Article Text

Abstract
The financing of public health facilities influences their performance. A key feature that defines health facility financing is the degree of financial autonomy. Understanding the factors that influence public health facility financial autonomy is pertinent to developing strategies to addressing challenges that arise from constrained autonomy. In this paper, we apply a complexity lens to draw on a body of research that we have conducted in Kenya over the past decade, from the onset of devolution reforms, to unpack the determinants of public health facility financial autonomy in a context of decentralisation and provide suggestions for pertinent considerations when designing interventions to address financial autonomy challenges. We find that the factors that affect public health facility autonomy are not only structural, but also procedural, and political and interact in complex ways. These factors include; the public finance management (PFM) laws, sense-making by actors in the health system, political interests in control over resources, subnational level PFM capacity, PFM implementation bottlenecks and broader operational autonomy. Drawing from this analysis, we recommend that efforts at resolving public health facility financial autonomy include: PFM capacity development for subnational levels of government in decentralised settings, the use of a political lens that recognises interests and seeks to align incentives in engagement and solution finding for health facility financial autonomy, the audit of PFM processes to establish and resolve implementation bottlenecks that impinge on public health facility autonomy, and the resolution of operational autonomy to as a facilitator of financial autonomy.
- Health policy
- Health systems
Data availability statement
All the literature from which this analysis draws on is presented in table 1 of the main manuscript.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Health facility financial autonomy is a key aspect of health financing, and determines the function and performance of public health facilities.
The legal framework and structure of public finance management (PFM) systems determines the extent of financial autonomy that public facilities have.
Beyond, legal and structural issues, public health facility financing is influenced by the complex interactions of multiple factors that include sense-making, political interests, health facility capacity, PFM bottlenecks and broader operational autonomy.
Subnational levels of government in decentralised settings should be supported to develop PFM capacity.
A political lens that recognises interests and incentives should be applied in engagement and solution finding for health facility financial autonomy.
An audit of PFM processes to establish and resolve implementation bottlenecks that impinge on public health facility autonomy should be explored.
Efforts at addressing financial autonomy should also resolve operational autonomy issues to give meaning to the former.
Introduction
The financing of public health facilities influences their performance, and ultimately, broader health system performance. A key feature that defines health facility financing is the degree of financial autonomy.1 Financial autonomy refers to the level of control and influence that health facility managers have, to mobilise, allocate and spend financial resources. Financial autonomy is only but one dimension of the broader concept of facility autonomy, which encompasses the level of control and influence that health facilities have over key functions that include health facility administration, financial management, procurement, human resource management and strategic management.1 The granting of autonomy to health facilities is a pathway to operationalising decentralisation in health systems. In the past three decades, several low-income and middle-income countries (LMICs) have implemented decentralisation reforms with the aim of improving the equity, efficiency and accountability of government service delivery.2 3 Three dimensions of decentralisation interact to influence the experience and outcomes of decentralisation; fiscal, political and administrative.4 Fiscal decentralisation refers to the assignment of financial management functions including budgeting, revenue raising and authority to spend. Political decentralisation refers to the assignment of political responsibilities to subnational levels, while administrative decentralisation refers to the transfer of administrative functions such as human resource management, procurement among others.
While the impact of health financial autonomy has been reported as mixed (enhancing health systems goals in some instances, and not doing so in other instances) and contingent on other factors, there is evidence that it may enhance the efficiency of resource allocation and operations, and responsiveness of public health facilities.5–7 For instance, hospital financial autonomy reforms have been shown to improve the technical efficiency (where outputs are maximised for a given level of resources or vice versa) of hospitals in Columbia,8 Uganda9 and Kenya.10 On the other hand, lack of financial autonomy can compromise health facility functioning in several ways. Inadequate autonomy can constrain access to resources, and compromise allocative efficiencies by misaligning priorities and reducing the responsiveness of health facilities to local health needs. Inadequate autonomy can also introduce operational inefficiencies because of bureaucratic delays, poor staff motivation and stock outs of essential supplies.11–13 Inadequate autonomy has also been shown to weaken health facility leadership, management and accountability.1
While decentralisation is often expected to enhance financial autonomy at the local levels, evidence has shown that this is not always the case.1 14 15 For instance, in Kenya decentralisation resulted in a counterintuitive recentralisation of autonomy over financial management from the public health facility level to the local government level.1 Understanding the factors that influence public health facility financial autonomy is pertinent to developing strategies to addressing challenges that arise from constrained autonomy. In this paper, we draw on a body of research that we have conducted in Kenya over the past decade (table 1), from the onset of devolution reforms, to unpack the determinants of public health facility financial autonomy in a context of decentralisation and provide suggestions for pertinent considerations when designing interventions to address financial autonomy challenges. We reviewed this literature to identify evidence on the factors that influence health facility autonomy in Kenya.
Reviewed literature
Kenya country context
In 2013, Kenya adopted a devolved government system characterised by a central government and 47 semiautonomous county governments.16 In the health sector, the national government retained policy and regulatory roles, and national referral services, while the county governments took on service delivery roles, including the ownership and management of public health facilities.17 Counties are now responsible for priority setting, planning and budgeting, and allocation of resources to the health sector; procurement and human resource management, as well as overseeing service delivery. Counties are funded from an unconditional block grant (equitable share) and specific conditional grants from the national government, from total government revenues, own source revenues and donor funding.17 The unconditional block grants allocations by the national government contribute the largest share of the county resources.18
The public healthcare delivery system is now organised into four tiers, namely community, primary care, county referral (all managed by counties) and national referral services (managed by the national government). Community health services include all community-based demand creation activities that are guided by theministry of health (MOH) community strategy. Primary healthcare includes services that are provided by public and private maternity homes, health centres and dispensaries. The county-level public health facilities are funded by county budget allocations, reimbursements and prospective payments by the public insurer, the National Health Insurance Fund, donor funding and (for hospitals), user fee collections.12 Alongside devolution, a new public finance management act (PFM act 2012) came into effect to guide the management of public resources under this new governance arrangement.
Determinants of public health facility financial autonomy
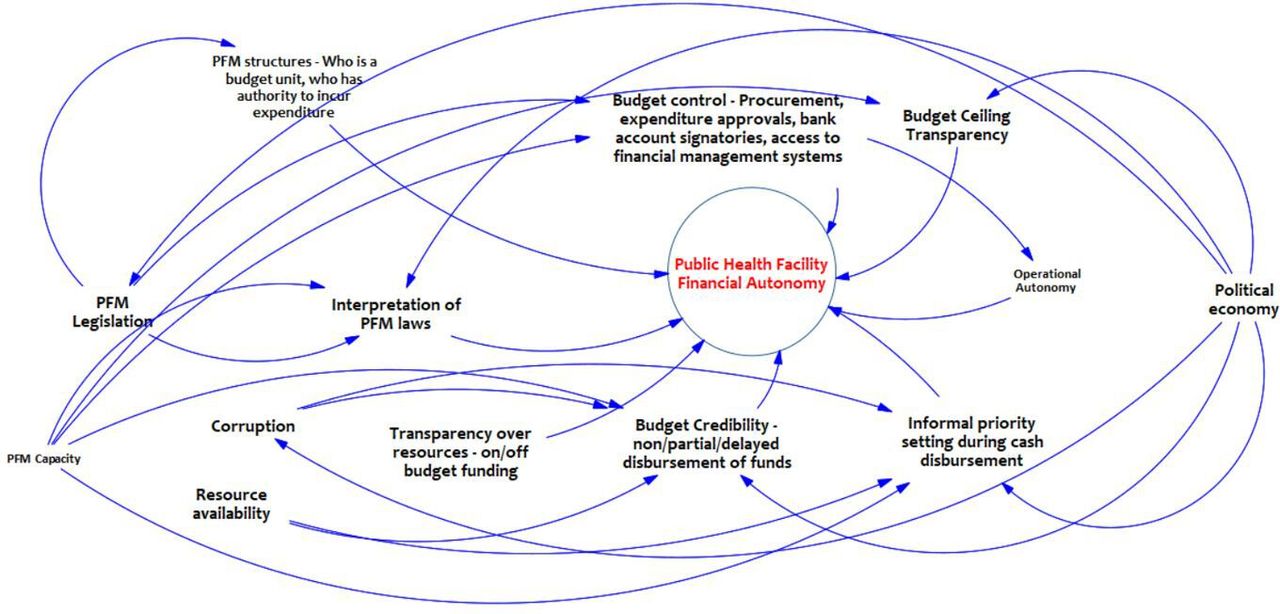
Predevolution, public health facilities in Kenya had greater financial autonomy.19 However, postdevolution, public health facilities in Kenya lost this autonomy.1 While this challenge (recentralisation within decentralisation) has often been thought of as formal and structural, the Kenyan experience shows that public health facility financial autonomy is determined by the complex interaction of both formal and informal factors. Similar findings have been reported in Uganda, where de jure autonomy is often different from de facto autonomy, with the latter being dynamic and influenced by multiple factors.5 Further, these factors are not only structural, but also procedural and political. Figure 1 identifies and outlines the interactions across these factors from the Kenyan experience. We discuss them in turn.

{kind=link}
Determinants of public health facility autonomy. PFM, public finance management.
Public finance legislation
Our early research on public health facility autonomy in Kenya identified legislation as the cause for the recentralisation of financial autonomy from the health facility level to the county level.1 17 The new PFM law, which defined fiscal decentralisation arrangements, created a single treasury account—the consolidated county revenue fund (CRF) and required that all county government resources including public health facility funds be rerouted to the CRF and managed centrally.1 17 The PFM act derolled public health facilities from being budgeting and expenditure units, having access to the integrated financial management information system and having rights to funds collected in their bank accounts. Public facilities hence lost the access and authority to directly spend cash resources from multiple sources (budget allocations, national hospital insurance fund reimbursements and user fee collections). PFM legislation determined the structure of the PFM system, which in turn constrained public health facility autonomy (figure 1). Legislation has also been shown to influence health facility autonomy in Turkey,20 Pakistan,21 Iran22 and Vietnam.23
This understanding of the problem informed policy discussions to either amend Kenya’s PFM laws to reinstal public health facility financial autonomy or develop county-level legislation that provide for health facilities to have access and control over financial resources. While the PFM act has not been amended, some counties have developed legislation to provide for health facility financial autonomy. However, this legal intervention has had mixed effects. While the introduction of county level legislation has resulted in the re-instalment of health facility financial autonomy in some counties, it has not had an impact in other counties.12 Further, some counties have reintroduced health facility financial autonomy without amending existing or developing new legislation.12 It is also instructive that negotiations between development partners and the government led to the creation of special purpose accounts for donor conditional grants for public primary health facilities.12 The creation of these special purpose accounts has been within the existing PFM laws and led to a situation in some counties where primary healthcare facilities have financial autonomy while public hospitals do not.12 So, while the PFM laws that determine PFM structure and processes clearly have a role to play in determining public health facility financial autonomy, it is apparent that this is only part of the picture, and that other factors are at play.
The role of sense-making
How system actors understand and interpret PFM legislation determines its de facto implementation. The Kenyan experience has been that while the PFM laws provide for provisions for public health facilities to have financial autonomy, system actors at the county level in some counties have inappropriately (mis)interpreted the PFM laws as providing no exceptions or options for autonomy at the public health facility level.12 Counties that allowed public health facilities to have financial autonomy without the need to develop or amend legislation correctly implemented PFM laws, while counties that developed or amended legislation and then provided health facilities with financial autonomy are likely to have innocently misinterpreted PFM legislation. However, we argue that counties that have continued to deny public health facilities financial autonomy, with or without new or amended legislation, are likely strategically misinterpreting PFM laws, driven by political interests in the control of resources. This is especially so because there have been extensive engagements with county governments and capacity development initiatives by non-state partners on PFM laws in Kenya over the past decade. These engagements have resulted in county governments agreeing on a joint resolution in 2020 to resolve the facility financial autonomy issue.
Political interest in control over resources
While decentralisation has at times been discussed in health literature as a technocratic process, aimed at solving technical problems, Kenya’s devolution has been shown to also be political aimed at solving political problems of resource allocation.17 24 Political decentralisation under Kenya’s devolution established a local political elite, with a Governor as the political head of the county government, and members of county assemblies as political representatives of wards. It also created a local bureaucracy, with the executive arm of county governments omposed of county executives that head sectoral county departments. Tensions between national and subnational levels over resource allocation, function allocation and control over resources in the context of decentralisation have been documented in literature.14 15 What we see in Kenya is similar tensions between the county government and subcounty levels that include public health facilities. At the county level, control over resources is concentrated at the county treasury, with other departments, including the county department of health and units under it, such as health facilities having limited power and control over resources.25 26 Given that public health facilities are one of the key sources of locally generated revenues at the county level, county-level actors are reluctant to relinquish control over these resources to public health facilities (figure 1). County leaders are keen to consolidate their power and retaining control over resources and decision making is one way to achieve this. This control could also be used inappropriately, and county level political interests have been shown to influence decisions with negative implications for health system performance.13 27 It is likely that such political interest in control over resources manifests in overt resistance by some counties to give public health facilities autonomy, or covert resistance, camouflaged in strategic misinterpretation of PFM laws. Similar findings have been reported in Malawi where politicians resisted hospital autonomy reforms on the basis that it would lead to loss of power and control over resources.28
PFM capacity at the decentralised level
We have also reported PFM capacity challenges at the county level. The rapid devolution resulted in the transfer of functions before the capacity to implement these functions were fully formed.17 29 Counties were characterised by lack of guidelines and fragmented approaches to planning and budgeting in the health sector, making it problematic for health facilities to plan and budget for their resources.17 30 Early on, county treasuries experienced challenges coping with financial requests.29 These capacity challenges have manifested in suboptimal budget formulation, execution and monitoring challenges that have affected health facility autonomy (figure 1).25 26 Capacity challenges as impediments to de facto autonomy have been documented elsewhere.5 6
Operational autonomy
Financial autonomy is only relevant to the extent that it allows health facility managers to take action over other health management issues. Administrative decentralisation arrangements in Kenya’s devolved system have transferred key health functions to county governments including human resource management (hiring, deployment remunerating and firing) and procurement. However, these functions are consolidated at the county level, with subcounty levels including health facilities relinquishing these roles. This has meant that health facilities have lost their operational autonomy over these functions. Operational autonomy refers to decision-making latitude over key organisational functions—human resource management, procurement, strategic management and administration. While debates about health facility autonomy focus more on financial autonomy, our work in Kenya shows that the autonomy of health facilities over other key functions (operational autonomy) is equally important. While operational autonomy is inherently important to public health facilities, it is also instrumentally important to the extent that it operationalises financial autonomy (figure 1).1 We found that health facility financial autonomy can only be leveraged on by health facilities if they also have autonomy over operational decisions.1 The fact that in Kenya, the recruitment and management of casual staff, the procurement of health commodities, and the planning and budgeting of healthcare resources were recentralised away from public health facilities to the county level meant that health facilities de facto lost autonomy even for funds that they retained at the health facility level because they could not exercise discretion in allocating funds to these key organisational functions.
PFM process bottlenecks
Our findings in Kenya show that even when the laws and structure de jure assure public health facility financial autonomy, everyday PFM bottlenecks may de facto constrain autonomy. With regard to budget formulation, we found that county health department budget ceilings are not always transparent and hence not communicated to public health facilities (figure 1).25 Without visibility over the resources that are allocated to them, public health facilities found it difficult to plan and budget and were hence disenfranchised from the opportunity to plan for and allocate resources. While the inadequate transparency of budget ceilings is partly attributed to process inadequacies, it is also a manifestation of political interests by county level actors that are keen to retain control over resource allocation and expenditure decisions.25 The inadequate visibility over resources available to health facilities was also caused by the off-budget support that counties and health facilities got from donors.25 Public health facility’s ability to adequately plan, prioritise, and spend is compromised by the practice whereby donors do not reveal their funding support to counties and health facilities, and go ahead to implement supported activities outside of government PFM systems and planning and budgeting processes.12 25 Further, in some counties, the budgeting and planning for public health facilities was carried out by the county health department rather than the public health facilities themselves. This entrenched the inability of health facilities to plan and allocate resources.12
Several bottlenecks are apparent with regard to the budget execution process (figure 1). We found that the credibility of health budgets in some counties was inadequate.26 County health departments often received less funds than what was originally allocated in official budgets. Further, funds disbursements by county treasuries to county departments of health, and public health facilities was often delayed. This was partly because of the fiscal constraints at the national level and hence delaying disbursements to county governments.26 Resource scarcity meant that funds were not available for disbursement at all, or on time. Non-disbursement or late disbursement was also because of the political interest in county-level actors to have control over resources. This manifested in the form of county level actor reallocating budgets originally meant for health, to other priorities through development of supplementary budgets.26 None or late disbursement was also because of corruption, whereby funds were either misappropriated or county level offers sought bribes before disbursements could be made (rent seeking). Non-credible budgets, coupled with funding disbursement delays resulted in constrained resources, and uncertainty about the level of funding, crippling planning and decision making. The cash disbursement process also affected public health facility autonomy. We found that treasury accountants that were responsible for cash disbursement unilaterally (to the exclusion of county health managers) prioritised what programmes or activities to disburse funds for.26 So, while on paper budgets outlined priorities, in practice, this informal priority setting by county treasury accountants determined priorities. The informal priority setting by county treasury was occasioned by lack of clear guidelines on how to prioritise disbursements. It was also as a manifestation of the county treasury desire for control over resources. It also offered an opportunity for corruption by rent seeking county treasury staff who demanded bribes to make payments. This contributed to the disempowerment of public health facility managers from making decisions about priorities and how to spend resources allocated to them.
Conclusion
While challenges in public health facility autonomy in LMICs are often treated as techno-structural phenomena, the experience in Kenya, applying a complexity lens reveals that process, and politics also play a key role, and that often these factors are interdependent. It is apparent that all three dimensions of decentralisation—political, fiscal and administrative interact to influence health facility autonomy. A focus on financial autonomy should be in tandem with a focus on operational autonomy, as well as the role of politics in facilitating health facilities to use their resources to carry out their functions. These observations have a range of potential implications for efforts to reform country health systems to provide public health facilities with financial autonomy.
First, it is imperative that subnational levels of government in decentralised settings are supported to develop PFM capacity. This includes the translation of overarching PFM laws into operational systems and processes that are adapted to the roles that have been assigned to them. It also includes PFM knowledge capacity development efforts of subnational level decision makers, especially in countries that are planning to or have only recently introduced decentralisation reforms. Second, a political lens that recognises interests and incentives should be applied in engagement and solution finding where subnational levels are not keen to relinquish control over resources. For instance, rather than making it a zero-sum game, where either the subnational level or the health facility gains control over resources, revenue sharing arrangements and other negotiated positions could be explored. Further, incremental and progressive reforms are more likely than large-scale overnight reforms, given that such reforms threaten entrenched actor interests. Third, anticorruption measures should be explored to minimise the impact of rent-seeking interests on PFM processes. A discussion of anticorruption strategies is beyond the scope of this paper. Fourth, an audit of PFM processes to establish and resolve implementation bottlenecks that impinge on public health facility autonomy should be part of efforts to address health facility autonomy issues. Lastly, financial autonomy is useless without operational autonomy. Efforts at addressing financial autonomy should also resolve operational autonomy issues to give meaning to the former.
Data availability statement
All the literature from which this analysis draws on is presented in table 1 of the main manuscript.
Ethics statements
Patient consent for publication
Acknowledgments
This manuscript is published with the permission of the Director of KEMRI. This work was Funded by an MRC/FCDO/ESRC/Wellcome Trust Health Systems Research Initiative (HSRI) Grant No. MR/R01373X/1. Additional funds from a Wellcome Trust core grant awarded to the KEMRI-Wellcome Trust Research Program (#092654) supported this work.
References
Footnotes
Handling editor Seye Abimbola
Twitter @edwinebarasa
Contributors EB wrote the first draft of the manuscript. All authors led (collected data, analyzed, and published) primary research that formed the basis of this analysis. All authors contributed to subsequent revisions of the manuscript.
Funding This study was funded by MRC/FCDO/ESRC/Wellcome Trust Health Systems Research Initiative. Wellcome Trust092654
Disclaimer The funders had no role in study design, data analysis, decision to publish, drafting or submission of the manuscript. The views expressed in the papers are for the authors and not for the organisations they represent.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.