Article Text

Abstract
Introduction Many families in low-income and middle-income countries have high out-of-pocket expenditures (OOPE) for healthcare, and some face impoverishment. We aimed to assess the effect of Kangaroo Mother Care initiated in community setting (ciKMC) on financial risk protection estimated by healthcare OOPE, catastrophic healthcare expenditure (CHE) and impoverishment due to healthcare seeking for low birthweight infants, using a randomised controlled trial design.
Methods We included 4475 low birthweight infants randomised to a ciKMC (2491 infants) and a control (1984 infants) arm, in a large trial conducted between 2017 and 2018 in Haryana, India. We used generalised linear models of the Gaussian family with an identity link to estimate the mean difference in healthcare OOPE, and Cox regression to estimate the HRs for CHE and impoverishment, between the trial arms.
Results Overall, in the 8-week observation period, the mean healthcare OOPE per infant was lower (US$20.0) in the ciKMC arm compared with the control arm (US$25.6) that is, difference of −US$5.5, 95% CI −US$11.4 to US$0.3, p=0.06). Among infants who sought care it was US$8.5 (95% CI −US$17.0 to −US$0.03, p=0.03) lower in the ciKMC arm compared with the control arm. The HR for impoverishment due to healthcare seeking was 0.56 (95% CI 0.36 to 0.89, p=0.01) and it was 0.91 (95% CI 0.74 to 1.12, p=0.37) for CHE.
Conclusion ciKMC can substantially reduce the cost of care seeking and the risk of impoverishment for households. Our findings show that supporting mothers to provide KMC to low birthweight infants at home, in addition to reducing early infant mortality, may provide financial risk protection.
Trial registration number CTRI/2017/10/010114
- Child health
- Health economics
- Health policy
Data availability statement
Data are available on reasonable request. The dataset pertaining to the results reported in the manuscript will be made available to others only for health and medical research, subject to constraints of the consent under which the data were collected. Deidentified individual participant data will be made available along with the data dictionary, study protocol and informed consent form. Data will be available beginning 12 months and ending 5 years after publication of this article. Requests for data should be made to TSC (tarun.choudhary@sas.org.in). The requester should provide a methodologically sound secondary research proposal, approved by an independent review committee. The requester must be able to show their ability to carry out the proposed use of the requested dataset through their peer review publications and declare conflicts of interest in relation to the requested dataset and their funding sources. The authors reserve the right to refuse sharing of data in the face of potential adversarial conflicts of interest. A Data Sharing Agreement that meets the data sharing requirements of the Society for Applied Studies (New Delhi, India) and Centre for International Health, University of Bergen (Norway) will be signed with the data requester. Data must only be used for the purpose described in the secondary research proposal as further stipulated in the Data Sharing Agreement. Data will be transferred only to requesters named in the original proposal and as specified in the relevant data sharing agreement.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Kangaroo mother care initiated in community settings (ciKMC) reduces neonatal and early infant mortality among low birthweight babies.
Evidence is lacking on the impact of ciKMC on financial risk protection for households.
WHAT THIS STUDY ADDS
This is the first study to assess the impact of kangaroo mother care on healthcare out of pocket expenditure, catastrophic healthcare expenditure and impoverishment of household due to healthcare seeking for low birthweight infants.
We show that ciKMC can substantially reduce the cost of care seeking and the risk of impoverishment for households.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our findings support the inclusion and scale-up of kangaroo mother care in communities with high burden of low birth weight.
Inclusion of non-health outcomes in randomised trials should be considered, as this evidence is important for priority setting and benefit package design.
Introduction
In 2020, 2.4 million children died worldwide within the first month of life; an estimated 4 out of 5 of them in low-income and middle-income countries (LMICs).1 Interventions which can reduce avoidable mortality exist, however, coverage and quality for such interventions remain modest in many LMICs.2 Earlier, we have shown that kangaroo mother care initiated in community settings (community initiated KMC or ciKMC) can substantially reduce early infant mortality (HR 0.75, 95% CI 0.60 to 0.93, p=0.01) and has beneficial equity impact.3 4 Poverty is a major barrier in accessing healthcare in LMICs. Clinicians often find it difficult to provide optimal care due to financial constraints in the households.5 Disease and healthcare seeking may plunge a family into poverty since much of health budgets in LMICs are funded by direct out-of-pocket expenditure (OOPE). High-quality evidence on interventions which can prevent impoverishment are needed. Health benefits should be supplemented with social welfare outcomes in randomised controlled trials (RCTs) of healthcare interventions.6
The RCT methodology is ideal for assessing the impact of healthcare on household economy. Still few, if any, RCTs have used impoverishment and catastrophic healthcare expenditure (CHE) as study outcomes to assess the impact of interventions on financial risk protection.7 Modelling studies have indicated that some health interventions provide dual benefits in reducing disease incidence and disease severity, which results in fewer healthcare visits and thereby reduced costs for families.8 9 An RCT design could be used to provide direct evidence for the extent to which an intervention can provide financial risk protection in addition to health benefits.
In 2019, India accounted for approximately one-fourth of all neonatal deaths globally.10 In 2020, the health expenditure in India was estimated to be US$73 per capita, of which 65% were OOPE, a regressive method of health financing.11 Healthcare seeking in India, therefore, imposes a substantial financial cost for households. Each year, between 14% and 44% of households in India experience CHE, defined as healthcare OOPE above a specified level of the total household expenditure (THE) (typically 10%) and around 5% of households become impoverished.12 13 High OOPE for care seeking of sick infants is a major barrier to accessing healthcare, especially among poor families.13–15 Health systems should ensure that people have access to services which improve health but without detrimental impact on other aspects of well-being. Financial risk protection is an integral component of universal health coverage and an important health policy goal. CHE and impoverishment due to healthcare seeking, which are measures of financial risk, are indicators for monitoring sustainable development goals targets.11 Protection from financial hardships can be ensured through a well-functioning social health insurance or by tax-financed health systems.16 However, such health financing mechanisms are currently not available in most resource constrained settings.7 Hence, assessing the financial risk protection from standard healthcare interventions is particularly important in countries with poorly functioning welfare systems.
To our knowledge, this is the first RCT which directly assesses the impact of a health intervention on financial risk protection. More specifically, we evaluated the effect of ciKMC on healthcare OOPE, the risk of CHE and impoverishment during the first half of infancy, among low birthweight (LBW) infants in the Indian state of Haryana.
Methods
Study design, setting and participants
This unmasked, parallel arm individually randomised superiority trial was a preplanned substudy of a randomised trial, which extended data capture, enabling the assessment of the impact of ciKMC on financial risk protection.3 The trial was undertaken to estimate the effect of ciKMC on postenrolment neonatal and early infant mortality among infants who weighed between 1500 and 2250 g within 72 hours after birth.3 It was conducted in rural and semiurban, low-income populations of Faridabad and Palwal districts in the state of Haryana, India from July 2015 to October 2018.3 17 In the substudy, which collected data on healthcare expenditures and household consumption, infants were enrolled from September 2017 to October 2018.
A written individual informed consent was obtained prior to enrolment. The consent form was translated into the local language and administered by a trained interviewer. For those unable to read, it was read out by the worker administering consent. In those unable to sign, a thumb imprint witnessed and countersigned by an impartial literate witness was taken. We ensured equitable authorship in the publication (online supplemental appendix S1 – Reflexivity Statement).
Supplemental material
Patient and public involvement
In the formative research conducted prior to trial initiation, qualitative research methods such as in-depth interviews, focus group discussions and observations were used to ascertain practices around birth and to assess the feasibility and acceptability of ciKMC. A prototype intervention package and delivery strategy were designed, and household trials were conducted to ascertain adoption rates among mothers of LBW babies.
Randomisation and masking
We randomly assigned LBW infants to either the ciKMC arm or the control arm in the trial. Infants from the same household were allocated to the ciKMC arm if a previously enrolled infant from the household had been allocated to the ciKMC arm; otherwise, assignment was done as per the randomisation sequence. The sequence was prepared by an independent statistician not involved with other trial activities using random permuted blocks of variable size. Detailed methods of the ciKMC trial have been published earlier.3 17
Procedures
The intervention was promotion of and support for KMC defined as prolonged skin-to-skin contact between neonates and their mothers or surrogates for as long as possible during the day and night, and exclusive breast feeding. An intervention delivery team made nine home visits in the ciKMC arm to initiate, promote and support KMC during the first 28 days of life. During the visits, the worker observed the mother practising KMC, enquired about skin-to-skin contact and breast feeding in the preceding 24-hour period and supported the mother and family to solve any problems or overcome barriers to effective KMC. No intervention was given to the control families but families in both the ciKMC and control arms of the trial continued to receive routine home-based care from the public health system.
Due to the nature of the intervention, mothers were not masked to allocation; however, efforts were made to keep the independent outcome assessors unaware of the intervention allocation and the study hypothesis. We collected information on socioeconomic and demographic variables for the household, mother, and father of the study infant as well as on different goods and services consumed by the members of the household during enrolment (table 1). Household consumption of goods and services is an important reflection of economic well-being and thereby of living standards. For infants who had received medical attention, information on healthcare OOPE related to each event of outpatient and inpatient care seeking were collected at the 28-day, 90-day and 180-day visits (table 1). A limited number of expenditure items were included in the questionnaire and the recall period was 4 weeks for the visit on 28th day of life and 2 weeks for visits on 90th and 180th day of life. The short recall period was intended to improve accuracy, as recommended in surveys on household economy.18
Items for which household consumption and cost of care seeking data were collected
Study outcomes
The primary outcomes of the study were healthcare OOPE, CHE and impoverishment of the household due to healthcare expenditure for the study infant. Secondary outcomes were THE, household healthcare OOPE for an episode of non-severe (ie, outpatient care) or severe (ie, in-patient care) illness and healthcare utilisation.
All the costs associated with care seeking during each visit (table 1) to a healthcare provider were considered an event of care seeking. Hence, a single episode of illness could lead to multiple events of care seeking if care was sought from different care providers or from a single provider multiple time. Financial risk protection was measured in two ways. The first considered the risk of falling below the national poverty line due to healthcare OOPE for households which were above the poverty line at baseline, and the second considered the risk of experiencing CHE from enrolment till 6 months of infant age. Healthcare expenditures were considered to be catastrophic at three different levels: ≥10% of THE, ≥25% of THE and ≥40% of the non-food expenditures as suggested by the World Bank and WHO.19 We also assessed the distribution of gross THE, and net household expenditure in the study arms. Net household expenditure was calculated by subtracting healthcare OOPE from THE. Because we only had data on healthcare expenditures for eight out of the 26 weeks of follow-up, total household consumption was calculated for a duration of 8 weeks, based on the items listed in table 1. We used the Indian urban threshold of US$0.72 per capita per day in total household consumption to calculate the number of people falling below the poverty line.20
Sample size
Literature suggests that CHE for different health conditions in India range between 14% and 44% and these estimates are sensitive to the source of care seeking (public vs private and inpatient vs outpatient).21 Data specific to CHE for healthcare seeking among families with LBW infants less than 6 months of age for the study setting was unavailable. Since we included both public and private sources of care seeking and included both inpatient and outpatient care seeking, we used a conservative CHE estimate of 15% for our control arm.15 To be able to estimate a minimum 25% relative risk reduction in CHE with ciKMC promotion and support, with a two-sided alpha of 0.05 and 90% power, we needed a minimum sample size of 1702 infants in each trial arm. We used a two-proportion test for calculating the sample size using the above assumptions.22 However, because the background CHE estimate was conservative and to enhance statistical precision of our estimates, we continued to enrol participants until the enrolment in the primary trial was completed.
Statistical analysis
We used Stata V.16.1 (StataCorp) and R statistical environment for all analyses. We summarised baseline characteristics using percentages, means with SD and median with IQR. We show the distribution of THE and net household expenditure in a Pen’s parade, which is generally used to show the income distribution in a population.19 We used generalised linear models of the Gaussian family with an identity link to estimate the mean difference with 95% CIs in healthcare OOPE. We calculated the effect of ciKMC promotion and support on CHE and impoverishment due to care seeking using Cox regression models to estimate HRs with 95% CIs. We used robust SEs to account for clustering due to more than one infant within a single household.23 Estimates for inpatient, outpatient and total costs were generated separately for all infants as well as for the infants who had at least one event of care seeking. Costs are reported in 2017 US$, with a conversion rate US$1=INR65.12.24
Results
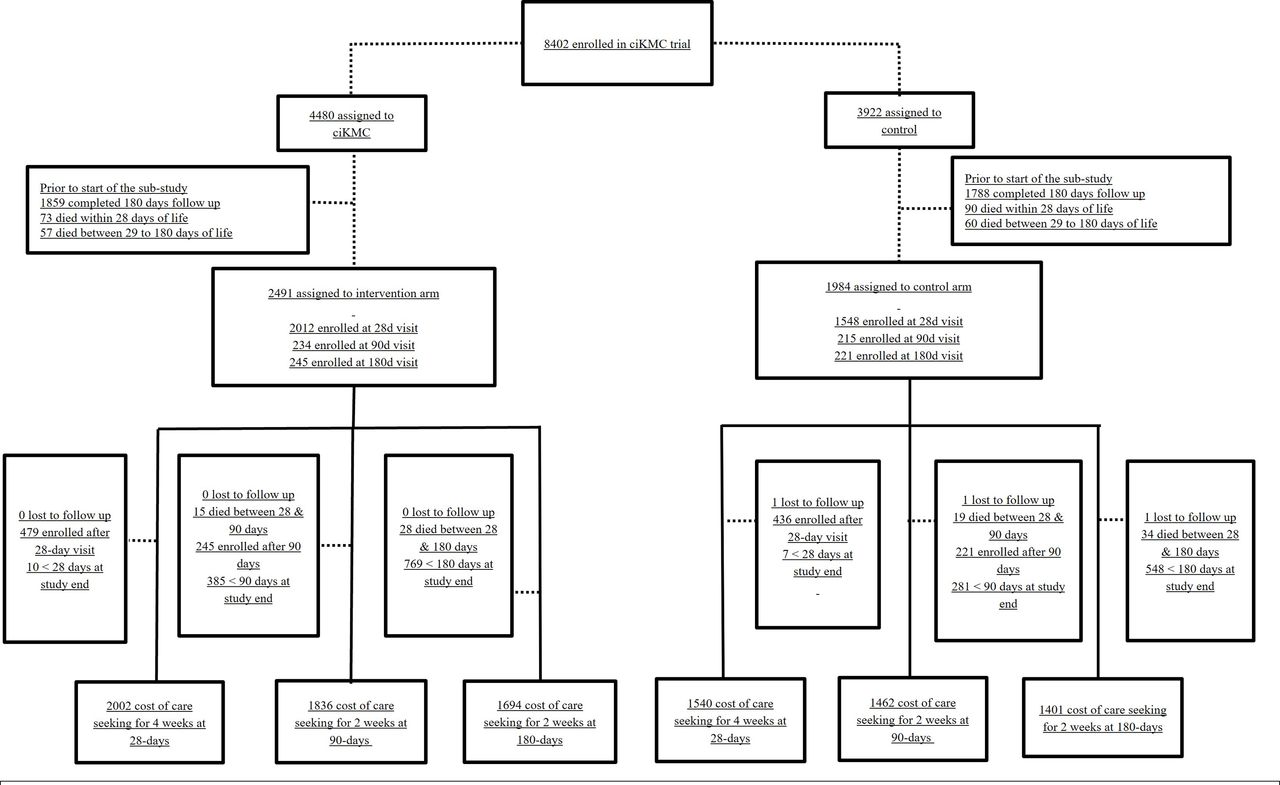
Between September 2017 and Oct 2018, 4475 infants were enrolled into the study. The infants were randomly assigned to either the ciKMC (n=2491) or control (n=1984) arm (figure 1). Table 2 shows the baseline characteristics of the infants, their mothers and their families. Randomisation effectively balanced important baseline characteristics of the study participants.

Trial profile. Note: The data safety and monitoring board stopped the trial before the last enrolled child could complete 180 days follow-up. Hence, at the time the trial ended, we missed eight weeks of information on care seeking expenditures if the child was younger than 28 days, 4 weeks if the child was younger than 90 days, and 2 weeks if the child age was younger than 180 days old. ciKMC, Kangaroo Mother Care initiated in community setting.
Baseline characteristics of the participants
Tables 3 and 4 show the impact of ciKMC on healthcare OOPE, and the HR of CHE and impoverishment of families due to care seeking for study infants. During the 8 weeks when patient cost data were available, the average healthcare OOPE was US$5.54 (95% CI −11.38 to 0.30) lower in the ciKMC arm compared with the control arm. The percentage of households experiencing CHE was high during the first 180 days of life, ranging between 4.7% and 7.9% in the control arm and between 3.7% and 7.2% in the intervention arm at different cut-offs. The risk of CHE was only 9% (HR 0.91) to 21% (HR 0.79) lower in the ciKMC arm as compared with the control arm for the different cut-offs used. ciKMC promotion and support caused a reduction in the risk of impoverishment due to healthcare expenditures of 44% (HR 0.56; 95% CI 0.36 to 0.89).
Healthcare OOPE in the first 180 days of life in both arms
Catastrophic HCE at various cut-offs and poverty impact of ciKMC in the first 180 days of life in both arms
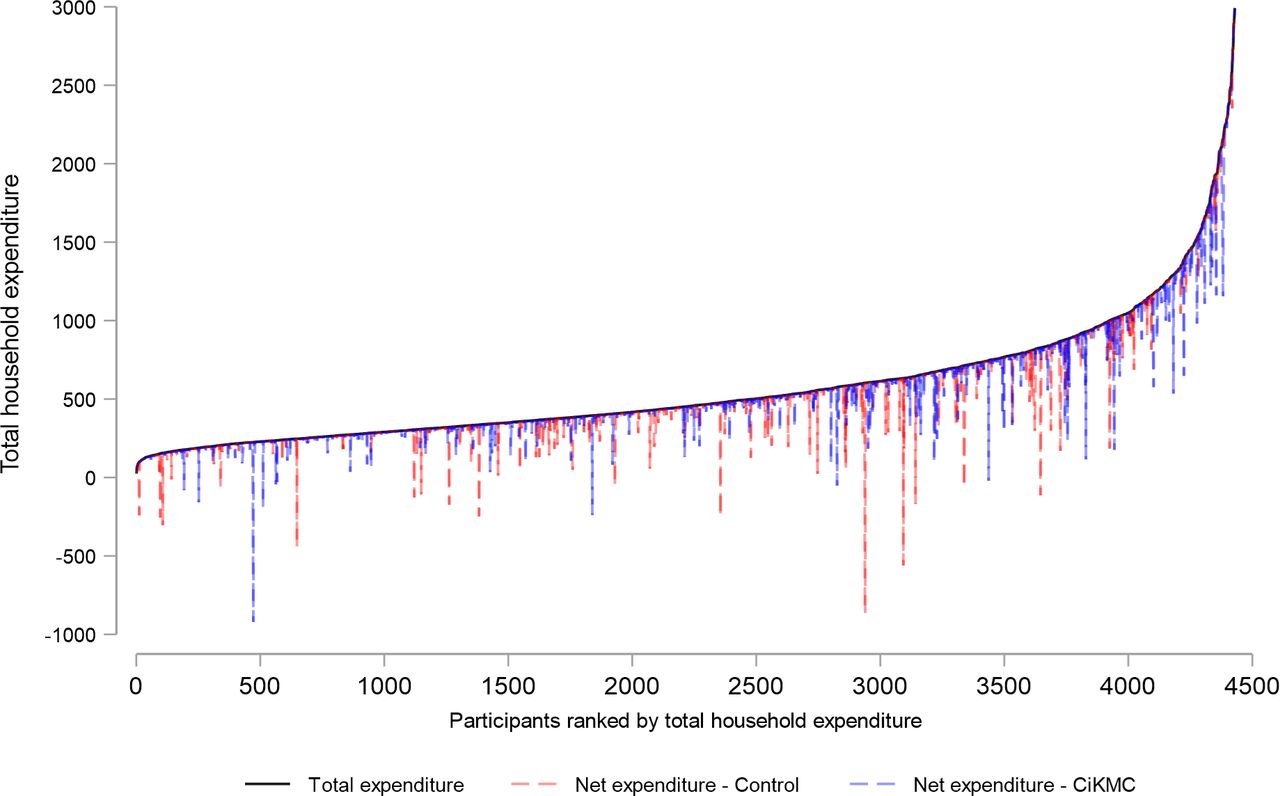
Figure 2 shows the distribution of THE and the net of healthcare OOPE, which was derived by subtracting healthcare OOPE (drop lines) from THE in the two trial arms. The plot shows participants ranked based on THE and the net of healthcare OOPE through droplines. Although participants across the whole gradient have healthcare expenses, the ones on the left-hand side of the distribution, that is, the marginalised population closer to poverty line, have higher risks of impoverishment or being further pushed into poverty due to healthcare seeking. Note that we see from figure 2 that some households have extremely high healthcare OOPE (seen by the long drop lines). These high expenses were more common among those seeking inpatient care and are presented in greater detail in table 5.

{kind=link}
{kind=link}
Pen’s parade graph of the distribution of total household expenditure and the net of healthcare OOPE for the ciKMC and control arm households. ciKMC, Kangaroo Mother Care initiated in community setting; OOPE, out-of-pocket expenditures.
Mean and mean difference (95% CI) in inpatient and outpatient healthcare OOPE; inpatient and outpatient care seeking event per infant and average time to care seeking per infant in the first 180 days of life in the study arms
As seen in table 5, the average number of out-patient care seeking events per infant was 0.07 or 9% (0.07/0.74) lower in the ciKMC arm than the control arm, whereas the number of inpatient care-seeking episodes per infant were similar. Importantly, families in the ciKMC arm sought care 3.5 hours earlier compared with the families in the control arm. The families who sought inpatient care spent an average of US$79 in the ciKMC as compared with US$106 in the control arm, suggesting that ciKMC induced a US$27 or 25% (26.9/106.0) reduction in inpatient cost per infant.
Discussion
In the current analysis, we showed that supporting mothers of LBW infants (1500–2250 g) to provide ciKMC had two important financial benefits to households: reduced risk of impoverishment due to care seeking for the infant and reduction in healthcare OOPE, especially for inpatient visits. Although estimated with limited statistical precision, the risk of catastrophic healthcare OOPE tended to be lower in the ciKMC arm at all thresholds examined.
Healthcare OOPE for study infants seeking inpatient care were 25% lower in the intervention group leading to considerable savings of family resources. This translates to a 12% increase in the median household consumption of US$228 that could be used to meet other household needs. ciKMC also protected families of study infants from the risk of impoverishment due to healthcare OOPE. This is particularly important in settings like India where coverage of public health insurance is low and around 65% of all total healthcare is financed through OOPE. Results from this RCT, therefore, provides important economic arguments for strengthening KMC to LBW infants in India and similar settings.
Financial risk protection of healthcare programmes and interventions have so far been assessed in modelling studies or data from cross-sectional and cohort studies.9 25–28 This study demonstrates, for the first time, that individual-level data from an RCT can be used to estimate the financial risk protection of an intervention. An RCT provides an excellent platform for including non-health outcomes in addition to the traditional clinical endpoints as the estimates are less likely to be unbiased.29 30 The true benefit of an intervention is best estimated when both health and non-health outcomes are taken into consideration. Using RCT methodology to provide better assessment of financial risk protection is relevant when assessing health technologies targeting conditions with high financial risk. Such RCTs may aid policy makers in assigning weight to poverty reduction and financial risk protection when setting priority between various health interventions for inclusion in national programmes and benefit packages.31 32
Household cost savings due to ciKMC, especially for vulnerable households at risk of outright poverty, can be attributed to several factors. We found that ciKMC reduced the number of illness episodes for which care was sought and led to early care seeking. These are particularly relevant for understanding how ciKMC reduces household healthcare expenses. The progression of illness is much faster in early life, especially among infants. Illness is also likely to be less severe in the early stages. Prompt care seeking for illness, as seen in the ciKMC arm, can therefore have both a survival and a cost reducing effect, especially by reducing the risk of hospitalisation. ciKMC has been shown to reduce neonatal and early infant mortality.3 Our analyses showed additional non-health benefits in the form of reduced healthcare OOPE and lower risk of impoverishment, further supporting the inclusion of ciKMC in the national health programme in India.
Globally, there are few healthcare interventions that provide as much health benefits per US$ invested as KMC initiated in hospital settings.33 34 Ruiz et al, reported that baseline case incremental cost utility ratio as cost saving (−US$1546), showing that KMC was dominant that is, less expensive, and more effective than standard care, and it was far below the willingness to pay threshold for Columbia.34 Lowson et al, concluded that the benefit to cost ratio of KMC ranged between 7.4:1 and 21.7:1 that is, the net return on investment was positive.33
Our findings should be interpreted considering the following strengths. We collected detailed data on the cost of care seeking including inpatient and outpatient costs. Data on household consumption was collected using a limited number of different items in the questionnaire and short recall periods to ensure better data quality. The large sample size, balanced randomisation and negligible lost to follow-up indicate a well-conducted RCT. Our estimates of household consumption are similar to previous estimates from the study setting.35 Nonetheless, our study suffers from the limitation that we only collected data for 8 out of the 26 weeks of follow-up. Assuming that the care-seeking patterns and associated costs for the 26-week follow-up period were similar to the 8-week sampling period, the actual savings would be higher than our estimates. Due to the nature of the intervention, it was not possible to mask mothers to allocation of the intervention.
Conclusion
ciKMC can substantially reduce the cost of care seeking and the risk of impoverishment for households. Our findings show that supporting mothers at home to provide KMC to LBW infants may, in addition to enhancing infant survival, provide financial risk protection.
Data availability statement
Data are available on reasonable request. The dataset pertaining to the results reported in the manuscript will be made available to others only for health and medical research, subject to constraints of the consent under which the data were collected. Deidentified individual participant data will be made available along with the data dictionary, study protocol and informed consent form. Data will be available beginning 12 months and ending 5 years after publication of this article. Requests for data should be made to TSC (tarun.choudhary@sas.org.in). The requester should provide a methodologically sound secondary research proposal, approved by an independent review committee. The requester must be able to show their ability to carry out the proposed use of the requested dataset through their peer review publications and declare conflicts of interest in relation to the requested dataset and their funding sources. The authors reserve the right to refuse sharing of data in the face of potential adversarial conflicts of interest. A Data Sharing Agreement that meets the data sharing requirements of the Society for Applied Studies (New Delhi, India) and Centre for International Health, University of Bergen (Norway) will be signed with the data requester. Data must only be used for the purpose described in the secondary research proposal as further stipulated in the Data Sharing Agreement. Data will be transferred only to requesters named in the original proposal and as specified in the relevant data sharing agreement.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Institutional Ethics Committee, Society for Applied StudiesReference No—SAS/ERC/PEIE/2017. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We acknowledge the contribution and support of the mothers and families of participating children. We acknowledge the hard work of all the data collectors and study team. The Society for Applied Studies acknowledges the core support provided by the Department of Maternal, Newborn, Child and Adolescent Health, WHO, Geneva (WHO Collaborating Centre IND‐158); the Centre for Intervention Science in Maternal and Child Health, Centre for International Health, University of Bergen (Norway); and Knowledge Integration and Translational Platform (KnIT), a Grand Challenges Initiative of the Biotechnology Industry Research Assistance Council (BIRAC), Department of Biotechnology, Government of India and Bill & Melinda Gates Foundation (USA).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Valery Ridde
Twitter @tarunschoudhary, @DoctorHaaland, @KA_Johansson
Contributors All authors contributed substantially to the conception or design of the study or to the data acquisition, analysis or interpretation. TSC, SM and ST were responsible for the day-to-day implementation of the study, data management and analysis. TSC, OH, HS and KAJ performed the statistical analysis. TSC, OFN, OH, KAJ, HS and SM drafted the manuscript. NB, RB, JM, MKB and HS provided technical support, monitoring, and coordination for the trial. All authors critically revised the manuscript for important intellectual content. TSC is the guarantor and corresponding author. He attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. The manuscript was reviewed and has final approval from all authors.
Funding A grant for the study was received from the Norwegian Research Council through its Centres of Excellence scheme and the University of Bergen to the Centre of Intervention Science in Maternal and Child Health (project No. 223269) and Equifinance (project no. 316354).
Disclaimer The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.