Article Text

Abstract
Introduction The extraordinary explosion of state power towards the COVID-19 response has attracted scholarly and policy attention in relation to pandemic politics. This paper relies on Foucault’s theoretical differentiation of the political management of epidemics to understand how governmental framing of COVID-19 reflects biopolitical powers and how power was mobilised to control the pandemic in Zimbabwe.
Methods We conducted a scoping review of published literature, cabinet resolutions and statutory instruments related to COVID-19 in Zimbabwe.
Results The COVID-19 response in Zimbabwe was shaped by four discursive frames: ignorance, denialism, securitisation and state sovereignty. A slew of COVID-19-related regulations and decrees were promulgated, including use of special presidential powers, typical of the leprosy model (sovereign power), a protracted and heavily policed lockdown was effected, typical of the plague model (disciplinary power) and throughout the pandemic, there was reference to statistical data to justify the response measures whilst vaccination emerged as a flagship strategy to control the pandemic, typical of the smallpox model (biopower). The securitisation frame had a large influence on the overall pandemic response, leading to an overly punitive application of disciplinary power and cases of infidelity to scientific evidence. On the other hand, a securitised, geopolitically oriented sovereignty model positively shaped a strong, generally well execucted, domestically financed vaccination (biopower) programme.
Conclusions The COVID-19 response in Zimbabwe was not just an exercise in biomedical science, rather it invoked wider governmentality aspects shaped by the country’s own history, (geo) politics and various mechanisms of power. The study concludes that whilst epidemic securitisation by norm-setting institutions such as WHO is critical to stimulate international political action, the transnational diffusion of such charged frames needs to be viewed in relation to how policy makers filter the policy and political consequences of securitisation through the lenses of their ideological stances and its potential to hamper rather than bolster political action.
- Health policy
- Health systems
- Review
- Public Health
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
COVID-19 led to the explosion of state power in dealing with the pandemic, including in Zimbabwe.
The government of Zimbabwe responded to the pandemic with a range of public health strategies that were influenced by the broader contextual environment.
WHAT THIS STUDY ADDS
By applying Foucault’s theory of biopower, the paper departed from the traditional biomedical-oriented approaches to analysing the COVID-19 response in Zimbabwe and unpacked how framing and the mechanisms of sovereign, discipline and biopower shaped the political response to the pandemic.
The ideological ramifications of securitised frames in countries with highly charged (geo) political contexts such as Zimbabwe need to be checked since the intersection of such frames with prevailing ideologies can serve to both advance or retard intended policies.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
An effective epidemic response in Zimbabwe should not only emphasise the biomedical aspects while viewing history, power and politics as encumbrances; instead, a pragmatic approach that strategically endeavours to accommodate biomedical science within the realities of local context while seeking to capitalise the productive use of political power is required.
Introduction
On 30 January 2020, WHO declared coronavirus—the pathogen causing COVID-19—as a public health emergency of international concern.1 The declaration is WHO’s highest level of alarm—a rallying call to all countries is to immediately take notice and take action. Starting as an unknown pneumonia originating in Wuhan, the lexicon around the disease quickly shifted to ‘alarming’, ‘extraordinary’ and ’serious’ which culminated in pandemic declaration on 11 March 2020.2 The import of these words—meant to galvanise international action—is also emblematic of securitisation. The Copenhagen School defines securitisation as a speech-act process ‘through which an inter-subjective understanding is constructed within a political community to treat something as an existential threat to a valued referent object and to enable a call for urgent and exceptional measures to deal with the threat’.3 Securitisation of the COVID-19 epidemic became an international norm defined and promoted by WHO as a norm entrepreneur, and cascaded down to the level of member states.4 One central feature of the securitised discourse was the explosion of state power in dealing with the pandemic.
This paper analyses the influence of one form of power that is relevant to the government of pandemics—biopower—in relation to the COVID-19 response in Zimbabwe. The first case of COVID-19 in Zimbabwe was reported in March 2020 followed by a response trajectory consistent with state interventions to protect the health of the population or ‘biopower’.5 From this premise, this study aimed to understand the challenges and opportunities arising from the biopolitical response to the COVID-19 pandemic in Zimbabwe by examining two intertwining aspects: (1) How did the governmental framing of the COVID-19 pandemic reflect biopolitical powers? (2) In what ways was biopower mobilised in the Zimbabwean response to the COVID-19 pandemic? The rest of the paper is structured as follows. First, we present the analytical framework of biopower. Second, we describe the methods used to gather and analyse the data. Third, we present the findings that directly answer the two research questions. We then discuss the findings and conclude.
Analytical framework
Biopower is a concept coined by a French philosopher, Michel Foucault. It describes a form of power that exerts a positive influence on life, which endeavours to administer, optimise and multiply it, subjecting it to precise controls and comprehensive regulations.5 Closely related is the concept of biopolitics which is the style of government that regulates populations through biopower. According to Foucault, knowledge is linked to power and central to the analysis of power is the production of a discursive norm.6 In his power analysis, Foucault returned time and again to three infectious diseases and described the political response to them as models for three different forms of government namely: leprosy, plague and smallpox.7–10
The leprosy model: sovereign power
In his work Madness and Civilization: A History of Insanity in the Age of Reason that was first published in 1961,10 Foucault writes about the widespread infection of the population with leprosy from the beginning to the very end of the Middle Ages in Europe and proliferation of institutions accommodating those sick with the disease.10 The views towards the disease were viscerally hostile during the period, mainly driven by fear and moral stigma while those infected with the disease (lepers) were perceived as unclean both physically and spiritually. During the era, a form of power emerged that separated the healthy from the sick and excludes societal deviants. This form of power is associated with monarchical authority during the rise of modern Europe, when authorities could sovereignly rule through decrees. Foucault presented the sovereign power as legislative, prohibitive and censoring; a power that primarily makes use of the law and law-like regulations.11 12
The plague model: disciplinary power
In his work Discipline and Punish: The Birth of the Prison,8 that was published in 1975, Foucault introduces a description of a new model of management that originated as a response to the outbreak of another contagious disease—the plague. Unlike lepers who were socially ostracised, those infected by the plague were at the centre of the administrative system for the purpose of understanding and establishing the scope of the disease.13 The distinction in the models is a function of time and related to the aetiological differences between the two diseases. Leprosy was a relatively rare disease, with a low rate of transmission, advanced slowly and did not affect large groups but rather isolated individuals, which made the process of diagnosis quite easy and isolation of the infected much easier. Contrarily, the plague was highly contagious, spread rapidly and affected the entire communities which made the timely identification of the infected and their isolation from the community impossible.14 Thus, instead of ostracising the infected, typical of the leprosy era, the plague era shifted to the idea of introducing quarantine and monitoring mechanisms for the purpose of establishing a disciplined society or the exercise of disciplinary power.7
Smallpox model: biopower
In his lectures given in 1978 at the Collège de France, published in the book Security, Territory, Population,9 Foucault presented the third model of confronting infectious diseases, this time focusing on managing a crisis caused by the pandemic of smallpox in the 18th century. While the leprosy and plague models conjure a dark side of power, the smallpox model views power in a positive light. Unlike the repressive methods typical of the leprosy and plague eras, the phenomenon of the smallpox outbreak shifted the focus of attention to the understanding of the epidemic itself through determining the number of the infected, their age, medical consequences and mortality using statistical methods or biopower.9 Also accompanying biopower is the promotion of preventive measures to avert the spread of the infection including the use of vaccines and understanding their associated benefits and risks.15 Again, the shift from the leprosy and plague to smallpox model is also centred on differential aetiology. Smallpox was characterised by sudden and high increases of the number of infected and high death rate, which made the understanding of the course of the epidemic a priority.15 Preventive techniques that could be applied to the entire society without material and economic difficulties were thus more favourable, and, as Foucault points out, they were not the product of a known economic theory but of sheer practice and collection of field data.9 One of the underlying principles of biopower is the dividing practices that categorise the population according to vulnerability.16
Methods
This article used scoping review methods developed by Arksey and O’Malley (2005)17 to understand governmental framing for the COVID-19 in Zimbabwe and the mobilisation of power to respond to the pandemic. We selected this approach because of its emphasis on flexibility, relying on an abductive logic of enquiry, and its bias towards narrative-driven summation. The framework is presented as an iterative, qualitative review with five distinct stages: (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data and (5) collating, summarising and reporting the results.
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research since the study was aimed at understanding biopolitical power at the policy making level.
Research question
How did the governmental framing of the COVID-19 pandemic reflect biopolitical powers in Zimbabwe and in what way (s) was power mobilised in response to the pandemic?
Identifying relevant studies/data search
We conducted a search in electronic databases and search engines. We also conducted grey literature search.
Electronic databases and search engines
Between May and November 2022, we conducted a literature search in four electronic databases: EBSCOhost, PubMed/MEDLINE and WHO Index Medicus. We used the search terms COVID-19 AND Zimbabwe AND politics AND government and COVID-19 AND Zimbabwe AND Response. The search terms were deliberately broad since we anticipated that specific terms such as biopower might not be necessarily mentioned in the relevant literature. We also searched Google and Google Scholar.
Grey literature search
We purposively searched from the website of Veritas. Veritas provides information on the work of the courts, Parliament of Zimbabwe and the laws of Zimbabwe to the public. It archives relevant cabinet resolutions, statutory instruments (SI), bills, constitutional affairs and other law-related artefacts in an easily retrievable format. For this study, we retrieved postcabinet meeting statements issued from 4 February 2020 (corresponding to the onset of COVID-19) to 22 March 2022 and SIs on COVID-19 that were gazetted from March 2020 to October 2022.
Inclusion and exclusion criteria
To be eligible, a publication had to meet the following criteria: (1) solely focusing on Zimbabwe, (2) inclusion of Zimbabwe for papers that covered multiple countries and (3) cover the wider governmentality aspects that enabled, legitimised and justified the exercise and form of power for the COVID-19 response (consisting of the set of institutions, procedures, knowledge and strategies).
Screening
ATM conducted the screening for the electronic databases and grey literature.
Screening of papers from electronic databases
The initial database search generated 1128 papers. No time limit was set for the studies. Screening of the relevant papers involved three sequential stages. The first stage involved title screening of all the papers. From the title screening, 1017 papers were excluded mainly for being biomedical-oriented title (eg, focusing on laboratory testing) and not covering Zimbabwe. Of the 111 papers remaining, 18 duplicates were removed. After initial title screening and duplicate removal, 93 papers were eligible for the second stage which involved abstract screening. Out of these, 75 were excluded chiefly for focusing on the severity of the pandemic, its socioeconomic impacts, its implication on access to other health services, lack of preparedness and the need for urgent action. Of the 18 papers that were eligible for full article screening, all of them were found to be eligible for inclusion. A similar search process on Google and Google Scholar yielded 16’ additional papers, making a total of 34 papers that were eligible for full analysis.
Screening of cabinet statements and SIs
For both cabinet statements and SIs, a whole document was downloaded, and the entire text was read. A total of 56 cabinet statements mentioning COVID-19 were retrieved from the Veritas website, covering the period between 7 April 2020 and 22 February 2022. Out of these, 26 were found to be eligible. The other 30 were excluded mainly for mentioning general health system updates such as renovation of hospitals, industrial manufacturing of COVID-related materials and updates on availability of medical supplies. In terms of SIs, we retrieved a total of 68, covering the period between 23 March 2020 and 7 October 2022. Out of these, 17 were found to be eligible. The other 51 were excluded mainly for being minor repeals and replacements of the main SI, including spelling corrections and minor additions. Figure 1 shows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
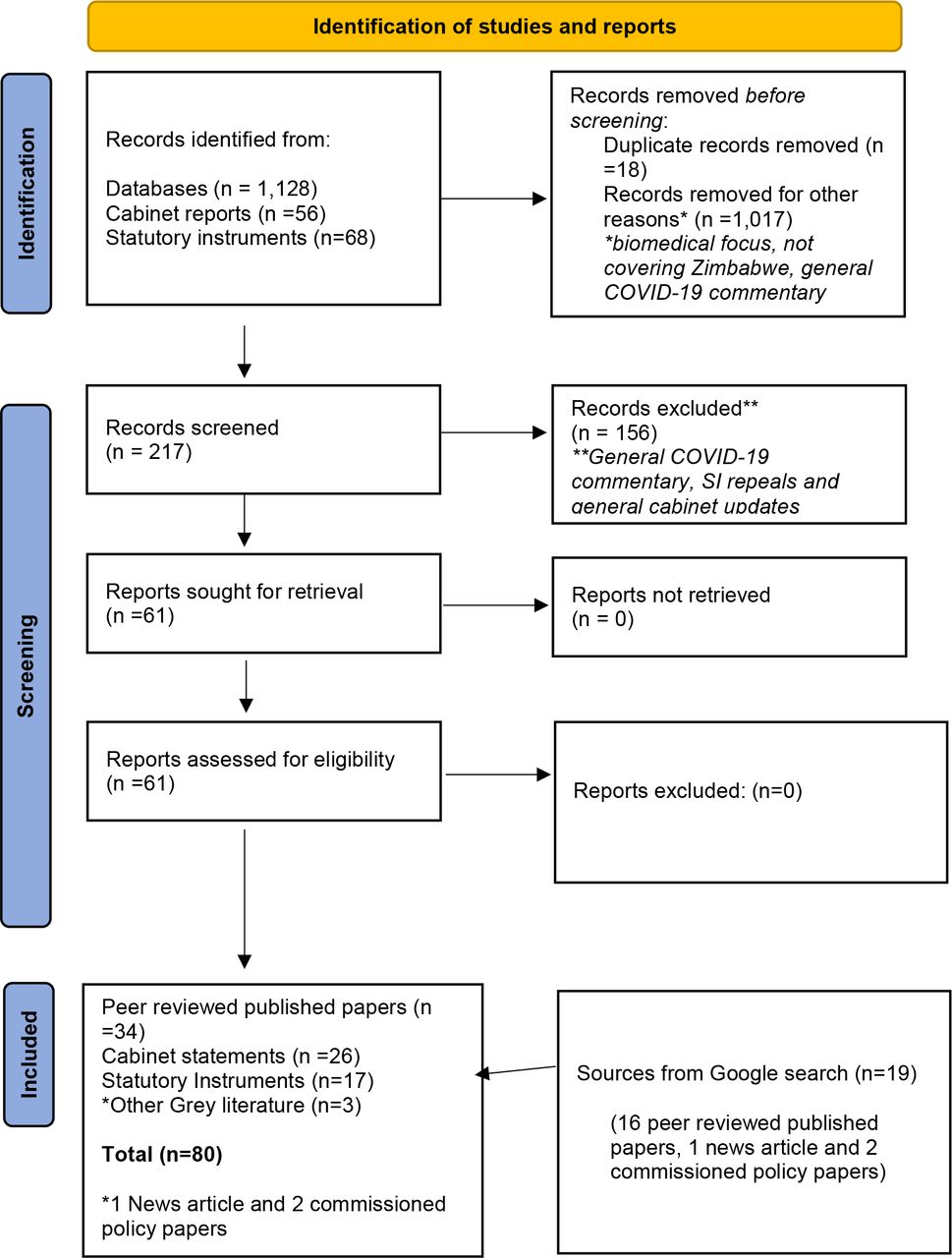
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. SI, statutory instrument.
The full list of included studies and cabinet statements is presented in online supplemental file 1.
Supplemental material
Data extraction
After identifying eligible articles, ATM conducted the data charting. Data charting is a technique for synthesising and interpreting qualitative data by sifting, charting and sorting material according to themes. A data charting tool (extraction tool) was developed in Microsoft Excel capturing essential characteristics such as the title of the paper, author, journal and year of publication. For the cabinet statements and SIs, we captured the title (for the SI, both the SI name and the actual regulations), the year and the date of release.
Data analysis
We conducted a thematic analysis by categorising the contents of each eligible article according to sovereign power, disciplinary power and biopower. The first step involved verbatim extraction of text excerpts from the selected articles which were categorised according to the themes in the data charting tool. The second step involved an iterative process of interpretive data analyses and refining.
Findings
The following sections present the findings of the study. We first present governmental framing for COVID-19 and then turn to the mechanisms of power mobilised in dealing with the pandemic.
Governmental discursive framing of the COVID-19 pandemic
We identified four discursive frames that shaped the COVID-19 response in the country: ignorance, denialism, securitisation and state sovereignty frames.
Ignorance and denialism frame
The early framing of COVID-19 vacillated between ignorance and confusion in relation to the threat imposed by the disease and who was affected.18 Addressing a political rally, when Zimbabwe had not reported any COVID-19 case while cases have started rising in other countries, a high-ranking ruling party official remarked:
Coronavirus is the work of God, punishing countries that imposed sanctions on us. They are now keeping indoors. Their economies are screaming just like they did to ours. Trump should know that he is not God.19
While this remark infers a false sense of invincible immunity on the part of Zimbabweans, which can be regarded as stemming from ignorance, it is more of geopolitical posturing than a random act of epidemic misfiring.
Denialism was also prevalent at both governmental and community levels. As of February 2020, the Minister of Health believed that COVID-19 was not a threat to the country and insisted that inter-country travel with China was safe.20 Ironically, at that stage China was the global epicentre for COVID-19 and it had imposed own travel restrictions. Ignorance and denialism were also present among the general citizenry. In an obituary for the first Zimbabwean to succumb to COVID-19, a journalist wrote:
…there was a feeling, among some of us, that coronavirus was some distant offshore pandemic. There was this myth, black people were immune to this virus and it could not survive in our hot conditions. We also told ourselves it only posed a danger for those above 70 years, and not the African youths, the ghetto youths.21
This racialised framing of COVID-19 as a ‘Whiteman’s disease’ was also prevalent at the community level.22 This pandemic ‘othering’ also shaped blame attribution for the origin of COVID-19 as captured in the following statement by a high-ranking government minister:
Isn’t it that there is another serious upsurge of Covid-19 cases in China? It’s them who had botched experiments. Now that’s killing us. They can’t reverse it anymore. Look at where the people we call friends have taken us to.23
Securitisation frame
On 17 March 2020, the President of Zimbabwe declared a national disaster over COVID-19. The securitised frame was quite apparent in his televised speech, describing the virus as a ‘threat’ while remarking that ‘humanity is at risk and stands at hazardous crossroads’.24 It is also important to note that at the point of declaration, Zimbabwe had not reported any case. Following the first COVID-19-related death in Zimbabwe, the cabinet acknowledged the ‘gravity’ of the pandemic. While this securitised framing is consistent with global trends, of particular interest in the Zimbabwean context is the use of military and war metaphors in framing the disease. COVID-19 was seldom framed as an existential threat and invisible enemy, with war-like language used to mobilise against the unseen enemy.25 The capability of the country to ‘fight’ the virus was also premised on the national leadership with impeccable war credentials and a track record of tact and resilience in dealing with monumental challenges. In May 2020, the then vice-president, himself a veteran of the liberation struggle, remarked:
I am sure we will conquer the current crisis just as we have done in the past. The 16 years of the brutal war towards independence taught us that no matter how hard and difficult a situation might be, there is light at the end of the tunnel.21
The belief in the efficacy of importing military strategy to fight COVID-19 was also shared within the academic circles. In their article entitled ‘The generals and the war against COVID-19: The case of Zimbabwe’, Maulani et al argued that the decorated military credentials of the country’s political leadership were strategic in fighting the coronavirus.26 Although the cases have subsided and the country much stable, the war rhetoric has lingered on, with a constant reminder that the ‘COVID-19 war is not yet over’.
Sovereignty frame
The sovereignty frame in relation to COVID-19 manifested in three ways: the emergency preparedness of the country to handle the pandemic, the capacity of the country to find ‘home grown’ solutions and the opportunity to use COVID-19 to consolidate geopolitical interests. The emergency preparedness frame emphasised that the country had capacity and was prepared to respond to COVID-19 despite the country’s disadvantaged economic position caused by Western sanctions.21 Sovereignty in relation to ‘home grown solutions’ manifested through portrayal of indigenous plant systems as effective against COVID-1927 28 and superior to Western medicine.29 The sovereignty frame also manifested in a sense of high self-efficacy to steer own breakthroughs in fighting the pandemic. At a time when the whole world was grappling to fully understand the science of the disease and find a suitable vaccine, a high-ranking cabinet minister anticipated a local breakthrough:
We have no vaccine here [yet]. I am not going to take other nations’ vaccines. Why should we not have ours? We are trying ours here (in Zimbabwe) with the Chinese. Maybe it will be successful.23
Another sovereignty frame relates to urging citizens not to be just vigilant against COVID-19 as an epidemic threat but as a national threat that could be manipulated by Zimbabwe’s aggressors to effect a regime change.23 Ahead of demonstrations planned against alleged corruption related to COVID-19 procurements in July 2020, a senior ruling party official remarked:
We know that they (opposition) have been given more than US$300 000 to sustain the planned demonstration and obviously they are being encouraged to break the law against COVID regulations. Zimbabweans should know that those who are funding these demonstrations are worried about why COVID has not killed people in Zimbabwe. And the information that we have got is that they are trying to get firing of tear gas and we are reliably informed that they also have some canisters containing COVID active material they hope to spread COVID to the Zimbabweans. We are reliably informed that they have got a mechanism of spreading Coronavirus which has been brought in by those funding the protests. So maybe what is important is to tell the Zimbabweans that it is up to their safety this time around to see how an experiment can succeed. So, this is what they are trying to do, to spread coronavirus and then blame the government for not being proactive.23
The ability of the country to deal with COVID-19 was also portrayed by re-tapping into the collective memory of the liberation for independence by reassuring the citizens that the pandemic—just like other previous foreign enemies such as colonisers—was going to be defeated.21
The sovereignty frame also reinforced self-reliance. While other countries waited for globally conceived mechanisms such as COVID-19 Vaccines Global Access (COVAX) to roll out their vaccination, the Zimbabwean government mobilised initial vaccine donations from China and thereafter allocated domestic finances to procure own doses from the same country.30 On 8 February 2021, the cabinet expressed interest to participate under the African Union (AU) COVID-19 Vaccination Programme at the same time resolving that the choice of vaccines was going to be based on independent decisions in the national interest, without undue influence.31 Two weeks later, the cabinet announced that the government of Zimbabwe had put together resources sufficient to procure COVID-19 vaccines to cover the herd immunity of 10 million people (60%).32 Self-reliance was also portrayed in how donor support was framed. In April 2021, the government acknowledged receipt of US$75 million from the Global Fund towards strengthening the COVID-19 response, but it was quick to qualify that this was complimentary since the government had largely self-funded the response, with ZW$11 billion having been released since the onset of the outbreak.33
Mechanisms of biopower
Having outlined the discursive frames that shaped the understanding of COVID-19 in Zimbabwe, we now turn to the mechanisms of power that were mobilised in relation to the pandemic response using Foucault’s theory.
The leprosy model: sovereign power
We found the exercise of sovereign power in two major forms: extended legalised power and extrajudicial power.
Extended legalised sovereign power
One of the first moves to curb the pandemic was to expand the legal powers of the central government. On 17 March 2020, the president of Zimbabwe declared a state of disaster over the COVID-19 pandemic in terms of section 27(2) of the Civil Protection Act (Chapter 10:06) of the national constitution. Subsequently, COVID-19 was declared a formidable epidemic disease in terms of section 64(1)(a) of the Public Health Act through SI 77 of 2020. As a new virus, COVID-19 was not on the existing list of ‘formidable epidemic diseases’ in section 64 of the Public Health Act. It was, therefore, necessary for the Minister of Health to make it a ‘formidable epidemic disease’ by a declaration through SI 77. To ensure compliance with the regulations, the SI spelt out a list of ‘enforcement officers’ that included police officers, health authorities and designated civil protection officers. Soldiers were later added to the list through the first amendment of the SI. On 28 March, a 21-day national lockdown effective from 30 March was declared through SI 83 of 2020. On top of the physical lockdown measures, section 14 of the SI had an effect on communication by specifying that:
For the avoidance of doubt any person who publishes or communicates false news—that has the effect of prejudicing the State’s enforcement of the national lockdown—shall be liable to a fine up to or exceeding level fourteen or imprisonment for a period not exceeding twenty years or both.34
After the promulgation of these first three SIs, SI 76 declaring national disaster, SI 77 declaring COVID-19 as a formidable disease and SI 83 declaring a national lockdown, nearly 50 follow-up SIs were issued, but still bordering on either tightening or relaxing the provisions contained in the three principal SIs. Table 1 shows a chronology of selected SIs from March 2020 to January 2022.
Selected COVID-19-related SIs in Zimbabwe between March 2020 and January 2022
Extrajudicial sovereign power
Whilst the above regulations were put in place under the pretext of controlling COVID-19, legal minds and human rights commentators raised a number of concerns regarding the extrajudicial application of sovereign power. The lockdown regulation that criminalised false reporting on COVID-19 has been viewed as a clampdown on media and speech freedom aimed at censoring legitimate criticisms of the authorities’ response to the pandemic.35 36 SI 225A on the suspension of elections was also viewed as an over-reach of sovereign power, including the paradox of lifting of lockdown measures on other areas while the moratorium on holding elections unduly persisted.36 The extrajudicial nature also manifested at the point of enforcement. The enforcement approach by the police was characterised by overzealousness, heavy-handedness and gross misinterpretation of the COVID-19 regulations in their dealing with civilians.37 This included personal humiliation, assault, illegal confiscation of vendors’ merchandise, illegal mounting of roadblocks, arbitrary arrests and indiscriminate rounding up of people into police vehicles.26 36 38 In what seemed to be the state’s tacit acknowledgement of extrajudicial enforcement of the regulations, six police officers were arrested over an accusation of assaulting two women in one of the major cities in Zimbabwe.39 The government also acknowledged that police were acting outside the regulations in dealing with civilians.37 Following a litany of legal actions against brutality by enforcement officers, the high court ruled that the police and other state security agents should respect human rights while enforcing the lockdown regulations.34 40
The plague model: disciplinary power
On 30 March 2020, the country started implementing a 21-day national lockdown through SI 83 of 2020. As described earlier, a hard lockdown was enforced encompassing home confinement, severe mobility restrictions and criminalisation of falsehood communication. Special mobility exemptions were made for the acquisition of essential items such as food stuffs and medicines. These lockdown measures and exemption mechanisms align with Foucault’s assertion of the actions that were taken when a plague first appeared in town: ‘on the appointed day, everyone is ordered to stay indoors: it is forbidden to leave on pain of death… Each family will have made its own provisions; but, for bread and wine, small wooden canals are set up between the street and the interior of the houses’.41 The lockdown was extended twice and by mid-May, a further ‘indefinite’ extension was announced. Due to a cocktail of strict lockdown measures, the extended duration and the heavy-handedness in enforcement, Zimbabwe stands out among the countries that enforced one of the ‘hardest lockdowns’.42
In line with Foucault’s conceptualisation of knowledge as a source of power, in general, lockdown measures were adjusted according to the shifting knowledge about the local and global epidemic situations. This included reversion to stiff lockdown measures (level 4) during local outbreaks—including differential tightening of regulations due to clustered outbreaks in certain geographical loci—and tightening of travel restrictions after emergence of more lethal variants such as Omicron and Delta in other countries. However, the protracted application of disciplinary measures such as the extended closure of schools at the beginning of the 2022 learning calendar against a growing body of evidence,suggesting that schools could safely reopen,led the scientific community to question why the government was obdurate to science.43 At a broader level, it may not be far-fetched to speculate that the government delayed the opening of schools to avoid a clash with teachers who had issued threats of labour withdrawal citing poor working conditions.44
In relation to penalties, as with SI 77, SI 83 on lockdown provided a range of disciplinary powers that can be summed up with the provisions below:
Any person who is found to be in breach of the lockdown shall: (a) be charged and notified that he or she will be summoned before a court to answer that charge, and ordered to return immediately to his or her home, for which purpose an enforcement officer may accompany him or her; or
(b) if he or she refuses to return immediately to his or her home, or has no home, or is unable to immediately return to his or her home by reason of being outside of a radius of 5 km (or in the case of a person who is a driver or passenger of a vehicle, 20 km) from his or her home, be treated as having escaped from any place of detention, isolation or quarantine, and accordingly may be arrested without warrant and put in any place of detention, isolation or quarantine under the terms of the principal regulations.
Violation of these lockdown regulations attracted a fine not exceeding level 12 or to imprisonment for a period not exceeding one year. As described under extrajudicial sovereign power, the arrests became excessively arbitrary. By 19 July 2020, a total of 105 000 people had been arrested for violating COVID-19-related regulations, against 101 375 tested for coronavirus,45 leading critics to voice concern that authorities had deployed proportionate resources—if not more—to arrest citizens than to respond to the pandemic.23 By November 2020, the cumulative ‘COVID-19 arrests’ had soared to 224 037, with police intending to heighten surveillance and enforcement as they cited laxity in the wearing of masks and adherence to other protocols.37 Disciplinary power was also extended to commercially oriented activities. There were widespread demolitions of vending stalls belonging to informal traders within major cities and other high-density suburbs as they were deemed to be illegal, unhygienic and potential super spreaders for the virus.42 When partial relaxation was extended to businesses, informal traders could only resume operations after formal registration and payment of presumptive tax.46
The smallpox model: biopower
Like in most countries, in the bid to control the spread of the coronavirus, the government of Zimbabwe put in place a variety of measures aimed at directly controlling routine behaviour and movement at individual and collective levels. Consistent with biopower, statistical surveillance and predictability informed the shift in response measures over time, informed by local epidemiological trends but heavily borrowing the control measures from WHO guidelines. The shifts were also informed by the evolution in the scientific knowledge and market access to relevant tools for detecting and preventing the disease. At the beginning of the pandemic—when the virus was conceived to be a distant offshore threat that could only get into the country through importation—most controls were aimed at inbound travellers. At that time, the main biopower approach was centred on mandatory quarantine at designated government-run facilities. However, unsafe and unsanitary conditions caused returnees to flee Zimbabwe’s facilities and to evade quarantine requirements by entering the country through unofficial entry points, likely facilitating viral spread in rural communities.47
When surveillance showed that local transmission superseded imported cases, very specific norms consistent with containing community spread were put in place such as mask wearing, observance of one meter apart distance between individuals, avoidance of gatherings, hand washing and temperature checks.38 Consistent with Foucault’s normalisation theory, these ‘norms’ became ingrained in the behaviour of individuals,48 particularly at the beginning of the pandemic when there was so much fear over the disease, although adherence waned over time. The advent of COVID-19 tests also shifted the nature of biopower. While early controls were geared towards quarantine and self-isolation, proof of ‘COVID-19 free certificate’ became another requirement for inbound travellers and for people returning to work. Although advances in science were meant ‘to optimize life’, they were also manipulatively used as discriminatory instruments attached to disciplinary power. For example, some private and public hospitals made a mandatory requirement for a confirmed COVID-19 negative test result before patients could access treatment and care services, a practice that had been viewed as a violation of human rights.49
The availability of the vaccine had a major influence on biopower. As stated earlier, the self-reliance sovereignty frame influenced Zimbabwe to embark on a largely domestic funded vaccination programme. In February 2021, the cabinet announced that the government had set aside US$100 million for the procurement of COVID-19 vaccines31 with a target of reaching 60% vaccination coverage to ‘achieve herd immunity’, a call that was reiterated several times.50 As a result, Zimbabwe became one of the first five countries to roll out the COVID-19 vaccine in Africa.30 With a clear mandate to achieve a herd immunity, the government steered a well-elaborated vaccination programme that involved inclusion of the private sector, vaccination campaigns and the gradual access to previously excluded groups such as children, based on expert scientific advice. By early October 2021, cabinet announced that over 13 million out of the 20 million doses needed to reach the herd immunity had been received,51 and the national vaccination coverage stood at 37.3% for the first dose and 28.3% for the second dose by mid-October.52 Thus, the country emerged as a regional front-runner in the vaccination effort.53 54 The vaccination programme has been relatively well organised since it started in February 2021 and the country’s number of administered coronavirus vaccine doses per 100 people ranked an impressive 13th in Africa as of May 2022.20 Overall, the emphasis that the vaccine did not prevent infection but protects against disease severity aligns with one of the underlying principles of biopower: abandonment of the idea of complete eradication of the pathogens towards accepting that ‘we have to live with it’.
While the preceding account is consistent with the purpose of biopower ‘to optimize life’, as the vaccine became more available, biopower started to gravitate towards the repressive character of sovereign and disciplinary power . A number of vaccination related decrees and mandates were issued, often accompanied with a set of punitive measures for those who deviated from ‘the norm’. On 29 June 2021, the cabinet announced that 20% of the front-line workers yet to be vaccinated by 14 July will not receive COVID-19 insurance payouts.55 By mid-September, the cabinet extended mandatory vaccination for all government employees, with those opting out barred from working.56 That was put into legal force by SI 234 of 2021, gazetted on 17 September 2021, which contained the provision below:
No later than the 15th October, 2021—(a) every member of the Public Service shall be fully vaccinated, and any member—(i) not so vaccinated shall be barred from the workplace after the 15th October, 2021 and not be paid while he or she is so barred.
The availability of the vaccine also reinforced one of the underlying principles of biopower: the dividing practices that categorise the population according to vulnerability. However, the categorisation approach stirred some controversy. From onset, ‘more vulnerable population’ or ‘high risk groups’ were classified as individuals with chronic conditions, the elderly and front-line health workers. However, on the occasion of receiving the first consignment of vaccine doses, a top Ministry of Health official highlighted that due to supply constraints, priority access could be accorded to front-line workers, ministers, Members of Parliament (MPs) and members of the security sector. Overall, notwithstanding the over-reach in sovereign power and the excessive disciplinary powers noted earlier, the biopower approach employed by the Zimbabwean government in relation to controlling COVID-19, encompassing scale-up of the vaccine programme, the vigorous containment measures and decentralising testing has been credited for helping to control the spread of the virus.50
Discussion
The mechanisms of power mobilised to deal with the COVID-19 pandemic in Zimbabwe aligned with Foucault’s ideal typical description and theoretical differentiation of the three derived management models reflecting the historical and political responses to the emergence of three infectious diseases: leprosy, the plague and smallpox. Underpinning these power mechanisms are interlocking discursive frames that were constructed to negotiate a shared understanding of COVID-19 and make attributions regarding who or what is to blame, articulate an alternative set of arrangements and urge others to act in concert to affect change.57 The securitisation frame emerged as the overarching driver for directing the overall response which led to a largely plague-based model rooted in the mechanisms of disciplinary power. While overlaps in the mechanism of power could be expected, the persistence of a securitised sovereignty frame and the dominance of disciplinary power throughout the pandemic—even in the face of shifting knowledge—are suggestive of a biopower response that was subjected to science and monitored by a similar ideology. From this premise, the findings of this study are significant in five respects in relation to the COVID-19 response in Zimbabwe, with potential for wider implications.
First, this study underscores that how epidemics are presented or portrayed (framing) does matter. Essentially, framing shapes the perception of what needs to be done, the urgency required, how it has to be done and who is to be involved. Framing of COVID-19 as a distant, offshore divine punishment induced both ignorance and denialism as the case with HIV/AIDS in the 1990s58 and cholera in the late 2000s.59
COVID-19 ‘othering’ and denial were also prevalent in other developing countries60 and developed countries alike,61 in all contexts inducing either outright complacence or enervated actions. However, when the frame shifted from denialism to securitisation, there was an upswing in the approach from a lackadaisical one to a very aggressive form characterised by extrajudicial sovereign power and excessive disciplinary power.
Second, this study demonstrates that the transnational diffusion of frames to country level depends on how policy makers filter the policy and political consequences of securitisation through the lenses of their ideological stances. A comparison of administrative instruments between Zimbabwe and Botswana—its neighbouring country—showed that while both countries invoked a similar securitisation frame, Botswana had a much moderate application of sovereign and disciplinary powers.36 This is in line with other scholars who have noted that the securitisation of the COVID-19 at the level of the member states was a political choice by policy makers and not a ‘natural’ state, as scholars of the Copenhagen School have argued.62
This therefore suggests that it is not the securitisation frame itself that invokes dark power, but how local policy makers engage in sense making of such frames within their ideological inclinations. This underscores that when norm-setting institutions such as WHO securitise epidemics, to stimulate biopower, it is importnat to consider the unitended consequnces associated with such charged frames. This is because in practice, the intersection of such frames with prevailing ideological stances at country level can inspire ultrasecuritisation, y that invokes excessive application of sovereign and disciplinary powers that can actually hamper rather than bolster the epidemic response.
Third, this study has shown that the COVID-19 response in Zimbabwe was far from a purely biomedical mechanism for disease control. Rather, it sparked several wider governmentality issues that invoked ideological framings and mobilisation of various mechanisms of within the country’s history, politics and power dynamics. Of particular interest is how COVID-19 opportunistically resuscitated the existence of sanctions, a polarising subject that has placed Zimbabwe at loggerheads with Western countries since the early 2000s with widely divergent frames on their existence, nature and effects.63 64 Thus, the government portrayed sanctions as one of the foremost constraints in responding to the pandemic whilst raising the tempo for their removal. The portrayal of sanctions as a major hindrance for controlling COVID-19 was also echoed amongst Zimbabwe’s long-standing geopolitical allies that have similar grievances against Western countries such as Iran, Cuba and Venezuela.65 66 This underscores that an effective epidemic response in Zimbabwe should not only emphasise the biomedical aspects while viewing history, power and politics as encumbrances. Instead, a pragmatic approach that strategically endeavours to accommodate biomedical science within the realities of local context while seeking to capitalise the productive use of political power is required.
Fourth, this study illustrates the nexus between sovereignty and securitisation does not always breed sovereign and disciplinary powers, but can also mobilise productive power (biopower). Zimbabwe’s protracted shaky relationship with Western countries could have motivated a sense of self-reliance and ambivalence towards donor funding, which led the country to embark on a domestically financed vaccination programme based on similar fears that inspired the creation of the national AIDS Trust Fund in the early 2000s.67 Zimbabwe’s sceptical position towards heavy donor reliance could have been vindicated. The COVAX mechanism—which majority of developing countries relied on to access the COVID-19 vaccine—was severely undermined by ‘vaccine nationalism’ by richer countries68 which reinforced the underlying enduring legacy of ‘imperialism’ and ‘colonization’69 70 while exposing the dangers of Western dependency.71
Fifth, this study demonstrates that despite biopower’s positive influence over the social body, it does not render sovereign and disciplinary powers redundant.72 As shown through Foucault’s prism, the pursuit of biopolitical objectives in Zimbabwe such as achieving herd immunity through vaccination still relied on sovereign and disciplinary power mechanisms. Vested geopolitical interests in relation to the vaccination programme also cast elements of dark power. For example, in September 2021, the government rejected a donation of 3 million doses of the Johnson & Johnson vaccine (UK-manufactured vaccine) from the African Union, a move that was criticised as a sovereign posture reflective of the Harare-London diplomatic tiff.73 74 This demonstrates that in relation to the COVID-19 response in Zimbabwe, sovereign, disciplinary and biopower mechanisms acted as complementary instruments in the administration of populations.72 Since biopower is ‘pastoral’, in the sense that it seems positive and constructive, it even might feel like love and care,6 the overlap in these power mechanisms requres careful monitoring. Of particular importance is the need to guard against the manipulation of ‘pastoral responsibilities’—presented as the authorities’ extra concern for protecting public healthas a way of justifying excessive application of sovereign and disciplinary power.’
Finally, this study points out that while there is much preoccupation with visible power that openly manifests as coercive and non-coercive actions towards epidemic control in Zimbabwe, invisible mechanisms involving thought control can make power more efficient and insidious.75 Instead of solely relying on physical surveillance, the criminalisation of misinformation fostered a more disciplined society by co-opting surveillance mechanisms that aligned with Foucault’s concept of panopticism.41 Panopticism improves the efficiency of power mechanisms as individuals develop a conscious state of being permanently watched, thus become more disciplined through practices of self-surveillance,76 even if the watcher is not there or their presence is unverifiable. Thus, a more insightful approach to power analysis should focus on power as decision-making, and how power can make citizens acquiesce with given policies, even if such policies are not in their own interests.
While the six points above portray power as a resource, this study also carries important conceptual implications in relation to one of Foucault’s recurrent assertions that the exercise of power depends on the scaffold of knowledge supporting it.6 Thus, all the mechanisms of power, whether dominated by the dark side of power such as sovereign and disciplinary powers or driven by the productive side of power, such as biopower, were shaped by claims to epidemiological knowledge. While the early response was mediated by fear that induced dominantly sovereign and disciplinary mechanisms of power aimed at eradicating the pathogen or ‘destroying the enemy’, the rapid evolution in scientific knowledge shifted the pandemic view from a catastrophe to an endemic illness that could be controlled by using a combination of strategies or ‘learning to live with the virus’.77 This signified a shift towards biopower mechanisms, where there is abandonment of the idea of complete eradication of the pathogens in favour of curbing the epidemic.15
A holistic approach to biopower through the lens of knowledge or truth also helps to understand the public’s negative reaction or violation of COVID-19 regulations, akin to what Foucault terms resistance to power.6 Rabinow and Rose78 claim that biopower must include three elements: truth discourses (in this case the severity of COVID-19), specific strategies (measures to control the disease) and conditions that facilitate individuals to act according to the truth discourse (conditions that facilitate compliance with the COVID-19 regulations). Invoking this holistic approach to biopower points out that the government of Zimbabwe emphasised claims to the truth and the related strategies without paying attention to conditions of subjectification. In a country plagued with high unemployment rate, heavy reliance on informal incomes and skyrocketing inflation, a hard lockdown without an effective cushioning system forced the majority of population to make ‘choices between being hungry and risk of getting infected’79 or in biopower terms a trade-off between truth and subjectification. This contradiction carried practical implications among Zimbabwe’s regional neighbours. For example, in Malawi, the announcement of a lockdown incited public protests against anticipated disruption of livelihoods, leading the high court to issue a court injunction to block the move unless the government intervened with welfare subsidisation.80 Therefore, what was viewed as wanton violation of COVID-19 regulations in Zimbabwe—or resistance to power—was in biopower terms a rational choice by citizens to reconcile the truth and the subjectification.
Strengths and limitations of the study
This study has limitations and strengths worth highlighting. In terms of the limitations, first, this study majorly investigated the role of formal power—hidden and unhidden—in shaping the COVID-19 response. For a response that invoked wider governmentality issues, the role of informal power needs to be further investigated. Second, due to methodological fidelity to biopower, we did not explore the effects of the COVID-19 response on the general health system governance. This is also an area that requires further research. Despite these limitations, this paper has strengths that are worth noting. First, to the best of our knowledge, this is one of the very few papers that examined the COVID-19 response using theoretically grounded concepts of power relevant to epidemic governance in the Zimbabwean context, departing from the dominant biomedical emphasis and the non-application of relevant theory to explain the COVID-19 response dynamics. Second, this paper examined the COVID-19 response within the full spectrum of Foucault’s theoretical differentiation of the historical evolution of epidemic governmentality which enriches the existing body of knowledge that focused on isolated aspects of Foucault’s theory.
Conclusion
The COVID-19 response in Zimbabwe aligned with Foucault’s theoretical differentiation of the political management of emerging epidemics, ranging from a host of censoring and prohibitive laws typical of sovereign power, to the imposition of heavily monitored and protracted lockdown accompanied with severe penalties for violations, typical of disciplinary power, to the reliance on statistics and models of response aimed at controlling rather than curbing the pandemic, including vaccination, typical of biopower. Securitisation of the pandemic was filtered through the lens of sovereignty, geo (politics) and war ideology, resulting in a dominantly plague-based model (disciplinary power) that overshadowed the positives of biopower. This underscores that when securitisation is invoked at global level, its intersection with prevailing ideology needs to be monitored as it diffuses to country level, since the literal activation of such charged frames may serve to undermine their intended purposes. However, power was not only used negatively, instead the sovereignty- securitisation nexus shaped a generally well-executed domestically funded vaccination (biopower) programme. This underscores that power is not something that needs to be criticised or avoided per se, instead effort should be directed at investigating what forms of power are at work in different situations and how it can be productively used to influence policies.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Stephanie M Topp
Contributors ATM and CCM codesigned the manuscript. ATM led the conduct and analyses of the manuscript and drafted the initial version of the manuscript. Both authors made a substantial contribution to the structure and content of the manuscript. ATM is the guarantor responsible for the overall contents of this paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.