Article Text

Abstract
The history of the Maasai tribe in northern Tanzania is characterised by marginalisation, discrimination and political subjugation. Inequities, enacted through power relations, influence healthcare access, practices and outcomes among the Maasai. Cultural safety and ethical space provide lenses into social, political and historical influences on access to care, helping to understand the realities of historically marginalised populations such as the Maasai, and responses to health services. This study aims to examine Maasai experiences of accessing and uptake of health services within a postcolonial discourse in Tanzania. In an ethnographic study examining access and perceptions of healthcare services in Maasai communities, lead authors conducted participant observations and at health facilities to document experiences. Household interviews, a group oral history and interviews with NGOs working with Maasai communities, contributed to the data analysed. Inductive thematic analysis was used to understand healthcare experiences within a framework of cultural safety and ethical space. Despite trust in biomedicine, Maasai people have a strong desire for health services with particular characteristics. Quality of care, including facilities and diagnostics available and used, was important. A sense of fairness was a determinant in respecting services including ‘first come first serve’ system and transparency when unable to treat a condition. Trust in health services was also influenced by personal interactions with health workers, including provision of health information provided to patients and instances of being mistreated. These findings offer an understanding of ways in which spaces of healthcare can be more approachable and trusted by Maasai. Incorporating cultural safety and ethical spaces to understand healthcare access can help to reduce the power imbalance possibly resulting from a history of marginalisation. This can inform development of culturally appropriate programmes, used to educate healthcare professionals and advocate for improved healthcare services for marginalised groups.
- Health services research
- Public Health
- Qualitative study
Data availability statement
Data are available on reasonable request. Data cannot be shared publicly without a request for a data transfer agreement from the Tanzania national ethics committee. Individual requests for transfer of data can be directed to National Institute for Medical Research in Tanzania (contact via ethics@nimr.or. tz) for researchers who meet the criteria for access to confidential data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The Maasai tribe of Tanzania are particularly disadvantaged in their health status. Considering a history of social and political subjugation, trust and access to health services can be a result of how Maasai have been treated historically. Indigenous peoples are overlooked in healthcare policy and practice.
WHAT THIS STUDY ADDS
This study used a framework of cultural safety and ethical space to explore historical, social and political influences impacting Maasai experiences with healthcare and interpersonal relationships in Tanzania. Quality of care, facilities, diagnostics and a sense of fairness are determinants in respecting services. This study highlights the impact of trust, power and language on accessing and uptake of health services resulting from colonialism.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These results demonstrate a need to involve Maasai and other marginalised groups in defining their needs for cultural safety in healthcare settings. This can inform development of culturally appropriate health programmes for these communities and inform policy to incorporate cultural safety into training of healthcare professionals.
Introduction
Since the turn of the 20th century, the Maasai, a traditional pastoralist tribe in East Africa, have encountered social and political subjugation. The Maasai tribe and similar tribes who share the same language have settled in parts of Kenya and Tanzania, having different historical, political and socioeconomic influences. This research focuses on Maasai in Northern Tanzania.
In the early 1900s, periods of colonial rule by the Germans followed by the British, led to a land shortage for the Maasai of Tanzania. Land tenure policies, many of which still exist today, were an effort to consolidate and isolate the Maasai people and their cattle into designated areas and restrict their movement and interactions outside those areas.1–7 Land tenure policies were motivated by efforts to establish and protect conservation areas and national parks in Tanzania and further to protect revenue generating from European trophy hunting. They were also a response to British colonialists efforts to capitalise on what they saw as economic benefits from the pastoralists.8 9 Among the Maasai, resistance to such policies led to avoidance of cattle inoculations, circumventing cattle quarantine restrictions and disregarding restrictions on their movement in and out of areas.8–11 This marginalisation and power imbalance wove into many facets of life for Maasai people carrying into the present, in which Tanzanian society postindependence has redefined local norms and shaped social structures including healthcare delivery and access.12
Today, land disputes continue to complicate the livelihoods of Maasai and builds on a historical sense of marginalisation and cultural discrimination. The lack of health facilities and schools in their communities, poor access to health services in urban settings partly due to language barriers and the different views on their ‘development’ held by government and international donors have shaped access to opportunity, economic conditions and overall health of Maasai.13
The Maasai originated in what is today Sudan and the lower Nile Valley and slowly migrated south along the Rift Valley to Tanzania.3 Although Maasai are 1 of around 120 ethnic groups in Tanzania14 of which it can be argued are all indigenous, the focus on Maasai as ‘indigenous’ for this analysis is the maintenance of a way of life and a history of social and political marginalisation. Indigenous peoples conform with social, economic and cultural customs that are sharply distinct of dominant groups. There is a lack of control to preserve traditions through their political position and policies from imposed cultural hegemony.15 We argue that Maasai people are similar to indigenous groups in North America, New Zealand and Australia with respect to the value of upholding historical traditions and their struggles to maintain a particular way of life.
Access to healthcare
While healthcare delivery to rural settings in Tanzania has improved in recent years, there has been little attention to tailoring services for marginalised communities, including Maasai.16–18 Poverty and poor healthcare exist among other ethnic groups in Tanzania, yet the Maasai are particularly disadvantaged with regard to zoonotic diseases,19–21 antimicrobial resistance,22–24 women’s health25–28 and nutrition.16 29 30 In comparing the health status of five ethnic groups of northern Tanzania,16 in which poverty exists in all groups, the Maasai were the most disadvantaged in regard to child nutritional status and disease compared with the Rangi, Sukuma, Meru and mixed ethnicities. Food insecurity was severe and vaccination coverage the lowest among the Maasai. Poor health status among the Maasai people may be linked to reduced access to healthcare, access to knowledge and poor health seeking behaviours.17 Trust and access to health services can be a result of how groups of people have been treated or are seen by others. The most common reasons for dissatisfaction with health services in Tanzania include long waiting times; only brief encounters with medical staff; negative attitudes of staff towards patients; feelings of confusion and being alone in an unfamiliar environment; and prescribed medication with no explanation of the cause of illness.31–33 Consequently, such experiences may contribute towards a level of mistrust in health systems, particularly among marginalised groups.
In considering the Maasai’s access to healthcare, we argue that low uptake of the formalised healthcare system among Maasai people is linked to blame for their ‘culture’ and for health services not being aligned with their social norms. Although the shifting concept and definition of ‘culture’ is highly debated,34–36 culture is a multidimensional phenomenon that encompasses processes, products and results of human activity, material and spiritual, transmitted from generation to generation in a non-biological way.34 Yet the focus of culture as only external, differentiated societies and labelled Maasai as ‘primitive’, ‘backwards’ or ‘different’. Culture is a problematic concept and ways in which it is negatively deployed, results in indigenous groups being blamed for their social norms. Ferguson37 argues that rather than cultural inferiority, inequities should be understood in terms of political, economic inequality or a result of hierarchical relations.
Health systems are dominated by values, procedures and processes often not aligned with and less inclusive of marginalised populations. Barriers encountered by Maasai people when accessing health services are rooted in a historical, political context. This impact on the relationship between the health system and Maasai community has not been well explored by researchers. These inequities are enacted through power relations and influence healthcare access, practices and outcomes among this community.
Postcolonialism
The definition of postcolonial varies and is dependent on time periods, geographical context and the experiences of colonialism, past and present. In Tanzania, it is the way in which culture, ethnicity and race have been constructed and experiences of oppression and resistance as a result of German and British colonial practices.12 38 Drawing on Smye and Browne,39 McConaghy describes post-colonial as a time for back and forth reflection, on ideas of the past, solutions for today and the structures that create them.
Referred to as ‘The Disaster’ from 1884 to 1994 outbreaks of bovine diseases wiped out 95% of cattle in East Africa.40 41 Introduced diseases such as smallpox and leishmaniasis coupled with famine wiped out two thirds of the Maasai population.40 One of the results of their reduced population was a reduction in the practice of traditional ecological control measures and increase in tsetse flies and a rinderpest epidemic among wildlife, decreasing populations among some species while creating resistance among others. This coincided with the start of German rule of Tanganyika (name given to mainland Tanzania pre-independence) that was formalised in 1890 by the Anglo-German Agreement (Hodgson 1999). German colonialists were confronted with an environment scarcely populated by people and wildlife impacted by rinderpest, setting ‘a benchmark by which wildlife conservation has been judged ever since’.9 Despite Maasai playing a significant role in ecological balance, the German colonial government assumed the Maasai people and their cattle were incompatible with the landscape. This initiated the separation of wildlife conservation, hunting and pastoralism and the implementation of practices of state rule and discriminatory policies against Maasai.
The German administration imposed direct rule and established a system of monitoring and controlling Maasai raiding and movement.8 41 Germans allied with the Maasai’s neighbouring tribe of Kilimanjaro, the Chagga, to defend against Maasai raids of Chagga settlements for their cattle. The German administration formed a Maasai Reserve to consolidate the ethnic group to make way for European settlement and cutting them off from important trade opportunities and critical grazing areas.8 41
These practices were later continued and expanded by the British colonial government who took over Tanganyika informally in 1915 and formally in 1920 under a League of Nations mandate. In 1929, central Serengeti became a game reserve and in 1951, a national park, moving Maasai communities to Ngorongoro Conservation Area. Up to the present, further establishment of game reserves, national parks and Wildlife Management Areas in Maasai land led to evictions or restrictions on cultivation.2 42 The British set up a system of indirect rule of the Maasai, reshaping gender and age relations within their communities. Specifically, this system of government extended authority to men, particularly elder men, to hold new rights and responsibilities including collecting taxes, enforcing livestock decisions and codifying customary law.43 A plural wives tax put women in the same category as taxable property and from 1927 to 1940s, Tanganyika’s highest tax rate was paid by Maasai.43 Gendered spaces of ‘political’ and ‘domestic’ were partly attributed to the gendered nature of the British administration itself. Veterinary policies implemented under British colonial rule included a permit system for the Maasai’s movement of cattle within and outside of the reserve, quarantines for cattle to be inoculated and systems to ‘improve’ Maasai animal husbandry practices. Such livestock restrictions were a form of control over the pastoralists lifestyle and their strong social relations.2 8 11 Public health and medical services were designed and introduced by the British administration, as a system catered to protect the colonialists.44
Such colonial practices created norms of oppression that were carried over into independence by the Tanzanian government from 1961 and shaped the power imbalances between the Maasai and the state. This included further restricting access to rangeland, greatly reduced market for livestock trade and limited access to health facilities and education.2 45 A discourse of blaming Maasai for irrational pastoralism influenced state led development programmes to modernise land management, settle communities and manage resources through an introduction of villagisation, ranches and Wildlife Management Areas.2 4 7 9 Maasai epistemology of health is pluralistic incorporating biomedicine and veterinary knowledge. Current ‘livestock policies further embedded livestock and human health policies, processes and provisioning of services in separation and bordering’. (Davis et al p.546)
Today healthcare workers are not descendants of colonialists but descendants of Africans from many ethnic groups also living in Tanzania for centuries.14 Health worker’s discriminatory practices towards nomadic groups and in particular Maasai has been well documented.28 47–50 This legacy of the ethnic groups’ colonial past and neocolonial present along with globalisation has shaped the relationships between Maasai and other African Tanzanians in healthcare settings. The coloniser or oppressor, and the colonised or oppressed are fluid categories with restructuring of global capital, new information technologies and emerging thought and power relations that define the elite and the marginalised today.12 It is important to recognise the complexity of social interactions that do not lend themselves to binary distinctions. In doing so there is a danger of supporting the power imbalances aiming to be disassembled.51 52 McConaghy describes the focus as ‘An important task to better understand the specific nature of specific oppressions at specific sites: to understand current forms of oppression’ (McConaghy53 p.8). Aware of this critique, postcolonial discourse is a useful and important perspective for understanding and addressing health inequities among Maasai people.
Theory:cultural safety and ethical space
Cultural safety provides a lens to reflect on how cultural and social power dynamics impact health worker and patient relationships. Cultural safety is an approach of focusing healthcare delivery based on the experience of the patient and, in particular, the attitudes and interactions of the health professionals with whom they interact with. Culturally safe practice involves ‘actions which recognise, respect and nurture the unique cultural identify of an ethnic group and safely meets their needs, expectations and rights’.54
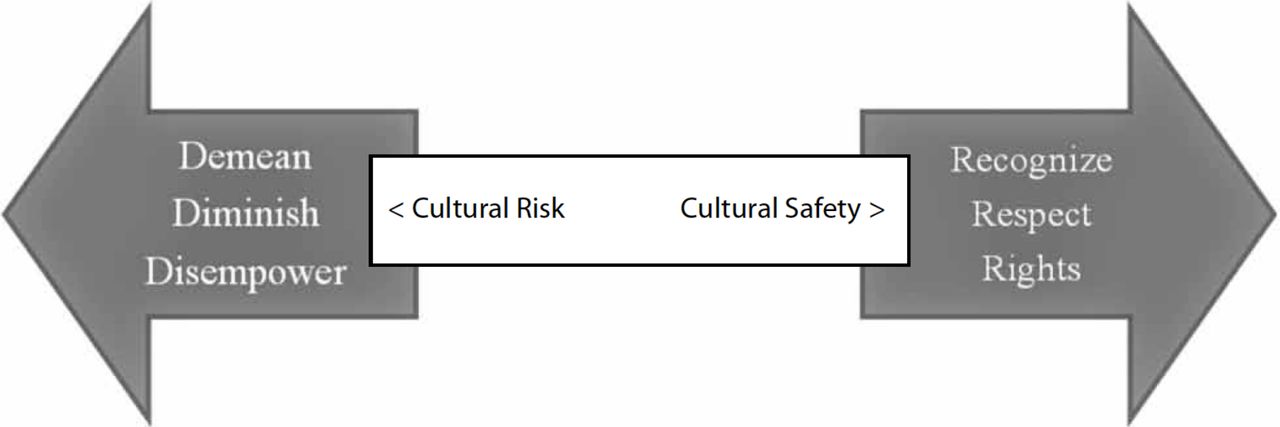
Cultural safety should not be confused with cultural competence, knowledge, awareness, understanding or sensitivity although all of these are antecedents of cultural safety.52 Cultural competence, when combined with self-reflection, is a necessary element of cultural safety that aims to shift the power imbalance so healthcare workers do not assume complete command of others’ culture.55 56 It requires mutually trusting relationships between health worker and patient. A model of cultural safety developed by Wood and Schwass54 depicts culturally unsafe practices with ‘3 D’s’ (demean, diminish, disempower) and cultural safety by ‘3 R’s’ (recognise, respect, rights) (figure 1) ‘Safety’ in this concept refers beyond avoiding physical injury and avoids any feelings of inferiority or alienation or depriving a patient of healthcare.57 Cultural safety focuses on recognising social, economic and political influences that contribute towards marginalisation of a group, community or society.
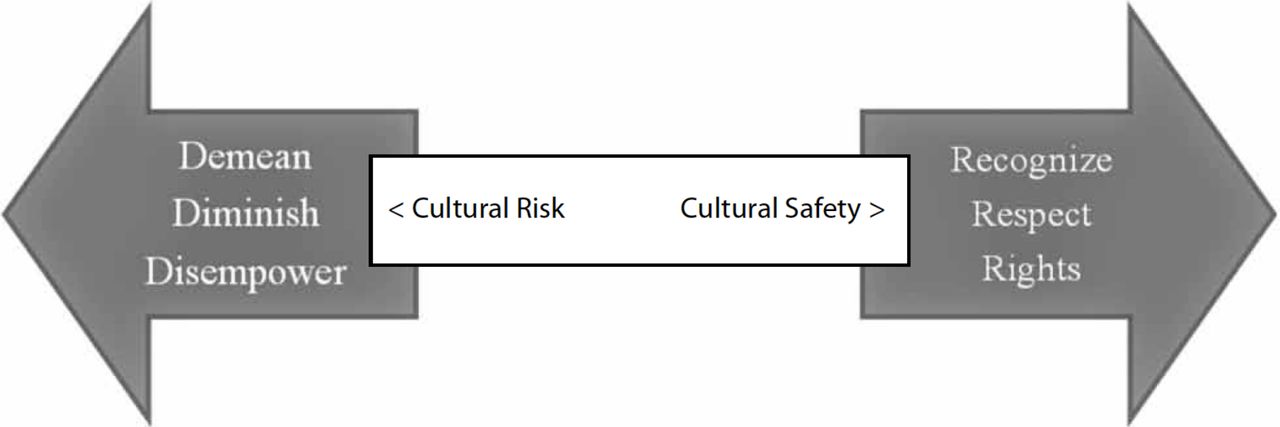
Visual representation of Wood and Schwass (1993) model of cultural safety and cultural risk.
Cultural safety emerges from critical social theory reflecting on the postcolonial period.12 38 39 The concept emerged in response to health inequities of Māori, the indigenous people of New Zealand,58 resulting from power imbalances stemming from colonialism that continue into healthcare settings today.59 60 The impact of colonisation on health inequities among indigenous peoples globally and the current poor response to the impacts on these communities by governments has been well documented.61–65 Cultural safety addresses power imbalances resulting from post-colonial discourse and the health worker patient dynamics in many settings. The ways in which cultural safety supports a shift in power in practice is dependent on the historical, social and political context and needs of a marginalised group. Cultural safety can be applied to any group who differ from that of their healthcare provider in regards to age, gender, sexual orientation, socioeconomic status and class, ethnicity, religious or spiritual beliefs or disability.66
Ethical space is a framework for guiding respectful interactions across cultural differences to mutually explore epistemologies and ontologies entering that space.67 Ethical space ‘is formed when two societies, with disparate worldviews, are poised to engage each other’.68 It moves from a monoculture in healthcare, which can inadvertently create health inequities, to listening, acknowledging and working with local knowledge and beliefs and voices of marginalised groups. The space can be simultaneously physical, social and psychological60 although more widely understood in terms of active space of process, action and energy.69 Barina70 discusses space as being value-laden and the need to assess the values produced in healthcare spaces. The application of ethical space in assessing healthcare is scarce although it has been used among indigenous groups to facilitate discussions and collaborations on healthcare71 sustainability and conservation.72 73
Through the lens of cultural safety and ethical space, against a backdrop of postcolonial discourse, we analyse how historical, social and political influences impact individual choices and decisions around healthcare and interpersonal relationships in this setting. We aim to highlight experiences of accessing and uptake of health services among Maasai people in Tanzania within a postcolonial discourse in order to facilitate transferring power to healthcare recipients.
Methods
The findings, on which this paper is based, are drawn from an ethnographic study, using non-positivist inquiry to examine experiences of access to healthcare among a Maasai community in Northern Tanzania. Non-positivism maintains that there is no single ‘true’ position, and that meaning is dependent on the context and interpretation of social actors.74 The constructivist approach to this inquiry assumes that it is meaningful to generate knowledge by making sense of realities, specifically social constructs.75 The emphasis is on introspective-investigator accounts of social contexts. The researcher examines and interprets the forces that shape and influence behaviours.76 The research was carried out by TBM and JM from September 2016 to December 2017 in various settings to understand the lived experiences of the Maasai tribe.
Data collection
Qualitative data were collected by employing a variety of methods in the larger project of ethnographic research looking at Maasai people’s experiences and perceptions of healthcare with a case study of trachoma control in Sinya Ward in Longido District. This paper will report on the methods used for this paper’s analysis (table 1).
Data collection methods
Observations
Along with a Maasai research assistant (JM), the lead author conducted participant observation in three villages in Sinya Ward of Longido District-Il Donyo, Leremeta and Endonyoemali. Observations were conducted in social settings, such as the market, people’s homes, community meetings, the community bore-holes, celebrations; in two government dispensaries; and during various medical outreach programmes. Outside of the villages, TBM and JM conducted observations in different healthcare settings in Arusha and Kilimanjaro regions, accessed by Maasai and non-Maasai patients including private and Non-governmental organization (NGO)based health facilities, a district hospital and a referral hospital to understand experiences. Observers were based in patient waiting rooms, and interactions with Maasai patients and families occurred naturally and willingly via a Maasai research assistant.
Household interviews
Household interviews were conducted with twenty randomised households in the three villages of Sinya Ward with a set of questions on experiences, perceptions and access to health services used in this analysis. Internet-based sample builder was used to randomly select two enkang from each of the 10 subvillages (www.randomizer.org) for household interviews. An enkang is a homestead or joint residential unit composed of a number of households. They are headed by one male and in a polygamous culture, each wife with her children have a hut within the boma.18 If the first randomly selected enkang was not available, the next enkang in the randomisation list was approached to participate. The interview guide consisted of open-ended questions on their experiences and perceptions of health and non-health related programmes in the community. Interviews were conducted at the enkang with both men and women present and lasted 1 hour on average.
Oral history
An oral history was recounted by elderly Maasai women to furnish an understanding of the history of medicine among the Maasai. Community leaders and Maasai research assistants advised that women are the carers in the enkang. Despite men making the final decision around healthcare seeking, men rely on and respect women’s opinions and choices. Five elders were selected using purposeful snowball sampling to assure inclusion of women estimated to be older than ninety years to allow for a richer history of medicine among Maasai. The 2-hour discussion was guided by a topic guide consisting of significant historical time points and the impact on health and medicine in the Maasai context. The venue for the discussion was under a tree near the market on a non-market day.
Semistructured household interviews and oral history were conducted in Maa, the primary language spoken by Maasai people, by a native Maa-speaking interviewer, JM, in a conversation-like manner, with TBM present for all interviews. The discussions were audio recorded and later transcribed and translated from Maa to English by JM.
NGO interviews
TBM also conducted in-depth interviews with NGOs working with Maasai communities. Purposeful sampling was used to include as many NGOs that met the criteria of supporting Maasai communities in areas of health or development. Of 14 NGOs contacted, 5 NGOs from Arusha region agreed to have a representative interviewed. The interview guide consisted of open-ended questions on their experiences and perceptions of health and non-health-related programmes in the community. This analysis includes three of those interviews in which the topic of access to healthcare was discussed. Interviews were conducted in English, lasting 90 min on average and detailed notes were taken.
Data management and analysis
Transcription of household interviews and oral history was done directly from Maa to English; some translations were corrected to ensure more understandable English while assuring meaning was not changed. Participants who were interviewed were assigned a unique identification number and data anonymised in the transcription process. Audiorecordings, transcripts and field notes were stored in a locked cabinet in the field and later in a locked office in Moshi, Tanzania. English transcripts and field notes were entered into NVivo V.11 Software. Initial interpretation included familiarisation of the data. Using a thematic content approach,77 data were first coded by lead author, TBM, and verified by author SL. Through data immersion and ongoing review and discussions on the data with Maasai research assistants throughout the ethnographic fieldwork, emerging themes were identified. Impressions and interpretation of the themes were discussed with the native-speaking interviewers and coauthors. Narrative text was applied around the constructs, and direct quotes presented are used to show dominant views of participants.
Information about the oral history was read aloud in Maa to the elderly women in a group setting. Information about the household interviews was discussed in Maa and consent obtained from the male head of the enkang. The Maa-speaking interviewer again repeated information about the interview to the entire household at the start of the interview. Written informed consent was obtained for all interviews. A witness was present for non-literate participants and signed in addition to the participant making their mark. Permission to digitally record interviews was obtained from each male head of enkang, and the elderly women for the oral history. The NGO respondents did not consent to be audio recorded and therefore detailed notes of these interviews were taken. Consent for ethnographic field observations was obtained from community leaders and members including men and women at a meeting to introduce the research in September 2016. Permission to conduct observations at health facilities was verbally granted from persons in-charge at facilities. Financial incentives were not provided rather a sign of appreciation with sugar and soap was provided to individuals and households who participated in interviews.
Patient and public involvement
Patients were not involved in this study. The fieldwork for this research was discussed with community leaders prior to entering the field and later presented to a wider community audience for feedback and inputs on research questions, design and approaches to carrying out data collection. Involvement of community leaders and members was continuous throughout fieldwork to assure recruitment approaches were respectful and appropriate. At least one community member escorted researchers in the field and assisted with introductions for interviews. Dissemination of initial study findings was conducted at a larger community meeting, and consultation with community members continued thereafter to confirm ongoing analyses. See online supplemental file 1 statement of author reflexivity.
Supplemental material
Findings
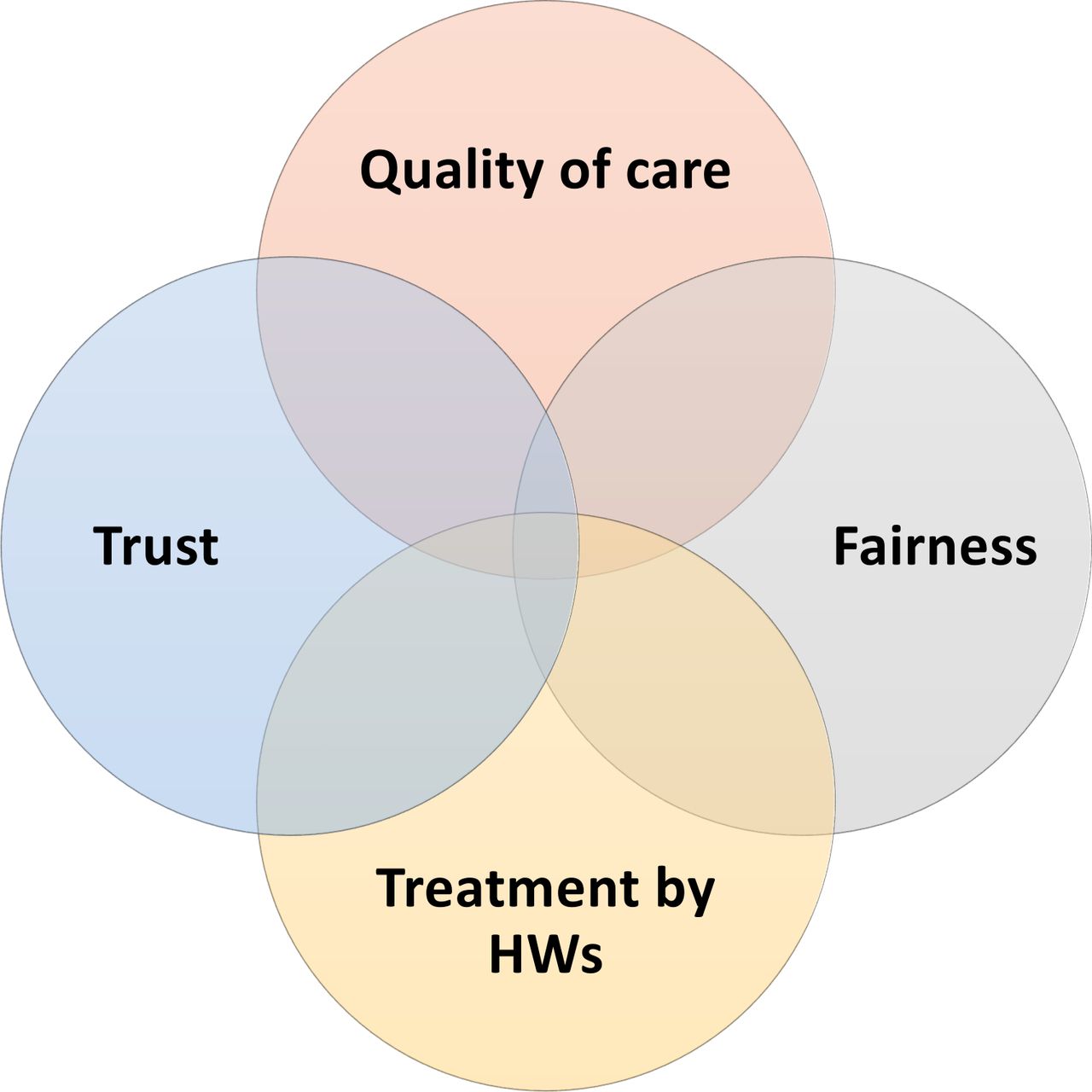
Inductive thematic analysis of Maasai people’s experiences of facilitators and barriers to accessing healthcare were categorised into four themes: fairness, personal interactions with health workers, trust and quality of care. Although presented as distinct themes, these concepts are interconnected (figure 2). What defined each theme is through the lens of the Maasai in this study. Fairness is about transparency in the processes to serve people in healthcare settings. Quality of care is the perceptions of healthcare regarding technology and thoroughness of examinations. Treatment by health workers is the health workers use of language and ethical treatment of people. Trust was determined by the level of cultural understanding and involvement of Maasai leaders in decisions and delivery of health services.

{kind=link}
{kind=link}
Facilitators and barriers to accessing health care among Maasai. HWs, healthcare workers.
Theme 1: fairness
Fairness emerged in how Maasai were being respected and treated. This came out in observations of Maasai patients in comparison with non-Maasai patients, and Maasai respondents and NGO elicited experiences. Health workers were observed giving Maasai patients and their family members less information and instructions compared with non-Maasai patients, which was interpreted as assuming Maasai people speak minimal Swahili, the national language of Tanzania, or do not have the education to understand. It was observed at facilities that Maasai patients seemed to be less prioritised than non-Maasai patients. In one case, the researcher (TBM) brought a Maasai patient to clinic and his file was the first given to the nurse. After an hour, he was still not attended to while other patients were. The researcher asked the nurse why and she replied, ‘Oh he’s with you. He will be next.’ It mattered who you are and/or who you know to receive timely and fair care. The Maasai valued a system where patients were attended to in the order in which they had arrive at the health facility.
When you go to our clinic centers there is no proper arrangement of treating people as per the time they came… In this clinic [NGO based health facility serving Maasai community], people are equal and you will be treated as per time of your attendance and not otherwise. [household interview 4–1]
Maasai respondents reported that quality health services and health workers are those that demonstrate honesty and transparency with regard to what they can treat and availability of treatment.
They [health workers in an NGO based health facility serving Maasai community] are not cheating because if they are not able to treat you they can advise you to go for referral. [household 4–1].
Yet several instances were reported in which health workers would promise things but not deliver. A common example was outreach programmes that would offer medical examinations to people and say they would return for follow-up or treatment but never returned.
Koko that was present said she used olputet [locally made tweezers] 10 min before we arrived and had used it a few times for epilation. She told us she was not around when case finders came to check a few weeks ago. There was another koko in the boma that case finders identified [as having trichiasis] and promised to come back to take her for surgery and examine this koko that missed them when they previously came. The organization never came back, and both are willing to have surgery. [Field notes]
Theme 2: personal interactions with health workers
Interactions with health workers included overall ethical treatment and respect for cultural knowledge, the setting and norms. Many Maasai respondents told stories of health workers using harsh words, insulting and even beating Maasai patients. Despite women knowing the importance of antenatal visits and following the childhood vaccination schedule, they sometimes missed visits due to migration in the dry season or competing economic priorities. When they attended clinic visits late, the nurses would punish them by hitting them, serving them last, and, in some cases, charging them money when such services are free. ‘We do follow [vaccination schedule] because there are many good things which we saw from that program and even now a days, nurses are very serious and they even hit us if we don’t follow those timetable,’ [household interview 01–1].
An NGO working in Maasai communities discussed with local government officials about the poor quality of services in Maasai communities including the language barrier, lack of medical resources and fewer health facilities. She reported that the response from government was: ‘You Maasai think you are special,’ [NGO interview 104]. There is also a perception in government facilities that Maasai people cannot afford health services resulting in delivery of inadequate care. Yet a health worker at a facility which was highly regarded by the Maasai told us, ‘Maasai are honest, we trust them. Some cannot pay on the spot but then they go home to sell cows and return to pay’ [NGO interview 103]. Workers at this same facility discussed the importance of knowing your population, their culture and the barriers.
Maasai responded more positively to health workers who involved the family in sharing information and decision making, who did not exert authority and asked permission to do procedures and treatments. One participant told the story of a female elder who had surgery without appropriate permissions of family members.
The surgical outreach team came on market day when the family were not at home and took her to the dispensary where they were performing surgery. ‘We returned from market they found her bandaged,’ the family member said, ‘They did surgery to her and even she didn’t realize they were doing surgery on her. We were not happy’. They requested that I, as a trusted outsider, to explain to the outreach programme that they should be involving local leaders and family and provide adequate information about the patient’s condition. [Field notes]
Decision making among Maasai is collective including other family members, elders and leaders. Health seeking choices are initiated by women with men making final decisions often dependent on household economics. The response to health services is linked to the extent to which the decision-making process according to their social norms is respected and allowing for time to discuss healthcare decisions with family.
In many Maasai settings, market day comes only once a week and often their only opportunity to obtain food and supplies. Market day is an economically and socially important part of their livelihoods. Several health programmes would visit communities on market day, and observations showed how Maasai people reacted bitterly that it was disruptive to their activities related to market. It also indicated to them that the programmes did not respect social norms of including village leaders in planning and decisions making to provide services. If they had, the leaders would have informed them not to come on market day.
It was observed that health workers would examine patients without explaining what they were doing and asking permission to touch patients and do a procedure. Yet often Maasai patients would ask the health worker what they were doing, what the problem is and request clarification on treatment, often to be ignored or shushed. In one case, an outreach doctor listened and respected a patient’s needs and choices and negotiated an alternative treatment.
A younger mama needed trichiasis surgery on one eye. They had come on market day to take her for surgery. She insisted that getting food for her family was more important than her eyes at the moment. The doctor instead epilated an eye lash from her and the women was pleased she didn’t need surgery. She walked away satisfied and went to market. [Field notes]
This particular doctor was well received by Maasai patients. Although she does not speak Maa, she waited for someone to translate, provided thorough information and asked permissions to examine patients. This is contrary to a lot of health workers in outreach programmes who appear to be rushed and poorly engage with the patient and their needs. It was observed in some instances, that health workers assumed a Maasai patient does not speak Swahili. They would limit the information provided to patients, talk direct to family they knew spoke Swahili, or in some cases speak poorly about the patient assuming they cannot understand. When it was apparent that a Maasai patient did not speak Swahili, health workers made little or no effort to find a translator.
Theme 3: trust
Trust is a key component to uptake of health services. We observed in health facilities that non-Maasai Tanzanians trusted nurses and doctors. They did not question clinicians nor hesitate to follow doctors’ orders. Yet Maasai tended to demonstrate more trust when they felt there was cultural respect. Respected services and outreach programmes were those that involved local leaders in the process to give trust to the community. They also responded positively to health workers and services that provide education in addition to the services. Several respondents talked about getting second opinions or in some instances of visiting several health facilities until the care ‘felt’ right.
The doctor [at one of the village dispensaries] said when the eye programme team from the regional hospital go to the village there is a better response because although they may be looking for something specific, they treat patients with other problems and counsel them. Whereas the case finders are only for trichiasis and give no attention to other eye issues or providing education. [Field notes]
It is like this, even if all doctors are good at the clinic, but the best doctor is the head who is a Maasai. This is because he is the one who is taking people for x-ray and again, he always doing two best things. The first is when patients are many he first gives seminar about the importance of having health insurance card which is active for one year. And always he insists us that after having that card to never pay any money when you come to hospital, because your card will be used to pay all bills and if there will be any doctor who will ask any money before you pay ask him for receipts. Second he is a Maa person so we can speak with him for those that don’t understand Kiswahili, [household interview 05–1]
NGOs working in Maasai communities emphasised the need to build trust. They offered suggestions such as health programmes having satellite offices close to Maasai communities for better oversight. Staff of health programmes in the cities are not aware of what is happening at the community level. It was also observed that the main offices for health service programmes would have quotas to meet, and health workers in the filed were under pressure to report numbers on delivery of services.
Additionally, there is a lack of trust in the government providing adequate services associated with the existing poor quality of services and access in some areas. One household [04–1] explained ‘the vaccination posts are few and far away from bomas. Distances are even more when we migrate [in dry season]’. There is little consideration of threats of wildlife on the journey to posts. Despite this, households plan for one woman in the enkang to take all the children for vaccinations while most other households fail to attend. Yet this household [04–1] reported there was a shortage of vaccines in the previous year. There appeared to be apprehension to trust in the services in the context of complex livelihoods.
There is only one district hospital in this region. Some villages are very remote and have no access. Yet the largest part of the government revenue comes from tourism here so why are they not helping the communities of this area? [NGO interview 103]
The study uncovered a few instances in which inadequate and/or inaccurate information was provided to Maasai patients. Few understood the purpose of outreach programmes providing screening, or drugs for prevention or treatment. Without this understanding there were refusals and lack of trust in the outreach programme. Observations revealed focus was more on achieving the programme’s target numbers rather than providing quality and appropriate services. In government facilities and some outreach health programmes, little information was given on the diagnosis, treatment and possible outcomes.
A health worker in a Maasai community said “Maasai like to have all the information before making decisions and they want respect. But once they change they are committed.” [field notes]
Theme 4: quality of care
Quality of care tended to be measured by the type of, and extent of, diagnostics done. This was not related to actual treatments provided but rather reassurance that diagnosis and treatments were based on evidence. This includes taking of vital signs and further diagnostics such as laboratory tests, ultrasound and X-rays.
The big issue in Maasai is measurement. If you take a person to the hospital and the doctor doesn’t take measurements they don’t feel they have been treated well. [household interview 5–1]
Elders explained that post- independence in Tanzania (1960s-1980s) ‘diagnostics were available at health facilities and doctors were treating patients well but it is not like this today’ [oral history]. Many respondents reported that they were treated based on symptoms. No vital signs or physical exam conducted, ‘they just look at you and give drugs’ [household interview 16–1]. This was not considered quality care.
Inadequate health resources in facilities were often reported in Maasai communities, in particular supplies of medicines, healthcare personnel, equipment and outreach programmes. Maasai respondents talked about health facilities (government, private and NGO) that they perceived as ‘excellent’ but which many had never attended, yet simply based on them having an ultrasound or x-ray machines they were highly regarded.
Discussion
This study aimed to examine experiences of accessing and uptake of health services among Maasai people within a postcolonial discourse. Overall, the findings reveal that Maasai value biomedicine and the importance of health services but that there are significant barriers to accessing services and to feeling safe in healthcare settings including lack of fairness, quality of care, treatment by health workers and trust. Similar themes of communication and trust have been identified it other studies of Maasai perceptions of health programmes.18 78 The barriers and facilitators identified do not stand alone but rather in many cases one factor might carry more weight than others in uptake of services. For example, some facilities such as government referral hospitals were well equipped with medical resources, diagnostics and staff but the healthcare workers were reported to mistreat Maasai people and many avoided such facilities. The findings indicate that many facilities and services are not safe spaces for Maasai people limiting their choices to accessing services. In understanding these factors that influence safe healthcare spaces through the lens of cultural safety and ethical space, it highlights the importance of social and political influences on everyday experiences.
Power
Overall power imbalance was a common thread in examining barriers and facilitators effecting choices in accessing services and ultimately respecting human rights. Politics and power relations have created a subaltern voice and impacted the cultural, economic and social effect on uptake of public health programmes.79 From the first interactions with ‘outsiders’, power has been a central theme in social relations with the Maasai from relocation from their land, restricted movement and agricultural policies.8 Historically power has shaped medicine in general in Tanzania80 as well as the culture of the Maasai8 43 so has it influenced their decision-making and responses to health services.16 46 Critical to establishing trust, respect, honesty and empathy is the health workers ability to deconstruct the power imbalance between the patient and themselves.81
Participants talked about shopping around for health services to find one that ‘feels right’; a search for a fair share of power in the healthcare relationship. Maasai women’s preferences for home deliveries with traditional birth attendants has been well documented and partially attributed to experiences of women in labour being turned away from health facilities and poor health worker attitudes.28 47–49 Gendered experiences can also be attributed to women having to seek permission from husbands who are in positions of power regarding material resources.82 83
Jungersen66 discussed considerations to make healthcare spaces safe for Māori in New Zealand. The context, a patient’s home, their community or a clinic; defines different ways of being and requires an awareness of verbal and non-verbal cues to navigate the healthcare setting. For example, honouring cultural protocols of introductions demonstrates a level of respect, reducing the power differential.
Trust
Trust in this study is linked to respect, kinship and sense of connectedness. It assumes power will not be used against a patient’s interest. If health workers take time with patients, announce outreach visits in advance, provide information and engage family, they would transfer some power to the patients and gain more trust. Trust is not a mental state. It is earned, built and created. Gilson84 discussed ‘particularised trust’ among groups that define themselves in opposition to other groups. Further it is easier for those with power and access to the social, economic and political system than those who are more marginalised.
The historical shift from a socialist to a neoliberal public health system in Tanzania impacted inequities in healthcare access.85 Factors important for Maasai participants to trust and access care are similar to those reported since this transition to more recently in Tanzania including availalbility of diagnostics and medicines, competent health workers and respectful communication.86–88 Trust among indigenous groups is further complicated by historical experiences of being misled and marginalised. Maasai participants discussed mistrust in vaccination programmes possibly linked to colonial veterinary and human disease control methods used to capitalise on land resources and restrict their movement.1–7 Participant references to the government prioritising tourism over healthcare resources in Maasai communities, originates from colonialists protecting lands for financial gains of trophy hunting. Since then, several national parks and conservation areas have been established on lands inhabited by Maasai, forcing them to relocate to more harsh environments. Few efforts to share the financial benefits of tourism with Maasai communities have been successful, often attributed to the lack of communication, trust and respect for the community.4 7 89
We saw particularly in outreach programmes, driven by reporting numbers, that there was no space for building trust to ultimately improve responses to such health programmes. Alternatively, trust in community health workers in Tanzania was attributed to them being embedded or ‘connected’ to the community.90 Trust can be built by including the target population in planning and delivery of programmes. In studies in Tanzania, and other countries in Africa, kinship relations or an ‘insider’ link provided a strong basis for positive, trusting relations between communities and health workers.90–92 In a study of a hard to reach community in Tanzania, men who engage in sex with other men, trustworthy health services were those that employed people from their community, have friendly staff and provide training to health workers on the lived realities of same-sex attracted men.93 Maasai respondents did not articulate the issues of (mis)trust or unsafe spaces but in many instances identify other reasons for inadequate services such as an increased population and lack of resources. This may be due to a strong sense of hope. Indigenous people’s resistance and resilience to colonialism, racism and oppression in an effort for social justice requires a strong sense of hope. First nations author, Absolon94 explained that hope affirms the possibilities, strengths and indigenous knowledge that guide a shared desire for social inclusion. Hope is made, in practice, and can be a guiding force in Maasai maintaining a traditional lifestyle.
Language
De and Richardson95 put communication and language at the top of the skillset for achieving cultural safety. Language can create a power imbalance. Beyond dialect, language includes how people use it to engage with others and creating a familiar and comfortable space. For example, this may include use of terminology not familiar to patients or not communicating diagnosis or treatment options. Transparency was often lacking and a barrier to accessing health services in this population. Swahili is the national and dominant language in Tanzania while Maa is only spoken by a few pastoralist groups including the Maasai tribe. When a health worker spoke Maa, it was more than a common dialect but reassurance of being understood culturally and gave permission for Maasai patients to be open with the healthcare worker.
In the case described in box 1, healthcare workers displayed cultural competency of Maasai social norms and further, a respect for patients. Communication facilitated a safer space for patients. It was more than speaking Maa but included a language of respect by providing information and allowing patients and families to communicate. Culturally safe occupational therapy with Māori patients in New Zealand requires a recognition that boundaries for ‘therapy’ are variable, contrary to a more compartmentalised western expectation.66 Safe practice is about healthcare providers approaching patient care with humility and openness. In a prenatal wellness programme for Canadian indigenous communities, cultural safety includes care provided in the local language, as well as integrating traditional values and understandings into prenatal care. A collaborative community partnership includes elders to explain to women prenatal care to be received through the formal health system in the context of indigenous teachings and traditions.96
‘Safe space’
Observations and informal discussions were done at an Non-governmental organization (NGO)-based health facility near to a Maasai community. This facility was always busy with Maasai patients some who had travelled hours by foot to access what they deemed a safe space for health services. One elderly woman, koko, had travelled 4 hours, 20 km on the back of a donkey while her two sons and daughter-in law accompanied her on foot until they could access public transport for another 80 km to the facility. She had a tumour in her neck that was obstructing her ability to eat and her breathing was laboured. The family had taken her to several health facilities near their home where she was not diagnosed and told there was nothing they can do. The sons said no physical or laboratory exams were done at other facilities. A few days after meeting this patient and her family, she had been diagnosed with untreatable cancer after having blood tests, a biopsy and ultrasound performed. The daughter-in-law remarked that doctors asked them a lot of questions, performed diagnostics and provided information on the diagnosis and management. Despite the diagnosis, the family was very happy with the support and care. They were relieved to get a specific diagnosis for koko, to be educated on cancer, to be supported on managing her and what was sensed as being treated as an equal. The healthcare workers at this facility were a mix of Maasai, other Tanzanians and non-Tanzanians. They displayed cultural competency of Maasai social norms and further, a respect for the patients. Communication was observed to be an important link to patients and more thorough and mutual compared with other health facilities. Communication was more than speaking Maa but included a language of respect by providing information and allowing patients to communicate. Maasai patients and their families were more open to healthcare providers at this facility than others due to the safer space created.
Applying cultural safety and ethical space
Indigenous groups as well as Maasai have complex knowledge and beliefs of health and wellness that may be seen as backwards or stigmatising them as difficult patients in healthcare settings. Central to Maasai sense of well-being is the value of land and livestock contributing to their cultural identify, security and wealth.83 Yet colonialists ideals of what the African landscape ‘should’ be, led to the use of binary terms of wilderness and domestication46 despite centuries of pastoralists living in harmony with nature.9 This sentiment highlighted by Hodge in46 describing pastoralists as ‘roaming over the landscape’ rather than being ‘proper’ inhabitants. Pastoralist knowledge and experiences of disease control in the African environment were undermined by colonialists importing western veterinary and quarantine practices.10 Maasai management of animal and human disease is embedded in spiritual beliefs and relations to nature. For example, burning grasses for tick control and use of orpul healing retreats for cleansing and healing, opposed western approaches to maintaining animal and human health.9 11 97 98
The poor understanding and respect for their beliefs and practices impedes on relationships today. According to Farmer,99 public health authorities are guilty of a social framing of disease by which suffering is attributed to culture rather than disease or poverty. This leads to a harsh judgement on marginalised communities’ ability to take responsibility and care for themselves. This ignites the resentment of colonialism and post colonialism practices and mistrust in development among marginalised populations.100 The politics of blaming vulnerable populations for the spread of disease100 exists among the Maasai. Women reported being mistreated by health workers with harsh words or even beaten when they missed vaccination visits yet there was little concern for the local context including competing economic priorities, few vaccination posts and far distances in harsh environments.
Cultural safety and ethical space provide a useful framework that allows for healthcare workers and systems to reflect on and appropriately change interactions and behaviours to avoid unsafe healthcare relationships and experiences.69 Polaschek101 emphasises that cultural safety is about recognising the position of a group in society and how they are treated and perceived, more so than the things that make a group different. In the case of the Maasai, it is the current social political subjugation most evident in land tenure policies. It is marginalisation regarding reduced access to education and health services. Cultural safety goes beyond cultural competency and focuses on sharing; ‘shared respect, shared meaning and shared knowledge and experience, of learning together with dignity and attention’.102
Ethical space could be analysed in terms of the boundaries created in the healthcare space that may be interpreted as ‘policed by gatekeepers’67 a similar historical experience for Maasai. For example, longer waiting times than non-Maasai patients, lack of information provided and mistreatment of patients were experiences reported in these spaces. Although it was not possible to assess self-reflection of healthcare workers in this study, a critical component of cultural safety, it was evident that in those health facilities that Maasai patients felt safe, there was a sense of respect for this community. Traditional practices of healing including the use of traditional medicines and rituals are well incorporated into notions of healing among Maasai.97 103 Health workers understanding, acknowledgement and incorporating indigenous knowledge or practices into the healthcare setting may contribute towards creating ethical spaces as has been done for other indigenous groups.52 66 69
New Zealand, Australia and Canada have adopted cultural safety as an educational component to address the needs of indigenous populations.58 102 104 105 In Tanzania, consideration should be given to ensuring that Maa-speaking staff acting as translators and/or patient advocates are available at all large health facilities and in predominantly Maasai communities. In Canada, the concept of ‘Two-Eyed Seeing’ was developed by indigenous elders.69 106 This emphasises a way of ‘walking in two worlds’ by incorporating traditional knowledge and modern or western knowledge into healthcare settings and interactions. Similarly, Maasai and other marginalised groups in Tanzania can inform policy, education and healthcare delivery to acknowledge these groups, breaking down barriers and assuring ethical space in healthcare settings. To address cultural safety and ethical space in Tanzania, medical and nursing training curricula should incorporate cultural competency and patient-focused care.
Limitations
There are limitations. The lead researcher is not from Maasai community, which may have led to power differentials in interviews and conversations. Maasai respondents often did not articulate what was observed by researchers and this may be explained by a history of not feeling authorised to offer critiques to ‘outsiders’. This was mitigated by the researcher spending extended periods of time in a Maasai community along with a Maasai research assistant. The emic and etic perspectives were shared and together formed a more cohesive interpretation of observations and findings. The domains of cultural safety identified in this study are specific to the Maasai population in Tanzania. We realise that these domains are not ‘one size fits all’ but provides a framework to be extended to assessment of barriers and facilitators in other marginalised populations.
Conclusion
These findings highlight the importance of deploying cultural safety and ethical space to inform shifts in healthcare spaces to make them more accessible, trusted and safe for Maasai people and other marginalised populations. This postcolonial discourse sheds light on ongoing power relations and how systems of dominance transcend healthcare settings, raising ethical questions about healthcare practice.
Employing Maa-speaking professionals or use of translators and/or patient advocates should be a more immediate consideration in Maasai communities. There is a need to enable Maasai and other marginalised groups to define their needs for cultural safety that can be met in a resource limiting context. This can inform development of culturally appropriate programmes and be used to educate healthcare professionals on culturally safe practices for marginalised groups.
In the long term, there is a need to redefine the healthcare worker, patient relationship including changing perceptions of patients towards a ‘person of value’,12 a need for critical reflection of power relations and avoid making assumptions. Cultural safety should be used as a moral discourse guiding national policy and evaluating inclusion and equity for marginalised populations in Tanzania
Data availability statement
Data are available on reasonable request. Data cannot be shared publicly without a request for a data transfer agreement from the Tanzania national ethics committee. Individual requests for transfer of data can be directed to National Institute for Medical Research in Tanzania (contact via ethics@nimr.or. tz) for researchers who meet the criteria for access to confidential data.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Ethics Committees of the National Institute for Medical Research, Tanzania (certificate no. NIMR/HQ/R.8a/Vol.IX/2237) and the London School of Hygiene & Tropical Medicine, UK (certificate no. 11237). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like first and foremost to extend their gratitude to the community for their participation in the study and welcoming the field team into their homes. Village leaders are particularly appreciated for their support for, and collaboration with, the study inception, design and data collection. The authors acknowledge the health facilities and patients who welcomed the field team to ‘hang out’ in facilities. Lastly, the authors would like to thank the thoughtful and thorough reviewers of this 890 paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Contributors TBM: conceptualisation, methodology, analysis, investigation, resources, data curation, writing-original draft, writing-review and editing, visualisation, project administration, funding acquisition; JM: analysis, investigation, writing-review and editing; JS: methodology, writing-review and editing; MJB: resources, supervision, writing-review and editing; SL: methodology, analysis, writing-review and editing, supervision. TBM is the guarantor who had access to all the data, and accepts responsibility for the work, the conduct of the study and the decision to publish.
Funding This study was funded by Chadwick Trust Travelling Fellowship and MJB is funded by Wellcome Trust (098481/Z/12/Z207472/Z/17/Z).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The reflexivity statement for this paper is linked as an online supplemental file 1.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.