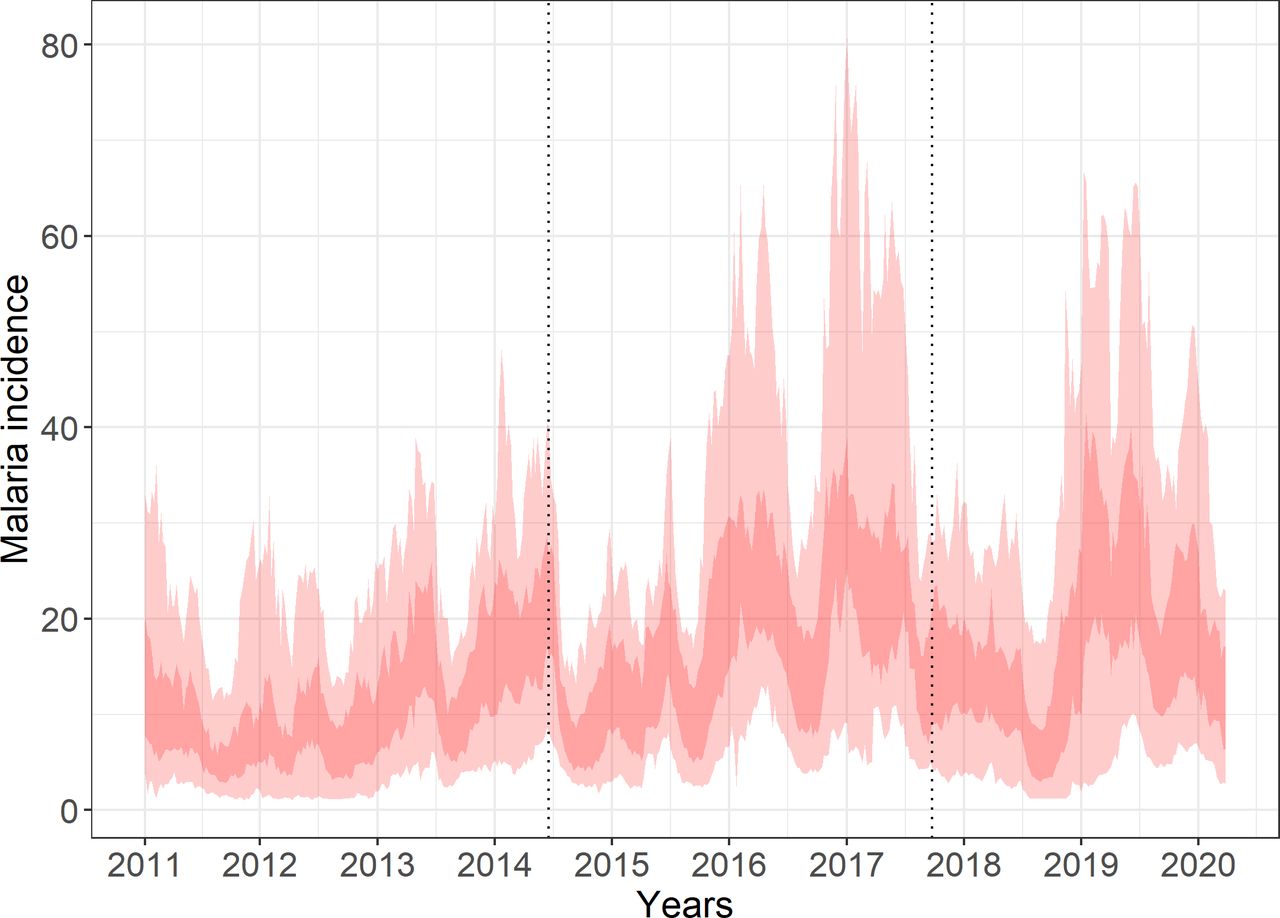
Weekly malaria incidence (cases per 1000 people) for endemic highland health districts between 1200 and 1850 m elevation in Burundi. The envelope represents the interquartile (dark red) cases for the health districts with minimum-maximum values (light red). Vertical dotted lines represent time periods when LLINs were distributed in the different health districts. LLINs, long-lasting insecticidal nets.

The effect of different time components on malaria incidence (cases per 1000 population) in the endemic highland health districts of Burundi as estimated by a generalised additive mixed model. (A) Seasonal fluctuations during the year. (B) The effect of LLIN distributions in 2014 and 2017. (C) The trend during the entire study period. The envelope represents the 95% CI on the average malaria incidence estimated over all time periods and health districts. LLINs, long-lasting insecticidal nets.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
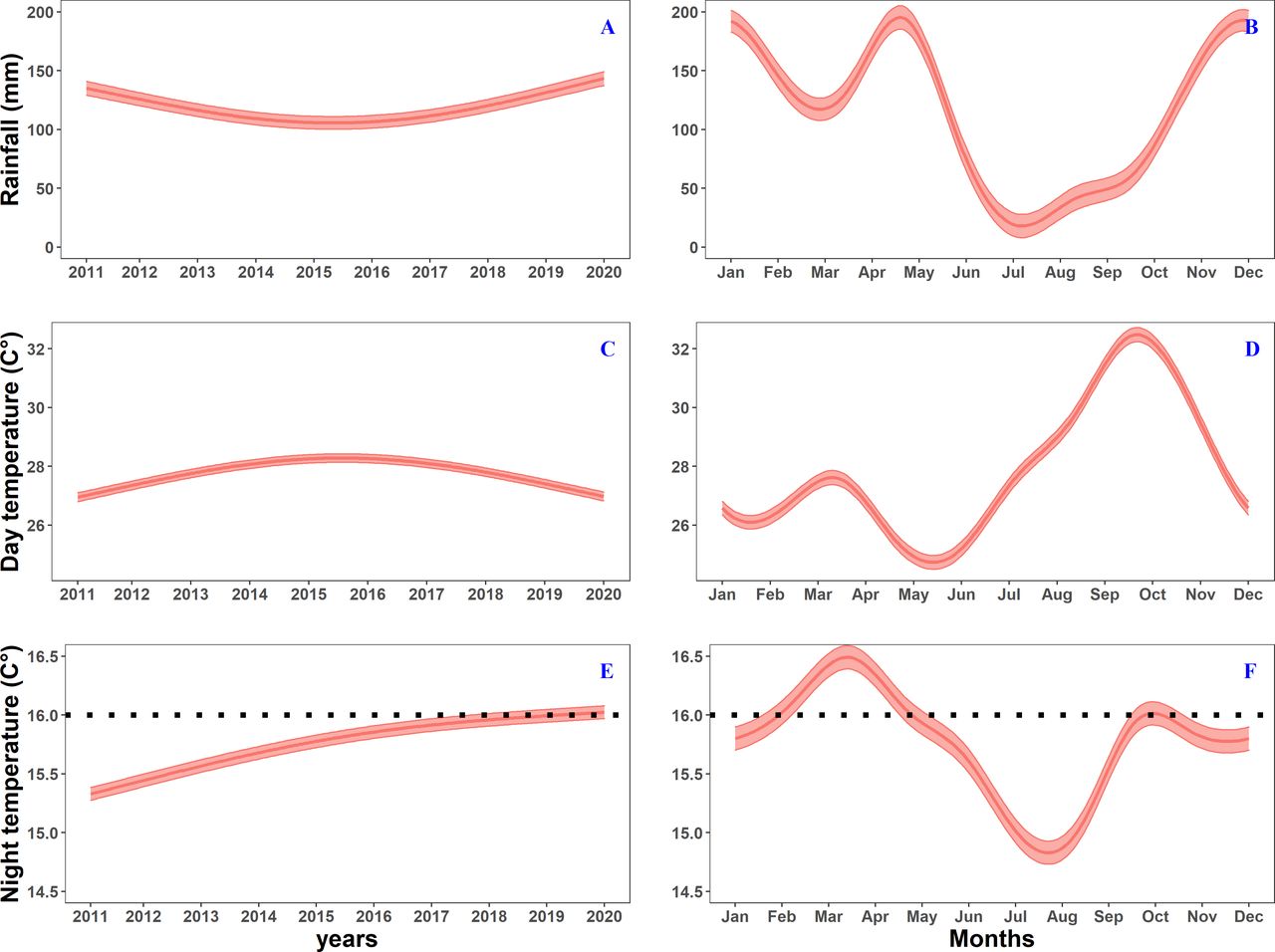
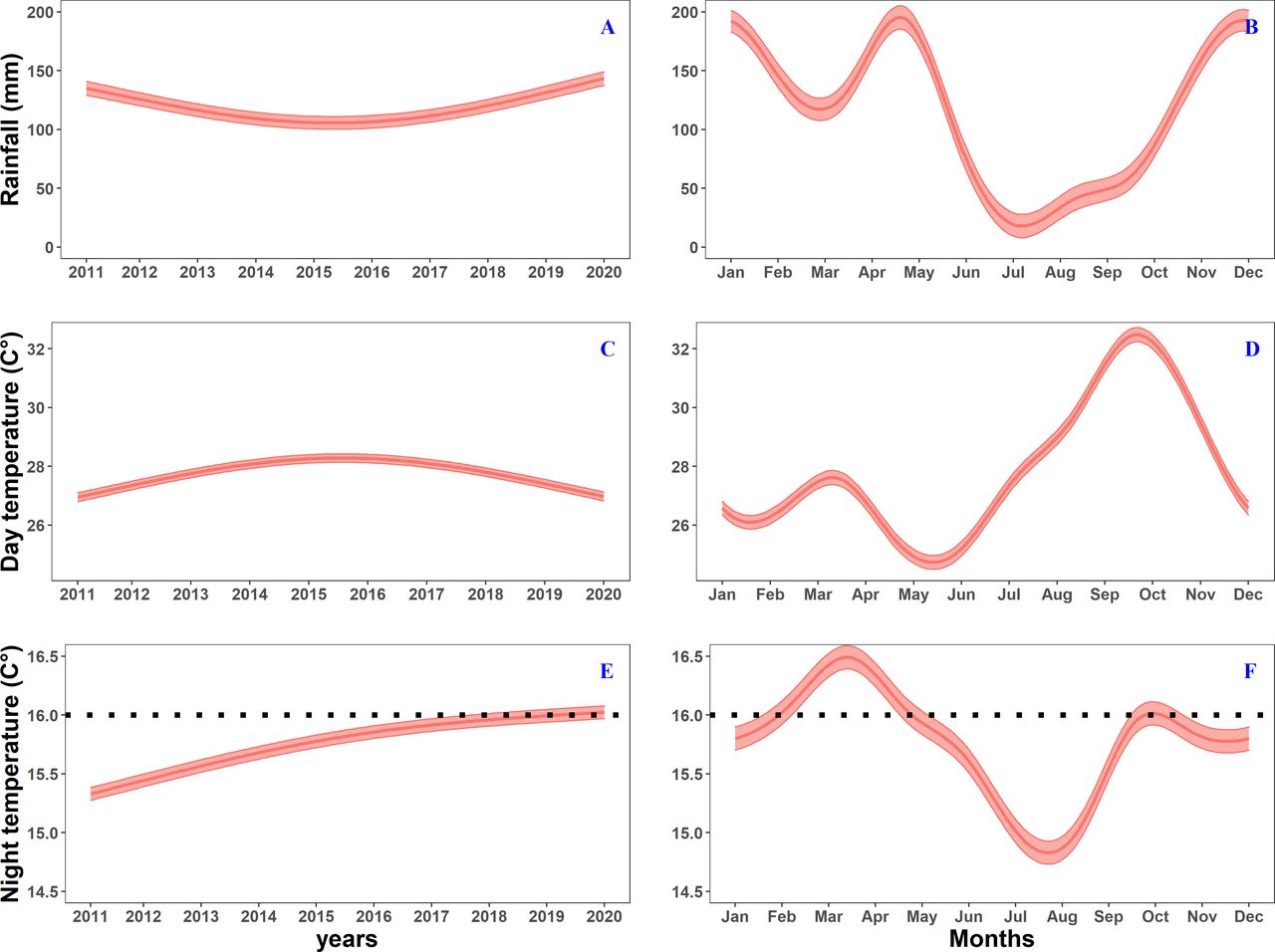
Estimated mean climate variables as function of seasonal and continuous time components as predicted by generalised additive mixed models for the endemic highland health districts in Burundi. (A, B) Show rainfall as function of time, (C, D) show changing day temperatures as function of time and (E, F) show changing night temperatures as function of time. The black dotted line in figure (E, F) represents the minimal required temperature for Plasmodium falciparum’s sporogony. The red envelope represents the 95% CI on the average climate variable estimated over all time periods and health districts (see online supplemental figure S2 for the full time-series model).
The effect of the LLIN distribution on malaria incidence was significant (edf=9, p<0.0001, ΔAIC=814). The malaria incidence decreased during the first weeks after the LLIN distribution (figure 4B), demonstrating the most important effect between week 20 and week 40 postdistribution, while a decrease of effect can be observed afterwards, coming to predistribution malaria incidence levels at week 65. It increased further to levels higher than before the LLIN distribution in years 2 and 3. The overall trend of malaria incidence showed a non-linear increase (edf=2, p<0.0001, ΔAIC=1903) (figures 3C and 4C).
Trends in climate and land cover variables
We observed clear seasonal trends for the three climate variables (table 1) with seasonal night temperature also fluctuating around the minimal required temperature for P. falciparum sporogony (figure 5B, D and F). The overall mean night temperature in the health districts increased significantly almost linearly during the first 6 years (edf=1.9, p<2e-16, ΔAIC = −353, figure 5E). The observed effect was small (+0.7°C over 6 years) but occurred around 16°C which is the minimal required temperature for P. falciparum sporogony35 (figure 5E). We only found a slight but significant parabolic trends in mean rainfall (edf=1.9, p<0.0001, ΔAIC = −83, figure 5A) and mean day temperature (edf=1.9, p<0.0001, ΔAIC=245, figure 5C). Although the different land cover variables significantly decreased over time in models that included a time component (based on p values), models without a temporal component were preferred based on AIC values (table 1, online supplemental figure S2). Therefore, it remains difficult to conclude that land-use change (as measured by LC10, LC30 and LC40) explains variation in the malaria incidence.
Summary statistics of the different climate and land cover variables that could affect malaria incidence in Burundi
Discussion
Based on a time series of routinely collected surveillance data, we noted a fast and steep decline of malaria incidence during the first year after the mass LLINs distribution of 2014 and 2017 in Burundi. This supports the utility of LLINs in the control of malaria in an endemic highland setting with marked seasonality. However, LLINs seemed to lose their impact after only 1 year, with a higher proportion of malaria cases recorded in the following years. Our findings are similar to a longitudinal analysis of malaria-endemic regions in Madagascar that reported a decline in reported malaria alerts through sentinel site monitoring and increasing alerts after 2 and 3 years following mass distribution campaigns of LLINs.36
The noted malaria incidence above pretreatment levels after 2 years might be due to an increase in susceptible individuals after the intervention in an area where immunity might have already been low because of the marked seasonality of malaria transmission.37 The initial benefits after the intervention may be countered by a greater disease burden, as immunity (or at least protection from severe disease) wanes.38–42 The rebound effect is also well documented in association with premature discontinuation of IRS, not-timely replacement with LLINs in a high transmission setting,43 and when (seasonal) chemoprophylaxis are abruptly stopped.44 45 The overall conclusion of these studies, and ours, is that sustainable malaria control is only possible through continuously maintained interventions that keep transmission suppressed in endemic settings. Sustained and increased investments in malaria control are crucial to achieve this purpose.46 The provision of insecticide treated nets is such an investment that largely contributed to the observed worldwide decline of malaria.1
The initial decline of malaria incidence during the first year after the LLIN mass distribution can be explained by the initial high coverage and high use,24 25 which is in line with the modelled net access and use by Bertozzi-Villa et al.47 The reasons for the fast decline of the LLINs effect, before the three full years of expected lifespan, in the highland setting of Burundi might be multiple and related to the fast loss of physical integrity of the nets.48 The loss of physical integrity of LLINs will impact the use of the nets as shown in a study in Ethiopia where damaged LLINs were less commonly used.17 Also, torn nets are used for other purposes in Burundi and are no longer kept in the houses (WVB and CL, personal observations), further decreasing LLIN use. Studies in different African settings also showed that the effective lifespans of LLINs in the field are often shorter than 3 years, and rather depends on local conditions (influenced by living conditions and local behaviour of net maintenance that impact damage) than related to a specific LLIN brand.8 48 Another factor that might have contributed is the loss of bioavailability of the insecticide because of the dirtiness of the nets after 1 year (WVB and CL, personal observations). In addition, insecticide resistance of the main vector species A. gambiae and A. funestus might have decreased the community protection of the LLINs.49 50
Given the central role of insecticide-treated bed nets in reducing the burden of malaria during the past decade and the role it can play in the control of highland malaria as shown in this study, the use, durability and pyrethroid resistance will need to be managed carefully.51 In Burundi, the main vector species A. gambiae and A. funestus are endophagic and active when people are sleeping. Hence, effective LLINs have the potential to substantially contribute to malaria control. In the short term, the LLIN distribution strategy needs to be adapted to the local condition where nets are only effective for a short period of time. This can include more frequent mass distribution campaigns or a stronger reliance on routine distribution channels. In the long run, human behavioural, socioeconomic and entomological factors affecting the effective lifespan of LLINs need to be understood to optimise the impact of nets.
Malaria in Burundian highlands, primarily caused by P. falciparum and transmitted by A. gambiae and A. funestus, is clearly seasonal. The pattern is characterised by a delayed (2–4 weeks) decrease in incidence after the start of the main dry season (June–August) and an increase after the beginning of the short rainy season (September–November). Over the period 2011—2019, we observed a non-linear increase in incidence. Although it is impossible to pinpoint one factor to explain this increasing trend due to the correlative nature of our study (eg, the shift from paper based to DHIS2 in 2014 might be a confounder), it is of interest that the overall mean night temperature in the health districts also increased significantly in an almost linear way towards 16°C, the threshold above which P. falciparum sporogony can happen.35 52 A small increase in mean night temperature above this threshold might result in a steep increase in malaria cases. The malaria vectors A. gambiae and A. funestus often find suitable microclimates inside houses where the temperature is high enough for the sporogony of the parasite. The increase of the mean night temperature outside human dwellings indicates that the parasite’s sporogonic development might not to be hampered when the vectors forage outside or seeking breeding sites. It is likely that a further increase in night temperature, as expected by global climate change, will result in an increased malaria incidence until the optimal temperature boundary is reached, after which the incidence will decrease due to a reduction in survival rate of the adult mosquito (as empirically shown in different areas in Kenya).53 54
Based on our analysis, changing trends in rainfall, mean day land surface temperature and land-use were less likely to have affected the malaria incidence during the past decade in Burundi’s highlands.
This study was based on routine surveillance data collected from the entire population of the study areas on a weekly basis. This is not the case with typical cross-sectional surveys, which are often intermittent and underpowered. In Burundi, the completeness of DHIS2 reports is high, being 92% since 2014, and the case definition follows WHO recommendations and did not change over the study period, which gives more confidence of using these data for intervention evaluation.12 In the field of evaluation of impact of infectious disease control interventions, routine surveillance data are recognised as a rich source of data but yet underused, as is the case for malaria.19 Yet, these data have inherent limitations related to the potential reporting bias by the health districts. Also, as diagnosis relies on the availability of RDTs, stock rupture at the district level might impact case reporting. The analysis was based on the inclusion of 24 health districts. To account for both systematic and random natural variation in malaria cases between these districts, we included a health district component as random effect in the model. The routine case data only include people seeking care, which might underestimate the actual burden of malaria in Burundi.12 Yet, we could not account for possible changes in healthcare access or testing. Further, no information on severe malaria disease nor age group was available, limiting the interpretation of the data.
Conclusions
This is the first time that LLINs are evaluated in Burundi under operational conditions. This study highlights that LLINs did reduce the incidence in the first year after a mass distribution campaign, but in the context of Burundi the duration of the effective lifespan seemed to be much shorter than the 3 years distribution interval recommended by WHO. The reasons underlying these findings are legion, possibly related to human behavioural, socioeconomic and entomological factors, and need to be understood to enhance their impact to control malaria in such settings. Our results highlight the importance of continued epidemiological monitoring of malaria and the utility of routinely collected data to evaluate the temporal and spatial trends of malaria across the country to improve resource allocation and malaria control efforts. Further, the analysis also point to the importance of sustaining vector control to keep transmission suppressed and the need for continuous investment in improving the effective lifespan of LLINs or to adapt distribution campaigns to make ‘effective LLINs’ continuously available in the community.
Supplemental material
Data availability statement
Data are available on reasonable request. The analysis presented in this study is based on the malaria incidence between 2011 and 2019 using routinely collected surveillance data obtained from the National Health Information System. Data are aggregated at health district level. No information is available on severity nor gender.
Ethics statements
Patient consent for publication
Acknowledgments
This work is done in the context of a research collaboration agreement between Médecins Sans Frontières-Operational Center Brussels and the Institute of Tropical Medicine (ITM), Antwerp (Belgium) on malaria outbreaks in Burundi Highlands. The Outbreak Research Team of the ITM is financially supported by the Department of Economy, Science and Innovation of the Flemish government. Joachim Mariën is currently a research assistant of Research Foundation Flanders (FWO). The covariate data were supplied by the project 'Monitoring outbreak events for disease surveillance in a data science context' (MOOD), which is funded by EU grant 874850. The contents of this publication are the sole responsibility of the authors and do not necessarily reflect the views of the European Commission.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Alberto L Garcia-Basteiro
WVB and JM contributed equally.
Contributors WVB and JM conceptualised this study, performed the analysis and drafted the manuscript. BKMJ supported the data analysis, supported the interpretation of the study results and revised the manuscript. DS and PS provided the data and information on the implementation of the malaria control interventions in Burundi and supported the interpretation of the results. EL, RD’h, J-MM and ADW provided general support to the study, supported the interpretation of the study results and reviewed the manuscript. FV supported the conceptualisation of this study and reviewed the manuscript. NA and WW provided the co-variate data on precipitation, temperature and land use in a preprocessed and ready-made format. PM contributed to the interpretation of the results, provided general support to the study and reviewed the manuscript. VV supported the conceptualisation of this study, contributed to the interpretation of the results and reviewed the manuscript. CL supported the conceptualisation of the study, provided access to the routinely collected data and drafted the manuscript. All authors read, amended and approved the manuscript. See online supplemental 2 for the author reflexivity statement. WVB is acting as guarantor.
Funding Department of Economy, Science and Innovation of the Flemish government (Belgium) (no grant number); EU – H2020 Grant Number 874850; Fonds Wetenschappelijk Onderzoek (no award number).
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The reflexivity statement for this paper is linked as an online supplemental file 2.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.