Article Text

Abstract
Introduction We comprehensively evaluate whether the Chinese Government’s goal of ensuring Universal Health Coverage for essential health services has been achieved.
Methods We used data from the 2008, 2013 and 2018 National Health Services Survey to report on the coverage of a range of Sustainable Development Goals (SDG) indicator 3.8.1. We created per capita household income deciles for urban and rural samples separately. We report time trends in coverage and the slope index (SII) and relative index (RII).
Results Despite much lower levels of income and education, rural populations made as much progress as their urban counterparts for most interventions. Coverage of maternal and child health interventions increased substantially in urban and rural areas, with decreasing rich-poor inequalities except for antenatal care. In rural China, one-fifth women could not access 5 or more antenatal visits. Coverage of 8 or more visits were 34% and 68%, respectively in decile D1 (the poorest) and decile D10 (the richest) (SII 35% (95% CI 22% to 48%)). More than 90% households had access to clean water, but basic sanitation was poor for rural households and the urban poorest, presenting bottom inequality. Effective coverage for non-communicable diseases was low. Medication for hypertension and diabetes were relatively high (>70%). But adequate management, counting in preventive interventions, were much lower and decreased overtime, although inequalities were small in size. Screening of cervical and breast cancer was low in both urban and rural areas, seeing no progress overtime. Cervical cancer screening was only 29% (urban) and 24% (rural) in 2018, presenting persisted top inequalities (SII 25% urban, 14% rural).
Conclusion China has made commendable progress in protecting the poorest for basic care. However, the ‘leaving no one behind’ agenda needs a strategy targeting the entire population rather than only the poorest. Blunt investing in primary healthcare facilities seems neither effective nor efficient.
- health systems evaluation
- public health
- cross-sectional survey
- health policy
Data availability statement
Data may be obtained from a third party and are not publicly available. Please contact YZ, Centre for Health Statistics and Information, National Health Commission of China (email: zhangyg@nhc.gov.cn).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In China, two system-level efforts, scaled up in 2009, have been made towards achieving universal health coverage (UHC).
Half of the government health spending was made to expanding social health insurance for curative care in hospitals; while the other quarter of funds were allocated to primary healthcare (PHC) facilities for capacity building, and to finance the National Essential Public Health Programme, providing free preventive services.
Prior studies tracking China’s progress to UHC focused on hospital-based care and financial risk protection.
Research is lacking to assess China’s recent progress to UHC within the Sustainable Development Goals (SDG) 3.8.1 framework, particularly for preventive services and among the most vulnerable.
WHAT THIS STUDY ADDS
We incorporate recent developments in the measurement of health coverage among the most vulnerable populations to report on China’s national trends on the coverage and equity of specific health services.
Coverage of maternal and child health interventions increased in both urban and rural China, but rich-poor inequalities in antenatal care persisted in the rural areas.
Coverage of preventive services are much lower for non-communicable diseases, including management of hypertension, diabetes and screening for cervical and breast cancer.
Despite much lower levels of income and education in rural areas, rural populations made as much progress as their urban counterparts for most interventions, except for coverage of antenatal care and sanitation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We found little evidence of bottom inequality in both urban and rural areas, suggesting that the ‘“leaving no one behind’” agenda needs a strategy targeting the entire population rather than only the poorest.
We highlighted that uptake of preventive services—which were free at the point of use in PHC facilities—were poor in China, questioning success of the government decade’s effort in extending essential health services by investing in PHC facilities.
We draw lessons whether PHC services must be delivered via PHC facilities, to better achieve SDG 3.8.1.
Introduction
Ensuring universal health coverage (UHC) is fundamental to achieving the Sustainable Development Goals (SDG). UHC implies that everyone has access to essential health services without experiencing financial hardship resulting from healthcare payment.1 Two indicators have been adopted by the UN Statistical Commission1 2 to monitor progress to UHC: coverage of essential health services (SDG indicator 3.8.1) and the proportion of households with expenditures on health that represent a large share of total household consumption or income (SDG indicator 3.8.2). SDG indicator 3.8.1. requires the identification of tracer interventions among the general and the most disadvantaged populations that represent a range of essential services including reproductive, maternal, newborn and child health, infectious diseases, non-communicable diseases and service capacity and access. SDG indicator 3.8.2. captures the ability of populations to access quality healthcare without financial hardship. Global analyses suggest that while major progress has been made in the coverage of SDG interventions, many countries are still a long way from UHC, where compelling evidence shows that coverage gap in the poorest population is a primary cause for concern.2–5 The motto of ‘leaving no one behind’ has thus been called for progress to equity, suggesting more attention to the vulnerable population that may be especially lack of coverage.3
In China, substantial efforts have been made towards achieving UHC. Alongside continuing investments in primary education and poverty alleviation in rural areas, two system-level efforts, scaled up in 2009, have been particularly important.6 7 First, the Government invested half of the budget in expanding social health insurance for curative care in hospitals as a means to mitigate barriers to hospital admissions and catastrophic health spending.8 Second, the other quarter of funds were allocated9 to strengthen infrastructure and human resource capacity of primary healthcare facilities, and to finance the National Essential Public Health Programme in urban community health centres and rural township hospitals. This programme offers 12 essential public health services to all urban and rural citizens, with funding from ear marked central budgets, which increased from US$2.2 to $US8.7 per capita between 2009 and 2018. Free services include health propaganda and education, maternal and child healthcare (five basic antenatal visits, management of birth in health facilities, child immunisation and growth monitoring) and screening and management of hypertension and diabetes (periodical condition monitoring and consultations). Additional efforts were made to provide screening for breast and cervical cancer to rural women.10
Two comprehensive analyses were made to track China’s progress to UHC,6 7 focusing on insurance coverage, access to hospital-based outpatient and inpatient care and financial risk protection. Using the National Health Services Survey (NHSS), Meng et al7 reported that insurance coverage reached 96% in 2011, hospital admissions more than doubled in 2003–2011, when rich-poor inequalities vanished. Yip et al updated the analysis, with survey data from China’s Family Panel Studies, reported that hospital admission rates increased to 13.5% in 2016, without aggravating households’ financial hardship.6 However, these trends are difficult to interpret for monitoring essential health services coverage, since increases in overall utilisation may not represent health needs. As recent national data, focusing on multimorbidity and cardiovascular diseases, respectively, have otherwise revealed persistent inequalities in healthcare use that favour the urban population and wealthier groups.11 12 In addition, trends in the coverage of specific health interventions are less well documented, particularly in recent years and among the most vulnerable. We found no report that comprehensively assesses China’s recent progress to UHC within the SDG 3.8.1 framework. Data are particularly lacking for the preventive interventions delivered within the National Essential Public Health Programme.
In this paper, we use data from three nationally representative surveys from the NHSS, with new data from 2018, to evaluate whether the Chinese Government’s stated goal of ensuring UHC for essential health services has been achieved. We incorporate recent developments in the measurement of the coverage of essential health services among the most vulnerable populations. We report on the coverage of specific health services across a range of tracer indicators, as suggested by Hogan et al.2 We measure income deciles rather than the usual quintiles. As suggested by Barros et al,3 this approach commonly help to identify the poorest poor that lag behind, that is, bottom inequality, and the richest rich that are way ahead, that is, top inequality. To better examine patterns of inequality, we separate income groups within urban and rural areas. Showing the poor performance for indicators within the National Essential Public Health Programme, we draw lessons, for both China and other countries with similar context, that blunt investment to primary healthcare may not fit the UHC agenda.
Methods
Data and indicators
We used data from the 2008, 2013 and 2018 NHSS, which sampled households in all 31 provinces of mainland China stratified by urban/rural and geographic regions. Detailed survey methods have been described by Meng et al.7 We measured indicators representing the coverage of essential health services, adapting a global set of indicators1 2 4 to the context of China (table 1). We did not measure family planning with modern methods or immunisation coverage in infants—two indicators deemed important for UHC—because recent national surveys did not report these data. For maternal health, we measured the per cent of births in a health facility and the per cent of births with five or more and eight or more antenatal visits in accordance with China’s national and WHO’s recent guidelines.10–13 For infectious diseases, we measured household access to basic sanitation and clean drinking water using international standards.14 We also assessed care seeking for children with acute respiratory tract infections (ARI) and diarrhoea in the last 2 weeks.15 For non-communicable diseases, we measured access to treatment and adequate management for hypertension and diabetes, as well as screening for cervical cancer and breast cancer, using China’s national guidelines.10 For example, adequate management of hypertension refers to receiving of the four key preventive and curative interventions, including health check-up, health education and regular blood pressure monitoring, and taking antihypertensive medicines. A detailed description of each indicator is shown in table 1.
Universal health coverage tracer indicators to monitor progress on health service coverage
Statistical analysis
We created per capita household income deciles for urban and rural samples separately, within each survey. We linked household data to individual data to assess service coverage across each income decile. The survey reported very low prevalence of diarrhoea (489 out of 48 347 children), so we used quintiles rather than deciles of household income to assess service coverage for the treatment of diarrhoea in children.
To contextualise the changing inequalities in service coverage over time, we first examine changes over time in household income (adjusting per capita income to the monetary value of the year 2018 using consumer price indices) and women’s education in each of the three NHSS survey rounds. We then report all coverage indicators by income decile within urban and rural areas, assessing the magnitude of income inequalities and scrutinising the coverage patterns across deciles for evidence of bottom or top inequality, following the recommendations made by Barros and Victora.16 Absolute inequalities were measured by absolute differences between the 10th (D10) and the first decile (D1), and the composite index of the slope index of inequality (SII). Relative inequalities were measured by the ratio between D10 and D1, and the composite index of the relative index of inequality (RII). The SII and RII, are estimated by performing a logistic regression for each coverage indicator, respectively, on a variable ranking each subject by their income level as a continuous variable, and fitting the difference or ratio between the fitted values of 1 and 0 for the rank variable.17 We used logistic regression to follow routine by Barros and Victora.16 By including data from all income groups rather than just D1 and D10, the composite inequality indices SII and RII are considered to be better able to measure the inequality patterns across the whole population.16 We additionally assessed trends over time using a Poisson regression with robust SEs, and used the Wald test to test linear trends for each indicator over time, using the overall sample and within D1, D5 and D10, respectively. We used Poisson regression because many outcomes are common.18 We weighed the data against the probability that an individual would be included in the sample to obtain nationally representative estimations.19
Patient and public involvement
The public were involved in the pilot surveys that designed and adjusted the questionnaires. Aggregated statistics were released to the public in the form of government report, but all individual information were hidden.
Results
The sample size was large for each indicator and there were few missing data (online supplemental appendix table 1). There were substantial changes in household income over time in the NHSS (figure 1A). The median per capita income increased from ¥12 455 to ¥20 000 between 2008 and 2018 in urban areas, and from ¥4982 to ¥10 000 in rural areas, with almost no change between 2013 and 2018. Similarly, important changes were seen for education of women (figure 1B). Mother’s education was much higher in urban than in rural areas, with 53.5% and 22.0%, respectively having secondary or higher education in 2018. Per capita household income varied greatly across urban/rural areas (in 2018 median ¥20 000 urban, ¥10 000 rural), and the values for D1, D5 and D10 differ greatly in both urban and rural areas, for each survey, respectively. For example, the poorest D1 were those with an income of <¥5833 in the urban areas in 2018, compared with <¥2500 in rural areas (online supplemental appendix table 2).
Supplemental material
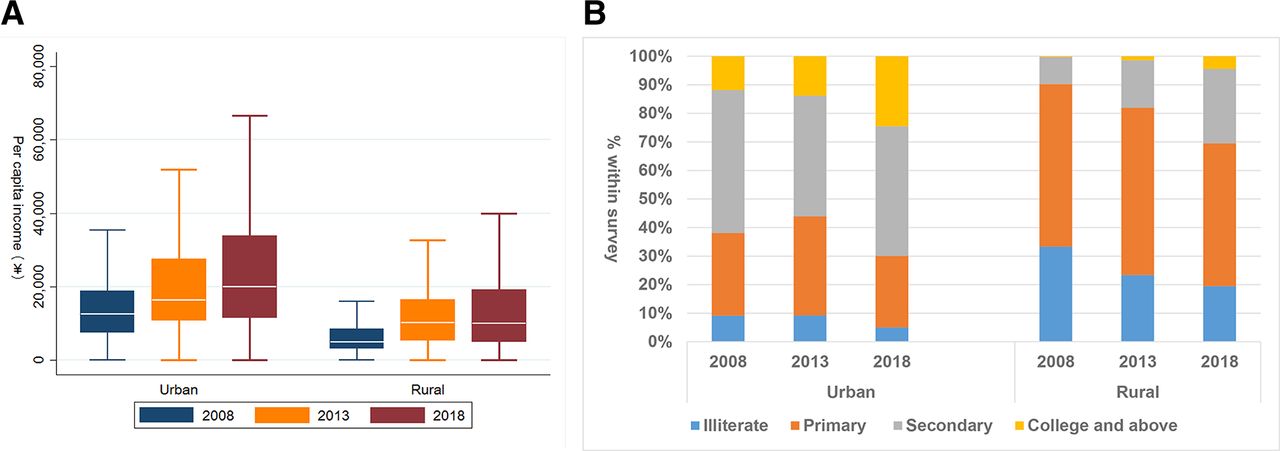
Changes in the distribution of household per capita income and women’s education in 2008, 2013 and 2018, in urban and rural China (income adjusted for consumer price indices, to values of the year 2018). (A) Changes in per capita income among households; (B) changes in education among women with a recent live birth.
Trends in the coverage of maternal health indicators are shown in figure 2 and table 2. Facility births increased dramatically in all income groups, achieving near universal coverage in both urban and rural China by 2018. Antenatal care coverage started at lower levels, but saw similar increases across all income deciles, in both urban and rural China. In urban China, there was some evidence of bottom inequality for coverage of antenatal care, but this reduced substantially over time. For example, in 2008, 22% of decile D1 (the poorest) and 76% of decile D10 (the richest) urban women had received eight or more antenatal visits (SII 61% (95% CI 43% to 78%)). By 2018, coverage increased to 64% and 89% among decile D1 and D10, respectively (SII 25% (95% CI 17% to 33%)). In rural China, shrinking inequalities were also seen in the coverage of five or more antenatal visits. However, there were rising top inequalities in coverage of eight or more antenatal visits over time. For example, the coverage of eight or more visits was 6% and 37% in D1 and D10, respectively in 2008 (SII 20% (95% CI 6% to 35%)), and increased to 34% and 68% in D1 and D10, respectively in 2018 (SII 35% (95% CI 22% to 48%)).
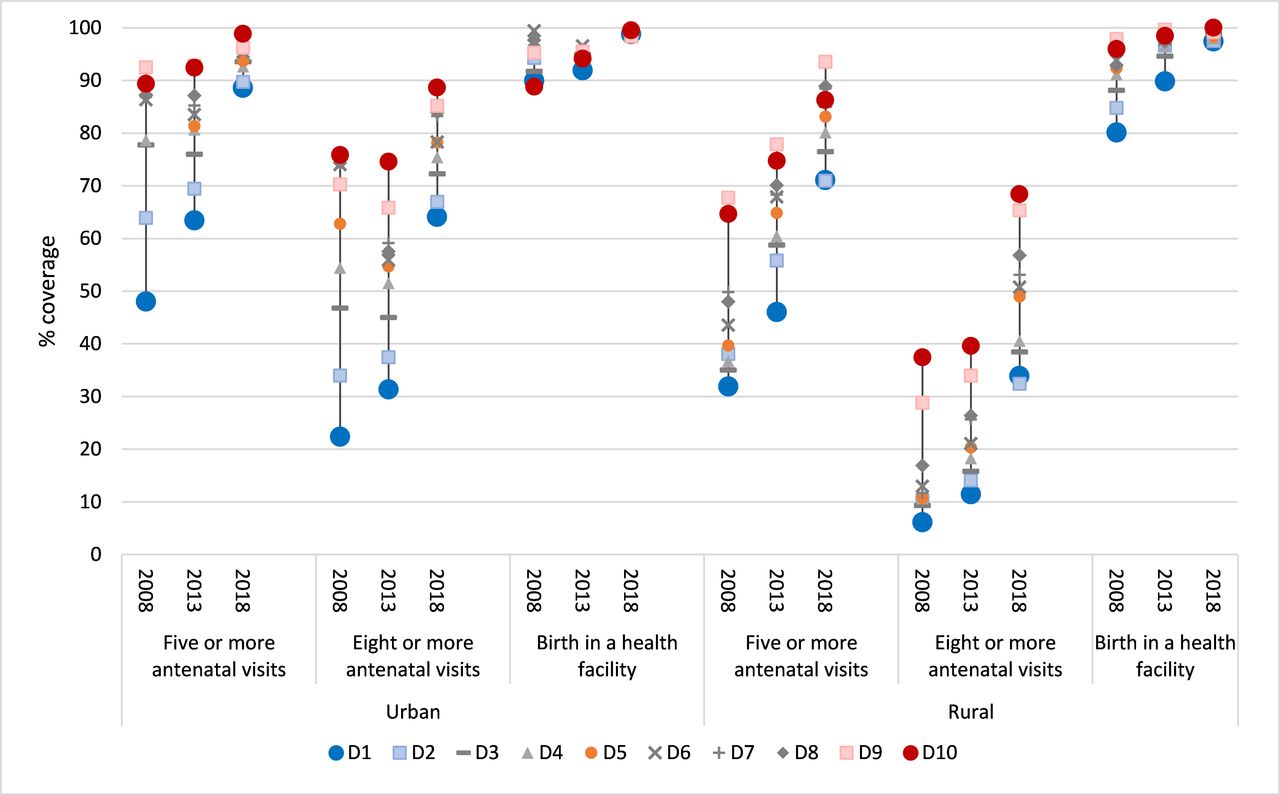
Service coverage for maternal health indicators in urban and rural areas, by year of survey and income decile.
Service coverage for maternal health indicators in urban and rural areas, by year of survey and income decile (income adjusted for consumer price indices, to values of the year 2018)
Access to clean water was high for all income groups, and nearly universal for urban households by 2018 (figure 3 and table 3). However, access to sanitation decreased over time for the urban poorest, with persistent bottom inequality as a result (SII in 2018 24% (95% CI 18% to 30%)). Access to sanitation was lower for rural households, with rising absolute inequalities over time (SII 26% (95% CI 15% to 38%) in 2008, 33% (95% CI 25% to 41%) in 2018). Coverage for treatment of ARI and diarrhoea was high and stable over time, without clear evidence of income-related inequalities. Inequality patterns for diarrhoea treatment were inconsistent due to the low numbers (only 160 cases out of 18 267 children in 2018).

Service coverage for infectious disease indicators in urban and rural areas, by year of survey and income decile. *Among the 11 402, 18 678 and 18 267 children under 5 years of age, the National Health Services Survey investigated 234 (2.1%), 95 (0.5%) and 160 (8.8 %) diarrhoea cases, in the 2008, 2013 and 2018 survey, respectively. Quintiles (Q1, Q3, Q5) were used in analysing equity in diarrhoea treatment because of the small sample size.
Service coverage for infectious diseases indicators in urban and rural areas, by year of survey and income decile (income adjusted for consumer price indices, to values of the year 2018)
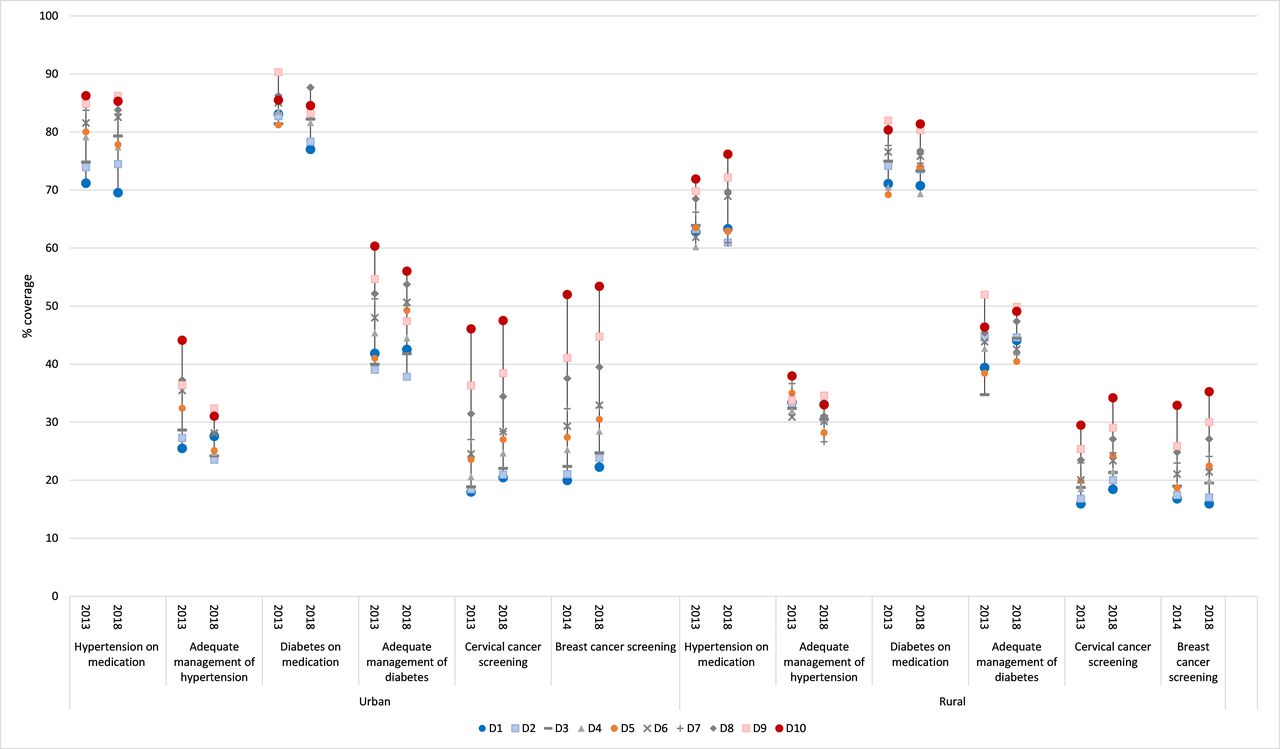
More than 80% of urban adults and around 70% of rural adults with hypertension or diabetes reported to be on medication, with no change between 2013 and 2018 (figure 4 and table 4). Income-related inequalities in medication for hypertension or diabetes persisted in both urban and rural China. For example, in 2018 the SII for hypertension on medication was 16% (95% CI 11% to 22%) and 13% (95% CI 3% to 22%) in urban and rural areas, respectively. When applying the full guideline criteria for adequate management of hypertension or diabetes that count in preventive interventions, coverage was much lower than for simple medication and decreased over time, although income inequalities were small in size and shrinking overtime. For example, coverage for the adequate management of hypertension decreased from 34% to 28% in urban areas, and from 34% to 31% in rural areas, respectively, with the SII in 2018 decreasing to 8% (95% CI 1% to 16%) in urban areas and 1% (95% CI −8% to 9%) in rural areas, respectively. Coverage for the screening of cervical cancer and breast cancer was low in both urban and rural areas, without much improvement during 2013–2018. Notably, coverage of cervical cancer screening was only 29% and 24% in 2018, in urban and rural China, respectively. For screening interventions for the two cancers, a clear pattern of top inequality persisted, particularly in urban areas (SII for cervical cancer screening in 2018 25% (95% CI 18% to 32%) in urban areas, in respect to 14% (95% CI 9% to 19%) in rural areas).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Service coverage for non-communicable disease indicators in urban and rural areas, by year of survey and income decile.
Service coverage for non-communicable diseases indicators in urban and rural areas, by year of survey and income decile (income adjusted for consumer price indices, to values of the year 2018)
Discussion
Using data from three nationally representative surveys between 2008 and 2018, we provided a comprehensive assessment of whether China achieved its goal of providing all citizens with equal access to essential health services. We found that the coverage of maternal and child health interventions had increased substantially in both urban and rural areas. However, coverage of health interventions for non-communicable diseases was generally low, with little progress over time. Adequate management of hypertension and diabetes was poor and top inequalities persisted in the screening of both cervical and breast cancer. Access to clean water was good, but access to basic sanitation decreased among the urban poor and rich-poor inequalities in sanitation increased in rural areas. Despite much lower levels of income and education in rural areas, rural populations made as much progress as their urban counterparts for most interventions, except for coverage of antenatal care and sanitation.
The achievements in maternal and child healthcare are consistent with findings from other studies, and a testament to China’s longstanding commitment to maternal and child health.20 21 Maternal and child mortality are low in most parts of the country.22 23 There is little doubt that the multisectoral approach that promoted facility-based birth, particularly efforts in improving women’s education and awareness, investment in comprehensive emergency obstetric care and promotion of universal health insurance have been critical to this success.20 21 The remaining challenge now is in equity and adequate use of antenatal care in rural areas. While the inequitable coverage may still be mainly influenced by economic factors, recent data from remote rural China suggest that varied investment through regional government may explain the difference.24 In addition, rural women may not trust the free antenatal services offered by the township hospitals, with evidence emerging that the rural poor are particularly vulnerable to poor quality care.21 Despite the direct subsidy to primary care facilities, there is however remarkably little information on the use of or quality of care in township hospitals. Use of ultrasound scans is common, but other valuable interventions may be lacking.24 25 There is a need to integrate more cost-effective interventions, for example, screening of infectious diseases and congenital anomalies, into routine antenatal programmes.20 26
Prevalence of hypertension and diabetes are on the rise in China.27 28 In the NHSS, the reported prevalence of hypertension and diabetes in adults aged 35 years or older increased from 12% to 23% and from 5% to 7%, respectively between 2008 and 2018 (data not shown), getting closer to epidemiological studies based on anthropometric measures and laboratory tests.27 28 Of the patients with hypertension in 2018, 78% of urban residents and 65% of rural residents were on medication, which is higher than previously reported.27 Similarly, our estimates of the coverage of treatment for diabetes was much higher than previous estimates.28 However, we found that adequate condition management, counting the continuum of three types of preventive interventions, was very low for both hypertension and diabetes, irrespective of where people live and how much they earn. Within the National Essential Public Health Programme, community health centres and township hospitals are tasked to proactively free preventive services of screening, condition monitoring and follow-up, including health education and consultation, to patient with hypertension or diabetes in their catchment area. However, these primary healthcare facilities have being challenged by the lack of qualified workforce and service capacity, with patients trust and perceived quality of care being much lower than general hospitals’ outpatient services.29 In addition, costs of medical consultations and medicines are covered by health insurances, offering patients free choices to seek care from any health facility for the prescription of medicine. Evidence are emerging that the National Essential Public Health Programme may help identify more patients with hypertension and/or diabetes, but who may eventually seek treatment from county or higher level hospitals—paying from their own pocket or through health insurance, without accessing the free follow-up care in community centres or township hospitals.30
The low coverage of cervical cancer screening between 2013 and 2018 are substantially lagging behind WHO’s objective of 70% towards 2030.31 Coverage level are very close to that from other sources of national surveys conducted in 2010 and 2014,20 suggesting that no progress had been made to extend coverage in the past 10 years. In addition, we found that rich-poor inequalities were substantial, with pronounced top inequalities in urban areas. Financing for the care of cervical cancer and breast cancer is fragmented in China, with costs of screening not covered by health insurance schemes. In rural China, the National Essential Public Health Programme offers free screening for both cancers, but funds are limited and volumes of patients are kept low. While in the urban areas, women have to pay themselves in order to take up screening services, unless reimbursement is offered by the employer. As we showed, screening coverage was lower than 50% even among the urban richest, where medical technology is generally available and affordable, suggesting that willingness to pay may be one other factor that undermines utilisation.
One prominent issue is the persistent poor sanitation in rural areas and the worsening bottom inequalities in urban areas. In China, ensuring access to clean water is the responsibility of Government, while the management of basic sanitation is the responsibility of individual families. Our findings on poor sanitation among rural poor are consistent with evidence from other studies showing that most Western provinces, who are poorer, still have challenges.32 33 The worsening access to sanitation for the urban poor is worrying, and may be related, at least in part, to rapid urbanisation. Between 2008 and 2018, the share of China’s urban population increased from 47% to 60%,34 challenging the provision of basic services for the urban poor. Low access to basic sanitation for the rural poor may reflect inadequate social awareness among the ageing rural population, and the question arises whether responsibility for basic sanitation should be fully taken over by government.
Importantly, our finding stresses the challenges for China’s primary healthcare strategy towards UHC. Since 2009, the Chinese government has been investing substantially to provide preventive services free at the point of use in PHC facilities. Unfortunately however, we found that uptake of these free services were very limited. Equity implications are profound as well, as rich-poor inequalities in antenatal care persisted in the rural areas. Despite the National Essential Public Health Programme, the government has been examining mechanisms to establish a primary health care-based integrated delivery system since 2015. However, emerging evidence suggested little success.6 29 In China, provision of preventive services have long been fragmented from treatment services. Hospitals could provide compelling outpatient services as well. With health insurance policies encouraging hospitals to compete clients, PHC facilities seem not be attractive, even among the rural poor. China’s case is not unique. Recent data from 56 low-income and middle-income countries (LMICs) also showed that a large proportion of the population bypassed PHC facilities when seeking primary healthcare.35 Experiences from high-income countries illustrated that PHC facilities could not meet population needs without systemic mechanisms that put forward people-centred financial incentives36 and incorporate multidisciplinary expertise comprehensively integrating preventive, clinical, social and mental services.37 Given the context and limited management capacity, it is very unrealistic in rural China, and other similar LMICs settings as well, to expect PHC facilities in achieving such integrations in a short-run. With emerging experiences in rural China that integrate primary care services to county and prefectural level providers,38 it merits to consider the question whether primary healthcare services must be delivered via PHC facilities.
The strength of our analysis is that we report on a comprehensive list of indicators across the SDG agenda that contextualised China’s recent efforts to achieve UHC. We did not measure indicators such as hospital bed density or physician density because they do not relate to specific services and optimal levels are not known. We draw lessons from recent methodological developments to monitor rich-poor inequalities, paying particular attention to the most vulnerable, by separating income deciles within urban and rural China to visually show the trends and spotlight the poorest rural population who might be left behind. Our analysis has important limitations as well. First, we did not include catastrophic health spending, because recent trends has been reported elsewhere.6 More importantly, the NHSS changed its questions in asking families expenditures, and prior studies39 40 have shown that the measurement of catastrophic health spending is very sensitive to how family expenditures are asked. Further analyses are warranted to yield robust estimates by pooling various survey data. Second, measuring effective coverage remains a challenge. For example, the 2018 NHSS survey did not include questions on vaccine coverage because such data are obtained through a surveillance system. Overall immunisation coverage has increased dramatically in China, reaching 93.1% for full immunisation by 2013,41 but coverage remains lower among migrants and those with low levels of education.42 In addition, the NHSS reported that almost all children reported having a vaccination card (data not shown), which are provided by the government to facilitate and document the free vaccinations. Third, presenting data by income deciles within urban and rural areas posed sample size challenges. Even when we used income quintiles, the indicators relying on subgroups of children with diarrhoea had small sample sizes, with inconsistent patterns as a result. Caution is required in the interpretation of inequalities in these groups.
Conclusions
In this paper, we comprehensively appraised China’s progress in ensuring UHC within the SDG 3.8.1. There was little evidence of bottom inequality in both urban and rural areas, commending China’s success in protecting the poorest for basic care. However, most indicators provided no evidence indicating success of the government decade’s effort to revitalise primary healthcare. Coverage was particularly low for preventive services and that for non-communicable diseases. Additional gaps remain in sanitation, a wider social determinants of health. The low use of free services in general suggest the ‘leaving no one behind’ agenda needs a smarter strategy targeting the entire population rather than only the poorest. Contextualising in China’s health reform, we draw lessons that universal health insurance does not necessarily translate to universal health coverage. Without systematic efforts that consolidate the fragmentation in health finance and service delivery, blunt investing in primary healthcare facilities seems neither effective nor efficient.
Data availability statement
Data may be obtained from a third party and are not publicly available. Please contact YZ, Centre for Health Statistics and Information, National Health Commission of China (email: zhangyg@nhc.gov.cn).
Ethics statements
Patient consent for publication
Ethics approval
The NHSS is Chinese national information source that monitor the country’s population health needs, utilisation, costs and responsiveness. The surveys are authorised by China’s Statistics Bureau and administered by Centre for Health Statistics and Information, National Health Commission of China. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Lei Si
Contributors XLF and CR conceived the paper. XLF and YZ led the analysis. XLF and CR wrote the paper. Other authors contributed to the critical interpretation of the data.
Funding The Newton Advanced Fellowship Programme (grant ref. no. 71761130083) jointly supported by National Natural Science Foundation of China and the Academy of Medical Science. The funds take no role in the analysis of the data and interpretation of the findings.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the 'Methods' section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.