Article Text

Abstract
Introduction This study aimed to determine the prevalence of unsafe listening practices from exposure to personal listening devices (PLDs) and loud entertainment venues in individuals aged 12–34 years, and to estimate the number of young people who could be at risk of hearing loss from unsafe listening worldwide.
Methods We conducted a systematic review and meta-analysis to estimate the prevalence of unsafe listening practices from PLDs and loud entertainment venues. We searched three databases for peer-reviewed articles published between 2000 and 2021 that reported unsafe listening practices in individuals aged 12–34 years. Pooled prevalence estimates (95% CI) of exposed populations were calculated using random effects models or ascertained from the systematic review. The number of young people who could be at risk of hearing loss worldwide was estimated from the estimated global population aged 12–34 years, and best estimates of exposure to unsafe listening ascertained from this review.
Results Thirty-three studies (corresponding to data from 35 records and 19 046 individuals) were included; 17 and 18 records focused on PLD use and loud entertainment venues, respectively. The pooled prevalence estimate of exposure to unsafe listening from PLDs was 23.81% (95% CI 18.99% to 29.42%). There was limited certainty (p>0.50) in our pooled prevalence estimate for loud entertainment venues. Thus, we fitted a model as a function of intensity thresholds and exposure duration to identify the prevalence estimate as 48.20%. The global estimated number of young people who could be at risk of hearing loss from exposure to unsafe listening practices ranged from 0.67 to 1.35 billion.
Conclusions Unsafe listening practices are highly prevalent worldwide and may place over 1 billion young people at risk of hearing loss. There is an urgent need to prioritise policy focused on safe listening. The World Health Organization provides comprehensive materials to aid in policy development and implementation.
- Health policy
- Prevention strategies
- Public Health
- ENT diseases
- Systematic review
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Voluntary recreational noise exposure, or unsafe listening, is a modifiable risk factor for hearing loss in young people and may increase the risk of hearing loss in ageing. Estimates of the prevalence of unsafe listening practices or of the global caseload of young people engaging in unsafe listening practices are not available in the published literature, although such estimates are needed to promote policy implementation to reduce risk of hearing loss in young people.
What this study adds
Results from this study indicate that unsafe listening practices from use of personal listening devices and attendance at loud entertainment venues are common (prevalence estimates 23.81% and 48.20%, respectively) and may place up to 1.35 billion young people at risk of hearing loss worldwide.
How this study might affect research, practice or policy
These data will be used to communicate the urgent need to implement policy that promotes safe listening habits to governments, industry, civil society and other relevant stakeholders. The World Health Organization has publicly available standards, recommendations and toolkits to aid in development and implementation of policy and public health initiatives to promote safe listening worldwide.
Introduction
Hearing loss is a public health concern that deserves global recognition and prioritisation. The World Health Organization (WHO) estimates that over 430 million people worldwide have disabling hearing loss and that its prevalence may almost double if hearing loss prevention is not prioritised.1 Recreational noise exposure is a modifiable risk factor for hearing loss and, in 2015, the WHO estimated that 1.1 billion adolescents and young adults were at potential risk of hearing loss from voluntary recreational noise exposure, referred to henceforth as ‘unsafe listening practices’.2 This exposure is largely attributable to the use of personal listening devices (PLDs; eg, mobile phones or MP3 players) and/or from attendance at loud entertainment venues (eg, discotheques, bars, clubs).3 Importantly, unsafe listening behaviours are likely to be modifiable with implementation of existing policy recommendations and known public health practices.3
Recurrent or even single instances of unsafe listening may cause physiological damage to the auditory system, presenting as transient or permanent tinnitus and/or changes to hearing.4–6 Damage from unsafe listening can compound over the life course, and noise exposure earlier in life may make individuals more vulnerable to age-related hearing loss.7 8 Importantly, hearing loss, when it is unaddressed, has sizeable economic costs estimated at almost US$1 trillion annually,1 and has serious impacts on individuals and families. In children, hearing loss and/or noise exposure has been associated with poorer academic performance and reduced motivation and concentration,9 10 which may lead to a trajectory of limited economic mobility later in life. In adults, hearing loss has been associated with poorer psychosocial well being, lower income and serious comorbid health conditions such as cognitive impairment.11 Tinnitus also has important impacts on the health and well being of individuals and is associated with poorer quality of life.12
Unsafe listening practices are common worldwide, particularly among adolescents and young adults, given high availability of PLDs and scarce enforcement of regulatory measures for PLDs and entertainment venues.13 Risk of hearing loss depends on the loudness, duration and frequency of noise exposure. Permissible levels of recreational noise exposure are often calculated from equivalent occupational noise exposure limits (eg, 80 decibels (dB) for 40 hours a week or 85 dB for 40 hours a week),4 which vary slightly by region and/or by regulatory agencies or organisations.14 Sound intensity (dB) is measured on a logarithmic scale and there is a time-intensity tradeoff (exchange rate) for permissible levels and duration of exposure, meaning that permissible levels change drastically by sound level. For example, based on a maximum permissible level of noise exposure of 80 dB for 8 hours a day (40 hours/week) with a 3 dB exchange rate, the permissible exposure time of a 92 dB sound is 2.5 hours, of a 98 dB sound is 38 min, and of a 101 dB sound is only 19 min.4 15 PLD users commonly choose volumes as high as 105 dB and average sound levels at entertainment venues range from 104 to 112 dB,16 therefore exceeding permissible levels even for very short periods of time. These findings suggest that many young people could be at risk of developing permanent hearing loss. Some systematic reviews on unsafe listening practices have been conducted, although estimates of the prevalence and global burden of exposure are not available in the published literature.17–19 Global prevention efforts would benefit from data on the prevalence and global burden of unsafe listening practices to effectively communicate the need for preventative intervention to governments, industries and other stakeholders responsible for implementing policy.
The importance of hearing loss prevention is gaining traction on the global agenda,1 20 making now a particularly important time to prioritise interventions to prevent hearing loss. The aims of this systematic review and meta-analysis were (1) to determine the prevalence of unsafe listening practices from PLD use and attendance at loud entertainment venues in adolescents and young adults; and (2) to create a global estimate of the number of adolescents and young adults who could be at risk of hearing loss from unsafe listening practices.
Methods
Search strategy and selection criteria
This systematic review and meta-analysis was conducted under the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.21 Peer-reviewed papers published in English, Spanish, French or Russian languages between 2000 and 2021 that were case–control, cross-sectional or cohort studies were eligible for inclusion.
The papers must have contained information on human subjects aged 12–34 years. Studies focused on PLDs must have reported objectively measured device output levels and time of exposure. This information was used to define prevalence of unsafe listening practices (or risk of hearing loss) as equivalent to exceeding permissible levels (eg, >80 dB for 40 hours a week).4 Sound output levels measured at a single time point were presented as equivalent continuous levels (LAeq), which is the integrated normalised sound pressure divided by the duration of the signal, representing the average total energy of the measured sound. The LAeq is presented corresponding to daily or weekly maximum permissible levels (eg, >80 or >85 dB).
Studies focused on loud entertainment venues must have reported participants’ attendance at venues at least one time per month. Study samples must have been representative of the general population. For example, studies focused only on staff members working at loud entertainment venues were not eligible for inclusion.
The databases PubMed, Web of Science (core collection) and Scopus were searched in English in December 2021 using a combination of MeSH terms and key words (see online supplemental file 1). Two separate searches were conducted, one for PLD use and one for entertainment venues. Reference lists of included articles were searched for potentially eligible articles, and studies that cited included articles (listed on Google Scholar) were considered for eligibility.
Supplemental material
Studies in Spanish, French and Russian were ‘hand-searched’ using translated search terms and were assessed for eligibility by speakers of those languages. Trial registries or unpublished studies were not included.
Selection process and data extraction
Several reviewers extracted papers from the three databases (based on the language of the papers) and a single reviewer removed duplicates and completed the title and abstract screen based on eligibility criteria. References were exported to Mendeley, and full-text articles were shared with all study team members. The study team agreed on inclusion of all articles and any differences in inclusion/exclusion were reconciled via discussion among study team members.
Data extraction tables were developed by WHO biostatisticians. Extracted data included: (1) meta-study information (eg, authors, year of publication, journal, country, country income level); (2) sample characteristics (eg, age, sex, population, sample size); (3) prevalence of exposure to PLDs or loud entertainment venues that exceeded permissible sound levels; and (4) definitions of noise exposure and related measurements. Data were extracted by multiple reviewers and verified for accuracy by a separate reviewer. If duplicate data were included in eligible studies, we used the study with the best available data (ie, fit best with outcome of interest and target population). The primary outcome was the prevalence of the study population exposed to unsafe listening practices, defined as noise exceeding permissible exposure levels (eg, >80 dB LAeq for PLDs; attendance at loud entertainment venues ≥1 time per month).
Risk of bias assessment
A modified version of the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) scale was used to assess risk of bias for each study, based on the following categories: selection bias, study design, performance of data collection tools, completeness and reporting bias. For each study, these categories were ranked as strong, moderate or weak, which corresponded to presenting a low, moderate or high risk of bias, respectively. Studies were assigned an overall rating of weak if they were ranked as weak in at least one category; moderate if they had 0 rankings of weak and <2 rankings of strong; and strong if they had 0 rankings of weak and ≥2 rankings of strong. Sensitivity analyses evaluated pooled prevalence estimates after (1) excluding each study individually from analyses; (2) excluding studies considered to be weak (ie, high risk of bias); and (3) excluding studies considered to be weak and that defined risk with a definition classified as ‘other’.
Data analysis
Subgroup analyses by age category (adults: 18–34 years, minors: 12–19 years, mixed: 12–34 years), region and country income level were undertaken. Age was categorised based on age categories defined in included studies. Region was defined by the WHO classification22 and country income level was defined by the World Bank.23 Two categories of income were applied: (1) high income: ≥US$12 696 gross national income (GNI) per capita; or (2) middle income (including low-middle and high-middle income countries): US$4096–12 695 GNI per capita.
Following the corresponding Cochrane’s Q (χ2) and I2 statistics suggesting a large dispersion of effect sizes and a large amount of heterogeneity (between studies), we used random effects estimates to determine pooled prevalence of exposure and corresponding 95% CI. Varying but considerable heterogeneity was found in all subsequent subgroup analyses, warranting use of random effects estimates for all subgroup analyses. Analysis was conducted with Comprehensive Meta-Analysis software (CMA 3.3). The study protocol was not registered prior to study completion.
Global estimate of individuals who could be at risk of hearing loss from unsafe listening practices
The global number of individuals who could be at risk of developing hearing loss from exposure to PLDs or loud entertainment venues (ie, unsafe listening practices) was estimated by considering the estimated global population aged 12–34 years in 202224 and the best estimates of exposure to unsafe listening practices from PLDs or loud entertainment venues ascertained from this systematic review. We present the estimated global population of individuals who could be at risk of hearing loss from unsafe listening practices as a range, using prevalence estimates of exposure to both unsafe listening practices from PLDs and loud entertainment venues.
Results
A total of 389 non-duplicate citations were identified by using the selected keywords. After the final review, 33 articles were eligible for inclusion in this study. The study selection process is shown in figure 1.

Flow diagram (PRISMA 2020) summarising the article screening process.
Pertinent study characteristics are shown in table 1. A total of 35 records from 33 studies corresponding to data from 19 046 individuals were included.5 25–54 Seventeen records focused on PLD use (n=8987 participants) and 18 records focused on loud entertainment venues (n=10059 participants). Studies were from 20 countries corresponding to representation from American (n=12), European (n=16), Middle Eastern (n=2) South-East Asian (n=1) and Western Pacific (n=4) regions. Twenty-seven and eight study records were from high-income and middle-income (upper or lower) countries, respectively. Sixteen study records focused on adults, 10 focused on minors, and nine focused on mixed age groups (adults and minors). The pooled samples had even distributions by gender (49% female, 51% male).
Pertinent study characteristics of all studies in the systematic review
Personal listening devices
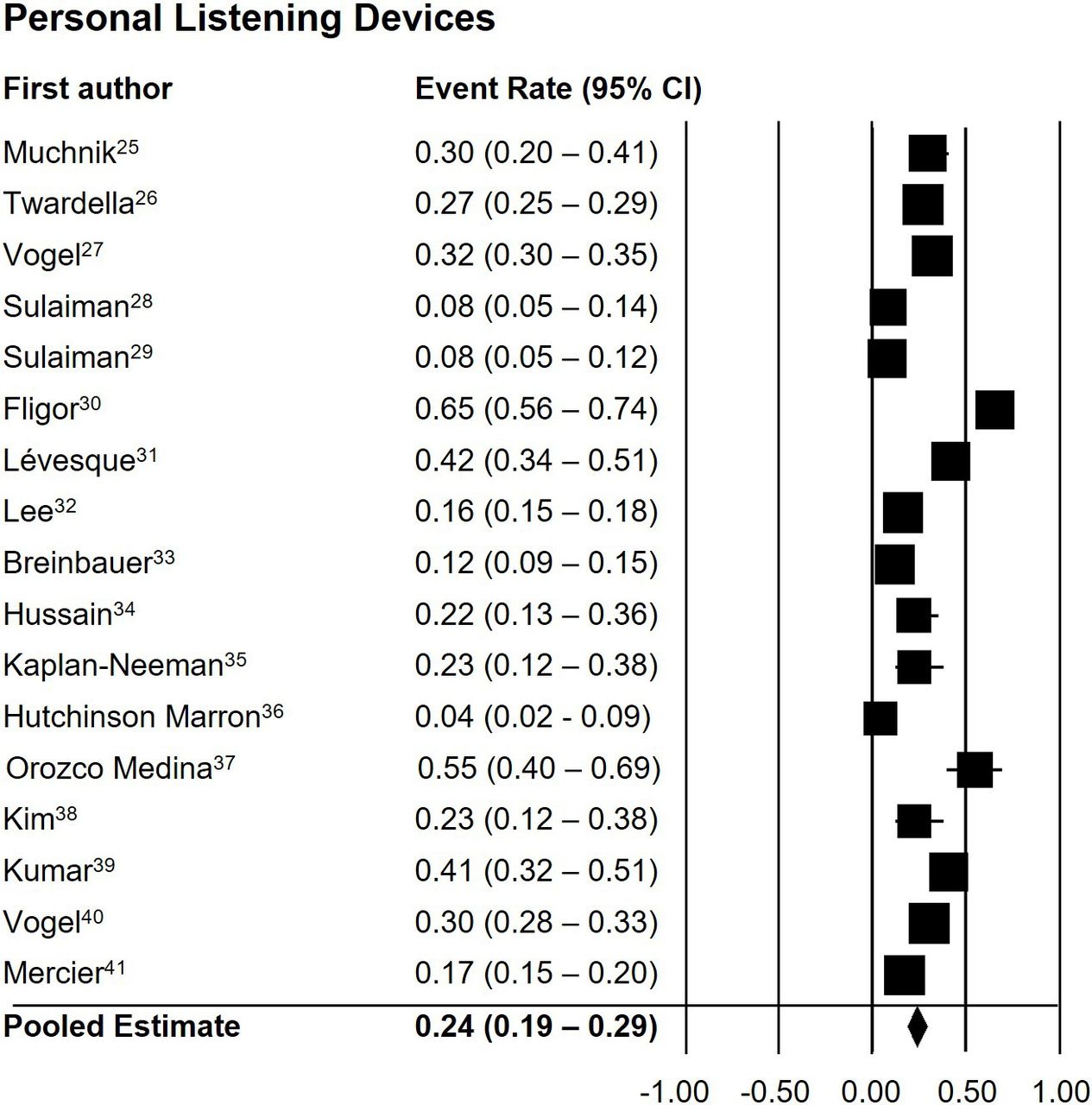
The pooled prevalence estimates of exposure to excessive noise from PLDs was 23.81% (95% CI 18.99% to 29.42%). Figure 2 is a forest plot showing point estimates from each study and the pooled prevalence estimate. Table 2 shows the pooled prevalence estimates of exposure to excessive noise from PLDs overall and by subgroups age category, income group and details of risk criteria. Prevalence estimates were similar for age categories (adults: 23.10% (95% CI 8.90% to 48.03%); minors: 27.10% (95% CI 21.25% to 33.88%); mixed: 21.55% (95% CI 14.65% to 30.53%)) and income groups (high: 24.51% (95% CI 19.35% to 30.53%); middle: 22.12% (95% CI 7.15% to 51.17%)), although the middle-income group showed substantial variability. Prevalence estimates were (non-significantly) highest in studies using definitions of weekly exposure (LAeq >80 dB (36.37% (95% CI 29.18% to 44.22%)) compared with definitions measuring daily exposure (LAeq >80 dB (12.95% (95% CI 5.10% to 29.20%); LAeq >85 dB (21.36% (95% CI 13.50% to 32.09%)) or using other definitions (23.15% (95% CI 11.28% to 41.67%)).
Pooled prevalence estimates of exposure to excessive noise from personal listening devices (PLDs)
{kind=link}
{kind=link}
Forest plot showing study-specific and overall prevalence estimates of exposure to personal listening devices for the 17 studies included in the meta-analysis.
Our risk of bias assessment showed that, for the 17 studies focused on PLDs, five (29%) were rated as strong, eight (47%) as moderate and four (24%) as weak (see online supplemental file 2). Sensitivity analyses evaluated changes in pooled prevalence estimates after removing each study individually from analyses. The prevalence estimates and confidence intervals were stable (<2% change) after removal of each study, indicating pooled prevalence estimates were insensitive to individual study inclusion. Sensitivity analyses removing studies with a high risk of bias (ie, rated as ‘weak’) and studies with a high risk of bias and with a risk criterion classified as ‘other’ did not return substantially different estimates compared with the estimate using data from all studies (23.81% (95% CI 18.99% to 29.42%)) (results not shown).
Supplemental material
Loud entertainment venues
The pooled prevalence estimate for exposure to excessive noise from loud entertainment venues was calculated from the 18 studies in the systematic review, but there was limited certainty (p>0.50) in our estimate. Thus, estimates (including subgroup analyses) calculated from the 18 studies are not presented.
The risk of bias assessment showed that, for the 18 studies focused on loud entertainment venues, two (11%) were rated as strong, 12 (67%) as moderate and four (22%) as weak (see online supplemental file 2). Sensitivity analyses that removed studies with a high risk of bias (ie, rated as ‘weak’) and studies with a high risk of bias and with risk criteria classified as ‘attending a loud entertainment venue at least once a week’ were conducted but also yielded estimates with limited certainty (results not shown).
Therefore, ad hoc analyses aimed to reduce heterogeneity across studies by considering only studies that equated intensity and duration of sound levels to LAeq values. There were three studies that met this criterion,27 40 41 all of which used slightly different definitions to define risk. Several steps were taken to select the preferred prevalence estimate used to compute the global estimate of individuals who could be at risk of hearing loss from unsafe listening practices at loud entertainment venues (described in online supplemental file 3).
Supplemental material
The chosen quadratic model was a very good fit for all the studies, with a higher quadratic dependence on intensity than on duration (see online supplemental file 3; figure S3b): Prev(x,y) = −5.3E-0.5x2+6.2E-05xy+0.003y2-0.56y+25.85. The model was then used to approximate a prevalence of 48.20% for an intensity threshold of 80 dB and duration threshold of 40 hours per week.
Thus, to estimate the number of individuals who could be at risk of hearing loss from unsafe listening, we used the estimated prevalence of 48.20% of exposure to excessive noise from loud entertainment venues given that this estimate (1) accounts for duration and level of exposure; (2) was consistent (of the studies in online supplemental file 3) with the WHO definition of excessive noise exposure based on permissible sound pressure levels of 80 dB for 40 hours per week2; and (3) that prevalence estimates for the three studies that had values of duration and intensity were commensurate.
Heterogeneity and publication bias
The I2 statistics for studies on PLD use and loud entertainment venues were 96.2 and 98.8, respectively, indicating a high amount of heterogeneity among studies. Funnel plots of SE by logit event rate (not shown) were symmetrical and thus did not suggest publication bias.
Global estimate of individuals at risk of hearing loss from unsafe listening practices
In 2022, the estimated global population aged 12–34 years was 2.8 billion.24 We used the pooled prevalence estimate of exposure to excessive noise from PLDs ascertained from this systematic review and meta-analysis (23.81% (95% CI 18.99% to 29.42%)). For loud entertainment venues, we used the prevalence estimate (48.20%) described above. Therefore, the global estimated number of adolescents and young adults who could be at risk of hearing loss from voluntary exposure to unsafe listening practices ranges from 0.67 to 1.35 billion. Estimates are shown in table 3.
Estimated global population of individuals exposed to recreational noise from personal listening devices or loud entertainment venues
Discussion
Results from this systematic review and meta-analysis show that unsafe listening practices are highly prevalent among adolescents and young adults and that an estimated 0.67–1.35 billion individuals worldwide could be at risk of hearing loss from voluntary unsafe recreational listening practices. These findings highlight the urgent need to implement policy focused on safe listening habits worldwide in order to promote hearing loss prevention.
Increased exposure to unsafe listening practices may be one cause of increasing prevalence of hearing loss in children.55 56 However, previous studies have reported inconclusive findings on associations between unsafe listening practices and permanent changes to hearing.57 Evidence showing consistent associations of adolescent recreational noise exposure and permanent hearing loss is sparse, and the potential dose-response relationship of recreational noise exposure and associated hearing loss is not understood. While some studies have not observed associations between recreational noise exposure and permanent hearing loss,58 59 others have indicated that the use of PLDs for extended periods of time can result in changes to hearing thresholds.60 Inconsistencies in existing research are likely in part because hearing loss is incremental and progressive, thus making it difficult to capture short-term effects of noise exposure in adolescents. Well-designed epidemiological studies are needed to evaluate the effects of early life recreational noise exposure on hearing throughout the life course and to identify relevant risk factors associated with unsafe listening practices.
Despite some inconsistent research on associations of recreational noise exposure and permanent changes to hearing in adolescence, studies conducted in animals and human subjects have provided compelling evidence for the biological plausibility of associations, demonstrated by the physiological impacts of loud noise exposure on the auditory system. Studies have indicated that repeated or even single instances of loud noise exposure may lead to physiological damage that presents as temporary hearing loss (temporary threshold shifts) which resolves within several hours or days, or acute tinnitus, both of which may be predictive of permanent hearing damage.5 6 49 61 62 Similarly, repeated or single exposures to noise and temporary threshold shifts have been tied to the presence of ‘hidden hearing loss’, also known as cochlear synaptopathy, which can be defined as damage to or a loss of synaptic contacts between cochlear hair cells and auditory nerve fibres that can exist without permanent changes to audiometric thresholds.63 Temporary threshold shifts and hidden hearing loss likely serve as predictors for irreversible permanent hearing loss and may present as difficulties hearing in challenging listening environments, such as in background noise. Studies have indicated that mechanisms of noise-induced hearing loss include damaged synapses, destruction of the sensory cells in the cochlea, and intense metabolic activity at the cellular level which leads to raised levels of cochlear free radicals, eventually leading to programmed and/or necrotic cell death.63–66 These physiological changes likely result in progressive and incremental, yet permanent, changes to hearing thresholds and/or the onset of tinnitus.67
The detrimental impacts of noise exposure on auditory and non-auditory health have been described, and unsafe listening practices are recognised as an important global public health problem.4 In 2015, the WHO launched the ‘Make listening safe’ initiative to ensure people of all ages can enjoy listening with full protection of their hearing.68 This initiative aims to modify unsafe listening behaviours and regulate and limit (when necessary) voluntary exposure to loud sounds from PLDs and other loud recreational settings, including from entertainment venues. ‘Make listening safe’ prioritises educating the general population, policymakers, health professionals and manufacturers about the importance of safe listening practices that are needed to prevent hearing loss. The WHO and its partners have released several publicly available resources in multiple languages that can be adapted to specific settings, including awareness materials for individuals,2 a depository of open-access resources, and the standards and toolkits briefly discussed below. The WHO offers support to member states, private sector entities and civil society in adopting and implementing these standards and toolkits, and promotes partnerships that will encourage implementation of ‘Make listening safe’.
In 2018, the WHO and International Telecommunication Union (ITU) released global standards for safe listening devices and systems to define suitable exposure limits and safety standards for listening devices/systems and this resource also details implementation strategies.69 The WHO toolkit for safe listening devices and systems provides a user-friendly summary and a stepwise approach for governments, industry and civil society to implement these standards.3 This year, the WHO released the global standard for safe listening venues and events, which aims to protect hearing of audience members at recreational venues such as discotheques, bars, concerts and festivals by providing standardised evidence-based recommendations and implementation strategies to reduce the risk of unsafe noise exposure.13 The features detailed in this standard can be implemented through governmental legislation or regulation, and/or by voluntary adoption by venue owners or managers. Also this year, the WHO released the mSafeListening handbook, which provides details needed to develop, integrate, implement and evaluate a national mSafeListening programme to promote hearing loss prevention and promotes the use of digital interventions.70
In addition to recommendations and standards for governments, industry and civil society, the WHO provides educational resources that can be used by the general public.2 71 Recommendations for safe listening focus on reducing sound levels and duration of exposure, monitoring listening levels (ie, through device settings), use of hearing protection and heeding the early signs of hearing loss, such as tinnitus and difficulties understanding in background noise.
Findings from this study support the need to implement the above policy recommendations. Prevalence estimates of exposure to excessive noise from PLD use and loud entertainment venues were high. However, high study heterogeneity was present and was particularly salient in studies focused on loud entertainment venues. The heterogenous methodologies and definitions used in these studies likely contributed to the low confidence (ie, higher p values) in pooled prevalence estimates that were created using all studies in the systematic review focused on loud entertainment venues (data not shown). These results highlight the need to reduce heterogeneity of measurement and outcome definitions in studies focused on exposure to unsafe listening. Thus, it is recommended that future studies focused on unsafe listening use internationally standardised definitions of excessive recreational noise exposure and measure sound exposure using standardised methodology.
There are likely demographic (eg, by gender, age, rurality) and personal differences in risk perception and preferences and engagement in risky behaviours, including voluntary recreational noise exposure.51 72 73 This notion is supported by pooled prevalence estimates of exposure to excessive noise from PLDs stratified by age group, which suggest that minors (vs adults) may be slightly more likely to be exposed to unsafe listening from PLDs. We were unable to evaluate potential differences across other demographic strata such as gender or rurality, given the limitations of data reported in the studies included in the systematic review. Our estimate of the global population likely exposed to unsafe listening levels was crude, yet was created with the most current and best available data.
Strengths and limitations
To our knowledge, this review is the first published article to estimate the prevalence of exposure to unsafe listening practices in adolescents and young adults and its global burden. These estimates are needed to communicate the urgency of prioritising hearing loss prevention to governments, industries and other stakeholders responsible for implementing policy. However, some limitations exist. This systematic review and meta-analysis are limited by the heterogeneity and lack of standardised research methodology of the studies included. As mentioned above, there was particularly high heterogeneity in studies focused on loud entertainment venues. Although we conducted the literature search in four languages, there may be published articles in other languages that were not captured in this systematic review. Most studies were from European and American regions and thus may not be reflective of unsafe listening practices in other regions. There were no studies from low-income countries eligible for inclusion in the meta-analysis, and therefore the estimates of prevalence or global burden may not capture unsafe listening practices in low-income countries. However, it is likely that the prevalence of unsafe listening practices is high in low-income countries given limited policies and regulations on noise exposure limits.13 Our global estimate of exposed individuals was crude and did not account for some potentially influential factors, such as demographic factors and recent changes to policy on safe listening in some countries/regions.
Conclusion
Exposure to unsafe listening practices from voluntary use of PLDs and attendance at loud entertainment venues is highly prevalent in adolescents and young adults. It is estimated that 0.67–1.35 billion adolescents and young adults worldwide could be at risk of hearing loss from exposure to unsafe listening practices. There is an urgent need for governments, industry and civil society to prioritise global hearing loss prevention by promoting safe listening practices. WHO global standards, recommendations and toolkits are available to aid in the development and implementation of policy and public health initiatives to promote safe listening worldwide.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors thank Artem A Shchepilov for translating the studies from Russian to English and Juan J Lopez Perez for extracting the studies in Spanish.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Press release
Footnotes
Handling editor Seema Biswas
Twitter @lauren_dillard
Contributors LKD (guarantor): Conceptualization, methodology, writing – original draft, visualization. MOA: Conceptualization, methodology, writing – review and editing. LL-P: Methodology, formal analysis, writing – review and editing. RXM: Methodology, formal analysis, writing – review and editing. LJ: Methodology, writing – review and editing. SC: Conceptualization, methodology, resources, writing – review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.