Article Text

Statistics from Altmetric.com
Global health has gained increased attention as a concept and academic discipline in recent years.1 The COVID-19 pandemic has highlighted the world’s interconnectedness and how public health threats are no longer the concerns of single nation-states, regions or discrete sectors. The war in Ukraine has further exemplified the fragility and complexity of global markets and its implications for food security and the well-being of millions far away from the actual conflict. The realisation that ‘we are all in this together’ is gaining momentum and is further exacerbated by extreme weather events, the looming energy crisis and brewing political unrest, all mediated by a global news industry at an ever-increasing pace. The need for transformation has never been greater and global health has the systemic potential to be an explanatory, investigative and constructive entity. Global health is, however, a contested term. Originating in tropical medicine and later in international health, it has colonial baggage that needs to be acknowledged and dealt with. Calls for ‘decolonising global health’ have been voiced.2 At the same time, old structures prevail and are reproduced.2 This is troublesome since the colonial narrative lingers on and thereby hampers the potential for global health to contribute to addressing the challenges it is fit for.
In an attempt to adapt to a changing world, global health is struggling to redefine itself. Global health is searching for a meaningful and easily communicated definition to distinguish itself from colonial history and the heritage of a bipolar world with ‘developed’ and ‘developing’ countries; a definition that stresses the global nature and the rapidly changing landscape of humanity’s health challenges. In a seminal paper, Koplan et al had crafted a definition of global health that had gained widespread acceptance. They consider global health to be a vehicle for (1) tackling transnational health threats like pandemics, antibiotic resistance and climate change and (2) focusing on health equity. This definition has merit and has been widely used.3 There is, however, built-in inertia in the redefinition of an already established field, and the perception of global health as a brushed-up version of international health has prevented the definition by Koplan et al from gaining full traction. This can, for example, be seen in a continued discourse of ‘global south’ and ‘global north’,4 in educational programmes where students hope to learn about how things are ‘over there’5 and the plethora of Western non-governmental organisations reproducing the narrative of ‘us and them’.6 The late Hans Rosling’s primary mission was to support the realisation that our perceptions of the world are outdated and that we need to embrace facts rather than past beliefs about how the world functions. Even if there is a shift towards a more global understanding, as advocated by Rosling and fast-tracked by the COVID-19 pandemic, the area of global health is still very much operating within an obsolete understanding of the world.
Furthermore, though there is merit to Koplan et al’s definition of global health, some shortcomings have become more and more pressing in a rapidly changing world. The most striking omission is the lack of a sustainability perspective. Even if it is becoming increasingly evident that the state of the world we live in is putting both constraints and posing challenges to human health, global health is more often than not limited to a public health perspective by focusing on the more direct aetiologies of ill health. The social determinants of health are used as explanatory factors rather than the object of intervention for global health practitioners and researchers when trying to avert or mitigate the transnational health challenges the definition speaks of. Thus, global health limits itself to being reactive rather than proactive, confined within a narrow perception of health rather than encouraging transdisciplinary, multistakeholder interaction. Similarly, sustainability, as narrated within the Sustainable Development Goals (SDGs), depicts health as one of 17 goals,7 fencing global health in a box among many and thereby delimiting its operating space. Even if WHO is trying to redefine the SDG agenda and acknowledge ‘health in all policies’, it is an uphill battle. Despite the implicit assumption that all efforts towards a sustainable future are to secure the survival and thriving of humankind rather than nature or the ecosystems of the planet, global health, under the current definition, becomes compartmentalised and limited to the sphere of epidemiology and preventive medicine.
The other leg of Koplan et al’s definition of global health is also problematic. The field of health equity has developed from Margret Whitehead’s scholarship on the proximal determinants of health8 to a deepened perspective of the ‘causes of the causes’, as outlined in the report from the Commission on Social Determinants of Health (CSDH).9 The report, first released in 2008, is still essentially a guiding document for understanding what creates and reproduces inequity in health outcomes. Koplan et al’s definition of global health was contemporary with the CSDH report and is very much influenced by its perspectives. This led to a one-sided focus on inequity, limiting global health to a discipline that tries to explore drivers of unjust health outcomes.
The good intentions of international health, promoting health for the disadvantaged, improving livelihoods and securing good health were somehow made invisible in Koplan et al’s definition. Although health equity implies that the highest attainable health is the goal for everyone, it often gets lost in a discourse that attempts to primarily reduce differences rather than focus on raising the overall level of health. This might be one reason for the slow transition from international to global health. Many global health practitioners are driven by a willingness to do good rather than challenging existing societal structures. Results and concrete problem-solving better fit the image of a global health worker rather than the political engagement needed to address the causes of the causes. However, global health needs to include both perspectives and emphasise ‘health for all’ rather than only reducing inequities.
Research initiatives that focus on maintaining and reproducing societal structures are often found in other disciplines. Global health’s potential to drive transformation is constrained by the absence of a sustainability perspective that transcends human public health and the inability to operate at a structural level to promote justice. In a worst-case interpretation, the discipline is made redundant and insignificant rather than the forerunner it ought to be. Instead, it risks becoming the guardian of the structures it claims to be challenging. A new narrative and self-image are needed for global health to incorporate, acknowledge, and address the political and societal dimensions not traditionally associated with medicine and public health. A narrative that redefines health to also include the biosphere and challenges the terms ‘global’ and ‘public’ to go beyond geography and anthropocentrism.10
One such narrative gaining traction is the dual challenge of improving health for all while staying within planetary boundaries.11 The so-called ‘sustainability quadrant’, the space where health equity and ecological sustainability meet and apply simultaneously,12 is receiving more and more attention (figure 1). This approach has merit by introducing the concept of planetary boundaries and linking it to human development and health. We argue that this must be a self-evident and integral part of all global health conceptualisation, just as the mainstream discourse on sustainability must consider health and well-being for all humans.13 14 It also connects well with ideas within the sustainability discourse that focus on both ecological and social dimensions of sustainability, such as the ‘sustainability doughnut’15 or the three domains of sustainability that also focus on the economic and/or political dimension.16 A further advantage of the sustainability quadrant is its challenge to the colonial heritage of global health, incorporating the need to address the ecological footprint within the rich countries within the realm of global health. This could help dissolve the notion of global health being only about proximal determinants of health in resource-poor settings. Furthermore, it extends the idea of health to also encompass societal and planetary health (figure 2).
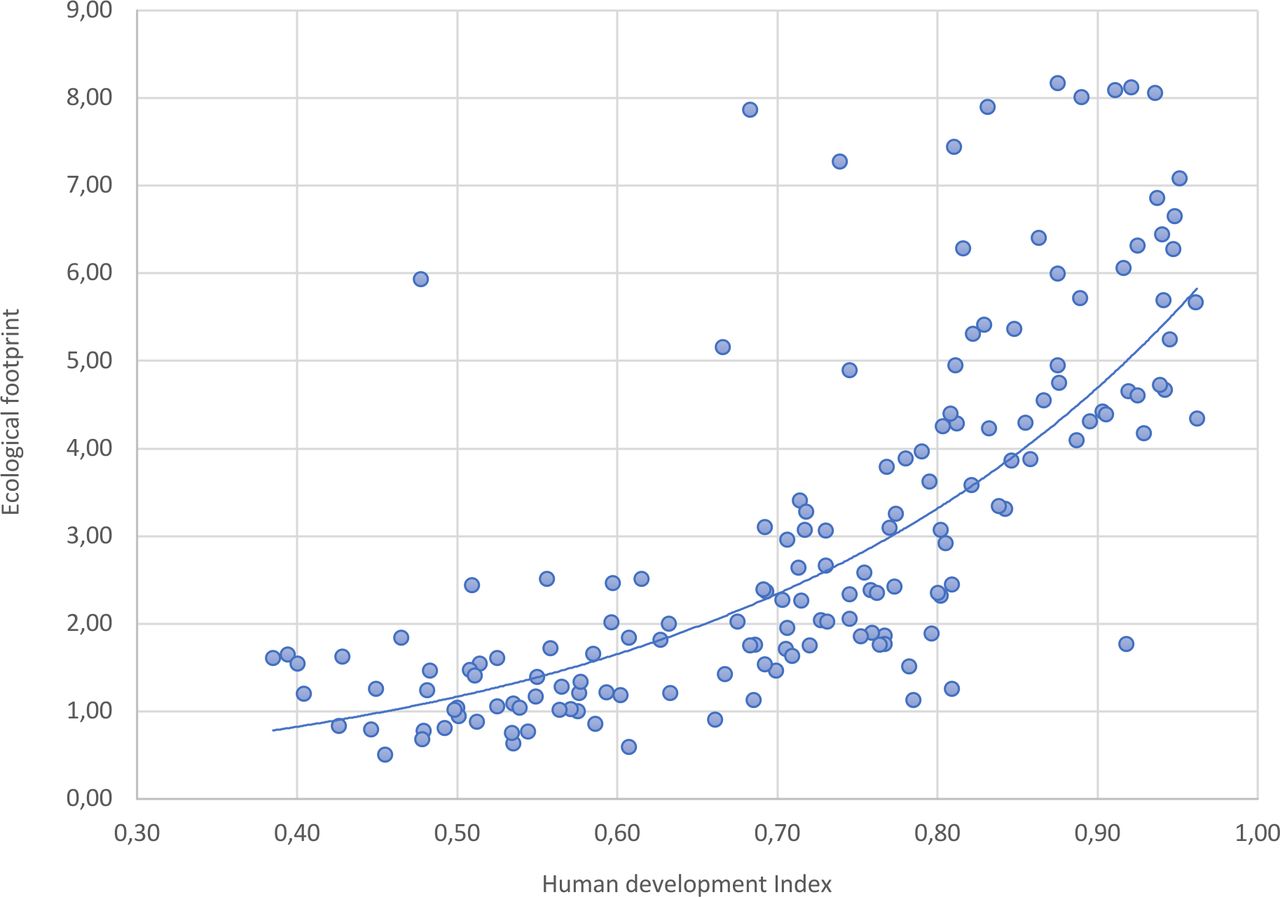
Human Development Index (2021)* and Ecological footprint (2018)** for 158 countries. Sources: (https://data.footprintnetwork.org/; https://hdr.undp.org/data-center). *Human Development Index “is a summary measure for assessing long-term progression of the three basic dimensions of human development: a long and health life, access to knowledge and a decent standard of living.” **Ecological footprint is defined as “a measure of how much area of biologically productive land and water an individual, population, or activity requires to produce all the resources it consumes and to absorb the waste it generates, using prevailing technology and resource management practices.”

{kind=link}
{kind=link}
. Conceptualization of different levels of health adapted from Bronfenbrenner, Urie (1989). "Ecological systems theory". In Vasta, Ross (ed.). Annals of Child Development: Vol. 6. London, UK: Jessica Kingsley Publishers. pp. 187–249.
But redefining the topic focus is not sufficient. A new narrative for global health also needs to include a shift from solely counting and concentrating on the outcome to more emphasis on the process, both as a research interest and an identity. Implementation science within global health has been established as a discipline of its own over the past decades.17 Derived in the notion that we do not use all the knowledge we have and that there is a gap between clinical evidence and practice (the know-do gap),18 it has become a field that studies implementation strategies and innovations that could extend far beyond the scope of health systems research. As an increasingly acknowledged part of today’s global health, implementation science can provide a foundation for the new narrative. Because if we define the topic of global health as the pursuit of the sustainability quadrant, the process of getting there becomes the most critical aspect. Within this context, we are, however, dealing with wicked problems—inherently unsolvable problems characterised by irreconcilable conflicts of interests, while at the same time being essential to the survival or functioning of a given system.19 Wicked problems cannot be solved within the same system, only navigated. To reach the sustainability quadrant is for global health a wicked problem. All the gains in health indicators, the rise in living standards and the fulfilment of human potential are made possible through the exploitation of finite natural resources. If we at all can maintain trustworthiness in our efforts to achieve global health, we need to acknowledge the need for transformation.
Global health needs to regain and widen the vision of a different and better world and further emphasise that business as usual is not accepted nor viable. To conclude, there is an urgent need for global health to embrace a new narrative, to define a focus and direction that moves beyond its colonial heritage and narrow perception of health as a human entity only. This new narrative can be expressed as health, sustainability and transformation.
Data availability statement
Data is available at https://data.footprintnetwork.org/; https://hdr.undp.org/data-center.
Ethics statements
Patient consent for publication
Footnotes
Handling editor Seye Abimbola
Twitter @matsmalqvist
Contributors MM conceptualise the paper and both authors jointly wrote the piece.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.